
Abstract
This study examined the hypothesis that maternal socialization of coping would make a differential contribution to youth depression and externalizing psychopathology depending on youths’ level of exposure to life stress. A sample of 155 youth (M age = 12.41, SD = 1.21) and their maternal caregivers completed semi-structured interviews and questionnaires in a two-wave longitudinal study over a 1-year period. Results provided evidence for two types of socialization × stress interactions—an amplification-effects model and a differential-effects model. In the context of interpersonal stress, findings supported an amplification-effects model wherein the risk and protective effects of engagement and disengagement socialization of coping emerged in youth exposed to high but not mild levels of stress. In the context of noninterpersonal stress, findings supported a differential-effects model wherein disengagement socialization of coping contributed to heightened risk among youth exposed to high stress but dampened risk among youth exposed to mild stress. This research identifies maternal socialization of coping as a noteworthy contributor to risk for youth psychopathology, and highlights the need to consider parenting × environment interactions when investigating parenting processes related to youth psychopathology.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
According to the psychological resource principle, parents influence youth development by providing cognitive, affective, and behavioral resources to assist in the completion of life tasks (Pomerantz and Thompson 2008). One such task that youth frequently face is coping with both normative and atypical stressors. During times of stress, parental provision of adequate resources may protect youth against psychopathology, whereas provision of inadequate resources may enhance risk for psychopathology. Although much theory and research on youth psychopathology highlights the salient role of the parenting context (e.g., Deater-Deckard and Dodge 1997; Ge et al. 1994; Kim et al. 2003; Patterson 2001; Sheeber et al. 2001), this work typically has not considered the specific type of resources that parents provide youth to cope with stress. The present research examined the contribution of maternal socialization of coping to youth psychopathology, specifically depression and externalizing disorders, during times of stress.
Socialization of coping refers to parenting behaviors that communicate messages to youth about possible methods of coping with stress. Such messages may be conveyed through explicit instruction or coaching of youth (e.g., “try not to think about it,” “try to do something to calm yourself down”) or through modeling of parents’ own coping behavior. This study focused on explicit socialization of coping, exploring whether the suggestions parents make to youth about coping with stress predict subsequent risk for depression and externalizing psychopathology. More specifically, drawing from Compas and colleagues’ framework of responses to stress (Connor-Smith et al. 2000), we distinguished between engagement versus disengagement coping suggestions. Engagement coping refers to voluntary responses directed toward the source of stress or stress-related cognitions and emotions, such as problem solving, reflection, or emotion expression. Disengagement coping refers to voluntary responses directed away from the source of stress or stress-related cognitions and emotions, such as avoidance or denial. Although some research documents positive associations between engagement and disengagement coping strategies (Sandler et al. 1994, 2000; Zimmer-Gembeck and Locke 2007), perhaps reflecting a general tendency to engage in more or fewer coping efforts, these dimensions of coping typically are differentially associated with youth psychopathology. More specifically, engagement strategies (e.g., problem solving, support seeking, positive thinking) typically are associated with fewer symptoms, whereas disengagement strategies (e.g., avoidance, denial) typically are associated with heightened symptoms (Sandler et al. 1994, 2000; Wadsworth et al. 2005; Wadsworth and Berger 2006; for a review, see Compas et al. 2001), Thus, the distinction between engagement and disengagement coping is useful for understanding risk.
Socialization of Coping: Parents as a Resource in Times of Stress
When parents engage in socialization of coping, they provide youth with cognitive, affective, and behavioral strategies for coping with stress, either reinforcing or redirecting children’s typical coping behaviors. Consistent with the psychological resource principle, which predicts that parents’ influence on youth development is strongest when youths’ own resources are strained (Pomerantz and Thompson 2008), the effects of parent socialization of coping may be most salient when youth face high levels of stress. In such circumstances, the demands placed on youth may exceed their capacity to cope independently, thereby increasing their reliance on, and sensitivity to, parental guidance. This interactive influence of coping socialization and stress exposure would be consistent with a parenting × stress amplification-effects model, wherein the effects of socialization of coping on risk for psychopathology are stronger for youth exposed to high levels of stress than for those exposed to mild levels of stress. This model would predict stronger risk effects for maladaptive coping suggestions and stronger protective effects for adaptive coping suggestions. Empirical support for the amplification of risk effects for negative parenting (e.g., harsh parenting, low involvement) has been established in the context of chronic stressors, such as economic or neighborhood disadvantage (Brody et al. 2003; Plybon and Kliewer 2001; Shek 2002; Walsh 1992) and parent divorce (Pettit et al. 1997), as well as temporary stressors, such as difficult homework assignments (Pomerantz et al. 2005). Empirical support for the amplification of protective effects for positive parenting (e.g., inductive reasoning, supportiveness, authoritativeness, monitoring) has been established primarily in the context of heightened neighborhood disadvantage (Beyers et al. 2003; Dearing 2004; Meyers and Miller 2004; Natsuaki et al. 2007).
Extending the psychological resource principle, which focuses on the amount of parental resources, the type of resources that youth need also may vary according to their exposure to stress. Unlike aspects of parenting that primarily have predictable positive or negative effects on psychopathology (e.g., support, warmth, rejection), different types of coping suggestions may prevent or heighten risk for psychopathology as the effectiveness of coping strategies may depend on characteristics of the stressor at hand (Compas et al. 2001; Sandler et al. 1994), including its severity. This interactive influence of coping socialization and stress exposure would be consistent with a parenting × stress differential-effects model, wherein socialization of coping has different, but equally significant, effects on risk for psychopathology in the context of high versus mild stress. That is, socialization of coping might significantly predict heightened symptoms among youth exposed to mild stress and fewer symptoms among youth exposed to high stress, or vice versa. Guided by these two types of parenting × stress models—i.e., amplification effects and differential effects—the present study examined the interactive contribution of socialization of coping and stress to youth depression and externalizing psychopathology.
Contribution of Socialization of Coping to Psychopathology
Theory and research implicate self-regulatory difficulties, including maladaptive styles of coping with stress, in the development of both depression (Durbin and Shafir 2007; Flynn and Rudolph 2007; Sandler et al. 1994; Garber et al. 1995; Sheeber et al. 2000; for a review, see Silk et al. 2003) and externalizing psychopathology (e.g., conduct disorder, oppositional defiant disorder; Eisenberg et al. 2001, 2005; Rydell et al. 2003; Silk et al. 2003; Wadsworth and Compas 2002; Zeman et al. 2002; for a review, see Cole and Zahn-Waxler 1992). The implicit assumption underlying the present research was that parental socialization of coping exerts protective or exacerbating effects on psychopathology by encouraging youth to engage in either effective or ineffective efforts to regulate cognitive, affective, and behavioral responses to stress. Consistent with this assumption, parent coping suggestions are associated with children’s coping behavior as assessed by child reports (Kliewer and Lewis 1995), mother reports (Miller et al. 1994), and observations of a mother–child discussion task (Kliewer et al. 2006), indicating that these suggestions play an important role in youths’ in vivo coping efforts. Importantly, we anticipated that the consequences of parents’ socialization efforts would vary according to the severity of stress to which youth were exposed.
Engagement socialization of coping includes suggestions to directly address stressors and their emotional consequences, such as problem solving, reflecting about potential positive effects of a stressor, or regulating affect. Disengagement socialization of coping includes suggestions to avoid or deny stressors. Engagement coping is most commonly associated with lower levels of both internalizing and externalizing psychopathology (for a review, see Compas et al. 2001). Disengagement coping is most commonly associated with heightened internalizing psychopathology; the association between disengagement coping and externalizing psychopathology varies across studies (for a review, see Compas et al. 2001), perhaps due to unmeasured moderation by stress.
According to both a parenting × stress amplification-effects model and a parenting × stress differential-effects model, we hypothesized that engagement socialization of coping would protect youth against psychopathology and disengagement socialization of coping would heighten risk for psychopathology in the context of high levels of stress. When youth are exposed to severe stress, encouraging active engagement likely facilitates the successful resolution of stressors and/or the effective regulation of emotions, whereas encouraging disengagement likely interferes with youths’ ability or inclination to effectively manage stressors and accompanying negative emotions. Failure to resolve stressors or to manage emotional arousal may, in turn, put youth at risk for depression and externalizing psychopathology.
The two models diverge in their predictions regarding the influence of coping socialization on psychopathology in the context of mild stress. An amplification-effects model predicts that coping socialization will have a negligible effect on psychopathology in the context of mild stress. Specifically, youth may be able to mobilize their own resources for coping with mild stress, and are therefore less dependent on, and sensitive to, parent socialization efforts. In contrast, a differential-effects model predicts that coping socialization will have a significant but different effect on youth exposed to mild relative to high levels of stress. This model assumes that youth require guidance for coping with both mild and severe stressors, but the optimal guidance may differ. Whereas parental encouragement to engage with severe stressors may be useful, an excessive focus on relatively mild stressors, which have little impact on youth, could lead youth to “over-think” rather than overlook such stressors. For example, encouraging cognitive engagement with everyday hassles could foster a ruminative response style, a known risk factor for depression (Papadakis et al. 2006; Treynor et al. 2003). Similarly, an inability to move past or shrug off daily hassles (in the form of hostile attribution biases or emotional overreactions) represents a risk factor for externalizing psychopathology (de Castro et al. 2002; Dodge et al. 1995). In contrast, encouraging disengagement from mild stressors may prevent or redirect excessive and inappropriate responses (e.g., anger, sadness, frustration, aggression). Thus, for youth exposed to mild levels of stress, it is possible that engagement socialization of coping would contribute to heightened psychopathology over time and disengagement socialization of coping would contribute to less psychopathology over time.
Stress Specificity and Sex Differences
We further examined whether the contribution of socialization of coping × stress interactions to youth psychopathology differed across domains of stress or across sex. Consistent with interpersonal theories of depression (Hammen 2006; Joiner et al. 1999), research suggests that interpersonal stress (e.g., disruptions or conflicts in parent–child, peer, or romantic relationships) more strongly predicts subsequent youth depression than does noninterpersonal stress (e.g., academic troubles) (Rudolph et al. 2009; for a review, see Rudolph et al. 2008). Some research also suggests that noninterpersonal stress is more consistently associated with externalizing psychopathology than is interpersonal stress (Little and Garber 2004; Rudolph et al. 2000). Thus, socialization of coping in the context of interpersonal stressors may be particularly relevant to depression, whereas socialization of coping in the context of noninterpersonal stressors may be particularly relevant to externalizing psychopathology.
Moreover, parent socialization of coping may have different effects on girls and boys, particularly in the context of interpersonal stress. Specifically, gender-linked social goals may lead to sex differences in the implementation of coping suggestions. For example, girls place a greater emphasis than boys on maintaining relationship intimacy and resolving peer problems (Rose and Rudolph 2006). Thus, for example, if parents encourage girls to engage in response to an argument with a friend, girls may discuss and resolve the dispute, thereby reducing stress and subsequent psychopathology. In contrast, boys place a greater emphasis than girls on self-presentation and control in relationships (Rose and Rudolph 2006). Thus, if parents encourage boys to engage in response to an argument with a friend, boys may confront their peer and attempt to establish dominance, thereby increasing stress and subsequent psychopathology.
Study Overview
In sum, the present study investigated whether exposure to interpersonal and noninterpersonal stress moderated the contribution of parent socialization of coping to subsequent youth depression and externalizing psychopathology. Maternal caregivers reported on coping suggestions they commonly make to their youth. Youth psychopathology was assessed using multiple methods, including a structured clinical interview, youth report (depression), and caregiver report (externalizing psychopathology). Finally, a life stress interview was administered to caregivers and youth. This methodology uses specific contextual information to determine the objective threat associated with particular life events, thereby limiting subjective reporting biases and yielding a relatively objective assessment of life stress.
Method
Participants
Participants included 155 youth (81 girls, 74 boys, M age = 12.41, SD = 1.21, 4th–8th graders at Wave 1) and their primary female caregivers (89% biological mothers, 3.2% adoptive mothers, 7.8% other) involved in a longitudinal study examining the development of psychopathology during the transition to adolescence (for previous reports on this study, see Krackow and Rudolph 2008; Rudolph 2008; Rudolph et al. 2009). Participants resided in small urban and rural communities in the Midwest. The majority of this subsample was White (74.2%); the remainder of the participants was African American (13.5%) or represented other ethnic groups and biracial youth (12.3%). The participants came from a wide range of socioeconomic classes as reflected in annual income (16.4% below $30,000; 50% $30–59,999; 21.1% $60,000–89,999, and 12.5% over $90,000).
Participants in the longitudinal study were recruited based on school-wide screenings using the Children’s Depression Inventory (CDI; Kovacs 1981). From the screening sample (n = 1985), we selected potential participants (n = 468) along the range of the CDI, oversampling slightly for youth with severe depressive symptoms (15.8% of the screening sample, 20.3% of targeted youth, and 24.1% of recruited youth had scores > 18). Participant recruitment criteria included CDI scores, the presence of a maternal caregiver in the home, and a 1-h driving proximity to the university. Potential participants were excluded if the youth had a non-English speaking maternal caregiver or a severe developmental disability that would prevent completion of the assessment.
Participants in the longitudinal study and nonparticipantsFootnote 1 did not significantly differ in sex, χ2(N = 468, df = 1) = 0.39, ns, ethnicity (White versus minority), χ2(N = 468, df = 1) = 0.02, ns, or CDI scores, t(280) = 1.11, ns. Participants (M = 12.41, SD = 1.19) were slightly younger than nonparticipants (M = 12.65, SD = 0.89), t(275) = 2.28, p < 0.05. Of the 167 families who participated in the study at Wave 1 (W1), 161 had socialization of coping data. At Wave 2 (W2), data relevant to these analyses were available for 155 families (92.8% of the total sample). Participants with complete data did not differ from those with incomplete data in sex, χ2(N = 167, df = 1) = 1.71, ns, ethnicity, χ2(N = 167, df = 1) = 0.06, ns, age, t(165) = 0.02, ns, W1 engagement coping suggestions, t(159) = −0.10, ns, W1 disengagement coping suggestions, t(159) = 0.02, ns, W1 interpersonal stress, t(165) = −0.63, ns, W1 noninterpersonal stress, t(165) = −1.60, ns, W1 depression, t(165) = −1.15, ns, or W1 externalizing psychopathology, t(165) = −1.57, ns.
Procedure
All procedures for this study were approved by the university Institutional Review Board. Families were invited to participate via phone calls to the primary female caregivers. Specifically, families were invited to participate in a longitudinal study about development across adolescence. Researchers conducted an in-person, 3- to 4-h initial assessment with interested families. Caregivers provided written informed consent, and youth provided written assent. Youth and their maternal caregivers completed the assessment separately. A follow-up interview was completed 1 year later. At each assessment, caregivers were compensated for their time with a monetary reimbursement ranging from $25 to $45, and youth were given a gift certificate.
To avoid contamination of the diagnostic and life stress information, two different staff members conducted these interviews. Diagnostic interviews were conducted by a faculty member in clinical psychology, a post-doctoral fellow in clinical psychology, psychology graduate students, or a post BA-level research assistant. All diagnoses were made through consultation with a clinical psychology faculty member or a post-doctoral student in clinical psychology. Life stress interviews were conducted by a post-doctoral student in clinical psychology, psychology graduate students, a post BA-level research assistant, or advanced undergraduate students. Interviewers underwent extensive preliminary training with the second author (or, for the life stress interview, a highly trained experienced interviewer) that involved: (a) reviewing the interview protocols and diagnostic criteria, (b) listening to prior audiotaped interviews and making independent diagnoses, and (c) role-playing and feedback. They also received extensive feedback based on audiotapes of their interviews, as well as during consensual coding sessions.
Measures
Table 1 presents descriptive information for the measures.
Socialization of Coping Questionnaire
A 17-item Socialization of Coping (SOC) Questionnaire was developed to assess general coping suggestions that parents commonly make to their children. The measure was designed to include coping suggestions appropriate for youth from middle childhood through adolescence in accordance with the engagement–disengagement framework of responses to stress (Compas et al. 2001). Eleven items were adapted from several subscales of the Responses to Stress Questionnaire (RSQ; Connor-Smith et al. 2000). These items were slightly reworded or truncated to reflect coping suggestions rather than coping behavior. Because direct socialization of coping only involves encouragement of purposeful coping responses, items reflecting involuntary responses to stress were not included. To provide a comprehensive coverage of types of coping that were deemed important but were not included in the RSQ, six additional items were written or adapted from other child coping measures. The resulting 17 items reflected cognitive, affective, and behavioral responses to stress. Mothers were prompted with the question: “When your child has a problem or is upset, how much do you do each of the following?” Mothers rated each item on a five-point scale (1 = Not at all to 5 = Very much).
To confirm the validity of the proposed engagement–disengagement framework of coping socialization, a maximum likelihood confirmatory factor analysis was conducted using AMOS 7.0 (Arbuckle 2006). Two latent variables were created. The latent variable Engagement was composed of eight indicators, each representing a suggestion that youth orient themselves toward the source of stress or negative emotion (e.g., “Encourage him/her to do something to try to fix the problem or take action to change things.” “Encourage him/her to think about things he/she is learning from the situation.”). Based on preliminary analyses, one Engagement item (“Encourage or allow him/her to cry about the problem”) was omitted due to a nonsignificant factor loading, leaving seven indicators on the Engagement latent variable. The latent variable Disengagement was composed of nine indicators, each representing a suggestion that youth distance themselves from stress or negative emotion (e.g., “Encourage him/her not to focus on his/her negative feelings.” “Encourage him/her to just act like the problem never happened and go on with his/her life.”). Given prior evidence that different dimensions of coping are often positively correlated (Sandler et al. 1994, 2000; Zimmer-Gembeck and Locke 2007), the Engagement and Disengagement latent variables were allowed to correlate with one another, but indicators were only allowed to load on one factor. Correlations between certain error terms for the indicators were allowed based on modification indices and consistency with the theoretical model. This model showed an excellent fit to the data, χ2(N = 156, df = 92) = 128.91, p < 0.01, χ2/df = 1.40, CFI = 0.97, IFI = 0.97, RMSEA = 0.05. All items loaded significantly on their respective factors (βs = 0.54–0.89, ps < 0.001, for engagement; βs = 0.56–0.76, ps < 0.001 for disengagement). Mean scores for engagement (α = 0.87) and disengagement (α = 0.89) coping suggestions were computed. As anticipated, engagement and disengagement suggestions were moderately positively correlated, r(161) = 0.39, p < 0.01. Strong cross-temporal stability was found for engagement suggestions, r(150) = 0.71, p < 0.001, and disengagement suggestions, r(150) = 0.73, p < 0.001. Establishing construct validity of the measure, coping suggestions significantly predicted youth-reported responses to stress both concurrently and over time.
Youth Life Stress Interview
Interviewers individually administered the Youth Life Stress Interview (Rudolph and Flynn 2007), an adaptation of the Child Episodic Life Stress Interview (Rudolph and Hammen 1999; Rudolph et al. 2000), to youth and their caregivers. This semi-structured interview applies the contextual threat method (Brown and Harris 1978) to assess the type and severity of episodic stress encountered by youth during the preceding year. Standardized probes elicit objective information about stressful events occurring across multiple life domains (e.g., same-sex and opposite-sex peer relationships, parent–child relationships, school, health). Interviewers began with a general open-ended question about youths’ exposure to stressful events in the past year, and then prompted youth regarding specific stressful events within each domain (e.g., end of a friendship, an argument with parents, receiving detention, an injury). Follow-up questions were used to elicit detailed information about each event, the timing and duration of the event, and the objective consequences of the event. Interviewers compiled this information into a narrative summary of each event, which was then presented to a team of coders with no knowledge of the youth’s diagnostic status or subjective response to the event.
Integrating information from youth and caregivers, the coding team provided a rating of the objective stress or negative impact associated with the event for a typical youth in those circumstances, from 1 (No negative stress) to 5 (Severe negative stress); events with ratings of 1 were excluded. The team also categorized each event as interpersonal (i.e., events that involved a significant interaction between the youth and another person or that directly affected the relationship between the youth and another person) or noninterpersonal (all other events). Two composite scores reflecting interpersonal stress (e.g., conflict with a parent, a friend moving away) and noninterpersonal stress (e.g., failing an exam, visiting the emergency room for an injury) were calculated by summing the stress ratings across all relevant events with a stress rating above 1. If only one informant provided information about an event, this information was used for the ratings. W1 interpersonal stress scores ranged from 0 to 36, and W1 noninterpersonal stress scores ranged from 0 to 21.5. To assess reliability, 160 life events (14% of the total reported events) were coded by two independent teams. High reliability was found for ratings of objective stress (ICC = 0.90) and dependence (ICC = 0.96), as well as for the categorization of event content (Cohen’s ĸ = 0.92).
Schedule for Affective Disorders and Schizophrenia for School-Age Children-Epidemiologic Version-5 (K-SADS-E)
To assess youth depression and externalizing psychopathology, interviewers individually administered the K-SADS-E (Orvaschel 1995) to youth and their caregivers. All interviews were coded in consultation with a clinical psychology faculty member or post-doctoral fellow. A best-estimate approach (see Klein et al. 1994, 2005) was used to combine caregiver and youth information regarding the nature, severity, frequency, duration, and resulting impairment of the reported symptoms according to DSM-IV-TR criteria (American Psychiatric Association 2000).
For each period of major depression and each period and type of externalizing psychopathology (e.g., conduct disorder, oppositional defiant disorder), interviewers provided ratings on a continuous 5-point scale: 0 = No symptoms, 1 = Mild symptoms, 2 = Moderate symptoms, 3 = Diagnosis with mild impairment, 4 = Diagnosis with severe impairment. Ratings were assigned along a single scale for both diagnosable episodes and subthreshold symptoms that occurred during the month preceding the interview, including the present. Subthreshold symptoms (i.e., mild or moderate; a rating of 1 or 2) reflected the presence of symptoms that failed to meet one or more of the DSM criteria for a diagnosis (e.g., the youth had fewer than the required number of symptoms or had the required number of symptoms for less than the required duration). Ratings were summed across period and type of psychopathology to create continuous scores of depression severity and externalizing psychopathology severity for each wave of the study. Higher ratings reflect more severe symptoms for a single diagnosis, the presence of symptoms of multiple diagnoses (e.g., conduct disorder and oppositional defiant disorder), and/or multiple periods of disorder (for similar rating approaches, see Davila et al. 1995; Hammen et al. 2003, 2004; Rudolph et al. 2000). Thus, these scores represent composite indexes of several different markers of depression and externalizing severity. This type of continuous index is consistent with contemporary conceptualizations, derived in part from taxometric analyses, that view psychopathology as best represented by dimensional continuums rather than discrete categories (Fergusson et al. 2005; Hankin et al. 2005; Lahey et al. 2008). Independent raters coded audiotapes of 25% of the interviews. Strong inter-rater reliability was found for the depression ratings (one-way random-effects intraclass correlation coefficient [ICC] = 0.95) and the externalizing ratings (ICC = 0.87).
Across the two waves of the study, 16.1% of the sample (18.3% of girls and 13.7% of boys) experienced subthreshold symptoms of major depression, and 8.0% (8.5% of girls and 6.8% of boys) experienced diagnostic-level major depression. For externalizing psychopathology, 22.5% of the sample (18.3% of girls and 27.4% of boys) experienced subthreshold symptoms, and 8.4% (7.3% of girls and 9.6% of boys) experienced diagnostic-level externalizing disorders. Thus, a reasonable percentage of participants experienced psychopathology over the course of the study.
Youth Depression Inventory (YDI)
Youth completed the YDI (Rudolph 2002), a self-report measure of depressive symptoms. This measure taps specific symptoms of depression drawn from the K-SADS interview. The measure includes 20 symptoms (e.g., “I feel sad, moody, or down a lot or like I’m going to cry,” “I feel tired a lot or have less energy than usual”), which youth rated on a 5-point scale of severity (1 = Not at all to 5 = Very much). A mean score of the items was computed, with higher scores reflecting higher levels of symptoms (α = 0.90).
Child Behavior Checklist (CBCL)
Mothers completed the externalizing subscale of the Child Behavior Checklist (CBCL; Achenbach 1991), which includes 13 items assessing delinquent behavior (e.g., “Doesn’t seem to feel guilty after misbehaving”) and 20 items assessing aggressive behavior (e.g., “Gets in many fights”). Mothers rated on a three-point scale (0 = Not true, 1 = Somewhat or sometimes true, 2 = Very true or often true) the extent to which each item applied to youth. A T score of the items was computed. The CBCL has been found to distinguish clinical and nonclinical groups (Achenbach 1991) and the factor structure has been validated in numerous samples (for a review, see Achenbach et al. 2008).
Creation of Composite Psychopathology Scores
Significant correlations were found between the interview and questionnaire measures of depression at W1 (r = 0.33, p < 0.001) and W2 (r = 0.49, p < 0.001). Likewise, significant correlations were found between the interview and questionnaire measures of externalizing psychopathology at W1 (r = 0.51, p < 0.001) and W2 (r = 0.53, p < 0.001). Because the interview and questionnaire measures of psychopathology were significantly correlated, and composite scores provide increased reliability and reduce the impact of measurement error (Rushton et al. 1983; Schwartz et al. 1985), composite scores were created (see Lengua 2006; Lengua et al. 2000; Sheeber et al. 2007; Wadsworth et al. 2005). Specifically, a composite score of depression was created by standardizing and summing the K-SADS and YDI depression scores within each wave. A composite score of externalizing psychopathology was created by standardizing and summing the K-SADS and CBCL externalizing psychopathology scores within each wave.
Results
Descriptive and Correlational Findings
Table 1 presents descriptive statistics separately by sex. A repeated-measures Multivariate Analysis of Variance (MANOVA) was conducted on the study variables with sex as a between-subjects factor, and wave as a within-subjects factor. This analysis revealed a marginal multivariate main effect for sex, F(6, 142) = 2.06, p < 0.10. Univariate analyses revealed that girls experienced marginally higher levels of composite depression across waves than did boys, F(1, 155) = 3.75, p < 0.10. Univariate analyses also revealed that boys experienced marginally higher levels of noninterpersonal stress across waves than did girls, F(1, 155) = 3.45, p < 0.10. The absence of a significant sex difference in interpersonal stress may be accounted for by the fact that more than half of the sample was younger than 13 years of age, and research suggests that a sex difference in interpersonal stress occurs during adolescence (Hankin et al. 2007; Rudolph and Hammen 1999).
Table 2 presents intercorrelations among the variables separately for girls and boys. Overall, there were few significant zero-order correlations between socialization of coping and psychopathology, with two exceptions. In girls, W1 engagement coping suggestions were significantly associated with less W2 externalizing psychopathology, and W1 disengagement coping suggestions were marginally associated with more W1 depression. Fisher r-to-Z transformations revealed that these associations were significantly stronger in girls than in boys (Zs ≥ 2.35, ps < 0.05). Interpersonal stress was positively associated with W1 and W2 depression and externalizing psychopathology in both girls and boys, but the association between interpersonal stress and W1 depression was significantly stronger in girls than in boys, (Z = 2.49, p < 0.05). No significant zero-order correlations emerged between noninterpersonal stress and depression or externalizing psychopathology.
Overview of Analyses
Four hierarchical multiple regression analyses were conducted to examine whether youths’ exposure to stress (interpersonal and noninterpersonal) moderated the effects of maternal socialization of coping (SOC) on subsequent youth psychopathology. Separate regressions were conducted to examine interactions between SOC and interpersonal versus noninterpersonal stress. The first set of analyses examined the prediction of W2 depression and the second set of analyses examined the prediction of W2 externalizing psychopathology, adjusting for prior (W1) levels of psychopathology (entered at the first step). To investigate the specificity of effects predicting depression versus externalizing psychopathology, each analysis also adjusted for the alternate type of W2 psychopathology at the first step.Footnote 2 The main effects of engagement SOC, disengagement SOC, stress, and sex were entered at the second step, the two-way interactions were entered at the third step, and the three-way interactions were entered at the fourth step. Continuous predictors were mean-centered prior to analysis and calculation of the interaction terms.
When the three-way interactions with sex were nonsignificant, follow-up regressions were conducted excluding sex from the analyses. When the three-way Engagement SOC × Disengagement SOC × Stress interaction was nonsignificant, this interaction was dropped from the analyses. The one significant three-way interaction with sex is summarized in the text. Tables 3 and 4 present the results of analyses collapsed across sex. Following Aiken and West (1991), significant two-way interactions were interpreted by solving the unstandardized regression equation to predict W2 psychopathology at mild (−1 SD), moderate (mean), and high (+1 SD) levels of stress. The single significant three-way interaction for sex was interpreted in the same manner separately for girls and boys. The single significant three-way Engagement SOC × Disengagement SOC × Stress interaction was interpreted by solving the unstandardized regression equation at low (−SD), moderate (mean), and high (+SD) levels of Engagement SOC separately for children exposed to high (above the median) versus low (equal to or below the median) stress.
Socialization of Coping × Stress Predicting W2 Depression
Table 3 summarizes results from regression analyses predicting W2 depression.
SOC × Interpersonal Stress
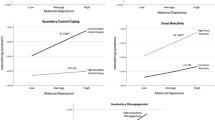
Regression analysis predicting depression in the context of interpersonal stress revealed no significant three-way interactions between sex and other predictors, |β|s ≤ 0.14, |t|s(138) ≤ 1.27, ns. A follow-up analysis collapsing across sex revealed a significant Disengagement SOC × Interpersonal Stress interaction, a significant Engagement SOC × Disengagement SOC interaction, and a significant Engagement SOC × Disengagement SOC × Interpersonal Stress interaction (β = −0.20, t(145) = −2.40, p < 0.05). This analysis revealed no other significant main effects or interactions. To decompose this three-way interaction, the two-way Engagement SOC × Disengagement SOC interaction was examined separately in children exposed to mild versus high interpersonal stress. For children exposed to mild interpersonal stress, analyses revealed nonsignificant main effects for Engagement SOC (β = −0.19, t(72) = −0.98, ns) and Disengagement SOC (β = −0.06, t(72) = −0.53, ns) and a nonsignificant Engagement SOC × Disengagement SOC interaction (β = −0.07, t(72) = −0.69, ns). For children exposed to high interpersonal stress, analyses revealed significant main effects for Engagement SOC (β = −0.26, t(71) = −2.20, p < 0.05) and Disengagement SOC (β = 0.35, t(71) = 2.55, p < 0.05) and a significant Engagement SOC × Disengagement SOC interaction (β = −0.24, t(71) = −2.15, p < 0.05). Decomposition of this two-way interaction revealed that W1 disengagement coping suggestions significantly predicted heightened W2 depression for youth who received low (β = 0.57, t(71) = 3.01, p < 0.01) or moderate (β = 0.35, t(71) = 2.85, p < 0.05) but not high (β = 0.13, t(71) = 1.04, ns) levels of engagement suggestions (Fig. 1). Thus, consistent with a parenting × stress amplification-effects model, the engagement × disengagement coping suggestions interaction predicted depression in youth exposed to high but not mild levels of interpersonal stress. Specifically, disengagement coping suggestions served as a risk factor for depression in the context of mild but not high levels of engagement coping suggestions.

Disengagement SOC × engagement SOC interaction predicting subsequent depression in the context of high interpersonal stress, adjusting for prior depression and concurrent externalizing psychopathology
SOC × Noninterpersonal Stress
Regression analysis predicting depression in the context of noninterpersonal stress revealed a marginal Engagement SOC × Disengagement SOC × Sex interaction (β = −0.21, t(138) = −1.98, p < 0.10); this analysis revealed no other significant three-way interactions (|β|s < 0.08, |t|s(138) < 0.77, ns). Decomposition of this interaction revealed no significant associations in boys or girls; thus, sex was dropped from the analysis. A follow-up analysis collapsing across sex revealed a marginal Engagement SOC × Disengagement SOC interaction; however, because this two-way interaction was moderated by interpersonal stress (as described earlier and depicted in Fig. 1), no further analyses were conducted. This analysis revealed no other significant main effects or interactions (see Table 3). Together, these findings were consistent with the hypothesis that interpersonal, but not noninterpersonal, stress would moderate the contribution of coping suggestions to depression.
Socialization of Coping × Stress Predicting W2 Externalizing Psychopathology
Table 4 summarizes results from regression analyses predicting W2 externalizing psychopathology.
SOC × Interpersonal Stress
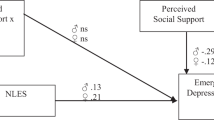
Regression analysis predicting externalizing psychopathology in the context of interpersonal stress revealed a significant three-way Engagement SOC × Interpersonal Stress × Sex interaction (β = −0.33, t(140) = −3.33, p < 0.01); this analysis revealed no other significant three-way interactions (|β|s ≤ 0.11 |t|s(138) ≤ 1.09, ns). Separate regressions were conducted to examine the two-way Engagement SOC × Interpersonal Stress interaction in girls and boys. For girls, analyses revealed a significant negative main effect for Engagement SOC (β = −0.25, t(76) = −2.48, p < 0.05), a nonsignificant main effect for Disengagement SOC (β = 0.03, t(76) = 0.30, ns), a significant positive main effect for Interpersonal Stress (β = 0.27, t(76) = 2.49, p < 0.05), a significant Engagement SOC × Interpersonal Stress interaction (β = −0.25, t(73) = −2.38, p < 0.05), and a nonsignificant Disengagement SOC × Interpersonal Stress interaction (β = −0.05, t(73) = −0.48, ns). For boys, analyses revealed nonsignificant main effects of Engagement SOC (β = 0.16, t(67) = 1.48, ns), Disengagement SOC, (β = −0.09, t(65) = −0.90, ns), and Interpersonal Stress (β = 0.15, t(67) = 1.54, ns), a significant Engagement SOC × Interpersonal Stress interaction (β = 0.32, t(64) = 2.62, p < 0.05), and a nonsignificant Disengagement SOC × Interpersonal Stress interaction (β = −0.05, t(64) = −0.38, ns). Decomposition of the Engagement SOC × Interpersonal Stress interactions revealed an opposing pattern of effects for girls and boys (see Fig. 2). For girls, the pattern of effects was consistent with a parenting × stress amplification-effects model. Specifically, engagement coping suggestions significantly predicted less W2 externalizing psychopathology for girls exposed to high (β = −0.50, t(74) = −3.21, p < 0.01) and moderate (β = −0.23, t(73) = −2.12, p < 0.05) levels of interpersonal stress, but were not significantly related to externalizing psychopathology for girls exposed to mild levels of interpersonal stress (β = −0.11, t(74) = −0.93, ns). For boys, the pattern of effects was not in the anticipated direction. Specifically, engagement coping suggestions significantly predicted heightened W2 externalizing psychopathology for boys exposed to high levels of interpersonal stress (β = 0.35, t(66) = 2.97, p < 0.01), but were not significantly related to W2 externalizing psychopathology for boys exposed to moderate (β = 0.10, t(63) = 0.88, ns) or mild levels of interpersonal stress (β = −0.18, t(66) = −1.20, ns). Thus, these results are most consistent with a parenting × stress amplification-effects model wherein socialization of coping exerted a significant effect only under high levels of stress. Overall, in the context of high interpersonal stress, engagement coping suggestions served as a protective factor against externalizing psychopathology for girls but as a risk factor for boys.

Engagement SOC × interpersonal stress interaction predicting subsequent externalizing psychopathology for a girls and b boys, adjusting for prior externalizing psychopathology and concurrent depression
SOC × Noninterpersonal Stress
Regression analysis predicting externalizing psychopathology in the context of noninterpersonal stress revealed no significant three-way interactions between sex and other predictors (|β|s ≤ 0.15, (|t|s(138) ≤ 1.49, ns). A follow-up analysis collapsing across sex revealed a significant Disengagement SOC × Noninterpersonal Stress Interaction; this analysis revealed no other significant main effects or interactions (see Table 4). Consistent with a parenting × stress differential-effects model, decomposition of this interaction revealed an opposing pattern of effects for youth exposed to different levels of stress (see Fig. 3). Disengagement coping suggestions marginally predicted heightened W2 externalizing psychopathology for youth exposed to high (β = 0.22, t(148) = 1.94, p < 0.10) and moderate (β = 0.14, t(146) = 1.74, p < 0.10) levels of noninterpersonal stress, and significantly predicted less externalizing psychopathology for youth exposed to mild levels of noninterpersonal stress (β = −0.23, t(148) = −2.30, p < 0.05). Thus, when predicting externalizing psychopathology, disengagement coping suggestions served as a risk factor for youth exposed to high or moderate levels of noninterpersonal stress but as a protective factor for youth exposed to low levels of noninterpersonal stress.

Disengagement SOC × noninterpersonal stress interaction predicting subsequent externalizing psychopathology, adjusting for prior externalizing psychopathology and concurrent depression
Discussion
The present research investigated the interactive contribution of maternal coping socialization and stress exposure to subsequent youth psychopathology. Two possible parenting × stress interaction models were proposed: an amplification-effects model and a differential-effects model. For socialization of coping × interpersonal stress interactions, results supported an amplification-effects model: The predictive effects of parent socialization of coping on depression and externalizing psychopathology were amplified for youth exposed to high relative to mild levels of stress. For socialization of coping × noninterpersonal stress interactions, results supported a differential-effects model: Socialization of coping predicted different patterns of psychopathology for youth exposed to high versus mild levels of stress.
Socialization of Coping and Youth Depression
Disengagement coping suggestions significantly predicted heightened depression for youth exposed to high, but not mild or moderate, levels of interpersonal stress. Furthermore, this association was only significant for children who received low, but not moderate or high, levels of engagement suggestions. This pattern is consistent with a parenting × stress amplification-effects model, wherein the harmful effects of disengagement coping suggestions on depression were amplified in youth exposed to more severe interpersonal stress. Furthermore, this interaction was significant for interpersonal but not noninterpersonal stress, supporting the idea that interpersonal stress is key to the development of youth depression (Rudolph et al. 2008).
Disengagement suggestions include encouragement to avoid, deny, or distract oneself from stress or negative emotions, strategies that are unlikely to promote successful resolution of relationship stressors if enacted by youth. As a result, parents who encourage youth to disengage in the context of recurring or severe relationship stress potentially undermine youths’ ability to maintain healthy relationships. As proposed by interpersonal theories of depression, poor quality relationships, interpersonal stress, and conflict are likely to create risk for depression (for a review, see Rudolph et al. 2008). Thus, disengagement suggestions might direct highly stressed youth toward a pathway that both prevents resolution of relationship stress and erodes social support networks over time, leaving youth vulnerable to depression. However, our results suggest that moderate to high levels of engagement suggestions, such as encouraging youth to problem solve or to regulate emotions, buffer children from the harmful effects of disengagement suggestions. In other words, the negative effects of disengagement suggestions only emerged for children who received low levels of engagement suggestions in the context of high interpersonal stress. It is possible that frequent encouragement to disengage from stress coupled with infrequent encouragement to engage with stress communicates to children that the parent does not believe the child is capable of dealing with stress directly, which would undermine children’s coping self-efficacy and self-worth, placing them at heightened risk for depression. Additionally, children who receive moderate to high levels of both types of coping suggestions will likely be equipped with a more comprehensive coping repertoire; although their parents encourage some maladaptive disengagement coping strategies, these children will also have more adaptive engagement strategies available, which will protect them from the emotional cost of developing depressive symptoms.
Although engagement coping interacted with disengagement coping and interpersonal stress to predict depression over time, engagement coping suggestions did not independently predict depression. Different types of engagement suggestions may have opposite effects on depression, resulting in a null effect. Socialization of behavioral engagement (e.g., problem solving) or active forms of cognitive engagement (e.g., forming a plan, rethinking the situation) may assist youth in resolving stress and reduce their subsequent emotional distress. Conversely, socialization of affective engagement (e.g., emotional expression) or passive forms of cognitive engagement (e.g., reflection upon the problem) could result in over-involvement with the stressor and consequent risk for emotional distress. Future research should be directed toward examining the effects of different types of engagement coping suggestions on psychopathology.
Socialization of Coping and Youth Externalizing Psychopathology
Engagement coping suggestions differentially predicted externalizing psychopathology in the context of interpersonal stress for girls versus boys. For girls, engagement suggestions had a protective effect, predicting less externalizing psychopathology over time. Consistent with a parenting × stress amplification-effects model, this association was strongest for girls exposed to high stress. For high-stressed boys, however, engagement suggestions had a detrimental effect, predicting heightened externalizing psychopathology. Thus, under high stress, when youths’ coping resources were most likely to be overwhelmed, girls benefited most from mothers’ encouragement to direct resources toward stressors, whereas boys were most at risk as a function of engagement suggestions.
In the context of interpersonal stress, girls and boys may react to socialization of coping in different ways. Research suggests that girls are more socially competent than boys (e.g., Jones et al. 1998; Rudolph and Conley 2005; Spinrad et al. 2006). As a result, in the face of severe interpersonal stress, girls may be more prepared than boys to effectively implement parent coping suggestions that potentially require social skills (e.g., resolving an argument, confronting a bully). Girls and boys also may select different strategies in response to parental encouragement to engage with stress. For example, when responding to peer conflict, boys are more likely than girls to have goals of gaining control or retaliating against peers (Chung and Asher 1996; Rose and Asher 1999). Thus, when parents encourage problem solving about interpersonal stressors, boys may be more likely than girls to view efforts to gain control or dominance as an appropriate strategy, placing them at risk for aggression and associated externalizing psychopathology.
In the context of noninterpersonal stress, support was obtained for a parenting × stress differential-effects model in both girls and boys: Disengagement socialization of coping served as a risk factor for externalizing psychopathology in high and moderately-stressed youth but as a protective factor against externalizing psychopathology in mildly stressed youth. Noninterpersonal stressors among youth typically include problems such as academic failure or school disciplinary actions. Encouraging youth to disengage in the context of moderate to severe noninterpersonal stress may communicate to youth either that parents are not concerned about academics and conduct, or that parents do not believe that engaging with such problems is a useful response. This could, in turn, lead youth to perceive these stressors as normative or inalterable, thereby decreasing their likelihood of resolving noninterpersonal stress. Disengaging from the school context is likely to promote further failures that increase risk for subsequent externalizing psychopathology (Patterson et al. 1989). However, disengagement suggestions in the context of mild academic and behavioral stressors could prevent youth from over-reactive responses, such as hostile attributional biases or angry/aggressive outbursts; avoidance of these responses would then decrease risk for externalizing psychopathology.
Implications for Theory and Research
Providing a novel theoretical perspective, the present research identifies socialization of coping as a domain of parenting behavior with critical implications for youth psychopathology. Although individual differences in parent socialization of coping and links with youth coping behavior have been established (Kliewer et al. 1996, 2006; Miller et al. 1994), this study is the first to examine the longitudinal contribution of coping socialization to psychopathology. Our results suggest that acting as a resource for youth in times of stress is a critical parenting task that warrants further study.
Specifically, these findings expand our understanding of the processes linking parenting and youth psychopathology in two ways. First, this study builds on previous research linking deficits in parent supportiveness and warmth to depression (e.g., Park et al. 2008; Sheeber et al. 2007) and externalizing psychopathology (e.g., Kim et al. 1999; Scaramella et al. 1999) by identifying socialization of coping as a specific mode through which parents provide youth with resources and consequently contribute to, or provide protection from, youth psychopathology. In our study, some highly stressed youth received parent support in the form of disengagement suggestions, but in certain contexts this form of support actually undermined youths’ well-being. Thus, these findings implicate the type of resources that parents provide and the context in which parents offer their support (i.e., severity and domain of life stress) as important determinants of risk for psychopathology.
Second, these findings add to a growing body of evidence that the link between parenting behaviors and youth psychopathology is moderated by contextual factors. For example, Natsuaki et al. (2007) found that the protective effect of parental inductive reasoning techniques against depression was strongest for families living in more troubled neighborhoods. Similar parenting × neighborhood disadvantage interactions have been observed for externalizing psychopathology (Beyers et al. 2003; Brody et al. 2003). Research also identifies other factors that moderate the influence of parenting practices on youth psychopathology, including maternal depression (Brennan et al. 2003), peer relationships (Lansford et al. 2003), temperament (Lengua et al. 2000), and family ethnicity (Lansford et al. 2004). Together, these findings suggest that understanding parent contributions to youth psychopathology requires a consideration of the context in which parenting takes place.
Implications for Intervention and Prevention
This research suggests that parent socialization of coping has the potential to reduce or intensify risk for psychopathology, depending on the form of coping suggestions offered and the type and severity of stressors. Socialization of appropriate coping strategies is a teachable skill that may be integrated into existing youth-centered coping interventions or broader parenting interventions. The challenge before us lies in helping parents learn how to generate appropriate coping suggestions that will support their child’s well-being.
The present study also suggests a need for parents to be sensitive to the type and amount of stress that youth experience. Overall, socialization of coping had the strongest protective and adverse effects for highly stressed youth. Thus, conditions of high stress represent a challenging but critical opportunity for parents to provide coping resources to their children and buffer them from the consequences of stress. However, our results suggest that socialization of coping has implications for psychopathology under conditions of mild stress as well, and parents may need to adjust their coping suggestions when youth are dealing with mild stressors. Helping parents and youth understand ways in which different coping strategies are appropriate for different situations is a key task for coping interventions.
Limitations and Future Directions
A few limitations of the current study should be noted. First, our investigation of parent socialization of coping relied on reports of maternal caregivers only. Fathers also likely serve as a critical resource for youth during times of stress. Fathers and mothers might vary in the content or tone of their coping suggestions, or boys and girls might respond differently to suggestions offered by fathers versus mothers; these patterns have been observed in studies of emotion socialization (e.g., Cassano et al. 2007; Klimes-Dougan et al. 2007). Thus, elucidating fathers’ socialization role is important. Moreover, obtaining youth reports of socialization of coping would provide insight into how youth receive or interpret parents’ messages. For example, it is possible that youths’ perceptions of parent coping suggestions vary as a function of the parents’ ability to effectively communicate socialization messages, the quality of the parent–child relationship, or characteristics of youth (e.g., temperament, cognitive style).
Mothers reported on general rather than context-specific coping suggestions. As a result, we cannot conclude that parent suggestions were made in direct response to particular stressors, only that those suggestions were offered to youth in the context of a certain type and amount of stress. Given that socialization of coping differentially predicted youth psychopathology across varying stressful contexts, future investigations would benefit from separately assessing parent coping suggestions in response to specific interpersonal and noninterpersonal stressors.
This study yielded evidence that parent socialization of coping contributes to youth psychopathology; however, it is also possible that youths’ characteristics elicit particular types of coping suggestions from parents. Parents may tailor their suggestions based on youths’ temperamentally based emotional reactivity; for example, parents may be more likely to encourage disengagement coping for youth who experience extreme negative affect in response to stress, and engagement coping for youth who are less reactive to stress. Furthermore, reciprocal associations may exist over time between parent socialization of coping and youth psychopathology. For example, parents may believe that youth with heightened symptoms are less capable of engaging with stress and consequently encourage disengagement, which could in turn exacerbate youths’ symptoms. Future research that simultaneously examines both predictors and outcomes of socialization of coping will shed light on these possibilities.
Finally, an important next step for this area of research is to examine potential mechanisms that account for the associations between socialization of coping and youth psychopathology. Given that youths’ coping is the immediate target of parent socialization in this context, additional research is needed to examine whether coping suggestions protect or exacerbate risk for psychopathology by shaping youths’ coping behavior. This process may operate in multiple ways. As discussed above, youth may vary in the extent to which they follow parents’ suggestions for coping with stress. Youth also may vary in the skill with which they enact parents’ suggestions. Other potential mediators include youths’ coping efficacy and self-esteem. Disengagement suggestions, for example, may communicate to youth that they are incapable of facing stressors directly, undermining their feelings of self-efficacy in stressful contexts and increasing risk for depression. Future work examining these potential mechanisms will inform prevention and intervention efforts that seek to reduce risk for youth psychopathology by targeting parent socialization.
Conclusion
Despite well-supported contributions of parenting practices and stress to youth psychopathology, little is known about the prospective influence of parent socialization of coping. The present research suggests that providing youth with coping resources in times of stress may reduce or amplify subsequent risk for depression and externalizing psychopathology. Furthermore, the impact of coping resources provided by parents varies as a function of both sex and the type and amount of stress encountered by youth. These findings highlight a need for researchers to continue to investigate parent support of youth coping behavior, as well as potential contextual moderators of parenting effects on youth adjustment.
Notes
Reasons for nonparticipation included being busy or not interested (n = 229), having moved or being unreachable (n = 40), chronic rescheduling (n = 5), and failing to meet eligibility criteria (n = 27).
Regression analyses also were conducted controlling for age in the first step. However, the results were nearly identical to those regressions excluding age. Thus, the results excluding age were retained.
References
Achenbach, T. M. (1991). Integrative guide for the 1991 CBCL/4–18, YSR, and TRF profiles. Burlington: University of Vermont, Department of Psychiatry.
Achenbach, T. M., Becker, A., Dopfner, M., Heiervang, E., Roessner, V., Steinbausen, H., et al. (2008). Multicultural assessment of child and adolescent psychopathology with ASEBA and SDQ instruments: research findings, applications, and future directions. Journal of Child Psychology and Psychiatry, 49, 251–275.
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing and interpreting interactions. Newbury Park: Sage.
American Psychiatric Association. (2000). (DSM-IV-TR) Diagnostic and statistical manual of mental disorders, text revision (4th ed.). Washington: American Psychiatric Press, Inc.
Arbuckle, J. L. (2006). AMOS 7.0 [Computer Software]. Chicago: Small Waters Corp.
Beyers, J. M., Bates, J. E., Pettit, G. S., & Dodge, K. A. (2003). Development of youths’ externalizing behaviors: a multilevel analysis. American Journal of Community Psychology, 31, 35–53.
Brennan, P. A., Le Brocque, R., & Hammen, C. (2003). Maternal depression, parent–child relationships, and resilient outcomes in adolescence. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 1469–1477.
Brody, G. H., Ge, X., Kim, S. Y., Murry, V. M., Simons, R. L., Gibbons, F. X., et al. (2003). Neighborhood disadvantage moderates associations of parenting and older sibling problem attitudes and behavior with conduct disorders. Journal of Consulting and Clinical Psychology, 71, 211–222.
Brown, G. W., & Harris, T. O. (1978). Social origins of depression: A study of psychiatric disorder in women. New York: Free Press.
Cassano, M., Perry-Parrish, C., & Zeman, J. (2007). Influence of gender on parental socialization of children’s sadness regulation. Social Development, 16, 210–231.
Chung, T., & Asher, S. R. (1996). Children’s goals and strategies in peer conflict situations. Merrill-Palmer Quarterly, 42, 125–147.
Cole, P. M., & Zahn-Waxler, C. (1992). Emotional dysregulation in disruptive behavior disorders. In D. Cicchetti & S. L. Toth (Eds.), Developmental perspectives on depression. Rochester symposium on developmental psychopathology (Vol. 4, pp. 172–209). Rochester: University of Rochester Press.
Compas, B. E., Connor-Smith, J. K., Saltzman, H., Thomsen, A. H., & Wadsworth, M. E. (2001). Coping with stress during childhood and adolescence: problems, progress, and potential in theory and research. Psychological Bulletin, 127, 87–127.
Connor-Smith, J. K., Compas, B. E., Wadsworth, M. E., Thomsen, A. H., & Saltzman, H. (2000). Responses to stress in adolescence: measurement of coping and involuntary stress responses. Journal of Consulting and Clinical Psychology, 68, 976–992.
Davila, J., Hammen, C., Burge, D., Paley, B., & Daley, S. E. (1995). Poor interpersonal problem solving as a mechanism of stress generation in depression among adolescent women. Journal of Abnormal Psychology, 104, 592–600.
de Castro, B. O., Veerman, J. W., Koops, W., Bosch, J. D., & Monshouwer, H. J. (2002). Hostile attribution of intent and aggressive behavior: a meta-analysis. Child Development, 73, 916–934.
Dearing, E. (2004). The developmental implications of restrictive and supportive parenting across neighborhoods and ethnicities: exceptions are the rule. Applied Developmental Psychology, 25, 555–575.
Deater-Deckard, K., & Dodge, K. A. (1997). Externalizing behavior problems and discipline revisited: nonlinear effects and variation by culture, context, and gender. Psychological Inquiry, 8, 161–175.
Dodge, K. A., Pettit, G. S., Bates, J. E., & Valente, E. (1995). Social information processing patterns partially mediate the effect of early physical abuse on later conduct problems. Journal of Abnormal Psychology, 104, 632–643.
Durbin, E. C., & Shafir, D. M. (2007). Emotion regulation and risk for depression. In J. R. Z. Abela & B. L. Hankin (Eds.), Child and adolescent depression: Causes, treatment, and prevention (pp. 149–176). New York: Guilford.
Eisenberg, N., Losoya, S., Fabes, R. A., Guthrie, I. K., Reiser, M., Murphy, B., et al. (2001). Parental socialization of children’s dysregulated expression of emotion and externalizing problems. Journal of Family Psychology, 15, 183–205.
Eisenberg, N., Zhou, Q., Spinrad, T. L., Valiente, C., Fabes, R. A., & Liew, J. (2005). Relations among positive parenting, children’s effortful control, and externalizing problems: a three-wave longitudinal study. Child Development, 76, 1055–1071.
Fergusson, D. M., Horwood, L. J., Ridder, E. M., & Beautrais, A. L. (2005). Sub-threshold depression in adolescence and mental health outcomes in adulthood. Archives of General Psychiatry, 62, 66–72.
Flynn, M., & Rudolph, K. D. (2007). Perceptual asymmetry and youths’ responses to stress: understanding vulnerability to depression. Cognition and Emotion, 21, 773–788.
Garber, J., Braafladt, N., & Weiss, B. (1995). Affect regulation in depressed and nondepressed children and young adolescents. Development and Psychopathology, 7, 93–115.
Ge, X., Lorenz, F. O., Conger, R. D., Elder, G. H., Jr., & Simons, R. L. (1994). Trajectories of stressful life events and depressive symptoms during adolescence. Developmental Psychology, 30, 467–483.
Hammen, C. (2006). Stress generation in depression: reflections on origins, research, and future directions. Journal of Clinical Psychology, 62, 1065–1082.
Hammen, C., Shih, J., Altman, T., & Brennan, P. A. (2003). Interpersonal impairment and the prediction of depressive symptoms in adolescent children of depressed and nondepressed mothers. Journal of the American Academy of Child & Adolescent Psychiatry, 42(5), 571–577.
Hammen, C., Shih, J. H., & Brennan, P. A. (2004). Intergenerational transmission of depression: test of an interpersonal stress model in a community sample. Journal of Consulting and Clinical Psychology, 72(3), 511–522.
Hankin, B. L., Fraley, R. C., Lahey, B. B., & Waldman, I. D. (2005). Is depression best viewed as a continuum or discrete category? A taxometric analysis of childhood and adolescent depression in a population-based sample. Journal of Abnormal Psychology, 114, 96–110.
Hankin, B. L., Mermelstein, R., & Roesch, L. (2007). Sex differences in adolescent depression: stress exposure and reactivity models. Child Development, 78, 279–295.
Joiner, T. E., Coyne, J. C., & Blalock, J. (1999). On the interpersonal nature of depression: Overview and synthesis. In T. E. Joiner & J. C. Coyne (Eds.), The interactional nature of depression (pp. 3–19). Washington: American Psychological Association.
Jones, D. C., Abbey, B. B., & Cumberland, A. (1998). The development of display rule knowledge: linkages with family expressiveness and social competence. Child Development, 69, 1209–1222.
Kim, J. E., Hetherington, M., & Reiss, D. (1999). Associations among family relationships, antisocial peers, and adolescents’ externalizing behaviors: gender and family type differences. Child Development, 70, 1209–1230.
Kim, J. K., Conger, R. D., Elder, G. H., Jr., & Lorenz, F. O. (2003). Reciprocal influences between stressful life events and adolescent internalizing and externalizing problems. Child Development, 74, 127–143.
Klein, D. N., Ouimette, P. C., Kelly, H. F., Ferro, T., & Riso, L. P. (1994). Test–retest reliability of team consensus best-estimate diagnoses of Axis I and II disorders in a family study. American Journal of Psychiatry, 151, 1043–1047.
Klein, D. N., Lewinsohn, P. M., Rohde, P., Seeley, J. R., & Olino, T. M. (2005). Psychopathology in the adolescent and young adult offspring of a community sample of mothers and fathers with major depression. Psychological Medicine, 35, 353–365.
Kliewer, W., & Lewis, H. (1995). Family influences on coping processes in children and adolescents with sickle cell disease. Journal of Pediatric Psychology, 20, 511–525.
Kliewer, W., Fearnow, M. D., & Miller, P. A. (1996). Coping socialization in middle childhood: tests of maternal and paternal influences. Child Development, 67, 2339–2357.
Kliewer, W., Parish, K. A., Taylor, K. W., Jackson, K., Walker, J. M., & Shivy, V. A. (2006). Socialization of coping with community violence: influences of caregiver coaching, modeling, and family context. Child Development, 77, 605–623.
Klimes-Dougan, B., Brand, A. E., Zahn-Waxler, C., Usher, B., Hasting, P. D., Kendziora, K., et al. (2007). Parental emotion socialization in adolescence: differences in sex, age, and problem status. Social Development, 16, 326–342.
Kovacs, M. (1981). Rating scales to assess depression in school-aged children. Acta Paedopsychiatry, 46, 305–315.
Krackow, E. & Rudolph, K. D. (2008). Life stress and the accuracy of cognitive appraisals in depressed youth. Journal of Clinical Child and Adolescent Psychology, 37, 376–385.
Lahey, B. B., Van Rathouz, P. J., Hulle, C., Urbano, R. C., Krueger, R. F., Applegate, B., et al. (2008). Testing structural models of DSM-IV symptoms of common forms of child and adolescent psychopathology. Journal of Abnormal Child Psychology, 36, 187–206.
Lansford, J. E., Criss, M. M., Pettit, G. S., Dodge, K. A., & Bates, J. E. (2003). Friendship quality, peer group affiliation, and peer antisocial behavior as moderators of the link between negative parenting and adolescent externalizing behavior. Journal of Research on Adolescence, 13, 161–184.
Lansford, J. E., Deater-Deckard, K., Dodge, K. A., Bates, J. E., & Pettit, G. S. (2004). Ethnic differences in the link between physical discipline and later adolescent externalizing behaviors. Journal of Chlid Psychology and Psychiatry, 45, 801–812.
Lengua, L. (2006). Growth in temperament and parenting as predictors of adjustment during children’s transition to adolescence. Developmental Psychology, 42, 819–832.
Lengua, L. J., Wolchik, S. A., Sandler, I. N., & West, S. G. (2000). The additive and interactive effects of parenting and temperament in predicting adjustment problems of children of divorce. Journal of Clinical Chlid Psychology, 29, 232–244.
Little, S. A., & Garber, J. (2004). Interpersonal and achievement orientations and specific stressors predict depressive and aggressive sypmtoms. Journal of Adolescent Research, 19, 63–84.
Meyers, S. A., & Miller, C. (2004). Direct, mediated, moderated, and cumulative relations between neighborhood characteristics and adolescent outcomes. Adolescence, 39, 121–144.
Miller, P. A., Kliewer, W., Hepworth, J. T., & Sandler, I. N. (1994). Maternal socialization of children’s postdivorce coping: development of a measurement model. Journal of Applied Developmental Psychology, 15, 457–487.
Natsuaki, M. N., Ge, X., Brody, G. H., Simons, R. L., Gibbons, F. X., & Cutrona, C. E. (2007). African American children’s depressive symptoms: the prospective effects of neighborhood disorder, stressful life events, and parenting. American Journal of Community Psychology, 39, 163–176.
Orvaschel, H. (1995). Schedule for affective disorders and schizophrenia for school-age children-epidemiologic version-5. Nova Southeastern University.
Papadakis, A. A., Prince, R. P., Jones, N. P., & Strauman, T. J. (2006). Self-regulation, rumination, and vulnerability to depression in adolescent girls. Development and Psychopathology, 18, 815–829.
Park, I. J. K., Garber, J., Ciesla, J. A., & Ellis, B. J. (2008). Convergence among multiple methods of measuring positivity and negativity in the family environment: relation to depression in mothers and their children. Journal of Family Psychology, 22, 123–134.
Patterson, G. (2001). The early development of coercive family processes. In J. B. Reid, G. R. Patterson & J. Snyder (Eds.), Antisocial behavior in children and adolescents: A developmental analysis and model for intervention (pp. 25–44). Washington: American Psychological Association.
Patterson, G. R., DeBaryshe, B. D., & Ramsey, E. (1989). A developmental perspective on antisocial behavior. American Psychologist, 44, 329–335.
Pettit, G. S., Bates, J. E., & Dodge, K. A. (1997). Supportive parenting, ecological context, and children’s adjustment: a seven-year longitudinal study. Child Development, 68, 908–923.
Plybon, L. E., & Kliewer, W. (2001). Neighborhood types and externalizing behavior in urban school-age children: tests of direct, mediated, and moderated effects. Journal of Child and Family Studies, 10, 419–437.
Pomerantz, E. M., & Thompson, R. A. (2008). Parents’ role in children’s personality development: The psychological resource principle. In O. P. John, R. W. Robins & L. A. Pervin (Eds.), Handbook of personality: Theory and research (3rd ed., pp. 351–374). New York: Guilford Press.
Pomerantz, E. M., Wang, Q., & Ng, F. F. (2005). Mothers’ affect in the homework context: the importance of staying positive. Developmental Psychology, 42, 414–427.
Rose, A. J., & Asher, S. R. (1999). Children’s goals and strategies in response to conflicts within a friendship. Developmental Psychology, 35, 69–79.
Rose, A., & Rudolph, K. D. (2006). A review of sex differences in peer relationship processes: potential trade-offs for the emotional and behavioral development of girls and boys. Psychological Bulletin, 132, 98–131.
Rudolph, K. D. (2002). Gender differences in emotional responses to interpersonal stress during adolescence. Journal of Adolescent Health, 30, 3–13.
Rudolph, K. D. (2008). Developmental influences on interpersonal stress generation in depressed youth. Journal of Abnormal Psychology, 117, 673–679.
Rudolph, K. D., & Conley, M. (2005). The socioemotional costs and benefits of social-evaluative concerns: do girls care too much? Journal of Personality, 73, 115–137.
Rudolph, K. D., & Flynn, M. (2007). Childhood adversity and youth depression: influence of gender and pubertal status. Development and Psychopathology, 19, 497–521.
Rudolph, K. D., & Hammen, C. (1999). Age and gender as determinants of stress exposure, generation, and reactions in youngsters: a transactional perspective. Child Development, 70, 660–677.
Rudolph, K. D., Hammen, C., Burge, D., Lindberg, N., Herzberg, D. S., & Daley, S. E. (2000). Toward an interpersonal life-stress model of depression: the developmental context of stress generation. Development and Psychopathology, 12, 215–234.
Rudolph, K. D., Flynn, M., & Abaied, J. L. (2008). A developmental perspective on interpersonal theories of youth depression. In J. R. Z. Abela & B. L. Hankin (Eds.), Child and adolescent depression: Causes, treatment, and prevention (pp. 79–102). New York: Guilford.
Rudolph, K. D., Flynn, M., Abaied, J. L., Groot, A., & Thompson, R. J. (2009). Why is past depression the best predictor of future depression? Stress generation as a mechanism of depression continuity in girls. Journal of Clinical Child and Adolescent Psychology, 38, 473–485.
Rushton, J. P., Brainerd, C. J., & Pressley, M. (1983). Behavioral development and construct validity: the principle of aggregation. Psychological Bulletin, 94, 18–38.
Rydell, A., Berlin, L., & Bohlin, G. (2003). Emotionality, emotion regulation, and adaptation among 5- to 8-year-old children. Emotion, 3, 30–47.
Sandler, I. N., Tein, J., & West, S. G. (1994). Coping, stress, and the psychological symptoms of children of divorce: a cross-sectional and longitudinal study. Child Development, 65, 1744–1763.
Sandler, I. N., Tein, J., Mehta, P., Wolchik, S., & Ayers, T. (2000). Coping efficacy and psychological problems of children of divorce. Child Development, 71, 1099–1118.
Scaramella, L. V., Conger, R. D., & Simons, R. L. (1999). Parental protective influences and gender-specific increases in adolescent internalizing and externalizing problems. Journal of Research on Adolescence, 9, 111–144.
Schwartz, J. C., Barton-Henry, M. L., & Pruzinsky, T. (1985). Assessing child-rearing behaviors: a comparison of ratings made by mother, father, child, and sibling on the CRPBI. Child Development, 56, 462–479.
Sheeber, L., Allen, N., Davis, B., & Sorenson, E. (2000). Regulation of negative affect during mother–child problem-solving interactions: adolescent depressive status and family processes. Journal of Abnormal Child Psychology, 28, 467–479.
Sheeber, L., Hops, H., & Davis, B. (2001). Family processes in adolescent depression. Clinical Child and Family Psychology Review, 4, 19–35.
Sheeber, L., Davis, B., Leve, C., Hops, H., & Tildesly, E. (2007). Adolescents’ relationships with their mothers and fathers: associations with depressive disorder and subdiagnostic symptomatology. Journal of Abnormal Psychology, 116, 144–154.
Shek, D. T. L. (2002). Family functioning and psychological well-being, school adjustment, and problem behavior in Chinese adolescents with and without economic disadvantage. Journal of Genetic Psychology, 163, 497–502.
Silk, J. S., Steinberg, L., & Morris, A. S. (2003). Adolescents’ emotion regulation in daily life: links to depressive symptoms and problem behavior. Child Development, 74, 1869–1880.
Spinrad, T., Eisenberg, N., Cumberland, A., Fabes, R. A., Valiente, C., Shepard, S. A., et al. (2006). Relation of emotion-related regulation to children’s social competence: a longitudinal study. Emotion, 6, 498–510.
Treynor, W., Gonzalez, R., & Nolen-Hoeksema, S. (2003). Rumination reconsidered: a psychometric analysis. Cognitive Therapy and Research, 27, 247–259.
Wadsworth, M. E., & Berger, L. E. (2006). Adolescents coping with poverty-related family stress: prospective predictors of coping and psychological symptoms. Journal of Youth and Adolescence, 35, 57–70.
Wadsworth, M. E., & Compas, B. E. (2002). Coping with family conflict and economic strain: the adolescent perspective. Journal of Research on Adolescence, 12, 243–274.
Wadsworth, M. E., Raviv, M. A., Compas, B. E., & Connor-Smith, J. K. (2005). Parent and adolescent responses to poverty-related stress: tests of mediated and moderated coping models. Journal of Child and Family Studies, 14, 283–298.
Walsh, A. (1992). Genetic and environmental explanations of juvenile violence in advantaged and disadvantaged environments. Aggressive Behavior, 18, 187–199.
Zeman, J., Shipman, K., & Suveg, C. (2002). Anger and sadness regulation: predictions to internalizing and externalizing symptoms in children. Journal of Clinical Child and Adolescent Psychology, 31, 393–398.
Zimmer-Gembeck, M. J., & Locke, E. M. (2007). The socialization of adolescent coping behaviours: relationships with families and teachers. Journal of Adolescence, 30, 1–16.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Abaied, J.L., Rudolph, K.D. Mothers as a Resource in Times of Stress: Interactive Contributions of Socialization of Coping and Stress to Youth Psychopathology. J Abnorm Child Psychol 38, 273–289 (2010). https://doi.org/10.1007/s10802-009-9364-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-009-9364-7