
Abstract
Deficits in positive emotionality (PE) have been implicated in the etiology of both social anxiety and depression; however, factors that contribute to divergent social anxiety and depression outcomes among youth low in PE remain unknown. Extant research suggests that parent-child stress and peer stress demonstrate differential patterns of associations with social anxiety and depression. Thus, the present study examined prospective interactive effects of PE and chronic parent-child and peer stress on simultaneously developing trajectories of social anxiety and depression symptoms among 543 boys and girls (age 8–16 at baseline, M[SD] = 11.94[2.32] 55.6% female). Parents reported on youth PE at baseline. Domains of chronic interpersonal (parent-child and peer) stress occurring between baseline and 18-months were assessed via child-report by trained interviews using the Youth Life Stress Interview (Rudolph and Flynn Development and Psychopathology, 19(2), 497–521, 2007). Youth completed self-report measures of depression and social anxiety every three months from 18- to 36- months (7 assessments). Conditional bivariate latent growth curve models indicated that main effects of parent-child stress, but not peer stress, predicted trajectories of depression in boys and girls. In girls, high levels of chronic interpersonal stress in both domains predicted stable, elevated trajectories of social anxiety symptoms regardless of PE. In boys, PE contributed to a pattern of differential susceptibility whereby boys high in PE were particularly susceptible to the effects of chronic interpersonal stress, for better or worse.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Social anxiety and depression symptoms increase across the transition from middle childhood through late adolescence (Beesdo et al. 2009; Hankin 2015; Saluja et al. 2004; Van Oort et al. 2009) and commonly co-occur during this developmental period (Brady and Kendall 1992; Chavira et al. 2004; Hamilton et al. 2016). The experiences of social anxiety and depression during childhood and adolescence are each associated with concurrent distress and impairment (Avenevoli et al. 2015) and predict life-course persistent sequelae, including risk for poor health, educational underachievement, poor interpersonal functioning, and ongoing mental health difficulties (e.g., Bittner et al. 2007; Fergusson and Woodward 2002). Social anxiety and depression are characterized by shared deficits in positive emotionality (PE), in contrast to other domains of internalizing psychopathology (e.g., Forbes et al. 2010; Kashdan 2007; Naragon-Gainey et al. 2009; see Epkins and Heckler 2011 for review). However, not all youth low in PE experience social anxiety or depression. Factors contributing to divergent social anxiety and depressive trajectories among youth low in PE have not yet been clarified, although identifying such factors may be critical to elucidating the etiological pathways by which social anxiety and depression emerge. One factor that may contribute to diverging outcomes among low PE youth involves exposure to different types of chronic stress.
Vulnerability-stress models of psychopathology posit that relatively stable individual differences, such as individual differences in temperamental PE, interact with stressful experiences to confer risk for the development of psychopathology (see Hankin and Abela 2005). A wealth of research supports prospective relations between chronic interpersonal stress and elevated levels of psychopathologies, including social anxiety and depression among youth (see Choukas-Bradley and Prinstein 2014; Epkins and Heckler 2011; Grant et al. 2004 for reviews). Notably, the developmental trajectories of social anxiety and depression are not isomorphic, indicating a role for both shared and relatively specific factors in their etiological pathways (Cummings et al. 2014), consistent with the principle of multifinality (Cicchetti and Rogosch 1996). Shared temperamental vulnerability may interact with different, relatively specific domains of chronic interpersonal stress to contribute to divergent outcomes. Indeed, in their review of the literature, Epkins and Heckler (2011) found evidence for differential patterns of associations between stressful experiences in the peer and parent-child domains and social anxiety and depressive outcomes, such that peer stress was more strongly related to social anxiety and parent-child stress was more strongly related to depression.
The literatures examining parent-child and peer stress as they relate to social anxiety and depression have largely developed independently of one another. Prospective associations between these distinct domains of interpersonal stress and social anxiety and depressive outcomes have not been examined simultaneously in a single sample of children and adolescents. Thus, the present study aimed to investigate the ways in which PE interacts with chronic parent-child stress and chronic peer stress to differentially predict the developmental trajectories of social anxiety and depressive symptoms. Such research can improve understanding of which youth experience social anxiety and depression symptoms, and why.
PE: Associations with Depression and Social Anxiety
Temperament reflects individual differences in reactivity and self-regulation that are hypothesized to be evident early in life and show relative consistency across time and contexts (Rothbart and Bates 2006). The temperament factor of positive emotionality (PE), roughly analogous to the personality factor of extroversion in adults (Shiner and Caspi 2003), captures dispositional attributes including sociability, approach motivation, and the tendency toward experiencing positive affect (Putnam 2012). Low PE is particularly interesting as temperamental susceptibility to psychopathology because this dimension demonstrates relatively specific associations with symptoms of depression and social anxiety (Kotov et al. 2007; Watson et al. 2005; see Watson and Naragon-Gainey 2010 for review), in contrast to other individual differences in temperament (e.g., negative emotionality, low effortful control) that relate transdiagnostically to multiple psychopathologies (Hankin et al. 2017; Ormel et al. 2013; Snyder et al. 2015). Indeed, low PE demonstrates strong associations with the criterial symptoms of depression (Watson and Naragon-Gainey 2010) and is emphasized as an important clinical feature in contemporary models of social anxiety (Morrison and Heimberg 2013, Naragon-Gainey and Watson 2011).
Prospective studies indicate that low temperamental PE predicts the development of depression and social anxiety in childhood and adolescence (Compas et al. 2004; Dougherty et al. 2010; Kendall et al. 2015; Wetter and Hankin 2009). In a sample of young children, Dougherty et al. (2010) found that low PE, assessed at age 3, prospectively predicted increases in children’s mean-level depressive symptoms at age 10. Among a sample of 6th to 10th grade students, Wetter and Hankin (2009) similarly found that self-reported PE prospectively predicted increases in mean-level depressive symptoms across a 5-month follow-up period. Relatively less work has specifically examined prospective relations between PE and social anxiety. Kendall et al. (2015) found that low PE prospectively predicted first onsets of depression and social anxiety disorder diagnoses over a 6-year follow-up period among a sample of older adolescents. Such evidence suggests that PE confers prospective risk for both social anxiety and depression; however, given that not all low PE youth develop symptoms of social anxiety or depression, research is needed to clarify under which conditions PE confers risk for these forms of internalizing psychopathology and elucidate relatively specific relations between specific domains of interpersonal chronic stress and later social anxiety and depressive outcomes.
Chronic Parent-Child and Peer Stress: Evidence for Differential Patterns of Associations
Exposure to interpersonal stress is a well-established risk factor for the development of depression and social anxiety among youth (Choukas-Bradley and Prinstein 2014; Epkins and Heckler 2011; Grant et al. 2004; Hamilton et al. 2016). Indeed, aversive experiences with parents (e.g., parental conflict, low parental support) and peers (e.g., peer rejection, low peer support) demonstrate both concurrent and prospective associations with youths’ symptoms of depression and social anxiety (see Choukas-Bradley and Prinstein 2014; Epkins and Heckler 2011; Yap et al. 2014 in review). Interpersonal theories of child and adolescent depression propose that early disturbances in familial relationships contribute to youth risk for depression, in part, by disrupting normative patterns of socioemotional learning, contributing to suboptimal relationship qualities with parents and peers, and reinforcing risk for psychopathology (Rudolph et al. 2008). These models emphasize both parent-child and peer- related stressors in the etiology of depression; however, these models frequently fail to account for co-occurring symptoms of social anxiety, despite high rates of depression-social anxiety co-occurrence (Brady and Kendall 1992; Chavira et al. 2004; Hamilton et al. 2016; Ranta et al. 2009). It is possible, therefore, that interpersonal stress in parent-child and peer domains may contribute to disparate patterns of outcomes. Indeed, recent work suggests that aversive peer experiences contribute to negative self-perceptions and dysfunctional cognitions that are specific to the social domain, whereas aversive familial experiences are related more broadly to individual differences in cognitive style associated with vulnerability to depression (Cole et al. 2016). This suggests that disturbances in familial relationships, which constitute a highly salient and relatively stable context for adolescent development, may inculcate youth with an array of negative beliefs concerning their selves, their future, and their worlds, consistent with depression, whereas disruptions in peer relationships may more narrowly influence youths’ beliefs regarding their own social competence and risk for interpersonal victimization and alienation, consistent with social anxiety.
Consistent with this conceptual model, extant literature suggests that parent-child stress may be more strongly related to depression relative to social anxiety, and peer stress may be more strongly related to social anxiety relative to depression (Epkins and Heckler 2011). Support for the relative specificity of effects of parent-child and peer stress on depressive and social anxiety outcomes, respectively, has emerged across a number of studies. Among a sample of preadolescent girls aged 9 to 12, Hutcherson and Epkins (2009) found that parental acceptance/rejection was more strongly related to youths’ depression than social anxiety, and peer acceptance was more strongly related to youths’ social anxiety than depression. Similarly, in a sample of 10- to 12-year-olds, Scanlon and Epkins (2015) found that parental acceptance/rejection and behavioral control were unrelated to youth social anxiety after controlling for comorbid depression; in contrast, parental acceptance/rejection continued to predict youth depression after controlling for comorbid social anxiety. Moreover, in a cross-sectional study of early adolescent girls, Starr and Davila (2008) found that after controlling for social anxiety, depression was more strongly related to parent-related variables, including parent-child chronic stress, whereas, after controlling for depression, social anxiety was more strongly associated with peer-related variables.
Taken together, this body of literature suggests that stress in the parent-child and peer domains may be associated with distinct risk profiles for the development of psychopathology in adolescence. Importantly, however, extant research examining specificity of effects has been predominantly cross-sectional in nature and has focused largely on the effects of acute or episodic stressors (i.e., discrete life events). The ways in which chronic parent-child- and peer stress (i.e., ongoing and enduring life difficulties) may prospectively confer relatively specific risk for depressive and social anxiety outcomes has not been examined. Relative to the consequences of acute or episodic stressors, the psychosocial sequelae of chronic stress experienced during adolescence have been less rigorously studied, although exposure to chronic stress is posited to be influential in the development of psychopathology across the lifespan (Epel et al. 2018; Hammen 2005; Hammen et al. 2009; Vrshek-Schallhorn et al. 2015).
Critically, the ways in which chronic parent-child and peer stress interact with dispositional vulnerability factors, such as temperamental PE, to prospectively predict risk for social anxiety and depression remain understudied. Recent work by Sewart et al. (2019) demonstrated interactive effects of chronic interpersonal stress and dispositional positive affect (PA) assessed using the Mood and Anxiety Symptom Questionnaire (MASQ; Watson and Clark 1991) on prospective social anxiety and depression symptoms in a sample of late adolescents. Their findings provide important preliminary evidence that aspects of youth PE may interact with chronic interpersonal stress to predict mean-level social anxiety and depressive outcomes. However, researchers collapsed across domains of chronic interpersonal stress in their analyses, preventing nuanced insight into the ways in which specific domains of interpersonal stress may confer relatively specific risk for social anxiety versus depression. Additionally, dispositional PA was assessed using the MASQ, which is conceptually distinct from PE. PE is roughly analogous to extroversion (Shiner and Caspi 2003), and encapsulates such cognitive and behavioral tendencies as approach motivation, novelty seeking, and sociability (Putnam 2012), whereas PA as assessed using the MASQ aligns with the experience of anhedonia. Finally, Sewart et al. (2019) examined the interactive effects of PA and chronic interpersonal stress on the amount of change in mean-level depression and social anxiety outcomes. This approach is unable to investigate effects of PE and chronic interpersonal stress on trajectories of depression and social anxiety symptoms to better understand the course or development of symptoms over time. Thus, research is needed to disambiguate relatively unique patterns of relations between distinct parent-child and peer domains of chronic interpersonal stress, youth PE, and developmental trajectories of social anxiety and depression across childhood and adolescence in boys and girls.
The Present Study
The present study aimed to examine interactive effects of youth PE and exposure to chronic stress in parent-child and peer domains on trajectories of social anxiety and depressive symptoms, informed by a vulnerability-stress model of psychopathology, among a moderately large sample of children and adolescents. Specifically, latent growth curve modeling (LGCM) was used to investigate effects of parent-child and peer stress, as measured using gold-standard contextual stress interview methods (i.e., the Youth Life Stress Interview [YLSI]; Rudolph and Flynn 2007), youth temperamental PE, and their interaction on symptom trajectories across an 18-month follow-up period. In contrast to self-report questionnaire or checklist measures of stress, contextual stress interview measures provide a rigorous and relatively objective index of youths’ experience of chronic stress, allowing for a particularly strong test of study hypotheses (Harkness and Monroe 2016). Additionally, a focus on developmental trajectories rather than mean-level outcomes lends nuance and precision, facilitating analyses of interactive effects of PE and chronic parent-child and peer stress on both initial symptoms levels and patterns of symptom change over time. Given that adolescence is a developmental period characterized by increasing rates of social anxiety and depression (Burstein et al. 2011; Costello et al. 2003; Merikangas et al. 2010), identifying factors that contribute to individual differences in these developmental symptom trajectories may be particularly important for circumventing risk and interrupting patterns of symptom escalation.
The present study additionally aimed to evaluate gender differences in patterns of interactive relations between PE and chronic interpersonal stress. Interpersonal theories of youth depression emphasize that disturbances in interpersonal functioning may be especially salient for the development of psychopathology among girls relative to boys due to girls’ relatively greater social orientation and investment in interpersonal relationships (Cyranowski et al. 2000; Rose and Rudolph 2006; Rudolph et al. 2008). Existing evidence demonstrates that relative to boys, girls report higher levels of interpersonal stress exposure, and endorse greater reactivity to interpersonal stress with regard to depression symptom measures (e.g., Hankin et al. 2007; Rudolph 2002; Shih et al. 2006). Of note, this research has been largely focused on peer-related interpersonal stress or has failed to differentiate between peer- and parent-child- related stress, and gender differences in youth reactivity to parent-child stress, specifically, are less clear. Based on previous theory and research, however, it is plausible that trait vulnerability to psychopathology may be particularly amplified in the context of chronic interpersonal stress among girls relative to boys. Thus, multiple group analyses were conducted to evaluate potential gender differences in models of symptom change.
We hypothesized that PE would interact with chronic parent-child stress to predict the trajectory of depressive symptoms. We additionally hypothesized that PE would interact with chronic peer stress to predict the trajectory of social anxiety. Further, we hypothesized that observed patterns of associations would differ between boys and girls. Specifically, given evidence for enhanced sensitivity to social feedback among adolescent girls relative to adolescent boys (e.g., Cyranowski et al. 2000; Hankin et al. 2007; Rudolph 2002), we expected that risk for psychopathology conferred by trait vulnerability (i.e., PE) would be particularly amplified in the context of interpersonal stress among girls relative to boys. Thus, relative to boys, we expected to observe stronger interaction effects between PE and domains of interpersonal stress in predicting trajectories of psychopathology in girls.
Methods
Participants and Procedures
Participants included 543 youth from the community recruited in 3rd (n = 168), 6th (n = 208), and 9th (n = 167) grade cohorts (age 8–16 at baseline, M = 11.94, SD = 2.32, 55.6% female) recruited from the greater Denver and central New Jersey areas in association with the Gene, Environment, and Mood (GEM) study (see Hankin et al. 2015). This grade cohort-based recruitment design was employed in order to characterize patterns of development as they unfold across the adolescent transition, from middle childhood through late adolescence (see Hankin et al. 2015). The range of participant ages represented in the present sample is generally consistent with other, nationally representative epidemiological studies examining psychopathology in youth (e.g., Merikangas et al. 2009). Inclusion criteria included English language fluency, absence of autism or psychotic disorder diagnosis, and IQ > 70 (i.e., lack of intellectual disability) as assessed via parent report. Sample demographics were approximately representative of the ethnic and racial characteristics of the United States population (70.7% Caucasian, 10.7% African American, 9.6% Asian/Pacific Islander, 5.0% Multi-racial, 4.0% other racial background; 10.5% Latinx). Further details regarding sampling procedures and participant characteristics are described elsewhere (Hankin et al. 2015).
All procedures were approved by the Institutional Review Boards at the University of Denver and Rutgers University. Informed consent was obtained from all participating parents, and assent was obtained from all child and adolescent participants at an initial baseline visit upon families’ enrollment in the study. Participants (youth and caregiver) completed a baseline assessment and were followed prospectively for three years. Parent report of youths’ PE was collected at baseline, and chronic parent-child and peer stress exposure experienced from baseline to the 18-month follow-up was assessed by trained interviewers via child-report. Youth self-reported symptoms of depression and social anxiety were assessed every 3 months between the 18- and 36- month assessments (7 total assessment points).
Measures
Positive Emotionality (PE)
Youth PE was assessed via parent-report at baseline using the high intensity pleasure subscale (9 items) of the Early Adolescent Temperament Questionnaire (EATQ-R; Ellis and Rothbart 2001). Participating parents were prompted to rate how true a series of statements were of their child on a 5-point Likert-type scale from 1 (almost always untrue of your child) to 5 (almost always true of your child). Items corresponding to the high intensity pleasure subscale include such statements as “Likes it when something exciting and different happens at school,” “Is energized by being in large crowds of people,” and “Thinks it would be exciting to move to a new city.” The EATQ-R high intensity pleasure subscale has been used in previous work as a measure of youth PE among samples ranging in age from 8 to19 (Creemers et al. 2010; Mezulis et al. 2011; Snyder et al. 2015). Internal reliability was acceptable in the present sample (α = 0.70).
Chronic Interpersonal Stress
Chronic parent-child and peer stress were assessed at the 18-month follow up assessment, to cover the degree of chronic stress exposure experienced from baseline to the 18-month time point, using the Youth Life Stress Interview (YLSI; Rudolph and Flynn 2007). The YSLI is semi-structured contextual stress interview designed to provide an objective measure of youths’ ongoing experience of stress. Previous work demonstrates strong interrater reliability in samples of children and adolescents, as well as concurrent and predictive validity; interpersonal domains of the YSLI, specifically, have been demonstrated to positively associate with both concurrent and prospective measures of psychopathology among youth (Conley and Rudolph 2009; Gershon et al. 2011; Rudolph and Flynn 2007). Interviewers asked youth standardized questions targeting aspects of parent-child and peer relationships (e.g., interpersonal closeness, communication and trust, conflict, etc.). Sample questions in the domain of parent-child relationships include: “Do you get along with your parent?,” “Do you argue or fight with your parent?,” and “Do you spend time with your parent?” Sample questions in the peer domain include: “Do you sometimes have trouble making friends?,” “How do you and your friends handle disagreements?,” “Do you have a crew or group of friends that you hang out with?”
Severity of chronic stress was rated via a consensus score assigned by a team of three or more masked raters. Severity scores ranged from 1 (little/no stress) to 5 (severe stress) and were based on behaviorally-specific anchors regarding such aspects of interpersonal relationships as interpersonal closeness, communication, and conflict. For example, in the domain of peer stress, an adolescent would receive a score of 1 if they reported having many close friends, being well-liked by others, engaging in social interactions outside of school frequently, and experiencing no peer conflict. An adolescent would receive a score of 5 if they reported having no friends, experiencing complete isolation or rejection from peers, and/or engaging in frequent peer conflicts. The scoring manual additionally instructs coders to take into account the age and developmental context of each participant when making their objective rating. Chronic stress ratings are adjusted based on normative development, and what would constitute average to severe stress for youth of different ages.
Depressive Symptoms
Youth depressive symptoms were assessed via youth self-report using the Children’s Depression Inventory (CDI; Kovacs 1985), a 27-item measure of depressive symptoms. The CDI shows good reliability and validity (Klein et al. 2005). It was administered at baseline and at each 3-month assessment; for our LGCM analyses, CDI data from 18- to 36- month follow up assessments were analyzed (7 assessment points). The CDI demonstrated good internal consistency across assessment points in the present sample (α’s > 0.78).
Social Anxiety Symptoms
Youth social anxiety symptoms were assessed via self-report using the Multidimensional Anxiety Scale for Children (MASC; March et al. 1997). The 9-item social anxiety subscale of the MASC demonstrates strong psychometric properties, including good reliability and discriminant validity (March et al. 1997; Wei et al. 2014). The MASC was administered at baseline and at each 3-month follow up assessment; for LGCM analyses, MASC data from the 18- to 36- month follow up assessments were included (7 assessment points). Internal consistency of this subscale was good across all assessment points (α’s > 0.80).
Data Analytic Plan
Hypotheses and data analytic plan were preregistered (https://osf.io/xd32v/). Analyses were conducted using structural equation modeling (SEM) implemented in the lavaan library in R (Rosseel 2012; R Core Team 2018) using full-information maximum likelihood (FIML) estimation to address missing data. All data were missing completely at random (MCAR) or assumed to be missing at random (MAR) as missingness was not consistently correlated with scores on the CDI or the social anxiety subscale of the MASC across all time points. As is it not possible to test whether data are truly MAR, MAR is an assumption when using FIML (Schafer and Graham 2002). Goodness of fit was assessed using convergence across multiple fit indices, including Root Mean Square Error of Approximation (RMSEA), Standardized Root Mean Square Residual (SRMR), and Comparative Fit Index (CFI), consistent with recommendations proposed by Hu and Bentler (1999). Specifically, good fit was indicated by RMSEA < 0.06, SRMR < 0.08, and CFI > 0.95 (Hu and Bentler 1999). Acceptable fit was indicated by RMSEA < 0.08 and CFI > 0.90. We prioritized convergence across indices over reliance on any one particular measure of fit (Barrett 2007; Kenny 2015). To compare non-nested models, we used Akaike Information Criteria (AIC) and Bayesian Information Criteria (BIC) to determine the best fitting model, with lower values indicating better fit.
We first fit a series of univariate growth models to characterize depression and social anxiety symptom trajectories (no-growth, linear, or quadratic) over the 18-month follow-up. After determining best fitting models representing trajectories of depressive and social anxiety symptoms, we tested main study hypotheses using structural equation models. To determine whether parent-reported PE interacted with particular chronic stress domains to predict trajectories of social anxiety and depressive symptoms, we regressed best-fitting growth factors for each symptom domain on youth PE, chronic parent-child stress, and their interaction in a single model in which growth factors were allowed to covary across domains. By simultaneously modeling the trajectories of social anxiety and depressive symptoms in a single model, we accounted for the co-occurrence of social anxiety and depressive symptoms, so that results represent variance unique to each respective symptom domain. PE and chronic interpersonal stress variables were mean centered prior to calculating the interaction term. Residuals were allowed to covary within time point to account for correlated errors associated with common method variance within measurement occasion. Figure 1 visually represents the basic conceptual model. Separate models were conducted for parent-child and peer chronic stress.

Conceptual model describing prospective associations between positive emotionality (PE), chronic parent-child and peer stress, and trajectories of social anxiety and depressive symptoms. Chronic parent-child- and chronic peer stress scores capture stress occurring between the baseline- and 18-month assessments. Concurrent CDI and SA scores were allowed to covary to account for correlated errors within timepoint; these paths are not pictured for ease of interpretation. CDI = depressive symptoms assessed using the Children’s Depression Inventory; SA = social anxiety symptoms assessed using the Multidimensional Anxiety Scale for Children
Multiple Group Models
Multiple group models were conducted to examine whether patterns of observed associations differed between genders. Models in which all associations were constrained to be equal across groups (constrained model) were compared to analogous models in which all associations were free to vary (unconstrained model). Models were compared using chi-square difference tests, change in CFI, and AIC and BIC indices. Additional sensitivity analyses were conducted for each model controlling for grade cohort to account for potential age effects, as well as controlling for baseline symptoms of social anxiety and depression. Full results from these models are reported in Supplementary Materials.
Results
Preliminary Analyses
Table 1 provides descriptive statistics for primary variables overall, and by gender. Compared to boys, girls experienced greater chronic parent-child stress, and reported higher levels of social anxiety symptoms and more depressive symptoms than boys at most time points.
Table 2 shows bivariate correlations among variables. As expected, symptoms of social anxiety and depression were positively associated across all times (r’s = 0.41–0.53). Chronic parent-child and peer stress were moderately correlated (r = 0.37), and both domains of chronic interpersonal stress were positively associated with symptoms of social anxiety and depression across timepoints (r’s = 0.18–0.37).
Growth Models
For symptoms of depression, a quadratic growth model was retained as the best-fitting (Table S1). On average, trajectories were characterized by a significant intercept (b = 4.99), negative linear (b = −1.02) and positive quadratic slope (b = 0.17) (see Table S2). For social anxiety, a quadratic growth model demonstrated best fit (Table S1). Growth in social anxiety was characterized by a significant intercept (b = 7.69), positive linear (b = 0.33) and negative quadratic slope (b = −0.06) (Table S2). All growth parameters demonstrated significant variance.
The bivariate LGCM in which parameter estimates were free to vary across boys and girls demonstrated good fit to the data (CFI = 0.96, RMSEA = 0.07, SRMR = 0.07) and fit significantly better than a model with parameters constrained to be equal across gender (Δχ2(14) = 46.24, p < 0.001).Footnote 1 Table S4 presents growth parameters separately for boys and girls. The intercepts of depression and social anxiety were positively associated in both boys and girls (β = 0.34 and β = 0.62, respectively); youth who reported elevated starting levels of depression exhibited elevated starting levels of social anxiety. In girls, slope terms describing trajectories of depression and anxiety symptoms were positively related (β = 0.42 and β = 0.45, for linear-linear and quadratic-quadric slopes, respectively). For boys these cross-domain growth parameters were of similar magnitude.
PE and Chronic Parent-Child Stress
We fit multiple group models in which PE, chronic parent-child stress, and their interaction were entered as predictors of depression and social anxiety intercepts and slopes. A model with parameter estimates free to vary across boys and girls demonstrated good fit (CFI = 0.95, RMSEA = 0.07, SRMR = 0.06) and fit significantly better than a model with parameters constrained to be equal across gender (Δχ2(32) = 77.99, p < 0.001). Thus, results are reported separately for boys and girls (Table 3). Patterns of results were generally retained after controlling for grade cohort (see Table S5), as well as after controlling for baseline symptoms (see Table S6).Footnote 2
Boys
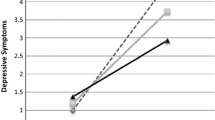
Main effects of chronic parent-child stress (b = 2.24) and PE (b = −0.10) were significantly associated with the depression intercept. Boys experiencing high levels of chronic parent-child stress in the preceding 18 months and boys low in PE reported higher starting levels of depression symptoms. Main effects of chronic parent-child stress were associated with linear (b = −0.45) and quadratic (b = 0.08) slopes for depression; boys high in chronic parent-child stress reported greater quadratic growth in depression symptoms relative to boys low in chronic parent-child stress (Fig. 2a). Main effects of PE were not associated with depression slope, and PE did not interact with chronic parent-child stress to predict depression trajectories.

a–b Projected growth in symptoms of depression in boys and girls at high (+1 SD) and low (−1 SD) levels of parent-child (P-C) stress
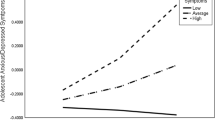
Main effects of chronic parent-child stress were associated with the social anxiety intercept (b = 1.39). Boys experiencing high chronic parent-child stress started higher in social anxiety symptoms. PE interacted with chronic parent-child stress to predict linear (b = 0.11) and quadratic (b = −0.02) slopes for social anxiety. Figure 3a shows post-hoc analyses indicating that at high levels (+1 SD) of chronic parent-child stress, boys high in PE (+1 SD) demonstrated greater initial increases with subsequent curvilinear declines in social anxiety (bi = 7.45, p < 0.001, bl = 1.15, p = 0.001, bq = −0.21, p < 0.001) whereas boys low in PE (-1SD) demonstrated consistently elevated symptoms that did not change over time (bi = 7.71, p < 0.001, bl = 0.10, p = 0.762, bq = −0.03, p = 0.573). At low chronic parent-child stress (−1 SD), boys high in PE (+1 SD) demonstrated consistently low social anxiety levels that did not change (bi = 4.75, p < 0.001, bl = −0.18, p = 0.559, bq = 0.03, p = 0.573), whereas boys low in PE (-1SD) demonstrated initial increases, and then subsequent quadratic declines, in social anxiety over time (bi = 6.30, p < 0.001, bl = 0.79, p = 0.015, bq = −0.15, p = 0.004).

a–d Projected growth in symptoms of social anxiety in boys and girls at high (+1 SD) and low (−1 SD) levels of positive emotionality (PE) and domains of chronic interpersonal stress
Girls
Main effects of chronic parent-child stress were associated with intercept (b = 2.47), linear (b = −0.67), and quadratic slopes (b = 0.12) of depression. Girls experiencing high chronic parent-child stress in the preceding 18 months reported higher starting depression and greater quadratic growth (Fig. 2b). PE was not associated with trajectories, and PE did not interact with chronic parent-child stress to predict trajectories of depression in girls.
Main effects of parent-child stress were associated with the social anxiety intercept (b = 1.75). Girls experiencing high parent-child chronic reported higher starting levels of social anxiety. PE interacted with parent-child stress to predict linear (b = −0.07) and quadratic (b = 0.01) slopes for social anxiety. Figure 3b illustrates post-hoc tests indicating that at high levels of parent-child stress (+1 SD), social anxiety symptoms were consistently elevated among girls at both high (+1 SD bi = 9.45, p < 0.001, bl = 0.02, p = 0.957, bq = −0.01, p = 0.863) and low levels of PE (−1 SD bi = 10.34, p < 0.001, bl = 0.15, p = 0.545, bq = −0.05, p = 0.263). At low parent-child stress (−1 SD), girls high in PE (+1 SD) demonstrated initial increases and subsequent quadratic declines in social anxiety (bi = 7.09, p < 0.001, bl = 0.93, p = 0.002, bq = −0.15, p = 0.002), whereas girls low in PE (−1 SD) demonstrated stable symptoms (bi = 7.58, p < 0.001, bl = −0.09, p = 0.751, bq = 0.01, p = 0.791).
PE and Chronic Peer Stress
Multiple group models were conducted with PE, chronic peer stress, and their interaction entered as predictors of depression and social anxiety intercepts and slopes. The model with parameters free to vary across genders demonstrated good fit (CFI = 0.95, RMSEA = 0.07, SRMR = 0.06) and fit significantly better than a model with parameters constrained to be equal (Δχ2(32) = 71.15, p < 0.001). Thus, results are reported separately for boys and girls (Table 4). Patterns of results were generally retained after controlling for grade cohort (see Table S7), as well as after controlling for baseline symptoms (see Table S8).
Boys
Main effects of chronic peer stress were associated with the depression intercept (b = 1.58). Boys experiencing high chronic peer stress in the preceding 18 months exhibited higher initial levels of depression. No main effects were observed for slopes, and PE did not interact with chronic peer stress to predict depression trajectories.
Main effects of chronic peer stress were associated with social anxiety intercept (b = 1.19). Boys experiencing high chronic peer stress reported higher initial levels of social anxiety. PE interacted with chronic peer stress to predict linear (b = 0.11) and quadratic (b = −0.02) slopes for social anxiety. Figure 3c shows post-hoc analyses indicating that at high levels (+1 SD) of peer stress, boys high in PE (+1 SD) demonstrated greater initial increases and subsequent quadratic declines in social anxiety across follow-up (bi = 6.94, p < 0.001, bl = 1.35, p < 0.001, bq = −0.22, p < 0.001), whereas boys low in PE (−1 SD) demonstrated elevated symptom levels that did not change (bi = 7.75, p < 0.001, bl = 0.36, p = 0.228, bq = −0.07, p = 0.126). At low chronic peer stress (−1 SD), boys high in PE (+1 SD) demonstrated low social anxiety that did not change (bi = 5.25, p < 0.001, bl = −0.23, p = 0.435, bq = 0.02, p = 0.395), whereas boys low in PE (−1 SD) demonstrated initial increases and subsequent quadratic declines in social anxiety over time (bi = 5.99, p < 0.001, bl = 0.73, p = 0.033, bq = −0.13, p = 0.015).
Girls
Main effects of chronic peer stress were associated with depression intercept (b = 2.18). Girls experiencing high levels of chronic peer stress in the preceding 18 months reported higher initial depression levels. No main effects of chronic peer stress or PE were observed for slopes, and PE did not interact with peer stress to predict depression trajectories.
PE interacted with chronic peer stress to predict intercept (b = 0.17) and linear slope term (b = −0.07) for social anxiety. No effects were observed for quadratic slope of social anxiety. Figure 3d illustrates post-hoc tests indicating that at high peer stress (+1 SD), social anxiety symptoms were consistently elevated among girls at both high (+1 SD bi = 10.06, p < 0.001, bl = 0.29, p = 0.335, bq = −0.05, p = 0.262) and low PE (−1 SD bi = 9.56, p < 0.001, bl = 0.40, p = 0.147, bq = −0.06, p = 0.173). At low chronic peer stress (−1 SD), girls high in PE (+1 SD) demonstrated low starting levels, initial increases, and subsequent curvilinear declines in social anxiety (bi = 6.10, p < 0.001, bl = 0.82, p = 0.011, bq = −0.13, p = 0.016), whereas girls low in PE (−1 SD) demonstrated stable social anxiety across follow-up (bi = 8.63, p < 0.001, bl = −0.26, p = 0.366, bq = 0.01, p = 0.819).
Discussion
Individual differences in temperamental PE have been implicated in the etiology of social anxiety and depression (Compas et al. 2004; Kendall et al. 2015); however, factors that interact with PE to differentially predict youth social anxiety versus depression trajectories have not been examined. The present study investigated interactions between youth PE and chronic parent-child and peer stress in predicting trajectories of social anxiety and depressive symptoms. Results show that chronic parent-child stress, but not chronic peer stress, predicted slopes of depression in boys and girls. Further, PE interacted with both domains of chronic interpersonal stress to predict trajectories of social anxiety in boys. In girls, trajectories of social anxiety were most meaningfully associated with chronic interpersonal stress, although small interaction effects between PE and chronic interpersonal stress were observed. Overall, findings suggest that chronic parent-child stress is relatively uniquely important in youth depression trajectories, chronic interpersonal stress in both parent-child and peer domains contribute to the maintenance of high levels of social anxiety in girls, and interactions between PE and chronic interpersonal stress influence progression of social anxiety in boys.
Boys and girls experiencing high chronic parent-child stress start higher and demonstrate more extreme change in depressive symptoms trajectories relative to youth experiencing low levels of enduring parent-child difficulties. Put another way, normative developmental trends of growth in depressive symptoms are amplified among youth experiencing elevated chronic parent-child stress. That chronic parent-child stress, but not chronic peer stress, predicted depression slopes in boys and girls is consistent with findings observed across parent-child- and peer stress- literatures (Epkins and Heckler 2011), as well as with a small body of cross-sectional work that examined the relative specificity of associations between parent- and peer- stressors and social anxiety and depression outcomes (Hutcherson and Epkins 2009; Scanlon and Epkins 2015; Starr and Davila 2008). Of note, main effects of both chronic parent-child and peer stress were observed on depression intercepts, suggesting that chronic peer stress contributes to mean-level differences in depressive symptoms, although it does not influence the rate of symptom growth. Exposure to enduring peer difficulties contributes to elevated depressive symptoms levels; however, exposure to chronically stressful parent-child relationships affects both elevated depressive symptoms levels and escalating patterns of symptom growth.
PE interacted with both chronic parent-child and chronic peer stress to predict social anxiety trajectories in boys. Decomposition of these interactions revealed patterns consistent with a differential susceptibility framework (Belsky and Pluess 2009), rather than a vulnerability-stress model. PE appeared to function as a “plasticity factor” in boys such that boys high in PE were particularly sensitive to both positive effects of low chronic interpersonal stress, as well as negative effects of high chronic interpersonal stress. Boys high in PE demonstrated consistently low and unchanging levels of social anxiety in interpersonal environments characterized by support and healthy communication. However, in interpersonal environments characterized by conflict and low social support, high PE boys endorsed high starting levels and initial increases in social anxiety. This pattern of differential effects may be driven by high PE boys’ desire to engage with their environments, for better or for worse. In the context of low chronic interpersonal stress, such high PE-approach tendencies may promote engagement coping and productive problem-solving. However, in the context of high chronic interpersonal stress, the high sociability and approach tendencies of elevated PE boys, which could involve their overutilizing or ineffectively implementing engagement coping, may result in increased social anxiety symptoms. This explanation is consistent with past work showing that boys who use engagement coping demonstrated prospective increases in externalizing symptoms when exposed to high levels of interpersonal stress (Abaied and Rudolph 2010).
In girls, chronic parent-child and peer stress contributed to social anxiety, as high exposure to chronic interpersonal stress related to consistently elevated symptom levels across the 18-month follow up period. Observed interaction effects between PE and domains of interpersonal stress were small in magnitude, and patterns of findings indicated that these interaction effects did not contribute to meaningful differences in symptom levels (see Fig. 3). Regardless of their levels of PE, girls experiencing high chronic interpersonal stress demonstrated high, unchanging levels of social anxiety across the 18-month follow-up period. Gender differences in patterns of findings are consistent with a rich body of research indicating that interpersonal factors may be more salient to adolescent girls relative to adolescent boys (e.g., Cyranowski et al. 2000; Hankin et al. 2007; Rudolph 2002), rendering adolescent girls vulnerable to internalizing psychopathology in the context of interpersonal stress, regardless of individual differences in PE.
Interestingly, PE did not buffer between chronic interpersonal stress and social anxiety or depressive symptoms. These findings contrast with Sewart et al.’ (2019) work suggesting PA protects against chronic interpersonal stress in predicting social anxiety and depression symptom severity. Differences in construct measurement and analytic approach may explain these divergent findings. Sewart assessed dispositional PA via the anhedonia scale of the MASQ; however, temperamental PE comprises cognitive and behavioral dimensions including approach motivation and sensation seeking, in addition to trait PA. Further, Sewart examined effects of PA and chronic interpersonal stress on mean-level change in social anxiety and depression severity, whereas we analyzed social anxiety and depression symptoms trajectories. The focus on symptom trajectories provides unique and novel insight into the ways in which PE and exposure to chronic interpersonal stress interact to prospectively contribute to patterns of growth in social anxiety and depression over time.
The present study demonstrated a number of strengths that advance knowledge of the etiology of adolescent social anxiety and depression. Chronic parent-child and peer stress were assessed using gold-standard contextual threat interviews, yielding reliable and unbiased measures of chronic stress exposure, consistent with best practice recommendations (Harkness and Monroe 2016). Additionally, data were included from multiple informants (i.e., parent report of youth PE, youth self-report of symptoms), minimizing reporter bias and providing a strong test of study hypotheses (Podsakoff et al. 2003). Further, youth symptoms were assessed every three months across an 18-month period, facilitating precise estimates of social anxiety and depressive symptom growth among a community sample of girls and boys. As the sample was recruited from the community, levels of depressive and social anxiety symptoms on average fell in the subclinical range. Importantly, however, youth with subclincal levels of depression and social anxiety also experience significant distress and impairment (Epkins and Heckler 2011), as both depression and social anxiety are dimensionally distributed at the latent level (Hankin et al. 2005; Liu 2016; Ruscio 2010). Further, subclinical syndromes are predictors of later disorder (Gerhardt et al. 1999). The present investigation of interactive effects of PE and domains of chronic interpersonal stress on trajectories of social anxiety and depressive symptoms represents a notable and novel addition to the extant literature, which has primarily focused on predicting mean levels of symptoms based on either parent-child or peer stress in isolation.
The study contains limitations that represent important areas for future research. The longitudinal, repeated-measures design facilitated social anxiety and depression symptom trajectories; research is needed to examine if effects replicate for disorder using diagnostic interview measures, given the distress and impairment associated with clinical levels of depression and anxiety (Avenevoli et al. 2015). Additionally, the contextual stress interview measures of stress included in the present study relied upon youth self-report, which may be biased in systematic ways; future research should aim to include multiple informants in the assessment of youth stress exposure and symptoms of psychopathology to strengthen confidence in findings. Moreover, the conceptual model informing the present analyses assumed relative stability in PE across time, consistent with leading contemporary models of temperament (e.g., Rothbart and Bates 2006). It is important to note, however, that temperament may be influenced by social and contextual factors, demonstrating bidirectional associations with social experiences and psychopathology (Atherton et al. 2017; Brown 2007); future work should aim to examine dynamic, reciprocal patterns of relations between PE, chronic stress, and psychopathology over time. Similarly, the present work was unable to account for the multitudinous host of factors that may influence levels of interpersonal stress, including family- and school- level dynamics, presence of other supportive relationships, and socioeconomic disadvantage. Likewise, it will be important to examine the bidirectional associations between parent-child and peer chronic stress. Future work should aim to address the ways in which these factors interact with youth PE to contribute to trajectories of psychopathology. Finally, given that patterns of differential susceptibility, although consistent with some previous research (see Abaied and Rudolph 2010), were unexpected a priori, the present findings should be replicated in independent samples to lend confidence in the pattern of observed effects. Findings should also be replicated in samples of youth of diverse social, ethnic, and cultural identities to evaluate the robustness of effects across a diversity of social and cultural groups.
Findings from the present study emphasize the role of interpersonal stress in contributing to psychopathology among both boys and girls, highlighting the salience of boys’ interpersonal sensitivity and social context in risk for psychopathology, in addition to girls’. Results of the present study suggest that interventions aimed at circumventing risk for internalizing psychopathology among child and adolescent youth would be well-served to prioritize targeting enduring patterns of interpersonal stress, and that targeting youths’ exposure to interpersonal stress may be more effective than capitalizing on endogenous tendencies toward high intensity pleasure in reducing risk for social anxiety and depressive psychopathologies. For those interventions aimed at reducing risk for depression, specifically, chronic stress in the parent-child domain may be an especially fruitful treatment target among both boys and girls. Findings further suggest that with regard to reducing risk for social anxiety, attention to interpersonal stress context may be especially warranted among boys high in PE-related tendencies toward approach and engagement, as these boys may be particularly sensitive to stress context, for better or for worse.
Notes
Complete model fit statistics for the constrained and unconstrained multiple bivariate growth models by gender are reported in Supplementary Table S3.
After accounting for baseline symptom levels, the effects of chronic parent-child stress on the linear and quadratic slope terms describing growth in depressive symptoms were moderately reduced in magnitude among boys. Main effects of chronic parent-child stress continued to predict slope terms describing depression trajectories in girls (see Table S6).
References
Abaied, J. L., & Rudolph, K. D. (2010). Mothers as a resource in times of stress: Interactive contributions of socialization of coping and stress to youth psychopathology. Journal of Abnormal Child Psychology, 38(2), 273–289.
Atherton, O. E., Tackett, J. L., Ferrer, E., & Robins, R. W. (2017). Bidirectional pathways between relational aggression and temperament from late childhood to adolescence. Journal of Research in Personality, 67, 75–84.
Avenevoli, S., Swendsen, J., He, J. P., Burstein, M., & Merikangas, K. R. (2015). Major depression in the national comorbidity survey–adolescent supplement: Prevalence, correlates, and treatment. Journal of the American Academy of Child & Adolescent Psychiatry, 54(1), 37–44.
Barrett, P. (2007). Structural equation modelling: Adjudging model fit. Personality and Individual Differences, 42(5), 815–824.
Beesdo, K., Knappe, S., & Pine, D. S. (2009). Anxiety and anxiety disorders in children and adolescents: Developmental issues and implications for DSM-V. Psychiatric Clinics, 32(3), 483–524.
Belsky, J., & Pluess, M. (2009). Beyond diathesis stress: Differential susceptibility to environmental influences. Psychological Bulletin, 135(6), 885.
Bittner, A., Egger, H. L., Erkanli, A., Costello, E. J., Foley, D. L., & Angold, A. (2007). What do childhood anxiety disorders predict? Journal of Child Psychology and Psychiatry, 48(12), 1174–1183.
Brady, E. U., & Kendall, P. C. (1992). Comorbidity of anxiety and depression in children and adolescents. Psychological Bulletin, 111(2), 244–255.
Brown, T. A. (2007). Temporal course and structural relationships among dimensions of temperament and DSM-IV anxiety and mood disorder constructs. Journal of Abnormal Psychology, 116(2), 313–328.
Burstein, M., He, J. P., Kattan, G., Albano, A. M., Avenevoli, S., & Merikangas, K. R. (2011). Social phobia and subtypes in the National Comorbidity Survey–Adolescent Supplement: prevalence, correlates, and comorbidity. Journal of the American Academy of Child & Adolescent Psychiatry, 50(9), 870–880.
Chavira, D. A., Stein, M. B., Bailey, K., & Stein, M. T. (2004). Child anxiety in primary care: Prevalent but untreated. Depression and Anxiety, 20(4), 155–164.
Choukas-Bradley, S., & Prinstein, M. J. (2014). Peer relationships and the development of psychopathology. In Handbook of developmental psychopathology (pp. 185–204). Springer, Boston, MA.
Cicchetti, D., & Rogosch, F. A. (1996). Equifinality and multifinality in developmental psychopathology. Development and Psychopathology, 8(4), 597–600.
Cole, D. A., Sinclair-McBride, K. R., Zelkowitz, R., Bilsk, S. A., Roeder, K., & Spinelli, T. (2016). Peer victimization and harsh parenting predict cognitive diatheses for depression in children and adolescents. Journal of Clinical Child & Adolescent Psychology, 45(5), 668–680.
Compas, B. E., Connor-Smith, J., & Jaser, S. S. (2004). Temperament, stress reactivity, and coping: Implications for depression in childhood and adolescence. Journal of Clinical Child and Adolescent Psychology, 33(1), 21–31.
Conley, C. S., & Rudolph, K. D. (2009). The emerging sex difference in adolescent depression: Interacting contributions of puberty and peer stress. Development and Psychopathology, 21(2), 593–620.
Costello, E. J., Mustillo, S., Erkanli, A., Keeler, G., & Angold, A. (2003). Prevalence and development of psychiatric disorders in childhood and adolescence. Archives of general psychiatry, 60(8), 837–844.
Creemers, H. E., Dijkstra, J. K., Vollebergh, W. A., Ormel, J., Verhulst, F. C., & Huizink, A. C. (2010). Predicting life-time and regular cannabis use during adolescence; the roles of temperament and peer substance use: The TRAILS study. Addiction, 105(4), 699–708.
Cummings, C. M., Caporino, N. E., & Kendall, P. C. (2014). Comorbidity of anxiety and depression in children and adolescents: 20 years after. Psychological Bulletin, 140(3), 816–845.
Cyranowski, J. M., Frank, E., Young, E., & Shear, M. K. (2000). Adolescent onset of the gender difference in lifetime rates of major depression: A theoretical model. Archives of General Psychiatry, 57(1), 21–27.
Dougherty, L. R., Klein, D. N., Durbin, C. E., Hayden, E. P., & Olino, T. M. (2010). Temperamental positive and negative emotionality and children's depressive symptoms: A longitudinal prospective study from age three to age ten. Journal of Social and Clinical Psychology, 29(4), 462–488.
Ellis, L. K., & Rothbart, M. K. (2001, April). Revision of the early adolescent temperament questionnaire. In Poster presented at the 2001 biennial meeting of the society for research in child development, Minneapolis, Minnesota.
Epel, E. S., Crosswell, A. D., Mayer, S. E., Prather, A. A., Slavich, G. M., Puterman, E., & Mendes, W. B. (2018). More than a feeling: A unified view of stress measurement for population science. Frontiers in Neuroendocrinology, 49, 146–169.
Epkins, C. C., & Heckler, D. R. (2011). Integrating etiological models of social anxiety and depression in youth: Evidence for a cumulative interpersonal risk model. Clinical Child and Family Psychology Review, 14(4), 329–376.
Fergusson, D. M., & Woodward, L. J. (2002). Mental health, educational, and social role outcomes of adolescents with depression. Archives of General Psychiatry, 59(3), 225–231.
Forbes, E. E., Ryan, N. D., Phillips, M. L., Manuck, S. B., Worthman, C. M., Moyles, D. L., et al. (2010). Healthy adolescents' neural response to reward: associations with puberty, positive affect, and depressive symptoms. Journal of the American Academy of Child & Adolescent Psychiatry, 49(2), 162–172.
Gerhardt, C. A., Compas, B. E., Connor, J. K., & Achenbach, T. M. (1999). Association of a mixed anxiety-depression syndrome and symptoms of major depressive disorder during adolescence. Journal of Youth and Adolescence, 28(3), 305–323.
Gershon, A., Hayward, C., Schraedley-Desmond, P., Rudolph, K. D., Booster, G. D., & Gotlib, I. H. (2011). Life stress and first onset of psychiatric disorders in daughters of depressed mothers. Journal of Psychiatric Research, 45(7), 855–862.
Grant, K. E., Compas, B. E., Thurm, A. E., McMahon, S. D., & Gipson, P. Y. (2004). Stressors and child and adolescent psychopathology: Measurement issues and prospective effects. Journal of Clinical Child and Adolescent Psychology, 33(2), 412–425.
Hamilton, J. L., Potter, C. M., Olino, T. M., Abramson, L. Y., Heimberg, R. G., & Alloy, L. B. (2016). The temporal sequence of social anxiety and depressive symptoms following interpersonal stressors during adolescence. Journal of Abnormal Child Psychology, 44(3), 495–509.
Hammen, C. (2005). Stress and depression. Annual Review of Clinical Psycholology, 1, 293–319.
Hammen, C., Kim, E. Y., Eberhart, N. K., & Brennan, P. A. (2009). Chronic and acute stress and the prediction of major depression in women. Depression and Anxiety, 26(8), 718–723.
Hankin, B. L. (2015). Depression from childhood through adolescence: Risk mechanisms across multiple systems and levels of analysis. Current Opinion in Psychology, 4, 13–20.
Hankin, B. L., & Abela, J. R. Z. (Eds.). (2005). Development of psychopathology: A vulnerability-stress perspective. Sage Publications, Inc.
Hankin, B. L., Fraley, R. C., Lahey, B. B., & Waldman, I. D. (2005). Is depression best viewed as a continuum or discrete category? A taxometric analysis of childhood and adolescent depression in a population-based sample. Journal of Abnormal Psychology, 114(1), 96–110.
Hankin, B. L., Mermelstein, R., & Roesch, L. (2007). Sex differences in adolescent depression: Stress exposure and reactivity models. Child Development, 78(1), 279–295.
Hankin, B. L., Davis, E. P., Snyder, H., Young, J. F., Glynn, L. M., & Sandman, C. A. (2017). Temperament factors and dimensional, latent bifactor models of child psychopathology: Transdiagnostic and specific associations in two youth samples. Psychiatry Research, 252, 139–146.
Hankin, B. L., Young, J. F., Abela, J. R., Smolen, A., Jenness, J. L., Gulley, L. D., Technow, J. R., Gottlieb, A. B., Cohen, J. R., & Oppenheimer, C. W. (2015). Depression from childhood into late adolescence: Influence of gender, development, genetic susceptibility, and peer stress. Journal of Abnormal Psychology, 124(4), 803–816.
Harkness, K. L., & Monroe, S. M. (2016). The assessment and measurement of adult life stress: Basic premises, operational principles, and design requirements. Journal of Abnormal Psychology, 125(5), 727–745.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6(1), 1–55.
Hutcherson, S. T., & Epkins, C. C. (2009). Differentiating parent-and peer-related interpersonal correlates of depressive symptoms and social anxiety in preadolescent girls. Journal of Social and Personal Relationships, 26(6–7), 875–897.
Kashdan, T. B. (2007). Social anxiety spectrum and diminished positive experiences: Theoretical synthesis and meta-analysis. Clinical Psychology Review, 27(3), 348–365.
Kendall, A. D., Zinbarg, R. E., Mineka, S., Bobova, L., Prenoveau, J. M., Revelle, W., & Craske, M. G. (2015). Prospective associations of low positive emotionality with first onsets of depressive and anxiety disorders: Results from a 10-wave latent trait-state modeling study. Journal of Abnormal Psychology, 124(4), 933–943.
Kenny, D. A. (2015). Measuring model fit. http://davidakenny.net/cm/fit.htm
Klein, D. N., Dougherty, L. R., & Olino, T. M. (2005). Toward guidelines for evidence-based assessment of depression in children and adolescents. Journal of Clinical Child and Adolescent Psychology, 34(3), 412–432.
Kovacs, M. (1985). The children's depression inventory (CDI). Psychopharmacological Bulletin, 21, 995–998.
Kotov, R., Watson, D., Robles, J. P., & Schmidt, N. B. (2007). Personality traits and anxiety symptoms: The multilevel trait predictor model. Behaviour Research and Therapy, 45(7), 1485–1503.
Liu, R. T. (2016). Taxometric evidence of a dimensional latent structure for depression in an epidemiological sample of children and adolescents. Psychological Medicine, 46(6), 1265–1275.
March, J. S., Parker, J. D., Sullivan, K., Stallings, P., & Conners, C. K. (1997). The multidimensional anxiety scale for children (MASC): Factor structure, reliability, and validity. Journal of the American Academy of Child & Adolescent Psychiatry, 36(4), 554–565.
Merikangas, K., He, J.-P., Brody, D., Fisher, P., Bourdon, K., & Koretz, D. (2009). Prevalence and treatment of mental disorders among US children in the 2001-2004 NHANES. Pediatrics., 125, 75–81.
Merikangas, K. R., He, J. P., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., et al. (2010). Lifetime prevalence of mental disorders in US adolescents: results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). Journal of the American Academy of Child & Adolescent Psychiatry, 49(10), 980–989.
Mezulis, A., Simonson, J., McCauley, E., & Stoep, A. V. (2011). The association between temperament and depressive symptoms in adolescence: Brooding and reflection as potential mediators. Cognition and Emotion, 25(8), 1460–1470.
Morrison, A. S., & Heimberg, R. G. (2013). Social anxiety and social anxiety disorder. Annual Review of Clinical Psychology, 9, 249–274.
Naragon-Gainey, K., & Watson, D. (2011). Clarifying the dispositional basis of social anxiety: a hierarchical perspective. Personality and Individual Differences, 50(7), 926–934.
Naragon-Gainey, K., Watson, D., & Markon, K. E. (2009). Differential relations of depression and social anxiety symptoms to the facets of extraversion/positive emotionality. Journal of Abnormal Psychology, 118(2), 299–310.
Ormel, J., Jeronimus, B. F., Kotov, R., Riese, H., Bos, E. H., Hankin, B., et al. (2013). Neuroticism and common mental disorders: meaning and utility of a complex relationship. Clinical Psychology Review, 33(5), 686–697.
Podsakoff, P. M., MacKenzie, S. B., Lee, J. Y., & Podsakoff, N. P. (2003). Common method biases in behavioral research: A critical review of the literature and recommended remedies. Journal of Applied Psychology, 88(5), 879–903.
Putnam, S. P. (2012). Positive emotionality. In M. Zentner, & R. L. Shiner (Eds.), Handbook of temperament; handbook of temperament (pp. 105-123, chapter xvii, 750 pages) the Guilford press, New York, NY.
R Core Team (2018). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing.
Ranta, K., Kaltiala-Heino, R., Rantanen, P., & Marttunen, M. (2009). Social phobia in Finnish general adolescent population: Prevalence, comorbidity, individual and family correlates, and service use. Depression and Anxiety, 26, 528–536.
Rose, A. J., & Rudolph, K. D. (2006). A review of sex differences in peer relationship processes: potential trade-offs for the emotional and behavioral development of girls and boys. Psychological Bulletin, 132(1), 98.
Rosseel, Y. (2012). Lavaan: An R package for structural equation modeling. Journal of Statistical Software, 48(2), 1–36.
Rothbart, M. K., & Bates, J. E. (2006). Temperament. In N. Eisenberg, W. Damon, & R. M. Lerner (Eds.), Handbook of child psychology: Social, emotional, and personality development (pp. 99–166). Hoboken: John Wiley & Sons Inc..
Rudolph, K. D. (2002). Gender differences in emotional responses to interpersonal stress during adolescence. Journal of Adolescent Health.
Rudolph, K. D., & Flynn, M. (2007). Childhood adversity and youth depression: Influence of gender and pubertal status. Development and Psychopathology, 19(2), 497–521.
Rudolph, K. D., Flynn, M., & Abaied, J. L. (2008). A developmental perspective on interpersonal theories of youth depression. In J. R. Z. Abela & B. L. Hankin (Eds.), Handbook of depression in children and adolescents (p. 79–102). The Guilford Press.
Ruscio, A. M. (2010). The latent structure of social anxiety disorder: Consequences of shifting to a dimensional diagnosis. Journal of Abnormal Psychology, 119(4), 662–671.
Saluja, G., Iachan, R., Scheidt, P. C., Overpeck, M. D., Sun, W., & Giedd, J. N. (2004). Prevalence of and risk factors for depressive symptoms among young adolescents. Archives of Pediatrics & Adolescent Medicine, 158(8), 760–765.
Scanlon, N. M., & Epkins, C. C. (2015). Aspects of mothers’ parenting: Independent and specific relations to children’s depression, anxiety, and social anxiety symptoms. Journal of Child and Family Studies, 24(2), 249–263.
Schafer, J. L., & Graham, J. W. (2002). Missing data: our view of the state of the art. Psychological Methods, 7(2), 147.
Sewart, A. R., Zbozinek, T. D., Hammen, C., Zinbarg, R. E., Mineka, S., & Craske, M. G. (2019). Positive affect as a buffer between chronic stress and symptom severity of emotional disorders. Clinical Psychological Science.
Shih, J. H., Eberhart, N. K., Hammen, C. L., & Brennan, P. A. (2006). Differential exposure and reactivity to interpersonal stress predict sex differences in adolescent depression. Journal of Clinical Child and Adolescent Psychology, 35(1), 103–115.
Shiner, R., & Caspi, A. (2003). Personality differences in childhood and adolescence: Measurement, development, and consequences. Journal of Child Psychology and Psychiatry, 44(1), 2–32.
Snyder, H. R., Gulley, L. D., Bijttebier, P., Hartman, C. A., Oldehinkel, A. J., Mezulis, A., Young, J. F., & Hankin, B. L. (2015). Adolescent emotionality and effortful control: Core latent constructs and links to psychopathology and functioning. Journal of Personality and Social Psychology, 109(6), 1132–1149.
Starr, L. R., & Davila, J. (2008). Differentiating interpersonal correlates of depressive symptoms and social anxiety in adolescence: Implications for models of comorbidity. Journal of Clinical Child & Adolescent Psychology, 37(2), 337–349.
Van Oort, F. V. A., Greaves-Lord, K., Verhulst, F. C., Ormel, J., & Huizink, A. C. (2009). The developmental course of anxiety symptoms during adolescence: The TRAILS study. Journal of Child Psychology and Psychiatry, 50(10), 1209–1217.
Vrshek-Schallhorn, S., Stroud, C. B., Mineka, S., Hammen, C., Zinbarg, R. E., Wolitzky-Taylor, K., & Craske, M. G. (2015). Chronic and episodic interpersonal stress as statistically unique predictors of depression in two samples of emerging adults. Journal of Abnormal Psychology, 124(4), 918.
Watson, D., & Clark, L. A. (1991). The mood and anxiety symptom questionnaire (MASQ). University of Iowa, Iowa City: Unpublished manuscript.
Watson, D., & Naragon-Gainey, K. (2010). On the specificity of positive emotional dysfunction in psychopathology: Evidence from the mood and anxiety disorders and schizophrenia/schizotypy. Clinical Psychology Review, 30(7), 839–848.
Watson, D., Gamez, W., & Simms, L. J. (2005). Basic dimensions of temperament and their relation to anxiety and depression: A symptom-based perspective. Journal of Research in Personality, 39(1), 46–66.
Wei, C., Hoff, A., Villabø, M. A., Peterman, J., Kendall, P. C., Piacentini, J., ... & Sherrill, J. (2014). Assessing anxiety in youth with the multidimensional anxiety scale for children. Journal of Clinical Child & Adolescent Psychology, 43(4), 566–578.
Wetter, E. K., & Hankin, B. L. (2009). Mediational pathways through which positive and negative emotionality contribute to anhedonic symptoms of depression: A prospective study of adolescents. Journal of Abnormal Child Psychology, 37(4), 507–520.
Yap, M. B. H., Pilkington, P. D., Ryan, S. M., & Jorm, A. F. (2014). Parental factors associated with depression and anxiety in young people: A systematic review and meta-analysis. Journal of Affective Disorders, 156, 8–23.
Acknowledgements
This material is based upon work supported by the National Science Foundation Graduate Research Fellowship Program under Grant No. DGE – 1746047.
Funding Source
The research reported in this article was supported by grants from the National Institute of Mental Health to Benjamin L. Hankin, R01MH077195, and to Jami F. Young, R01MH077178.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflicts of interest.
Ethical Approval
All study procedures were approved by the Institutional Review Boards at the Univerisity of Denver and Rutgers University.
Informed Consent
All participating parents provided consent to participation in the study, and all participating adolescents provided assent to study participation.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 56 kb)
Rights and permissions
About this article

Cite this article
Griffith, J.M., Long, E.E., Young, J.F. et al. Co-Occurring Trajectories of Depression and Social Anxiety in Childhood and Adolescence: Interactive Effects of Positive Emotionality and Domains of Chronic Interpersonal Stress. J Abnorm Child Psychol 48, 823–837 (2020). https://doi.org/10.1007/s10802-020-00634-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-020-00634-7