
Examined prospective associations among poverty-related family stress, coping, involuntary stress reactivity, and psychological symptoms in a sample of 79 rural, low-income adolescents. Poverty-related family stress predicted adolescents’ anxious/depressed and aggressive behavior 8 months later, controlling for prior symptoms. Coping interacted with initial symptoms and involuntary stress reactivity to predict changes in symptoms over time, showing that primary and secondary control coping were most strongly associated with changes in symptoms for adolescents with low initial symptoms and involuntary stress reactivity. The only significant predictor of coping over time was prior coping, suggesting that coping is not symptom-driven and may be somewhat trait-like. Implications for interventions and additional research are offered.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
It is well recognized that adolescents who experience economic hardship are at increased risk for social and emotional problems (McLoyd, 1998). Conger's Family Stress Model posits that poverty takes a psychological toll on children and adolescents via the large burden of stress it places on parents (Conger and Conger, 2002). Wadsworth and Compas (2002) extended Conger and colleagues’ research to show that poverty also takes a toll on adolescents via the large burden of stress it places directly on them. Millions of children and adolescents are exposed to the potent stress of living with chronic poverty, yet we know little about how children cope with living in such difficult circumstances. Identifying how adolescents successfully regulate themselves in the face of such chronic stress is critical because coping skills are likely to play an important role in contributing to or buffering against emotional/behavioral problems during this developmental stage and over the lifespan (Compas et al., 2001).
We are beginning to understand much about how school-aged children and adolescents cope with other types of stress in their lives, and that some types of coping appear to buffer stress for some individuals (Compas et al., 2001). There is some consensus that approach or engagement strategies are generally efficacious, at least in stressful circumstances in which the child has some degree of control. Conversely, strategies that disengage a child or adolescent from a stressor and their feelings, and often from sources of support, are generally less efficacious, except in circumstances that are difficult for them to control. Despite knowledge about which strategies are generally effective for coping with a variety of normative, nonchronic stressors, we are only just beginning to examine how adolescents cope with the stress of living in extreme environments such as chronic poverty, and whether coping can be helpful in such extreme circumstances.
Adolescents in Wadsworth and Compas’ study (2002) reported using a variety of strategies to cope with poverty-related family stress (economic strain and family conflict), and several of these were associated with aggressive and anxious/depressed behavior. In particular, consistent with previous research on coping with other types of stress, engagement coping—both primary control and secondary control engagement strategies—was associated with fewer symptoms. Primary control coping involves efforts to solve the problem or directly manage feelings and includes problem solving, emotional expression, and emotional regulation. Secondary control coping involves efforts to adapt oneself to stressful circumstances and includes acceptance, cognitive restructuring, distraction, and positive thinking. These findings suggest that primary and secondary control coping may buffer an adolescent from the ill effects of poverty-related family stress, although these associations have yet to be examined prospectively.
Interestingly, Wadsworth and Compas (2002) found that disengagement coping, which includes avoidance, denial, and wishful thinking, was not associated with worse functioning as it often is for children coping with other types of stress (e.g., Sandler et al., 2000). Thus, coping with poverty-related family stress may look different from coping with more normative types of stress. In fact, several recent behavior genetics studies have elegantly demonstrated the power of chronic poverty to disrupt developmental processes and affect, for example, the heritability of various personality characteristics such as IQ and aggression (e.g., Cleveland, 2003; Turkheimer et al., 2003). Consequently, it is not surprising that there may be differences in how adolescents cope with normative stressors versus how they cope with poverty-related family stress.
Longitudinal data on the associations between adolescent coping with poverty-related family stress and emotional and behavioral problems are sorely needed as they are crucial for determining the extent to which coping is capable of buffering this type of stress (Sandler et al., 1994). In addition, assuming that coping is related to symptoms over time only for certain individuals and/or under certain conditions, longitudinal data are needed in order to specify the conditions under which coping either buffers or accentuates stress. Finally, because poverty is a chronic condition for so many children, potentially requiring almost constant coping, longitudinal data are needed to examine the stability of coping over time in this context and the factors that predict whether a child tends to use efficacious or potentially harmful coping. The current study addresses each of these issues.
Longitudinal Associations Between Coping and Psychological Symptoms
A handful of studies have now shown strong associations between coping and psychological symptoms across time, with coping predicting changes in symptoms, and not the reverse (e.g., Holahan et al., 1997). A variety of coping strategies (both positive and negative) representing elements of all three types of coping introduced above (primary control, secondary control, disengagement) predicted changes in internalizing and externalizing symptoms over a year in Tolan et al.’s (2003) urban, low-income adolescent sample. Similarly, among children of divorce, coping predicted changes in depression and anxiety symptoms over five and a half months (Sandler et al., 1994). In none of these studies did symptoms predict changes in coping over time, suggesting that coping is not simply a proxy for symptoms, but rather is a resource or burden in the face of stress that affects psychological adjustment.
The current study examined the extent to which coping with poverty-related family stress predicted changes in symptoms over 8 months time, controlling for prior symptoms. To provide a strong test of coping's prospective effect, we also controlled for the amount of poverty-related family stress in predicting changes in symptoms. Thus, we assessed the degree to which coping predicted changes in symptoms over and above the variance accounted for by prior symptoms and poverty-related family stress.
Moderators of Coping's Effectiveness
Most longitudinal coping research has assessed the main effect of coping on changes in symptoms over time (as proposed above). However, it is very likely that the effectiveness of coping in buffering symptoms will depend on some characteristics of the child as proposed by Compas et al. (1999). Factors that may moderate coping's effect on symptoms over time include: stress level, initial level of symptoms, and involuntary stress reactivity.
As suggested by Sandler et al. (1994), coping may interact with the amount of stress experienced by the child. Sandler and colleagues found small interactions between active coping and stress in predicting concurrent conduct problems, and weak interactions between stress and coping in predicting prospective anxiety. Such an interaction is generally interpreted as evidence that coping serves as a stress buffer in studies of nonchronic stressors. However, in the face of a chronic stressful circumstance, a different question can be posed: is coping's efficacy dependent on the amount of stress present? In other words, is there only a buffering effect of coping for children under certain levels of stress? It is possible that the efficacy of coping may be reduced when an individual's resources are taxed by severely stressful circumstances (Matthews and Wells, 1996).
In addition, coping's effectiveness over time may be influenced by an individual's initial level of symptoms. Lazarus and Folkman (1984) proposed that appraisal or recognition of a stressor is needed for stress to impel coping. Whereas some appraisals of stressful circumstances or events are cognitive, it is also the case that symptoms can serve as an emotional appraisal of stress. As Rudolph et al. (1995) showed, symptoms can serve as an indication to an individual that something is wrong and needs to be coped with. Thus, we expect that coping with poverty-related family stress is likely to be maximally effective for someone with higher initial levels of symptoms to be reduced. However, it is also possible that symptoms interfere with the ability to use effective coping. Symptoms of psychopathology are associated with cognitive information-processing biases (e.g., see Weiss et al., 1998), which may hamper adolescents’ ability to employ cognitively demanding primary and secondary control coping strategies. Depressive symptoms, for example, are associated with a tendency to cognitively appraise events more negatively, over-generalize the meaning of negative events, and selectively attend to negative information (Chang and Strunk, 1999; Haaga and Beck, 1992; Lewinsohn and Talkington, 1979). In fact, there is some evidence to suggest that depressive and anxious symptoms exert deleterious effects on late adolescents’ abilities to effectively cope with daily stressors (Gunthert et al., 2002). Gunthert et al. (2002) found that use of emotion expression coping with daily stress, a component of primary control coping usually seen as helpful, was associated with reductions in positive affect for late adolescents high in initial depression. Thus, an alternative hypothesis investigated in the current study is that coping may actually be more efficacious under conditions of lower initial symptoms.
Finally, involuntary stress reactivity is the body's automatic cognitive, emotional, and behavioral responses to a stressful event. Involuntary stress reactivity, which includes involuntary responses to stress such as physiological reactivity, intrusive thoughts, and rumination, may interfere with adolescents’ ability to use coping effectively (Compas et al., 1999). Thus whether coping is effective may partially depend on whether the individual is experiencing significant amounts of intrusive thoughts, rumination, and/or physiological arousal. These types of involuntary stress responses can limit the availability of effortful processing resources necessary for positive primary and secondary control engagement coping (Wegner, 1994). Thus, it is expected that coping's efficacy may be reduced in the face of high involuntary stress reactivity.
Therefore, we considered three possible moderators of coping's prospective effect on symptoms in this paper. (1) First we examined the interaction between the amount of poverty-related family stress and adolescent coping. This tested the proposition that primary and secondary control coping's effectiveness depends on the amount of stress one is coping with. (2) Next, we examined the interaction between symptoms and coping. This tested the proposition that coping's effectiveness depends on one's initial levels of symptoms. (3) Finally, we examined the interaction between involuntary stress reactivity and coping. This tested the prediction that primary and secondary control coping are helpful (and disengagement coping is unhelpful) over time only when initial levels of involuntary stress reactivity are low. We expected that high levels of involuntary stress reactivity may interfere with effective coping and promote ineffective coping (Compas et al., 1999).
Predictors of Coping Over Time
Very little is known about what determines how an individual copes with stress. However, involuntary stress reactivity—which has obvious origins in temperament—can clearly contribute to the tendency of an individual to approach novel situations (e.g., Kagan et al., 1995) or to be capable of distraction (e.g., Rothbart et al., 1995). Thus, involuntary stress reactivity should predict individual differences in effortful coping over time.
Early conceptualizations posited that coping was a stable personality characteristic (e.g., Valliant, 1977). Lazarus and Folkman (1984) revolutionized the field by suggesting that coping is a process rather than a trait, and that coping is influenced by context. Current theory emphasizes that coping is a fluid and changing process that is influenced by contextual factors such as the degree and severity of stress (Compas et al., 1999). Thus, in addition to involuntary stress reactivity, the amount of poverty-related family stress may predict variation in coping over time. However, current theories of the development of coping such as the Responses to Stress Model (Compas et al., 1999) also acknowledge that there will be a degree of stability in an individual's coping repertoire owing to individual characteristics such as temperament and personality as well as stable aspects of the environment such as chronicity of stress and adversity.
We also examined both internalizing (anxious/depressed) and externalizing (aggressive) symptoms as possible predictors of coping. The cross-sectional relationship between coping and symptoms is often interpreted as reflecting the fact that coping influences symptoms (Compas et al., 2001). However, the reverse is an equally plausible interpretation. Perhaps symptoms drive coping, and thus symptoms should be a strong predictor of coping over time. We test this possibility in this study.
Purpose of the Current Study
The current study examines the associations among poverty-related family stress, responses to stress, and adolescent aggressive and anxious/depressed behavior over time among adolescents from low-income families. First, we test the extent to which coping contributes to changes in symptoms over time. Hypotheses: (1a) Consistent with prior research on coping with economic strain (Wadsworth and Compas, 2002), we predicted that primary and secondary control coping would predict decreases in aggressive (AGG) and anxious/depressed (A/D) behavior over time, controlling for prior symptoms and poverty-related stress. (1b) Disengagement will predict increases in AGG and A/D over time, controlling for prior symptoms and poverty-related stress. Second, we examine factors that may determine whether coping is related to symptoms over time, in order to deepen our understanding of how adolescents come to cope with such difficult circumstances. Hypotheses: (2a) Poverty-related stress will interact with coping in predicting changes in AGG and A/D, such that stress will interfere with adolescents’ ability to use helpful primary and secondary control coping and will encourage disengagement coping. This is based on research showing that stress can reduce attentional resources needed for effective coping (e.g., Matthews and Wells, 1996). (2b) Initial symptoms and coping will interact in predicting changes in AGG and A/D, such that primary and secondary control coping will predict decreases in symptoms primarily for those higher in initial symptoms, as high levels of initial symptoms are likely to serve as an indication of stress (Rudolph et al., 1995). (2c) Involuntary stress reactivity will interact with coping, in predicting changes in AGG and A/D, such that involuntary stress reactivity will interfere with adolescents’ ability to use helpful primary and secondary control coping and will encourage disengagement coping. This is based on theory and research suggesting that involuntary stress responses limit availability of effortful processing resources necessary for efficacious coping. Third, we examine the predictors of coping over time, to gain understanding of how coping may develop in harsh settings. Hypotheses: (3a) Involuntary stress reactivity will predict increases in disengagement coping and decreases in primary and secondary control coping over time, because involuntary responses to stress are believed to encourage immature coping and discourage complex, potentially beneficial coping (Compas et al., 1999). (3b) Poverty-related stress will predict increases in disengagement coping and decreases in primary and secondary control coping over time, due to stress’ ability to tax resources necessary for effective coping. (3c) Initial levels of AGG and A/D should also predict increases in disengagement coping and decreases in primary and secondary control coping over time, as symptoms can interfere with the ability to use efficacious coping (Gunthert et al., 2002)
METHOD
Participants and Procedure
Participants were 79 adolescents followed over 8 months, comprising a subsample of a larger study of family processes in lower-income families. Adolescents were recruited from a middle school and high school in rural northern New England for a “study of adolescent stress and coping behavior.” The county in which the schools are located has the second highest unemployment rate in the state and the towns served by these schools are considered to be among the poorest in the state. Comparisons between adolescents in the subsample and those in the larger sample revealed no differences in lunch program enrollment (29 vs. 34%, χ2(1)=0.9, ns), mean age (14.5 vs. 14.9, t(360)=−1.61, ns), or gender (58 vs. 48% females, χ2(1)=3.2, ns). Representative of this region of northern New England, 97% of the sample was Caucasian—one student identified as African American and one student as American Indian. The mean SES of the participating students estimated by Hollingshead's (1975) 9-point parental employment scale (1: lowest level) was 3.7, indicating that the average parent, if employed, was employed as a laborer or tenant farmer, for example. Approximately two-thirds of the adolescents (69%) reported living with two parents. The remaining adolescents lived with either zero (10%) or one parent (21%).
Four hundred sixty students were invited to complete questionnaires at the first time point—364 students with complete data were retained. One hundred of these students were randomly selected and invited for a second data collection—79 students took part. A sample size of 100 was sought to ensure adequate power to detect medium effects with up to four predictor variables (power=0.77 with current sample size). Questionnaires were completed by students during class time under the supervision of their teachers and research assistants. Students were informed that their responses were confidential. Survey booklets were devoid of personal identification information, but contained a unique identification number that was used to track respondents over time. A month prior to initial participation, all parents were mailed a packet of questionnaires regarding their child, a detailed description of the study, and a form to return if they did not wish for their child to complete the survey at their school. Parents thereby provided passive consent for their children's participation. Participating students provided their signatures of assent. Students who completed the survey received small gift certificates as compensation at both time points.
MEASURES
Stress and Coping
Adolescents completed the Responses to Stress Questionnaire (RSQ; Connor-Smith et al., 2000) at both time points to assess the ways that they coped with two potential sources of family stress—economic strain and family conflict.
Amount of Stress
The first portion of the RSQ assesses how often in the last 6 months the adolescent experienced each of 8 economic strain and family conflict stressful events. Family conflict items assessed both interparental as well as parent-adolescent conflict, and included: I argued with my parents about money; I heard my parents say mean things to each other; I heard my parents shouting at each other. Economic strain items included: My parents didn't have enough money to pay the bills; There's no money left over to do something fun as a family; We can't afford a nice house. Adolescents indicated on a four-point Likert-type scale how often each of the stressors occurred in the last 6 months (“0”: not at all; “1”: a few times; “2”: often; and “3”: almost every day). The scores for each stressor were summed to create a total economic strain score and a total family conflict score. Coefficient alpha indicated a high degree of internal consistency reliability for both 8-item stressor scales, with α=0.88 for family conflict and α=0.90 for economic strain. A composite poverty-related family stress variable was computed by summing the standardized scores from the two versions of the RSQ.
Coping Responses to Stress and Involuntary Stress Reactivity
The second portion of the RSQ contains 57 items that ask the respondents to report how they responded during the last 6 months to the stressors they endorsed. The RSQ contains 19 factor-analytically-derived scales that aggregate further into five primary factors: Primary control coping, secondary control coping, disengagement coping, involuntary engagement, and involuntary disengagement (Connor-Smith et al., 2000). Primary and secondary control coping are both considered to be types of engagement coping. The first three factors reflect voluntary coping processes, while the latter factors reflect involuntary responses that occur under stress. As this paper is concerned with coping and involuntary stress reactivity, the present analyses focus on the three volitional coping factors and involuntary (engagement) stress reactivity. Primary control coping is comprised of problem solving (e.g., I do something to try to fix the problem), emotional expression (e.g., I do something to let my feelings out), and emotional regulation (e.g., I do something to calm myself down when we are having money troubles: take deep breaths, pray, listen to music, walk, take a break, meditate). Secondary control coping is comprised of positive thinking (e.g., I tell myself everything's going to be alright), cognitive restructuring (e.g., I try to see the good that will come from the situation or what I will learn from it), acceptance (e.g., I realize I just have to live with things the way they are), and distraction (e.g., I keep my mind off the money troubles by: exercising, seeing friends, watching TV, playing video games, doing a hobby). Disengagement coping is comprised of cognitive and behavioral avoidance (e.g., I try to block out thoughts and feelings about the money problems), denial (e.g., I tell myself this isn't happening to me), and wishful thinking (e.g., I wish someone or something would come get me out of this mess). Involuntary stress reactivity is comprised of emotional arousal (e.g., When problems with my family come up, I get upset by things that don't usually bother me), impulsive action (e.g., When we are having trouble as a family, I can't control what I do or say), intrusive thoughts (e.g., When we’re having problems, I can't stop thinking about the problems when I try to sleep or I have bad dreams about them), physiological arousal (e.g., When I have problem with my family, I feel it in my body (check all that apply): my heart races, I feel hot or sweaty, my breathing speeds up, my muscles get tight), and rumination (e.g., When problem with my family come up, I can't stop thinking about how I am feeling).
The RSQ has demonstrated good reliability and validity with multiple samples (Connor-Smith et al., 2000). With this sample of adolescents, internal consistencies were: primary control coping (economic: 0.76, conflict: 0.82), secondary control coping (economic: 0.86, conflict: 0.83), disengagement coping (economic: 0.85, conflict: 0.89), and involuntary engagement (economic: 0.76, conflict: 0.95). Construct and criterion validity, and test–retest reliability have been demonstrated in other samples (Connor-Smith et al., 2000; Wadsworth et al., 2004). As recommended by Connor-Smith et al., 2000; factor scores on the RSQ were computed as proportions of the total score for all responses (i.e., sum of scores on primary control items/sum of all items) to control for overall responding biases. Composite poverty-related family stress coping and involuntary stress reactivity variables were computed by summing standardized scores for each of the five RSQ factors from the two versions of the RSQ.
Emotional and Behavioral Problems
The Youth Self Report (YSR; Achenbach, 1991) was used to assess adolescents’ self-reported emotional and behavioral problems. The YSR has excellent reliability and validity (Achenbach, 1991). This measure contains 112 items that assess a variety of behaviors. Adolescents indicated how often they exhibit each behavior on a three-point Likert scale (“0”: never true; “1”: sometimes true; and “2”: very often true). In this study we focused on two subscales of the YSR: Anxious/Depressed and Aggressive Behavior. These two scales are representative of internalizing and externalizing problems in adolescents and more closely match measures of psychopathology used in prior research (e.g., Conger et al., 1993; McLoyd et al., 1994) than would the broadband internalizing/externalizing scales of the YSR.
RESULTS
Descriptive Analyses
Table I contains the means, standard deviations, and ranges of all Time 1 and Time 2 variables. Table II contains correlations between Time 1 and Time 2 variables in order to examine the stability of adolescents’ coping, involuntary stress reactivity, amount of poverty-related family stress, and symptoms across an 8-month period. Adolescents’ reports of Time 1 and Time 2 coping and involuntary stress reactivity were significantly correlated. These results indicate that adolescent coping and involuntary stress reactivity in the face of poverty-related family stress were moderately stable across an 8-month period. The amount of poverty-related family stress was also consistent from Time 1 to Time 2. As expected, adolescent anxious/depressed and aggressive behavior at Time 1 and Time 2 were significantly related, though not as robustly as effortful coping.
Cross-sectional correlations among Time 1 and Time 2 variables were also examined (see Table II). At Time 1, amount of poverty-related family stress was negatively related to primary and secondary control coping and was positively associated with disengagement coping. At Time 1, adolescent aggressive and anxious/depressed behaviors were positively associated with disengagement coping, and involuntary reactivity to poverty-related family stress. In contrast, these symptoms were negatively related to primary and secondary control coping. The amount of poverty-related family stress was associated with more aggressive and anxious/depressed behavior. Cross-sectional correlations among Time 2 variables showed similar patterns to those at Time 1.
Because primary analyses involved predicting Time 2 symptoms and Time 2 coping over time, correlations also examined prospective associations between Time 1 predictor variables and Time 2 symptoms and between Time 1 predictor variables and Time 2 coping. Adolescent involuntary stress reactivity at Time 1 was positively correlated with aggressive and anxious/depressed behavior at Time 2. In addition, more disengagement coping at Time 1 was associated with more anxious/depressed behavior at Time 2. Amount of poverty-related family stress was not related to adolescent symptoms at Time 2.
Time 1 poverty-related family stress and symptoms were also correlated with coping and involuntary stress reactivity at Time 2. Time 1 amount of poverty-related family stress was negatively related to primary control coping and positively related to involuntary stress reactivity at Time 2. Aggressive and anxious/ depressed behaviors at Time 1 were negatively associated with primary control coping at Time 2. In contrast, these symptoms at Time 1 were associated with more involuntary stress reactivity at Time 2. In addition, aggressive behavior at Time 1 was related to less secondary control coping at Time 2.
Regression Analyses
A series of multiple regressions were conducted to examine prospective predictors of: (a) adolescents’ emotional/behavioral symptoms and (b) adolescents’ coping. In each set of analyses, initial levels of symptoms or coping were controlled in order to provide a strong test of the predictors of these outcomes over time. In addition, models were designed to examine the main and interactive effects of predictor variables on changes in symptoms; main effects models were run for predicting coping, as no interactions were specified.
Predictors of Adolescent Adjustment Over Time
A major objective of the current study was to examine the prospective relations of adolescent coping, stress responses, and amount of poverty-related family stress on subsequent adolescent anxious/depressed and aggressive behavior. A series of six hierarchical multiple regressions were conducted using Time 2 anxious/depressed behavior and Time 2 aggressive behavior as dependent variables. In the first step, adolescents’ symptoms at Time 1 (anxious/depressed or aggressive) were entered to control for initial levels of adjustment. Next, in steps 2–4 adolescents’ amount of family stress, involuntary stress reactivity, and coping at Time 1 were entered to examine these variables as predictors of symptoms over time. For both anxious/depressed and aggressive behavior, regressions were conducted separately for primary control, secondary control, and disengagement coping. The fifth to seventh steps tested three interactive effects. Because all variables in the interactions were continuous, the variables were centered (variable minus its mean) and then multiplied to calculate the interaction terms (Aiken and West, 1991). This approach to analyzing interaction effects in multiple regression is preferable because it preserves the continuous nature of the variable and thereby maximizes its variability (Aiken and West, 1991). In the fifth step, the interaction of Time 1 coping and Time 1 symptoms (anxious/depressed or aggressive) was entered to examine the interaction of coping and symptoms as a predictor of symptoms over time. Next, the interaction of Time 1 coping and Time 1 involuntary stress reactivity was entered into the equation and finally the interaction of time 1 coping and time 1 involuntary stress reactivity was entered. Six equations were run because of two types of symptoms and three types of coping.
Controlling for initial levels of anxious/depressed behavior, amount of stress at Time 1 significantly predicted anxious/depressed behavior at Time 2 (see Table III). Adolescents who reported greater levels of family stress at Time 1 were more likely to exhibit more anxious/depressed behavior 8 months later. There were no main effects of involuntary stress reactivity or coping on anxious/depressed behavior over time. However, the interaction of Time 1 disengagement coping and Time 1 anxious/depressed behavior significantly predicted anxious/depressed symptoms at Time 2. Adolescents who used more disengagement coping and had higher initial levels of anxious/depressed behavior were at greater risk for maintaining higher levels of anxious/depressed behavior 8 months later in comparison to adolescents who reported using less disengagement coping with family stress, for whom the same level of symptoms tended to remit somewhat. There was also an interaction between Time 1 stress and Time 1 primary control coping, showing that use of primary control coping was protective against future anxious/depressed behavior, especially for those with higher Time 1 stress.
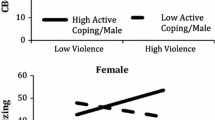
Controlling for Time 1 aggressive behavior, Time 1 involuntary stress reactivity was negatively associated with Time 2 aggressive behavior (see Table IV), but there were no main effects of Time 1 coping or amount of stress on Time 2 aggressive behavior. Both the interaction of Time 1 primary control coping with Time 1 aggressive behavior and the interaction between secondary control coping with Time 1 aggressive behavior were significant predictors of aggressive symptoms at Time 2. Greater use of both types of coping was associated with less aggressive behavior at time 2 for adolescents with lower, but not higher levels of initial symptoms. In addition, the interaction of Time 1 primary control coping and Time 1 involuntary stress reactivity was significantly associated with aggressive behavior at Time 2, indicating that involuntary stress reactivity moderated the link between primary control coping and aggressive symptoms. Primary control coping was associated with less aggressive behavior at Time 2 primarily for those with lower levels of stress reactivity. Finally, there was a trend interaction between disengagement coping and involuntary stress reactivity, showing that Time 1 disengagement coping was associated with more Time 2 symptoms at lower levels of involuntary stress reactivity.
Predictors of Adolescent Coping Over Time
A second aim of the present study was to examine adolescents’ amount of poverty-related stress, involuntary stress reactivity, and initial symptoms as predictors of adolescents’ coping skills over time. Controlling for coping at Time 1, there were no significant main effects of adolescents’ Time 1 stress, stress reactivity, or aggressive behavior on Time 2 coping (Table V). Anxious/depressed behavior contributed marginally to the prediction of disengagement coping. The most consistent predictor of adolescents’ coping over time was prior coping skills.
DISCUSSION
The current study examined the prospective associations among poverty-related family stress, coping, involuntary stress reactivity, and symptoms of psychopathology in a sample of adolescents living under conditions of economic hardship. The analyses revealed significant stability of poverty-related family stress over a period of 8 months, as well as significant stability of coping and involuntary stress reactivity over that time period. In addition, symptoms, amount of stress, and involuntary stress reactivity, along with their interactions with coping, predicted changes in symptoms over time.
Stability of Coping and Responses to Stress
One purpose of the current study was to assess the stability of adolescents’ coping and involuntary responses to family stress over time. Adolescents’ reports of all types of coping and involuntary stress reactivity were significantly related across an 8-month period. Moderate temporal stability of adolescents’ coping with family stress in low-income families is consistent with prior research demonstrating moderate continuity over time in coping with other types of stressors (Compas et al., 1988; Sandler et al., 1994; Sandler et al., 2000). As in other studies, this finding suggests that some amount of consistency in coping with family stress is indicative of coping responses being partly state-like, partly trait-like. However, the present study also found significant stability in poverty-related family stress. Thus, it is also likely that stability in coping reflects the stability of having to cope repeatedly with the same chronic stressor(s). This possibility is plausible given that the adolescents in the larger study comprised the vast majority of adolescents from this rural town in New England, which has seen very little economic change in the last four or five decades. Future studies could examine continuity in coping with poverty-related family stress for adolescents with more transitory family conflict and economic strains.
Predictors of Psychological Symptoms Over Time
A major aim of the present study was to examine the effects of poverty-related family stress, involuntary stress reactivity, and coping on adolescents’ psychological symptoms over time. Specifically, we examined the main effects and hypothesized interaction effects of these variables on changes in adolescents’ aggressive and anxious/depressed behavior over the span of 8 months.
Main Effects
First, we tested the main effects of coping, family stress, and involuntary stress reactivity on changes in adolescents’ anxious/depressed and aggressive behavior over time. Contrary to our predictions, there were no main effects of coping on changes in symptoms over time. Although disengagement coping at Time 1 was correlated with greater anxious/depressed behavior at Time 2, in the more conservative regression analyses disengagement did not predict later anxious/depressed behavior after controlling for prior symptoms, amount of stress, and stress reactivity. The limited prior research in this area has found some small prospective effects of coping with other types of stressors on child and adolescent adjustment, although these prior studies did not control for amount of stress, stress reactivity, and initial symptoms as we did (e.g., Sandler et al., 1994). Another major difference is that the current study included adolescents’ own reports of poverty-related family stress in a rural setting. Chronic poverty-related family stress, especially as measured by the adolescents themselves, may be such a powerful influence in an adolescent's life that it is difficult to compensate using coping. Thus, family stress in the context of more disadvantaged, low-income families may create a very different type of stressor in comparison to coping with other kinds of stresses among adolescents from more advantaged families. The reality may be that effortful coping in and of itself does not have a main effect on adolescents’ emotional and behavioral symptoms in this environment. As Grant and colleagues (2003) highlight in their review of the literature on stress and adjustment, the relations among coping, stress, and child and adolescent outcomes are more complex and transactional than can be captured in the statistical language of main effects (Grant et al., 2003). Thus, the interactions tested here may provide the better index of how coping unfolds to affect symptoms over time.
As we predicted, amount of poverty-related family stress contributed to changes in adolescent anxious/depressed behavior from Time 1 to Time 2. Family stress did not predict changes in adolescent aggressive behavior. Adolescents with greater levels of poverty-related family stress at Time 1 had more anxious/depressed behavior at Time 2, even after controlling for initial levels of anxious/depressed behavior. This finding is consistent with a large body of research that has well established various types of stress as significant risk factors for child and adolescent psychopathology, especially for internalizing problems such as depression (Grant et al., 2003). The current study contributes to our understanding of the specificity of the effects of poverty-related family stress on adolescent symptoms. In a recent review of what is known about the effects of specific stressors on specific child and adolescent psychological outcomes, McMahon and colleagues (2003) emphasize the importance of moving beyond research on the effects of general stress on general well-being, and instead beginning to understand what specific types of stressors are predictive of specific types of internalizing versus externalizing symptoms (McMahon et al., 2003). The current study is one of a handful of studies that have begun to examine the role of family stress in low-income families in determining adolescent internalizing and externalizing problems.
Our finding that poverty-related family stress predicted adolescent internalizing but not externalizing symptoms is somewhat consistent with a recent meta-analysis of the direct and indirect effects of poverty on adolescent symptoms (Grant et al., 2003). In their path-analysis of meta-analytic findings, Grant et al. found that the best fitting model contained poverty exerting a direct effect on adolescent internalizing symptoms. However, inconsistent with our results, the best fitting model for a small, subsample of longitudinal studies was a direct link between poverty and externalizing symptoms. As these authors emphasize, more research is clearly needed to address the specificity of poverty-related family stress on child and adolescent symptoms because of the dearth of studies addressing this link, particularly prospectively. Our data suggest that coping and involuntary stress reactivity may play a role in determining specificity.
Moderated Effects
Next, recognizing that the association between coping and symptoms over time may not exist as a straightforward main effect, we posited a number of moderated effects that could be in operation. Each of these moderated effects has been offered as a theoretical explanation in prior studies (e.g., Ebata and Moos, 1994), but this is one of the first studies to explicitly test each of these hypotheses. First, we hypothesized that the effectiveness of coping may depend in part on one's prior psychological functioning. Thus, it is possible that coping may only be beneficial if an individual is distressed to begin with, otherwise why would coping be enacted? This is consistent with proposed models of self-regulation (e.g., Eisenberg et al., 1997). However, it is also quite possible that high levels of symptoms may interfere with the ability to use effective coping (Matthews and Wells, 1996). Our results indicated that primary control and secondary control coping interacted with aggressive behavior, such that these types of coping were protective at lower, but not higher levels of initial symptoms. On the other hand, there was a significant interaction between adolescents’ disengagement coping and anxious/depressed behavior, such that adolescents’ disengagement coping predicted a worsening of anxious/depressed symptoms, only for adolescents with higher initial levels of anxious/depressed behavior. Therefore, our data support the latter assertion posed above: that higher initial levels of symptoms make it difficult to engage in the cognitively demanding primary and secondary control coping and instead encourage disengagement coping. Disengagement is often found to be associated with symptoms and is considered to be an ineffective coping strategy in most cases—our data suggest that this may be especially true for internalizing symptoms, as there was no interaction between disengagement coping and aggressive behavior.
This coping-symptom specificity is interesting to disentangle conceptually. Why would disengagement coping be particularly relevant for anxious/depressed behavior? Because a core component of the clinical syndrome of anxiety involves avoidance (and depression to a large extent as well), this type of coping may be particularly detrimental for individuals with a propensity to disengage. The salience of primary and secondary control coping for aggressive behavior can also be understood conceptually by considering some of the core deficits found in individuals with clinically significant aggressive problems. Undercontrolled behavior such as that associated with conduct disorder is often associated with poor problem solving abilities and poor emotional regulation skills (Cole et al., 1994), which are both elements of primary control coping. It is crucial to begin to disentangle this specificity issue in order to develop maximally effective interventions for at-risk adolescents.
Another possible indicator of distress from a stressor would be the involuntary engagement strategies we refer to as involuntary stress reactivity in this paper. Therefore, we also examined the interactions between coping and involuntary stress reactivity in predicting changes in symptoms over time. There was a significant interaction of primary control coping and involuntary stress reactivity in predicting aggressive behavior over time. Adolescents’ use of primary control coping with family stressors showed a buffering effect only under conditions of lower initial levels of involuntary stress reactivity. This suggests that involuntary reactivity to poverty-related family stress interferes with efficacious primary control coping. No other interactions of coping and involuntary stress reactivity on changes in symptoms were significant, although there was a trend toward an interaction between disengagement coping and involuntary stress reactivity. Why would only primary control interact with involuntary stress reactivity? Because emotional regulation is part of primary control coping (Connor-Smith et al., 2000), it is plausible that primary control coping is enacted in response to the emotional and physiological arousal comprising involuntary stress reactivity, and therefore may be especially relevant to the management of involuntary stress reactivity.
Finally, the efficacy of primary control coping vis á vis anxious/depressed behavior appears to depend in part on the degree of stress faced by the adolescent. Primary control coping served to protect against subsequent symptoms across the board, but the magnitude of the effect was much greater for those under higher amounts of poverty-related family stress. Of course another interpretation—that of stress buffering—is also possible. However, the chronic nature of poverty in this sample suggests that stress may well be the moderator here rather than coping. Three time points of data are necessary to sort out which plausible interpretation is most accurate.
Predictors of Coping Over Time
We also examined how family stress, involuntary stress reactivity, and psychological symptoms predicted adolescents’ coping skills over time. Our results indicated that the single, most consistent predictor of future coping skills was prior coping. This is highly consistent with the few studies that have examined predictors of coping over time. In Sandler et al. (1994) prior coping was the only predictor of subsequent coping in their sample; they did not find that symptoms predicted coping. Similarly, Holahan et al. (1997) examined whether depressive symptoms would predict positive or negative coping over time and found no evidence supporting either. Thus, it appears that the cross-sectional data showing significant associations between coping and symptoms most likely reflects the conceptual proposition inherent in most coping theory; that the directionality is from coping to symptoms and not the reverse. Thus, data are accumulating to show that coping contributes to or buffers us psychologically from stress, and that coping is not simply an index of current well-being.
Limitations and Future Directions
Several limitations apply to this study. The sample size was small, thus null findings may be artifacts of low power, rather than disconfirmations of hypotheses. However, we ensured that we had adequate power to detect medium and large effects. In addition, we believe that the ability to study symptoms over time controlling for prior symptoms in a sample of adolescents struggling to cope with poverty-related family stress adds preliminary information to the literature that can be extended in future research with larger samples. In addition, we found a number of main and interactive effects of key variables in predicting symptoms and coping over time, suggesting that there may be some very powerful effects of stress and coping with poverty-related family stress among this population.
Adolescents were the sole reporters in this study, which raises the specter of common method variance. We acknowledge that some of the relations between variables may be inflated due to common method variance. However, we made use of prospective data to control for reporting styles and controlled for initial symptom/coping levels so that analyses accounted for changes in symptoms/coping. These findings require replication to determine the extent to which these results can generalize beyond poor youth from rural New England. In particular, this sample was also highly racially homogeneous. It is possible that predictors of adjustment and coping may differ for adolescents from nonmajority populations. Gomel et al. (1998), for example, found that their models of family adaptation to economic hardship fit quite differently for Caucasian, African American, and Latina participants. Gutman and Eccles (1999), however, found no differences between African American and Caucasian participants in their models of the influence of financial strain on family relationships and adolescent academic achievement. Thus, it is crucial to study these constructs and models with diverse samples of adolescents, both to ensure adequacy of the constructs for diverse teens and to examine cross-cultural similarities and differences in patterns of association among poverty-related stress, coping, and adjustment.
It will also be important to compare the results of the current study with examinations of how youth cope with economic stressors in more urban settings, as the stresses and resources may vary considerably in rural and urban settings. For example, noise, crowding, pollution, crime, and residential turnover comprise stressors more frequently encountered by poor urban families (e.g., Wandersman and Nation, 1998). On the other hand, insularity, lack of insurance, transportation problems, limited access to services, and limited employment opportunities are chief concerns for many rural families (e.g., Hoyt et al., 1997; St. Lawrence and Ndiaye, 1997). Therefore, for urban families there may be more readily identifiable options for problem solving about finances, including access to a variety of services and employment options. Urban adolescents, for example, can sometimes find part-time jobs to help out with family finances, as some of the more successful adolescents in Elder and Caspi's (1988) studies did. Similarly, urban adolescents generally have better access to community centers and other such agencies where they may locate helpful adults to aid with problem solving and emotional modulation. Adolescents living in rural settings like the one in this study may have to rely more on secondary control strategies in the absence of access to primary control resources such as these. On the other hand, poor rural families can often rely on connections and networks within their communities and informal “services” or systems such as bartering. Comparing patterns of adjustment to economic stress in rural and urban families is an exciting avenue for future research.
Conclusions and Implications
There are several implications of these data for research and interventions. In terms of treatments for youths struggling with these types of issues, perhaps teaching coping skills will not be sufficient. In order for youths to be able to cope effectively with such stressors, the first step is likely for them to learn how to manage their involuntary stress reactivity and psychological symptoms. This is clearly consistent with the cognitive-behavioral treatments for depression, which incorporate teaching trainable coping skills in addition to affect management (e.g., Clarke et al., 1990).
This study also highlights the influence of adolescents’ family environment; we found a main effect of stress on anxious/depressed behavior over time, even controlling for symptoms. This adds to a growing literature showing the power of stress to contribute to psychopathology (Caspi et al., 2003). The study also highlights the influence of individual, biological variables; involuntary stress reactivity appears to be a powerful determinant of how one copes and how well one copes, especially with regard to aggressive behaviors. Additional research exploring the interplay between involuntary and effortful stress responses is needed.
Finally, this study adds to the small but growing literature on the effects of poverty-related family stress on children and how they regulate that stress. It is clear that stress and coping predict symptoms over time. However, these results do not suggest that coping is driven by symptoms; thus the association between symptoms and coping is not an artifact of symptoms. Rather, the direction appears to travel from stress and coping to symptoms. In light of other research showing reciprocal relations between stress and symptoms over time, (e.g., Kim et al., 2003) our findings suggest that stress and coping may be processes that operate very differently from each other. Given that eradicating poverty has proven to be rather difficult, preventing psychopathology by teaching how to cope with poverty's stress and manage one's involuntary stress reactivity may be a viable step toward breaking the cycle of poverty.
REFERENCES
Achenbach, T. M. (1991). Manual for the Youth Self-Report and 1991 Profile. University of Vermont Department of Psychiatry, Burlington, VT.
Aiken, L. S., and West, S. G. (1991). Multiple regression: Testing and interpreting interactions. Sage Publications, Thousand Oaks, CA.
Caspi, A., Sugden, K., Moffitt, T. E., Taylor, A., Craig, I. W., Harrington, H., et al. (2003). Influence of life stress on depression: Moderation by a polymorphism in the 5-HTT gene. Science 301: 386–389.
Chang, E. C., and Strunk, D. R. (1999). Dysphoria: Relations to appraisals, coping, and adjustment. J. Couns. Psychol. 46: 99–108.
Clarke, G., Lewinsohn, P., and Hops, H. (1990). Adolescent Coping with Depression Course. Castalia Publishing, Eugene, OR.
Cleveland, H. H. (2003). Disadvantaged neighborhoods and adolescent aggression: Behavioral genetic evidence of contextual effects. J. Res. Adolesc. 13: 211–238.
Cole, P. M., Zahn-Waxler, C., and Smith, K. D. (1994). Expressive control during a disappointment: Variations related to preschoolers’ behavior problems. Dev. Psychol. 30: 835–846.
Compas, B. E., Connor, J. K., Harding, A., Saltzman, H., and Wadsworth, M. (1999). Getting specific about coping: Effortful and involuntary responses to stress in development. In Lewis, M., and Ramsey, D. (eds.), Soothing and Stress. Cambridge University Press, New York, pp. 229–256.
Compas, B. E., Connor-Smith, J. K., Saltzman, H., Thomsen, A. H., and Wadsworth, M. E. (2001). Coping with stress during childhood and adolescence: Progress, problems, and potential in theory and research. Psychol. Bull. 12: 87–127.
Compas, B. E., Forsythe, C. J., and Wagner, B. M. (1988).Consistency and variability in causal attributions and coping with stress. Cogn. Ther. Res. 12: 305–320.
Conger, R. D., and Conger, K. J. (2002). Resilience in Midwestern families: Selected findings from the first decade of a prospective, longitudinal study. J. Marriage Fam. 4: 361–373.
Conger, R. D., Conger, K. J., Elder, G. H., Lorenz, F. O., Simons, R. L., and Whitbeck, L. B. (1993). Family economic stress and adjustment of early adolescent girls. Dev. Psychol. 29: 206–219.
Connor-Smith, J. K., Compas, B. E., Wadsworth, M. E., Thomsen, A. H., and Saltzman, H. (2000). Responses to stress in adolescence. Measurement of coping and involuntary stress responses. J. Consult. Clin. Psychol. 68: 976–992.
Ebata, A. T., and Moos, R. H. (1994). Personal, situational, and contextual determinants of coping in adolescents. J. Res. Adolesc. 4: 99–125.
Eisenberg, N., Fabes, R. A., and Guthrie, I. (1997). Coping with stress: The roles of regulation and development. In Sandler, I. N., and Wolchik, S. A. (eds.), Handbook of Children's Coping with Common Stressors: Linking Theory, Research, and Intervention. Plenum, New York, pp. 41–70.
Elder, G. H., and Caspi, A. (1988). Economic stress in lives: Developmental perspectives. J. Soc. Issues 44: 25–45.
Gomel, J. N., Tinsley, B. J., Parke, R. D., and Clark, K. M. (1998). The effects of economic hardship on family relationships among African American, Latino, and Euro-American families. J. Fam. Issues. 19: 436–467.
Grant, K. E., Compas, B. E., Stuhlmacher, A. F., Thurm, A. E., McMahon, S. D., and Halpert, J. A. (2003). Stressors and child and adolescent psychopathology: Moving from markers to mechanisms of risk. Psychol. Bull. 129: 447–466.
Gunthert, K. C., Cohen, L. H., and Armeli, S. (2002). Unique effects of depressive and anxious symptomatology on daily stress and coping. J. Social Clin. Psychol. 21: 583–609.
Gutman, L. M., and Eccles, J. S. (1999). Financial strain, parenting behaviors, and adolescents’ achievement: Testing model equivalence between African American and European American single- and two-parent families. Child Dev. 70: 1464–1476.
Haaga, D., and Beck, A. (1992). Cognitive therapy. In Paykel, E. S. (ed.), Handbook of Affective Disorders (2nd ed.). Guilford Press, New York, NY, pp. 511–523.
Holahan, C. J., Moos, R. H., Holahan, C. K., and Brennan, P. L. (1997). Social context, coping strategies, and depressive symptoms: An expanded model with cardiac patients. J. Pers. Soc. Psychol. 7: 918–928.
Hollingshead, A. B. (1975). Four factor index of social status. Unpublished manuscript. Yale University, Department of Sociology.
Hoyt, D. R., Conger, R. D., Valde, J. G., and Weihs, K. (1997). Psychological distress and help seeking in rural America. Am. J. Community Psychol. 25: 449–470.
Kagan, J., Snidman, N., and Arcus, D. M. (1995). Initial reactions to unfamiliarity. Curr. Dir. Psychol. Science. 1: 171–174.
Kim, K. J., Conger, R. D., Elder, G. H., and Lorenz, F. O. (2003). Reciprocal influences between stressful life events and adolescent internalizing and externalizing problems. Child Dev. 74: 127–143.
Lazarus, R. S., and Folkman, S. (1984). Stress, Appraisal, and Coping. Springer, New York.
Lewinsohn, P. M., and Talkington, J. (1979). Studies on measurement of unpleasant events and relations with depression. Appl. Psychol. Meas. 3: 83–101.
Matthews, G., and Wells, A. (1996). Attentional processes, dysfunctional coping, and clinical intervention. In Zeidner, M., and Endler, N. S. (eds.), Handbook of Coping: Theory, Research, Applications, pp. 573–601.
McLoyd, V. C. (1998). Socioeconomic disadvantage and child development. Am. Psychol. 53: 185–204.
McLoyd, V. C., Jayaratne, T. E., Ceballo, R., and Borquez, J. (1994). Unemployment and work interruption among African American single mothers: Effects on parenting and adolescent socioemotional functioning. Child Dev. 65: 562–589.
McMahon, S. D., Grant, K. E., Compas, B. E., Thurm, A. E., and Ey, S. (2003). Stress and psychopathology in children and adolescents: Is there evidence of specificity? J. Child Psychol. Psychiatry: Annu. Res. Rev. 44: 107–133.
Rothbart, M. K., Posner, M. I., and Hershey, K. L. (1995). Temperament, attention, and developmental psychopathology. In Cicchetti, D., and Cohen, D. (eds.), Developmental Psychopathology: Vol. 1. Theory and Methods. Wiley, New York, pp. 315–340.
Rudolph, K. D., Dennig, M. D., and Weisz, J. R. (1995). Determinants and consequences of children's coping in the medical setting: Conceptualization, review, and critique. Psychol. Bull. 11: 328–357.
Sandler, I. N., Tein, J., Mehta, P., Wolchik, S., and Ayers, T. (2000). Coping efficacy and psychological problems of children of divorce. Child Dev. 71: 1099–1118.
Sandler, I. N., Tein, J., and West, S. G. (1994). Coping, stress, and the psychological symptoms of children of divorce: A cross-sectional and longitudinal study. Child Dev. 65: 1744–1763.
St. Lawrence, J. S., and Ndiaye, S. M. (1997). Prevention research in rural communities: Overview and concluding comments. Am. J. Commun. Psychol. 25: 545–562.
Tolan, P. H., Gorman-Smith, D., Henry, D., Chung, K., and Hunt, M. (2003). The relation of patterns of coping of inner-city youth to psychopathology symptoms. J. Res. Adolesc. 12: 423–449.
Turkheimer, E., Haley, A., Waldron, M., D’Onofrio, B., and Gottesman, I. I. (2003). Socioeconomic status modifies heritability of IQ in young children. Psychol. Sci. 14: 623–628.
Valliant, G. (1977). Adaptation to Life. Little Brown, Boston.
Wadsworth, M. E., and Compas, B. E. (2002). Coping with economic strain and family conflict: The adolescent perspective. J. Res. Adolesc. 12: 243–274.
Wadsworth, M. E., Rieckmann, T., Benson, M. A., and Compas, B. E. (2004). Coping and responses to stress in Navajo adolescents: Psychometric properties of the Responses to Stress Questionnaire. J. Commun. Psychol. 32: 391–411.
Wandersman, A., and Nation, M. (1998). Urban neighborhoods and mental health: Psychological contributions to understanding toxicity, resilience, and interventions. Am. Psychol. 53: 647–656.
Wegner, D. M. (1994). Ironic processes of mental control. Psychol. Rev. 101: 34–52.
Weiss, B., Susser, K., and Catron, T. (1998). Common and specific features of child psychopathology. J. Abnorm. Psychol. 107: 118–127.
Author information
Authors and Affiliations
Corresponding author
Additional information
Assistant Professor, University of Denver. Received PhD from University of Vermont. Research interests include the effects of poverty on family functioning, developmental issues in stress and coping, and developmental psychopathology
Doctoral student in Clinical Psychology, University of Denver. Research interests include close relationship influences on adolescent development and psychopathology.
Rights and permissions
About this article
Cite this article
Wadsworth, M.E., Berger, L.E. Adolescents Coping with Poverty-Related Family Stress: Prospective Predictors of Coping and Psychological Symptoms. J Youth Adolescence 35, 54–67 (2006). https://doi.org/10.1007/s10964-005-9022-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-005-9022-5