
Abstract
Neuroimaging studies of typically developing children and adolescents have provided valuable information on global and regional developmental trajectories of brain development. As these studies become larger and population-based, they are generating an intersection between the fields of developmental neuroscience and epidemiology. However, few of these studies have adequately probed the contribution of multiple environmental and genetic factors on brain development. Studies designed to optimally evaluate the role of multiple environmental and genetic factors on brain development require both large sample sizes and the prospective collection of multiple environmental factors. The Generation R Study is a large, prospective, prenatal-cohort study of nearly 10,000 children that began in 2002 in Rotterdam, the Netherlands. In September of 2009, 6–8 year old children from the Generation R Study were invited to participate in a magnetic resonance imaging component of the study. We provide an overview of the study design and experience for the first 801 children recruited for the neuroimaging component of the study. The protocol includes a 1-h neuropsychological assessment using the NEPSY-II, a mock scanning session, and a neuroimaging session that includes high-resolution structural, diffusion tensor, and resting-state functional MRI sequences. Image quality has been good to excellent in over 80 % of the children to date. The infusion of imaging into the Generation R Study will set the stage for evaluating the role of multiple environmental and genetic factors in both typical and atypical neurodevelopment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The formation of the human brain involves a complex orchestration of events that begins as the first cell differentiates from ectodermal into neural tissue during the second week following conception [1, 2]. These early events are followed by a cascade of neurodevelopmental processes involving growth, migration, and pruning. Active processes of growth include symmetric and asymmetric cell division, cell differentiation and growth, neuronal migration, dendritic arborization, synaptogenesis, gyrification, and myelinization [3–6]. Brain development also includes active processes of elimination, including apoptosis and dendritic and synaptic pruning [7, 8]. Developmental neuroscience, whether through micro or macro approaches, is directed at understanding the neurobiological mechanisms behind these developmental processes.
While brain development is under tight genetic control, environmental, epigenetic, and stochastic processes also play a crucial role in its formation. In spite of the magnitude of the human genetic code, there is not enough genetic information to code for each location and connection of the billions of neurons and trillions of synapses that form during development [9]. Thus, the development of brain connectivity occurs with considerable redundancy; through the overproduction of neurons and synaptic connections that, following formation, undergo experience-modulated selective pruning [4, 5]. Optimal pruning results in the elimination of neurons and connections that do not contribute significantly to the overall efficiency of the brain. This overproduction of neurons and synapses with subsequent pruning provides a mechanism for resilience between environmental insults and unfavorable stochastic events. It also accounts for the considerable inherent plasticity of the developing brain.
There are a myriad of environmental determinants that could influence human brain development [10]. The emerging field of population neuroscience is directed at addressing questions surrounding the combined effects of environmental and genetic factors on human brain development [11]. Similar to studies that attempt to elucidate the genetic underpinnings of complex disorders, studies that explore the relationship between multiple environmental factors and neurobiology must not only consist of very large sample sizes, but also meticulously quantified data from the environment. This becomes especially important when attempting to examine the complex interactions between genes, environment, and the developing brain. Studies such as the Generation R Study are an extremely valuable source for exploring the interactions of genes and environment on neurobiological development.
The Generation R Study is an ongoing population-based prospective cohort study that began in 2002 with the recruitment of nearly 10,000 pregnant women in Rotterdam, the Netherlands [12, 13]. The primary aim of the study is to describe normal and abnormal patterns of growth and development, including fetal and postnatal brain development. Multiple prospective longitudinal measures crossing multiple domains of health and development have been obtained as a part of the Generation R Study [12, 14]. Measures such as pre- and postnatal diet, maternal and child infections, family function, prenatal substance use, home environment, and multiple measures of behavior, temperament, and attachment have been meticulously collected. One of the early measures of brain development within the Generation R was obtained using fetal ultrasound measures. Ultrasound imaging of the head, biparietal diameter, ventricular size, and cerebellar diameter was performed at least once during fetal life in 8,313 children [15]. In addition, postnatal fetal ultrasound measures were obtained at 1 month in 778 children [16]. Finally, cord and maternal blood samples have been collected for genetic analyses.
The infusion of brain magnetic resonance imaging (MRI) in sub-populations of Generation R began in September 2009 with the children being between 6 and 8 years of age. The Generation R neuroimaging component was initially directed at studying specific subpopulations within the Generation R cohort. These subpopulations can be characterized by neurodevelopmental factors related to either prenatal exposures or behavioral problems or traits in young children (Table 1). A dedicated wide-bore GE 3 Tesla scanner has recently been acquired and beginning in early 2013 all children will be invited to participate in the MR neuroimaging component of the Generation R Study. The goal of this paper is to introduce the study design and imaging protocol for the first wave of neuroimaging data collection within the Generation R Study.
Study design
Subjects
The children who are recruited are participants of the Generation R Study. An overview of the Generation R Study design and population is described in detail by Jaddoe et al. [12]. In brief, all pregnant women who were living within a well-defined region in Rotterdam (defined by postal codes) between April 2002 and January 2006 were invited to participate in the study. A total of 9,778 pregnant mothers provided informed consent and were recruited, with their unborn child, as members of the Generation R cohort. Of these mothers, a total of 6,691 (69 %) were enrolled during early pregnancy, 1,918 (19 %) during mid-pregnancy, 271 (3 %) during late pregnancy, and 898 (9 %) mothers were recruited at birth. The children and their parents have been followed prospectively with data collection occurring at multiple time points [12]. The most recent completed visit for the Generation R Study took place when the children were between 5 and 6 years of age and included nearly 7,000 actively participating children. The children are currently being invited for the 9-year follow-up visit.
Rotterdam is ethnically diverse, with 52 % of the population being non-Dutch. Recruitment into Generation R reflects this diversity. Of the 9,778 mothers, 62 % were Dutch or other-European, 8 % Surinamese, 8 % Turkish, 7 % Moroccan, 4 % Dutch Antillean, 3 % of Cape Verdian descent, and 8 % other [17].
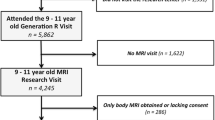
The structural and functional neuroimaging wave started in September of 2009 following the approval by the Medical Ethical Committee (METC) to scan children 6 years of age and older. The study has been performed in accordance with the 1964 Declaration of Helsinki and it’s later amendements. The inclusion criteria were based on specific criteria for recruitment into the subgroups shown in Table 1. Exclusion criteria included contraindications for the MRI procedure (i.e., pacemaker, ferrous metal implants), severe motor or sensory disorders (deafness or blindness), neurological disorders (i.e., seizures or tuberous sclerosis), and moderate to severe head injuries with loss of consciousness, and claustrophobia. A total of 801 children were recruited between September 2009 and February 2012 (Fig. 1). The imaging is ongoing with new invitations mailed to families inviting them to participate and following-up on families who have not yet come to the center. We are currently performing MRI scans at an average of 7.5 children per week, however, this will increase as we will begin a second wave of neuroimaging with plans to invite all of the approximately 7,000 children within the Generation R Study for an MRI scan.

Flow diagram for recruitment into the imaging component of the Generation R Study
Neuropsychological assessment
The neuropsychological battery consists of an array of subtests from the Dutch version of the NEPSY-2 [18]. The subtests chosen and their description are presented in Table 2. The subtests were chosen to tap into five specific domains, including: attention and executive function, language, memory and learning, sensorimotor function, and visuospatial processing. The battery takes no more than 60 min and is administered in one of four randomly selected counterbalanced orders. In addition to the NEPSY-2, handedness is measured using a modified version of the Edinburgh Handedness Inventory [19].
While most children participate in both the imaging and the neuropsychological assessment, some children or families opt only to participate in the neuropsychological battery (Fig. 1). The neuropsychological battery is typically planned on the same day as the scanning, although when this is not possible it is performed on a different day and only rarely during a home visit. Of the 608 children who participated in the MRI component of the study, a total of 594 (97.7 %) also received a NEPSY-2.
Mock scanning session
Prior to the actual MRI scanning session, the children participate in a mock scanning session to introduce them to the scanning environment. The mock scanner simulates the most important aspects of the actual scanning session, including the feeling of being within the MR bore, wearing headphones that plays recorded gradient sounds, and the ability to watch a forward-projected film via a mirror positioned on the head coil. The purpose of the mock scanning session is to provide an introduction to the scanning environment and to offer the opportunity for the child or parent to opt out of the procedure before going to the actual MRI scanner.
The children and their parents are asked several questions over their anxiety level and whether they thought it was fun or not. These questions are asked before the mock scanning session, immediately after the mock scanning session, and immediately after the actual MRI scan. If at any point the child responds to a visual analog scale that they are either too scared or that they find it not at all fun, then they do not progress to the actual MRI scanning session. The parents and researchers also rate the child’s fear along the same visual analog scale and if they feel that the child is too scared then the child does not progress to the MRI session. The visual analog scale is similar to that developed by Durston et al. [20].
Magnetic resonance imaging
MR images are acquired on a 3 Tesla scanner (General Electric Discovery MR750, Milwaukee, MI, USA) using an 8-channel head coil for signal reception. Care is taken so that children are comfortable in the scanner and soft cushions were used to assist with head immobilization. The children were able to watch a film of their choice during the structural MRI & DTI acquisitions. The film is projected onto a screen at the front of the scanner and the children watch though forward-directed mirrors. The film was only shown during the high-resolution structural and diffusion tensor imaging sequences. The film and sound was turned off during the resting state functional magnetic resonance imaging sequence (rs-fMRI) and the children were asked to close their eyes and to think of nothing in particular. All MRI sequences scanned the entire head (brain and cerebellum).
Structural imaging
Following a 3-plane localizing and coil intensity calibration scans, a high-resolution T1-weighted inversion recovery fast spoiled gradient recalled (IR-FSPGR) sequence is obtained with the following parameters: TR = 10.3 ms, TE = 4.2 ms, TI = 350 ms, NEX = 1, flip angle = 16°, readout bandwidth = 20.8 kHz, matrix 256 × 256, imaging acceleration factor of 2, and an isotropic resolution of 0.9 × 0.9 × 0.9 mm3. The total scan time for the T1 is 5 min 40 s. In addition, an axial fast spin echo (FSE) proton density (PD) weighted image is acquired with the following parameters: TR = 13,500 ms, TE = 6.7 ms, echo train = 12, readout bandwidth = 62.5 kHz, NEX = 1, matrix 256 × 256 with a voxel resolution of 0.9 × 0.9 × 1.0 mm3. The total scan time for the PD image is 3 min 50 s.
Diffusion tensor imaging (DTI)
The DTI sequence consists of a 35 direction echo planar imaging (EPI) sequence using the following sequence parameters: TR = 11,000 ms, TE = 8 ms, NEX = 1, flip angle = 90, b = 0 and 1,000 s/mm2, matrix 256 × 256 and an isotropic voxel resolution of 2.0 × 2.0 × 2.0 mm3. The b = 0 s/mm2 is acquired 3 times. The total scan time for the DTI sequence is 7 min 40 s.
Resting state functional magnetic resonance imaging (rs-fMRI)
Resting-state fMRI utilized a gradient-echo blood oxygen level dependent (BOLD) EPI sequence with a TR = 2,000 ms, TE = 30 ms, flip angle = 85°, matrix 64 × 64 and voxel resolution of 3.6 × 3.6 × 4.0 mm3. The total duration of the rs-fMRI session is 5 min. 20 s. (160 TRs) or 8 min. 20 s. (250 TRs). The longer rs-fMRI session was initially used to assess the length of time needed for an adequate rs-fMRI protocol. The children are asked to keep their eyes closed during the rs-fMRI sequence and to think about nothing in particular.
Ethics
The approval to scan typically developing children 6 years of age and older was granted by the METC at the Erasmus Medical Centre. A radiologist reviews all the structural MRI scans from the children. The consent form states that the presence of potentially serious incidental findings will be reported to the parents accompanied with expert advice. The METC approved the project with the condition that if the parents are not in accord with learning about any potential serious incidental findings on the MRI scan, then the child is unable to participate in the MRI session.
Image processing pipeline
Images are transferred from the GE console to the server and stored on a RAID system. The image-processing pipeline has been developed to constitute both a standard processing stream as well as user-specific branch points. The standard stream currently consists of a combination of freely available packages and MATLAB-based programs developed in-house. The structural imaging data are currently being analyzed with FreeSurfer (http://surfer.nmr.mgh.harvard.edu/) [21]. Diffusion tensor imaging (DTI) is processed with a combination of FSL (http://www.fmrib.ox.ac.uk/) [22, 23] and in-house MATLAB (MathWorks, Inc. Natick, Massachusetts) programs to assess for white matter ‘potholes’ [24]. Pre-processing of the rs-fMRI data is performed using a combination of Analysis of Functional NeuroImages (AFNI) (http://afni.nimh.nih.gov/afni/) [25] and FSL [22]. The rs-fMRI time series undergo time shifting and motion correction using AFNI. The motion correction parameters within a run are outputted to a text file and analyzed via a Matlab-based program to calculate head movement parameters.
Spatial normalization into MNI space is performed in three steps using FSL. First, 6-parameter affine transformation parameters are obtained, but not applied, to register each child’s motion corrected rs-fMRI to their high-resolution structural image. The structural MRI images undergo a 12-parameter affine transformation into MNI space and the transform parameters are then applied to register the rs-fMRI images. The images are then resampled to 2 mm isotropic voxels. Once pre-processed, the rs-fMRI images can be further processed using independent component analyses (ICA) or seed region correlation analyses (SRCA). The ICA analyses are performed using GIFT [26] or Melodic [27]. The SRCA is performed using an in-house MATLAB based program [28].
Rates of participation
A flow diagram showing the rates of participation is presented in Fig. 1 and the demographics of participants and non-participants are presented in Table 3. From the 1,153 families with whom contact was made, a total of 238 (20.7 %) declined to participate. Comparing those who consented versus those who declined participation, there were no significant differences in sex of the child or in the educational status or the age of the mother and father/partner. In addition, there were no differences in the household income between those who consented and those who declined. However, those who declined were more likely to be mothers with a national origin outside Europe (50.4 % of those who declined were non-Europeans versus 41.5 % who agreed, χ2 = 6.0, p = 0.01) and biological fathers with a national origin outside of Europe (50.4 % of those who declined were non-Europeans vs. 43.1 % who agreed, χ2 = 4.0, p = 0.04).
Within families who declined participation, 17 % of the parents were willing to participate but the child declined participation. There were no differences in either the total problem score on the Child Behavior Checklist, or differences on the internalizing or externalizing scales between children who participated and those who declined. While there were a number of children who sustained mild head injuries, no children were excluded as a result of severe head injuries or tumors. One child with a seizure disorder was excluded from participation. Children exposed to maternal smoking during pregnancy were less likely to participate, whereas children with a diagnosis of ADHD were more likely to participate (Table 4). A total of 801 families came to the imaging center and signed the consent form.
Demographics
The demographic information for the children and families who consented for the study are presented in Table 3. The mean age of the children who received an MRI scan (n = 608) was 92.0 months (SD 11.2 months). The mean age of the children at the time of the NEPSY-II (n = 744) was 91.7 months (SD 11.0 months). A total of 720 of the 744 children (97 %) had the NEPSY-II performed within three months of the imaging session of which 689 of the 744 children (93 %) had the NEPSY-II performed on the same day as the imaging session.
The ethnic distribution of the children who consented for the MRI study had an over-representation of Dutch/European participants compared to the Generation R cohort [17] and the demographics of Rotterdam [29]. The current ethnic distribution of Rotterdam includes 58.7 % Dutch and other European inhabitants, 6.5 % Moroccan, 7.8 % Turkish, 8.7 % Surinamese, 3.6 % Dutch Antilles, and 2.5 % Cape Verdian. The numbers and percentages of the ethnic distribution for the imaging and NEPSY-II sample are shown in Table 3.
Children’s experience
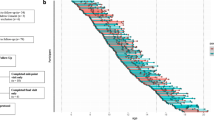
The vast majority of children were not scared by the procedure (Fig. 2a). A repeated-measures ANOVA found that children rated themselves as being less scared than the rating of the child by the parent or by the researcher (F2,2048 = 25.6, p < 0.0001: Fig. 2b). In addition, there was a main effect of time (Fig. 2b), with children experiencing decreasing levels of anxiety as they progressed through the mock scanning session to the actual MRI scan (F2,4096 = 59.5, p < 0.0001). There was no interaction between rater (parent, child, and researcher) and time (F4,4096 = 2.0, p = 0.1). A total of 109 children (15.2 %) decided to stop during the mock scanning session. Children who were exposed prenatally to SSRI’s were more likely to drop out compared to children not exposed to SSRIs (Table 4).

The children’s level of anxiety as they progress from the mock scanner to the actual scanning session. a The children’s rating of the experience during three different time points. b The level of anxiety for the children, their parent, and the researcher at three different time points
Image quality
Structural MRI
All the T1 and PD images were visually inspected and given a quality rating based on movement or other artifacts. The ratings were based on a six point Likert-scale and ranged from 5 (excellent), 4 (very good), 3 (good), 2 (fair), 1 (poor), and 0 (unusable). While the images that are poor are also likely to be unusable for most analyses, an unusable rating refers to major problems such as artifacts caused by the scanner hardware or the subject moved between scans such that a portion of the brain was outside of the field of view.
Approximately 80 % of the T1 scans have been rated as between good to excellent quality to date (Table 5). If the T1 image acquisition was determined to be fair, poor, or unusable, the scan was repeated in place of the PD image. The T1 was repeated in 59 children, with improvement in scan quality in 33 of the 59 children. A scan rating of good to excellent was found in 507 of the children. A Spearman rank order correlation between the T1 rating and the PD rating was 0.56 (p < 0.0001).
There were no serious CNS abnormalities identified on any of the 608 MRI scans obtained from the children.
Diffusion tensor imaging
The diffusion tensor imaging sequence took place following the T1 image and prior to the PD image. Children who remained still for both the T1 and PD sequences had little motion related artifacts during the 7 min 40 s DTI scan. A total of 571 children completed the DTI paradigm. To obtain an estimate of motion during the DTI scan, the sequences were motion corrected and the transformation matrices for each volume were quantified. While artifacts can influence the motion correction algorithm, we found that the majority of the subjects had good to excellent scan quality (Table 6).
Resting-state fMRI
The rs-fMRI was the last sequence of the MRI session. The movie was turned off during the rs-fMRI and the children were told to close their eyes and think of nothing in particular. In spite of the movie being turned off, the majority of children were able to keep quite still during the fMRI paradigm (Table 6). Over half of the children had less than 2 mm maximum head movement and approximately three-quarters had less than 3 mm maximum head movement. Using a typical cut-off of 3 mm total head movement would result in 399 of the 547 children (73 %) of the children with usable data.
Discussion
Pediatric population-based neuroimaging lies at the intersection between developmental neuroscience and epidemiology. Epidemiology is directed at understanding the determinants and characteristics of health in a population. Applied to neuroscience, the health states and events are those determinants and characteristics that lead to optimal brain development and thus optimal brain health. It is important to understand which determinants and characteristics lead to disrupted or inefficient brain development as these may contribute to an individual’s susceptibility to cognitive, neurological, or psychiatric disorders. These determinants and characteristics are driven through genetic, environment, and the interplay between genetic and environmental factors.
Of the 30,000 genes in the human genome, approximately one-third are expressed only in the development of the central nervous system [30]. Thus it is not surprising that measures such as cortical thickness and global and regional brain volume are highly heritable [31, 32]. Yet with at least 100 million neurons and 100 trillion synapses in the human brain [9], there is a considerable interplay between genetic, environmental, and stochastic processes taking place during neurodevelopment. Optimal neurodevelopment allows for sufficient proliferation and selective elimination of neurons and synapses that do not contribute to the overall efficiency of the brain. Such optimal growth would allow the brain to better overcome environmental insults and less favorable stochastic processes.
Less optimal early neurodevelopment, as could occur through a myriad of different events (i.e., maternal malnutrition, substance use, infection, maternal diabetes) could interfere with the efficient orchestration of brain function and increase the risk for the later development of cognitive, neurological, or psychiatric disorders. The number of potential environmental variables that could interact with brain development is legion. Thus, studying the relationship between environmental factors and neurodevelopment requires large numbers of subjects, with multiple measures collected over time in these subjects. Such a study in essence forms a merging between the fields of developmental neuroscience and epidemiology.
It is within this framework that we introduce the infusion of neuroimaging into the population-based Generation R Study. The Generation R Study [12], with its large sample size, its initiation during fetal life, the spectrum of multimodal measures obtained, and the inclusion of all children within a region serves as the perfect source for the intersection between developmental neuroscience and epidemiology. Multiple measures of maternal and child health (including mental health) have been prospectively collected beginning in early pregnancy to the present (the children are currently between 6 and 10 years of age). Already studies within the Generation R cohort using prenatal ultrasound measures of brain development have shown a link with environmental variables such as maternal stress [33], smoking during pregnancy [34], and cannabis use during pregnancy [35]. In addition to numerous other questions, the use of MRI provides the opportunity to test with much finer resolution whether these brain changes continue into childhood or whether they are molded or erased through the inherent plasticity of the early developing brain.
The primary goal of this paper is to describe the recruitment procedure and the initial experience for the 6–8 year old children involved in the imaging component of the Generation R Study. Between September 2009 and February 2012 a total of 801 children and their families consented to participate. From this group, a total of 744 children performed the NEPSY-II neuropsychological assessment and 608 children underwent neuroimaging (Fig. 1).
Approximately 21 % of the families who were called decide that they did not want to participate in the imaging component. The participation rate is higher than in other large population-based studies [36], likely secondary to the children being involved in an ongoing, longitudinal prenatal cohort study. The experience of the children and their families during the imaging session was reported to be very good. While typical worries and fears are highly prevalent in school age children [37], the vast majority of children participating in the imaging protocol were not frightened by either the MRI environment or scanning procedure (Fig. 2a). Approximately 14 % of the children or their parents did decide to stop the study either prior to or immediately following the mock scanning session. There were no differences in demographic measures between those who stopped prior to the MRI scan, however, children who were exposed prenatally to SSRI’s were more likely to drop out compared to children not exposed to SSRIs (Table 4). Similar to the findings of Durston et al. [20] we found that the use of the mock scanner was beneficial in reducing the level of anxiety for both child and parents alike (Fig. 2b).
The ability to obtain quality scans in these young, school age children was quite good. The quality of the high-resolution T1 scans were rated between good and excellent in 83 % of the children. The PD imaging was rated between good and excellent in 80 % of the cases. The rs-fMRI sequence was the last sequence and the movie was turned off and the children were asked to close their eyes and think of nothing in particular. The quality of the rs-fMRI had 73 % of the scans with less than 3 mm maximum movement (Table 6).
In addition to several important smaller studies [38–40], there are several large developmental neuroimaging studies that have greatly contributed to our understanding of global and regional differences in brain development [41–44]. One of the earliest and largest studies began in the early 1990s at the Child Branch of the National Institutes of Mental Health in Bethesda, Maryland [41]. This longitudinal study of structural brain development in typically developing children and adolescents has provided significant insights into the regional specific trajectories of neurodevelopment [45–47]. More recently, an NIH extramural study performed at six different sites in the United States has recruited a total of 384 children between the ages of 2 months to 18 years in a prospective, accelerated longitudinal study [42]. Two additional large imaging studies in Canada [43] and Europe [44] have been initiated as hypothesis-directed studies to evaluate the effects of prenatal exposure to nicotine and emerging substance abuse, respectively.
The Generation R Study has some characteristic differences with these large population-based studies. Since the Generation R is a population-based cohort study in which the children were recruited during fetal life, there was no exclusion criteria based on the physical or emotional health of the child. Both the intramural and extramural NIMH studies [41, 42] had strict criteria for inclusion, which is a good approach for studying typical development, but does bias the results toward the neurodevelopment of ‘super controls.’ Within the Generation R Cohort, if we exclude those children who have been exposed to nicotine, cannabis, maternal depression, or maternal SSRI use, and those who are below the clinical range for either the internalizing or externalizing range on the Child Behavior Checklist, it leaves 323 children. Excluding children with the same exposures as above, but who fall below the borderline range for the CBCL internalizing and externalizing scales, the number of children drops to 298. Thus, approximately half of the children with imaging data are reflective of the cohort within the NIMH studies, which is not surprising since the children were not randomly selected from the Generation R Study.
Another strength of the Generation R Study is the very large sample size, which is crucial for parsing out genetic, environmental, and interaction effects. Large sample sizes are considered important for tracking developmental changes [48] since developmental trajectories show considerable variability [41]. In addition, there were no exclusion criteria based on ethnicity, as was true in the Saguenay Youth Study [43] and the IMAGEN study [44]. Similar to the NIH intramural study [41] and the Saguenay Youth Study [43], all neuroimaging within the Generation R Study has been performed at one site and on the same scanner. Finally, since the Generation R was designed as an epidemiological study crossing the different disciplines of pediatrics and child and adolescent psychiatry [13], it contains a vast array of physiological and environmental measures.
One of the early measures of brain development within the Generation R was obtained using fetal ultrasound measures. Ultrasound imaging of the head, biparietal diameter, ventricular size, and cerebellar diameter was performed at multiple time points during fetal life in 8,313 children [15]. In addition, postnatal fetal ultrasound measures were obtained at 1 month in 778 children [16]. These early ultrasound studies can provide an important link to understanding global measures of brain changes over time. Similar to other large neuroimaging studies, the Generation R imaging component has a high-resolution structural imaging scan. However, only the IMAGEN study [44] has included both diffusion weighted and functional imaging paradigms.
In combination with neuroimaging data, many studies also include a neuropsychological battery as a component of the study [36]. Neuropsychological testing was developed prior to the development of MRI and was often used in attempt to identify the location of specific deficits or lesions [49]. While lacking spatial specificity, a thorough neuropsychological battery provides valuable information on the underlying brain function and dysfunction [50]. The neuropsychological measures will be combined with the neuroimaging data to better understand the differential characteristics of age and sex in brain development. The neuroimaging is ongoing and we will soon be inviting children for the second wave of scanning. This second wave of scanning will take place on a new dedicated GE 3 Tesla wide bore scanner and all of the approximately 7000 children from the Generation R Study will be invited for an MRI scan.
Conclusion
In conclusion, the Generation R Study is an epidemiological study of child health and development that began in 2002 with the recruitment of nearly 10,000 mothers in early pregnancy or who had recently given birth. The infusion of MRI imaging into the Generation R Study began in September 2009 with 801 children recruited up to the 29th of February 2012. The Generation R imaging study is characteristically different from other large neuroimaging studies in that it is a population-based prenatal cohort with multiple waves of data collection. In addition, the inclusion criteria are broader, allowing for a better representation of the pediatric population in general. This will provide not only a better overview of neurodevelopmental trajectories in typically developing children, but also for children with emerging developmental or psychiatric problems. Both the experience of the children and the quality of the data has been very good thus far. In summary, the infusion of imaging into the Generation R Study will prove to be incredibly valuable in addressing questions of the role of genes and multiple environmental factors in neurodevelopment and neurodevelopment gone awry.
References
Kandel ER, Schwartz JH, Jessell TM. Principles of neural science. 4th ed. New York: McGraw-Hill Health Professions Division; 2000.
Pomeroy SL, Kim JY. Biology and pathobiology of neuronal development. Ment Retard Dev Disabil Res Rev. 2000;6(1):41–6.
White T, Su S, Schmidt M, Kao CY, Sapiro G. The development of gyrification in childhood and adolescence. Brain Cogn. 2010;72(1):36–45. doi:10.1016/j.bandc.2009.10.009.
Huttenlocher PR. Morphometric study of human cerebral cortex development. Neuropsychologia. 1990;28(6):517–27.
Huttenlocher PR, De Courten C, Garey LJ, van der Loos H. Synaptic development in human cerebral cortex. Int J Neurol. 1982;17:144–54.
Yakovlev PI, Lecours AR. The myelogenetic cycles of regional maturation of the brain. In: Minkowski A, editor. Regional development of the brain in early life. Oxford: Blackwell; 1967. p. 3–70.
Huttenlocher P. Developmental anatomy of the prefrontal cortex. In: Krasnegor N, editor. Development of the prefrontal cortex: evolution, neurobiology, and behavior. Baltimore: Paul H. Brookes Publishing Co., Inc.; 1997. p. 69–83.
Huttenlocher PR, de Courten C. The development of synapses in striate cortex of man. Hum Neurobiol. 1987;6(1):1–9.
Williams RW, Herrup K. The control of neuron number. Annu Rev Neurosci. 1988;11:423–53. doi:10.1146/annurev.ne.11.030188.002231.
Gressens P, Mesples B, Sahir N, Marret S, Sola A. Environmental factors and disturbances of brain development. Semin Neonatol. 2001;6(2):185–94. doi:10.1053/siny.2001.0048.
Paus T. Population neuroscience: why and how. Hum Brain Mapp. 2010;31(6):891–903. doi:10.1002/hbm.21069.
Jaddoe VW, van Duijn CM, van der Heijden AJ, Mackenbach JP, Moll HA, Steegers EA, et al. The Generation R Study: design and cohort update 2010. Eur J Epidemiol. 2010;25(11):823–41. doi:10.1007/s10654-010-9516-7.
Hofman A, Jaddoe VW, Mackenbach JP, Moll HA, Snijders RF, Steegers EA, et al. Growth, development and health from early fetal life until young adulthood: the Generation R Study. Paediatr Perinat Epidemiol. 2004;18(1):61–72.
Tiemeier H, Velders FP, Szekely E, Roza SJ, Dieleman G, Jaddoe VW et al. The Generation R Study: a review of design, findings to date, and a study of the 5-HTTLPR by environmental interaction from fetal life onward. J Am Acad Child Adolesc Psychiatry. 2012;51(11):1119–35 e7. doi:10.1016/j.jaac.2012.08.021.
Verburg BO, Steegers EA, De Ridder M, Snijders RJ, Smith E, Hofman A, et al. New charts for ultrasound dating of pregnancy and assessment of fetal growth: longitudinal data from a population-based cohort study. Ultrasound Obstet Gynecol. 2008;31(4):388–96. doi:10.1002/uog.5225.
Roza SJ, Govaert PP, Vrooman HA, Lequin MH, Hofman A, Steegers EA, et al. Foetal growth determines cerebral ventricular volume in infants The Generation R Study. Neuroimage. 2008;39(4):1491–8. doi:10.1016/j.neuroimage.2007.11.004.
Jaddoe VW, Mackenbach JP, Moll HA, Steegers EA, Tiemeier H, Verhulst FC, et al. The Generation R Study: design and cohort profile. Eur J Epidemiol. 2006;21(6):475–84. doi:10.1007/s10654-006-9022-0.
Brooks BL, Sherman EM, Strauss E. Test Review: NEPSY-II: a developmental neuropsychological assessment, second edition. Child Neuropsychol. 2010;16:80–101.
Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia. 1971;9(1):97–113.
Durston S, Nederveen H, van Dijk S, van Belle J, de Zeeuw P, Langen M, et al. Magnetic resonance simulation is effective in reducing anxiety related to magnetic resonance scanning in children. J Am Acad Child Adolesc Psychiatry. 2009;48(2):206–7. doi:10.1097/CHI.0b013e3181930673.
Fischl B. FreeSurfer. Neuroimage. 2012;. doi:10.1016/j.neuroimage.2012.01.021.
Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TE, Johansen-Berg H, et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage. 2004;23(Suppl 1):S208–19. doi:10.1016/j.neuroimage.2004.07.051.
Smith SM, Jenkinson M, Johansen-Berg H, Rueckert D, Nichols TE, Mackay CE, et al. Tract-based spatial statistics: voxelwise analysis of multi-subject diffusion data. Neuroimage. 2006;31(4):1487–505.
White T, Schmidt M, Karatekin C. White matter ‘potholes’ in early-onset schizophrenia: a new approach to evaluate white matter microstructure using diffusion tensor imaging. Psychiatry Res. 2009;174(2):110–5. doi:10.1016/j.pscychresns.2009.04.014.
Cox RW. AFNI: software for analysis and visualization of functional magnetic resonance neuroimages. Comput Biomed Res. 1996;29(3):162–73.
Kim DI, Manoach DS, Mathalon DH, Turner JA, Mannell M, Brown GG, et al. Dysregulation of working memory and default-mode networks in schizophrenia using independent component analysis, an fBIRN and MCIC study. Hum Brain Mapp. 2009;30(11):3795–811. doi:10.1002/hbm.20807.
Beckmann CF, Smith SM. Probabilistic independent component analysis for functional magnetic resonance imaging. IEEE Trans Med Imag. 2004;23(2):137–52. doi:10.1109/TMI.2003.822821.
Langeslag SJ, Schmidt M, Ghassabian A, Jaddoe VW, Hofman A, van der Lugt A, et al. Functional connectivity between parietal and frontal brain regions and intelligence in young children: the Generation R study. Hum Brain Mapp. 2012;. doi:10.1002/hbm.22143.
Gemeente-Rotterdam. Bevolking van Rotterdam naar etniciteit (CBS-definitie), op 1-1-2001 t/m 2011 Centrum voor Onderzoek en Statistiek, Rotterdam, the Netherlands. http://www.cos.rotterdam.nl/ (2011). Accessed 23 June 2011.
NINDS. Genes at work in the brain. Bethesda, Maryland: National Institutes of Neurological Disorders and Stroke. U.S. Department of Health and Human Services; 2010.
White T, Andreasen NC, Nopoulos P. Brain volumes and surface morphology in monozygotic twins. Cereb Cortex. 2002;12(5):486–93.
Bartley AJ, Jones DW, Weinberger DR. Genetic variability of human brain size and cortical gyral patterns. Brain. 1997;120(Pt 2):257–69.
Henrichs J, Schenk JJ, Roza SJ, van den Berg MP, Schmidt HG, Steegers EA, et al. Maternal psychological distress and fetal growth trajectories: the Generation R Study. Psychol Med. 2010;40(4):633–43. doi:10.1017/S0033291709990894.
Roza SJ, Verburg BO, Jaddoe VW, Hofman A, Mackenbach JP, Steegers EA et al. Effects of maternal smoking in pregnancy on prenatal brain development. The Generation R Study. Eur J Neurosci. 2007;25(3):611–7. doi:10.1111/j.1460-9568.2007.05393.x.
El Marroun H, Tiemeier H, Steegers EA, Jaddoe VW, Hofman A, Verhulst FC, et al. Intrauterine cannabis exposure affects fetal growth trajectories: the Generation R Study. J Am Acad Child Adolesc Psychiatry. 2009;48(12):1173–81. doi:10.1097/CHI.0b013e3181bfa8ee.
Waber DP, De Moor C, Forbes PW, Almli CR, Botteron KN, Leonard G, et al. The NIH MRI study of normal brain development: performance of a population based sample of healthy children aged 6 to 18 years on a neuropsychological battery. J Int Neuropsychol Soc. 2007;13(5):729–46. doi:10.1017/S1355617707070841.
Cartwright-Hatton S, McNicol K, Doubleday E. Anxiety in a neglected population: prevalence of anxiety disorders in pre-adolescent children. Clin Psychol Rev. 2006;26(7):817–33. doi:10.1016/j.cpr.2005.12.002.
Sowell ER, Thompson PM, Leonard CM, Welcome SE, Kan E, Toga AW. Longitudinal mapping of cortical thickness and brain growth in normal children. J Neurosci. 2004;24(38):8223–31.
Pfefferbaum A, Mathalon DH, Sullivan EV, Rawles JM, Zipursky RB, Lim KO. A quantitative magnetic resonance imaging study of changes in brain morphology from infancy to late adulthood. Arch Neurol. 1994;51(9):874–87.
Jernigan TL, Trauner DA, Hesselink JR, Tallal PA. Maturation of human cerebrum observed in vivo during adolescence. Brain. 1991;114(Pt 5):2037–49.
Giedd JN, Blumenthal J, Jeffries NO, Castellanos FX, Liu H, Zijdenbos A, et al. Brain development during childhood and adolescence: a longitudinal MRI study. Nat Neurosci. 1999;2(10):861–3. doi:10.1038/13158.
Evans AC, The NIH. MRI study of normal brain development. Neuroimage. 2006;30(1):184–202. doi:10.1016/j.neuroimage.2005.09.068.
Pausova Z, Paus T, Abrahamowicz M, Almerigi J, Arbour N, Bernard M, et al. Genes, maternal smoking, and the offspring brain and body during adolescence: design of the Saguenay Youth Study. Hum Brain Mapp. 2007;28(6):502–18. doi:10.1002/hbm.20402.
Schumann G, Loth E, Banaschewski T, Barbot A, Barker G, Buchel C, et al. The IMAGEN study: reinforcement-related behaviour in normal brain function and psychopathology. Mol Psychiatry. 2010;15(12):1128–39. doi:10.1038/mp.2010.4.
Giedd JN, Rapoport JL. Structural MRI of pediatric brain development: what have we learned and where are we going? Neuron. 2010;67(5):728–34. doi:10.1016/j.neuron.2010.08.040.
Tiemeier H, Lenroot RK, Greenstein DK, Tran L, Pierson R, Giedd JN. Cerebellum development during childhood and adolescence: a longitudinal morphometric MRI study. Neuroimage. 2010;49(1):63–70. doi:10.1016/j.neuroimage.2009.08.016.
Giedd JN, Lenroot RK, Shaw P, Lalonde F, Celano M, White S et al. Trajectories of anatomic brain development as a phenotype. Novartis Found Symp. 2008;289:101–12; discussion 12-8, 93-5.
Gogtay N, Giedd JN, Lusk L, Hayashi KM, Greenstein D, Vaituzis AC, et al. Dynamic mapping of human cortical development during childhood through early adulthood. Proc Natl Acad Sci USA. 2004;101(21):8174–9. doi:10.1073/pnas.0402680101.
Glozman JM. A.R. Luria and the history of Russian neuropsychology. J His Neurosci. 2007;16(1–2):168–80. doi:10.1080/09647040600550368.
Luciana M, Nelson CA. The functional emergence of prefrontally-guided working memory systems in four- to eight-year-old children. Neuropsychologia. 1998;36(3):273–93.
Acknowledgments
The Generation R Study is conducted by the Erasmus Medical Center in close collaboration with the Erasmus University Rotterdam, the Municipal Health Service in the Rotterdam area, the Rotterdam Homecare Foundation, Rotterdam and the Stichting Trombosedienst & Artsenlaboratorium Rijnmond (STAR-MDC), Rotterdam. We gratefully acknowledge the contribution of children and parents, general practitioners, hospitals, midwives and pharmacies in Rotterdam. We also gratefully acknowledge the hard work of the PhD students who have assisted with data collection. These include Nikita Schoemaker, Sabine Mous, Gerbrich van den Bosch, Ryan Muetzel, Sandra Thijssen, Andrea Wildeboer, Laura Blanken, Carolyn Langen, and Akvile Lukose. Neuroimaging studies within the Generation R are supported through the Netherlands Organization for Health Research and Development (NWO) (ZonMw TOP 40-00812-98-11021), the European Community’s 7th Framework Programme (FP7/2008–2013) under grant agreement 212652 (NUTRIMENTHE), the Stichting Sophia Kinderziekenhuis Fonds, and General Electric Healthcare. The Generation R Study is made possible by financial support from the Erasmus Medical Center, Rotterdam, the Erasmus University Rotterdam, ZonMw (ZonMW 10.000.1003), the Netherlands Organization for Scientific Research (NWO), the Ministry of Health, Welfare and Sport, and the Ministry of Youth and Families.
Conflict of interest
None of the authors have any conflicts of interest associated with this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
White, T., Marroun, H.E., Nijs, I. et al. Pediatric population-based neuroimaging and the Generation R Study: the intersection of developmental neuroscience and epidemiology. Eur J Epidemiol 28, 99–111 (2013). https://doi.org/10.1007/s10654-013-9768-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-013-9768-0