
Abstract
Low rates of participation in parenting interventions may undermine their effectiveness. Although a wide range of strategies to engage parents in interventions are described in the literature, little is known about which engagement strategies are most effective in enhancing parental engagement. This systematic review explores effective engagement strategies to encourage initial parental engagement (recruitment, enrolment, and first attendance) in parenting interventions for parents of children aged 2–8 years old. This review was conducted based on the guidelines of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins and Green 2011) and the Preferred Reporting Items for Systematic Review and Meta-Analysis (Moher et al. 2009). Electronic systematic searches from January 1996 to August 2017 were conducted in PsycINFO, Scopus, ProQuest Social Sciences Journals, CINAHL, and PubMed databases. Eight studies met the inclusion criteria representing 1952 parents from four different countries. Of the engagement strategies tested in included studies (monetary incentive, setting, testimonial, advertisement, and engagement package), three strategies (advertisement, incentive, and engagement package) showed a significant effect on a stage of engagement, but none across stages. The low methodological quality of the selected studies limits their generalisability and thus provides limited evidence regarding effective engagement strategies to increase recruitment, enrolment, and first attendance rates in parenting interventions. There is a need for further, more methodologically rigorous, research evidence regarding how to engage parents more effectively in the early stages of parenting interventions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Parenting interventions are effective in promoting positive parenting practices, nurturing parent–child relationships, and reducing coercive parenting and child behaviour problems (Sanders et al. 2014; World Health Organization 2009). However, most parents do not participate in any parenting intervention, and even few take part in evidence-based interventions. In targeted interventions calls, fewer than 30% of the initially targeted parents attend a given parenting intervention (Girvin et al. 2007; Miller and Prinz 2003). Furthermore, a survey study reported that of those parents who perceived emotional and behavioural problems in their children, only half had actually sought help and only one-third had participated in a parent education programme (Sanders et al. 1999). Therefore, there is a gap between those parents who are in need of support and those who actually seek help and access that support.
Although many parenting interventions are targeted to parents in need of support, there are increasing calls for preventive approaches. Some parenting interventions provide varying levels of support, and this diverse offer makes them suitable to be disseminated from a public health perspective (Sanders 2012). This approach aims to target parents at a population level and offer different intervention doses, ranging from very brief to intensive to benefit the population of children and families as a whole (Calam et al. 2008; Chu et al. 2014; Prinz et al. 2009). Studies focused on these preventive interventions have reported fewer than 30% of the parents who were invited to participate then attended the first session (Garvey et al. 2006; Heinrichs et al. 2005); but if parents do not engage in these offered parenting interventions, these interventions are potentially inefficient and less cost-effective.
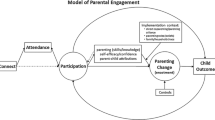
In the last 20 years, research has aimed to identify factors influencing how parents engage in parenting interventions (Shaffer et al. 2001). Parental engagement refers to the active involvement of a parent throughout the process of a parenting intervention to learn and develop parenting skills. This engagement occurs in a multistage process involving recruitment, enrolment, participation (including session attendance, quality of participation, and completion), and technique utilisation (Eisner and Meidert 2011; McCurdy and Daro 2001; Morawska and Sanders 2006).
Previous studies have varied in defining parental engagement, but the majority have recognised that it is a process involving several stages (Dumas et al. 2010; McCurdy and Daro 2001; Morawska and Sanders 2006; Piotrowska et al. 2017). These stages include: intervention reach (Morawska and Sanders 2006), recruitment (Piotrowska et al. 2017), intent to enrol (Dumas et al. 2010; McCurdy and Daro 2001), cognitive preparation (Becker et al. 2015), enrolment (Gross et al. 2011; McCurdy and Daro 2001), attendance (Dumas et al. 2010; Gross et al. 2011), retention (McCurdy and Daro 2001; Piotrowska et al. 2017), quality of participation (Lefever et al. 2013; Piotrowska et al. 2017), homework completion (Chacko et al. 2016), attrition (Chacko et al. 2016), intervention completion (Eisner and Meidert 2011; Morawska and Sanders 2006), and technique utilisation (Eisner and Meidert 2011; Piotrowska et al. 2017). Thus, whereas some definitions have focused only on stages during the intervention (Gross et al. 2011; Lefever et al. 2013), other definitions have included pre-intervention phases (Chacko et al. 2016; Dumas et al. 2007; McCurdy and Daro 2001) and also post-intervention stages (Eisner and Meidert 2011; Piotrowska et al. 2017). Some of these stages (i.e. recruitment and enrolment) may overlap or be defined differently across studies, which may lead to misunderstanding of those stages and reported outcomes. However, the majority of studies have operationally defined their conceptualisation of each stage, which facilitates comparison across studies.
The measurement of parental engagement has also varied across studies, which usually focuses on parent’s behaviour. Thus, indicators such as number or percentage of parents signing up, completing consent forms, and attending sessions have been used as measures of parental engagement (Dumas et al. 2010; Garvey et al. 2006; Heinrichs 2006; Miller and Prinz 2003). Still, there are some discrepancies in how these measures have been reported. For instance, Dumas et al. (2010) measured enrolment based on those parents who returned registration forms, while Garvey et al. (2006) and Gross et al. (2011) included those who both consented to participate and completed baseline assessments. The common emphasis on behavioural elements of engagement, such as attending a session, may cloud the various factors that contribute to engagement. Becker et al. (2015) highlighted that cognitions are important elements of engagement, and they need to be taken into account throughout the process. However, few studies have included some measures focusing on parents’ attitudes and intentions about participation in a parenting intervention (Dumas et al. 2010; Eisner and Meidert 2011).
Research has largely focused on engagement during the intervention, while the initial stages of parental engagement have received less attention (Chacko et al. 2016; Lefever et al. 2013). Initial parental engagement is the process in which parents intend and commit (attitudinal component) to participate in a parenting intervention in order to learn and develop parenting skills. It includes the stages of recruitment, enrolment, and first attendance at a parenting intervention. Recruitment is the process of attracting parents to engage in a parenting intervention, enrolment is the parent’s decision to engage in a parenting intervention, and first attendance is their actual behaviour involving completion of the first action required for a parenting intervention, such as attending the first face-to-face session. It has been reported that of those parents who met the inclusion criteria, an attrition rate of 25% has been reported before enrolment (Chacko et al. 2016). Similarly, attrition rates over 20% have been reported from enrolment to first attendance (Heinrichs 2006). Therefore, it is critical to consider strategies to engage parents earlier and to capitalise on positive attitudes and intentions.
Low levels of initial engagement in parenting interventions are problematic for a number of reasons. The results of intervention research may be brought into question undermining their generalisation (Bruzzese et al. 2009; Heinrichs et al. 2005; Morawska and Sanders 2006) and weaken the economic efficiency of such intervention as consequence of those resources unused (Dumas et al. 2007; Gross et al. 2011; Morawska and Sanders 2006). When outcomes are based on parents who are engaged in a parenting intervention, it may lead to a positive bias in results that are not representative of all parents from a given population. Contrarily, when fewer parents participate than planned, outcome validity can be affected due to small samples reducing power to detect effects (Garvey et al. 2006).
In the context of mental health services, parental engagement has been addressed from a theoretical (Becker et al. 2017; McCurdy and Daro 2001; Staudt 2007) and practical perspective (Becker et al. 2015, 2017; Chacko et al. 2012; Lindsey et al. 2014). However, the evidence of engagement in these services may not be applicable to parenting interventions, given that mental health services focus on the treatment of psychiatric disorders (Becker et al. 2015). Instead, the implementation of evidence-based parenting interventions at a population level requires an approach with more emphasis on a preventive focus, where all parents are able to learn and develop specific parenting skills to support their children’s development.
Research on parental engagement in parenting interventions has commonly addressed barriers to engagement. One primary reason parents fail to attend parenting programmes reported in the literature is stigma, but other reported factors include gender issues, perceived lack of resources, accessibility, confidentiality, and time constraints (Mytton et al. 2014; Ohan et al. 2015). Given that parenting interventions are also conceived as a preventive intervention suitable for any parent to enhance his/her parenting skills (Sanders and Kirby 2012), it is relevant to reinforce parents’ participation beyond tackling barriers towards those factors facilitating parents’ involvement in parenting interventions. For example, some evidence suggests that parents are more likely to participate in further parenting interventions when they have participated in an earlier intervention (Bérubé et al. 2014; Chislett and Kennett 2007). Others have found that when parents attend the first session, they showed more positive attitudes towards the intervention and continued attendance (Garvey et al. 2006).
In order to advance the consolidation of parenting interventions as evidence-based practice, their dissemination and implementation need to take into account best practice in the engagement of parents as primary consumers of such interventions (Sanders and Kirby 2012). Currently, the dissemination of parenting interventions includes continuous evaluation and programme refinement as well as appropriate training of providers and fidelity of the programme delivery (Olofsson et al. 2016; Sanders and Kirby 2015). Sustainable dissemination needs to provide tools to practitioners to effectively engage parents throughout the parenting intervention, beyond removing barriers towards providing evidence-based strategies to enhance parents’ engagement.
Engagement Strategies
A wide range of strategies have been used to engage parents in parenting interventions (Morawska and Sanders 2006; Shaffer et al. 2001), but they have been more commonly described, rather than empirically tested to report to what extent they are effective in engaging those parents who participated. To address this gap, we operationally defined an engagement strategy as any action implemented to introduce a parenting intervention to parents in order to encourage their engagement.
One of the better-studied approaches is the use of monetary incentives (Cullen et al. 2016; Dumas et al. 2010; Guyll et al. 2003; Heinrichs 2006). Some studies have reported that payment for participation has increased enrolment and first attendance rates (Guyll et al. 2003; Heinrichs 2006). On the other hand, other researchers have found incentives to have limited effects (Dumas et al. 2010; Gross et al. 2011; Heinrichs 2006) and have sometimes received criticism for introducing a market perspective into the provision of parenting interventions (Cullen et al. 2016). As a consequence, this kind of incentive has been questioned and discouraged (Dumas et al. 2010), which can be also difficult to implement given the limited resources that are typically available to implement parenting interventions.
Although engagement strategies have been used and examined in many studies, their impact on parental engagement remains unclear due to the diversity of definitions of parental engagement and how it has been measured (Chacko et al. 2016; Haine-Schlagel and Walsh 2015; Ingoldsby 2010). Consequently, the analysis of these individual studies can lead to misleading results when studies are examined in isolation, and comparison across studies can be difficult to achieve. Given that studies have usually implemented engagement strategies as a package (Dumas et al. 2010), how each strategy influences engagement remains unknown. There are some narrative and systematic reviews addressing parental engagement in the context of interventions for parents (Becker et al. 2015, 2017; Chacko et al. 2016; Haine-Schlagel and Walsh 2015; Ingoldsby 2010; Lindsey et al. 2014; Morawska and Sanders 2006). However, these reviews have focused on reporting engagement data (Chacko et al. 2016), describing engagement strategies used (Lindsey et al. 2014; Morawska and Sanders 2006), presenting engagement outcomes for stages during the intervention (Haine-Schlagel and Walsh 2015; Ingoldsby 2010), and describing clinical practice elements linked to engagement outcomes (Becker et al. 2015, 2017). The majority of these reviews are from the field of mental health (Becker et al. 2015, 2017; Haine-Schlagel and Walsh 2015; Ingoldsby 2010; Lindsey et al. 2014), whereas only two reviews addressed engagement strategies in the context of parenting interventions (Chacko et al. 2016; Morawska and Sanders 2006). Although these reviews have contributed to expanding the existing knowledge regarding parental engagement, we still do not know which engagement strategies are the most effective in engaging parents to parenting interventions during recruitment, enrolment, and first attendance.
This review aims to fill this gap by identifying the effectiveness of engagement strategies tested in experimental studies on initial parental engagement. It focuses on the question: What engagement strategies have been tested, and to what extent have they been effective in promoting parental engagement in the initial stages of parenting interventions? Given that several reviews of parental engagement have been inconclusive, this review was restricted to experimental studies to ensure that we only include studies that rigorously tested the effectiveness of engagement strategies during recruitment, enrolment, and first attendance to a parenting intervention. The aim of this study was to explore effective engagement strategies to encourage initial parental engagement (recruitment, enrolment, and first attendance) in parenting interventions for parents of children aged 2–8 years old. We have focused on this age group because there is a high prevalence of emotional and behavioural difficulties at this age when they are still in early onset (Dittman et al. 2011). Thus, early interventions may be more effective and represent greater benefits for children and their parents, if this support is provided from early childhood when they are at higher risk of developing emotional and behavioural problems. Additionally, the earliest official age that children enter pre-primary education is 3 years old and the oldest age to enter primary school is 7 years old (UNESCO Institute of Statistics 2018). Thus, the age range of 2–8 years old captures comprehensively preschool and the transition from preschool to primary school worldwide. The contribution of this review is to systematically summarise the strategies tested and their outcomes and provide evidence of effective strategies to enhance initial parental engagement in parenting interventions.
Methods
This systematic review was conducted based on the Cochrane Handbook for Systematic Reviews of Interventions (Higgins and Green 2008, 2011) and the Preferred Reporting Items for Systematic Review and Meta-Analysis, PRISMA (Moher et al. 2009).
Protocol and Registration
The protocol for this review was registered on PROSPERO (CRD42016039826) before completion of searching and data entry.
Search Methods for Identification of Studies
Electronic Searches
Searches were limited to journal articles published in English or Spanish in the last 20 years (January 1996–August 2017) in peer-reviewed journals in the following databases: PsycINFO, Scopus, ProQuest Social Science Journals, CINAHL, and PubMed. The search date was 25 August 2017 for all five databases. The search strategy used a combination of search terms, “parental engagement/participation/involvement” and “parental training/intervention/program”. These search terms were adapted following requirements of search strategies for each database according to De Brún and Pearce-Smith (2014) as presented in Table 1. These terms were searched using all possible combinations across databases.
Criteria for Selecting Studies for this Review
Type of Studies
To be included in this review studies needed to be: (a) experimental studies with randomised allocation to at least two different conditions and (b) written in English or Spanish.
Type of Participants
The inclusion criteria for participants were: (a) parents of children aged 2–8 years old at the beginning of the intervention. For studies with a different age range of children, studies were included when the average age of the participants was between 2 and 8 years; (b) birth and step-parent or parents living with the child in the same house or assuming parental responsibilities over the child; (c) participants are mothers only or samples with both mothers and fathers. Thus, studies focused only on father engagement were excluded as they represent an emerging research area with particular challenges in regard to fathers’ engagement in parenting interventions (Cowan et al. 2009; Frank et al. 2015a, b); and (d) parents of typically developing children.
The exclusion criteria for participants were: (a) parents of children less than two or more than 8 years old; (b) parents of children with developmental disabilities or life-threatening illnesses; and (c) parents with severe mental illness, teen parents, and those experiencing significant psychosocial stressors that can significantly impact their role as parents, such as homelessness and imprisonment. Thus, parents facing special conditions were excluded given that their needs may not be representative of a general community sample, which this review aimed to provide evidence for. Parents’ special conditions may undermine the impact of a parental intervention (Shaffer et al. 2001), which may need specialised treatment or engagement strategies prior to intervention. On the other hand, engagement strategies that may be effective for the general population may not be as effective with high needs groups, which may result in misleading results.
Type of Intervention
The interventions were: (a) any engagement strategy designed to enhance parental engagement at the initial stages of an intervention for parents, regardless of intervention characteristics (e.g. delivery format, intervention length or number of sessions, practitioner involvement, target population, or delivery setting). Parenting interventions were defined as ones, which provided both information and skills training for parents in terms of child development, child behaviour, or parenting. Interventions providing information only were not included; (b) the engagement strategy consisted of any action implemented by practitioners or researchers to introduce the intervention to parents and encouraged their involvement in it; and (c) initial stages of parenting interventions were understood as recruitment, enrolment, and first attendance. Recruitment was considered as the timeframe where direct and indirect actions are oriented to introduce a parenting intervention to parents (targeted or at a population level). During this stage, parents may be invited to participate in interventions through strategies such as posters, letters, and informative sessions. Enrolment implied the following stage between the introduction of an intervention to parents and their actual enrolment. This stage may involve, for instance, parents completing registration forms and consent forms. Given that these two stages can overlap in studies, the study definitions were fit to the definitions operationalised in this review. First attendance referred to parent’s completion of the first action required by the parenting intervention (e.g. attending a face-to-face session, completing an online intervention module).
Type of Outcome Measures
Any outcome presented as an indicator of parental engagement during recruitment, enrolment, and initial attendance was included. We expected these to include information such as percentage of attendance at a first session or percentage of parents enrolling.
Data Collection and Analysis
Selection of Studies
Search results from all five databases were merged, and duplicate records were removed. Titles and abstracts of the remaining articles were examined to remove irrelevant reports according to inclusion and exclusion criteria. Two reviewers independently conducted the selection of articles by full-text of potentially relevant papers. This process involved a pilot test on a sample of the first ten articles in order to clarify eligibility criteria and train reviewers. The level of agreement for the whole list of full-text revision was also established. Disagreements between reviewers were recorded and resolved with the second author as the third reviewer. The detailed information about the selection process was detailed using an adapted PRISMA flow diagram (Moher et al. 2009).
Data Extraction and Management
The following information from each study was extracted: study design and methods, sample characteristics, intervention characteristics, comparisons, and primary outcomes.
Assessment of Risk of Bias in Included Studies
Selected studies were evaluated using the Cochrane Collaboration’s tool for assessing the risk of bias (Higgins et al. 2011; Higgins and Green 2008, 2011). The dimensions assessed are selection bias (random sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessment), attrition bias (incomplete outcome data), reporting bias (selective reporting), and other bias. The judgement of the risk of bias criteria is categorised as “high risk”, “low risk”, or “unclear risk”. The risk of bias graph and summary were prepared using Review Manager (RevMan) of The Cochrane Collaboration (2014).
Dealing with Missing Data
Corresponding authors were contacted when relevant information regarding inclusion and exclusion criteria was missing in the study, i.e. mean age of children. If the author did not answer the email after three attempts (emails sent), the article was excluded.
Results
This systematic review identified eight studies for inclusion in the analysis. Figure 1 illustrates the study selection process in detail using an adapted PRISMA flow diagram. To summarise, initially 2244 articles were located, and 1024 remained after duplicate records were removed. Irrelevant articles were eliminated by title and abstract, resulting in 32 articles for full-text review. Two articles reported two studies with different samples within the same article (Morawska et al. 2011; Salari and Backman 2016), which were separated to be analysed independently. Therefore, this review reports on six articles, corresponding to eight independent studies, which were the studies included for analysis in this review. The level of agreement of both reviewers for the full-text revision of the 32 articles was excellent (κ = .80, p < .001).

Adapted PRISMA flow chart
Due to the diversity of engagement strategies tested and outcomes reported, this review presents a description of the selected studies and their results using a qualitative synthesis, which includes the outcomes of the assessment of risk of bias and the description of included studies.
Assessment of Risk of Bias
The overview of the judgements regarding the risk of bias for each criterion across studies and for each individual study is presented in Figs. 2 and 3, respectively. All eight studies showed some methodological weaknesses that resulted in some risk of bias.

Risk of bias graph

Risk of bias summary
Random Sequence Generation
In terms of the description of the method used to generate the allocation based on randomised sequence, all eight studies reported that participants were randomised to experimental conditions. However, only two studies described the random sequence generation process used; a computer-generated list of random numbers (Morawska et al. 2011: Study 1) and assignment by lottery (Winslow et al. 2016), which resulted in a low risk of bias. One study (Salari and Backman 2016: Study 1) used a type of sequence that is categorised as high risk of bias. Five studies did not describe randomisation procedures (Dumas et al. 2010; Gross et al. 2011; Heinrichs 2006; Morawska et al. 2011: Study 2; Salari and Backman 2016: Study 2).
Allocation Concealment
This criterion refers to the concealment of allocation to both participants and investigators. Five studies were at high risk of bias (Dumas et al. 2010; Gross et al. 2011; Heinrichs 2006; Salari and Backman 2016: Study 2; Winslow et al. 2016), whereas three studies were considered as unclear risk of bias (Morawska et al. 2011: S1&S2; Salari and Backman 2016: S1).
Blinding of Participants and Personnel
This criterion is likely to be compromised in most studies involving psychosocial interventions due to participants and personnel knowing in which intervention the participant was involved (Higgins and Green 2008, 2011). Two studies were implemented online facilitating the blinding of participants and personnel (Morawska et al. 2011: S2; Salari and Backman 2016: S1), while the remaining studies showed a high (Dumas et al. 2010; Gross et al. 2011; Heinrichs 2006; Salari and Backman 2016: S2; Winslow et al. 2016) or unclear risk of bias (Morawska et al. 2011: S1).
Blinding of Outcome Assessment
All eight studies included objective measures or specific questions used across all the experimental conditions to gather initial parental engagement outcomes (Dumas et al. 2010; Gross et al. 2011; Heinrichs 2006; Morawska et al. 2011: S1&S2; Salari and Backman 2016: S1&S2), reducing this risk of bias to low.
Incomplete Outcome Data
Seven studies did not report missing outcome data (Dumas et al. 2010; Gross et al. 2011; Heinrichs 2006; Morawska et al. 2011: S1&S2; Salari and Backman 2016: S1&S2). One study reported missing data for one secondary measure (Winslow et al. 2016). Regarding exclusion of outcome data, six studies reported outcomes from all measures presented in the method sections in their articles (Dumas et al. 2010; Gross et al. 2011; Morawska et al. 2011: S1&S2; Salari and Backman 2016: S1&S2). However, two studies showed some exclusions of outcomes in their analysis (Heinrichs 2006; Winslow et al. 2016).
Selective Reporting
None of the eight studies reported protocol registration prior to data collection. Six studies reported outcomes from all measures presented in the method sections in their articles (Dumas et al. 2010; Gross et al. 2011; Morawska et al. 2011: S1&S2; Salari and Backman 2016: S1&S2). One study reported all outcomes from measures presented in the method sections in their articles but no data from some engagement measures for the control group, using intent-to-treat analysis instead (Winslow et al. 2016). In one study, participants completed several self-report measures of which only one instrument was reported in the study (Heinrichs 2006).
Other Sources of Bias
Six studies received funding to conduct the study, but all grants were from national institutions and other non-profit organisations (Dumas et al. 2010; Gross et al. 2011; Heinrichs 2006; Salari and Backman 2016: S1&S2; Winslow et al. 2016), who do not stand to benefit in any way from the findings. The authors of six studies presented affiliation to institutions which have developed and implemented the parenting interventions of the study (Morawska et al. 2011: S1&S2), work relations with these institutions (Salari and Backman 2016: S1&S2), or a role in developing and evaluation of such parenting interventions (Dumas et al. 2010; Gross et al. 2011). However, these studies aimed to assess engagement strategies rather than the effectiveness of the parenting intervention; therefore, this affiliation/role was not a source of bias. We did not identify any other potential sources of bias.
Characteristics of Included Studies
The summary of the characteristics of included studies is presented in Table 2.
Study Details
Three studies were conducted in the USA (Dumas et al. 2010; Gross et al. 2011), two studies were carried out in Australia (Morawska et al. 2011: S1&S2), two in Sweden (Salari and Backman, 2016: S1&S2), and one in Germany (Heinrichs, 2006). The studies were published between 2006 and 2016.
Participants
None of the studies reported conducting a sample size calculation prior to the study. Seven studies included a total of 1952 participants (Dumas et al. 2010; Gross et al. 2011; Heinrichs 2006; Morawska et al. 2011: S1&S2; Salari and Backman 2016: S2 Winslow et al. 2016). Sample size varied from 70 (Morawska et al. 2011: S1) to 706 participants (Salari and Backman 2016: S2). One study did not report sample size (Salari and Backman 2016: S1). The setting for recruitment was primarily educational institutions. Three studies recruited parents from primary schools (Morawska et al. 2011: S2; Salari and Backman 2016: S2; Winslow et al. 2016), two from childcare centres (Dumas et al. 2010; Gross et al. 2011), and one from preschools (Heinrichs 2006). One study was conducted online through local newspapers’ websites (Salari and Backman 2016: S1), while one study did not specify the source of recruitment (Morawska et al. 2011: S1).
Seven studies reported sociodemographic characteristics of the sample (Dumas et al. 2010; Gross et al. 2011; Heinrichs 2006; Morawska et al. 2011: S1&S2; Salari and Backman 2016: S2; Winslow et al. 2016). The majority of the participants were mothers, and the predominant ethnicity varied across studies. Regarding educational level, three studies indicated that the majority of the participants had tertiary education (Morawska et al. 2011: S1&S2; Salari and Backman 2016: S2), while two studies presented a higher percentage of participants with equal and less than a high school education (Heinrichs 2006; Winslow et al. 2016).
Engagement Strategies
Several engagement strategies were tested. Three studies used monetary incentives, either as payment (Dumas et al. 2010; Heinrichs 2006) or as a discount (Gross et al. 2011). One study used setting options (individual vs. group) additional to monetary incentive conditions (Heinrichs 2006). Two studies used testimonials in video format (Morawska et al. 2011: S1&S2), while two studies used advertisements (Salari and Backman 2016: S1&S2). These four studies used dichotomy when communicating messages through their strategies, fear versus non-fear (Morawska et al. 2011: S1&S2), and promotion versus prevention (Salari and Backman 2016: S1&S2). One study used an engagement package, which included a family testimonial flyer, teacher endorsement, group leader engagement call, and brochure (Winslow et al. 2016). Seven studies clearly identified theoretical frameworks used to design engagement strategies, such as the theory of planned behaviour, the behavioural economics, the self-regulatory focus theory, and other theories of health-related behaviour (Dumas et al. 2010; Gross et al. 2011; Morawska et al. 2011: S1&S2; Salari and Backman 2016: S1&S2; Winslow et al. 2016).
Types of Comparator
Three studies compared an experimental to a control condition (Dumas et al. 2010; Gross et al. 2011; Winslow et al. 2016). Two studies used experimental groups allocated to different engagement strategies such as promotion versus prevention (Salari and Backman 2016: S1&S2). One study used two types of conditions (payment and setting) resulting in four experimental groups with a combination of payment type (payment vs. no payment) and setting (individual vs. group) (Heinrichs 2006). Two studies considered three conditions given by two intervention groups (either expert vs. parent testimonial or fear vs. non-fear expert testimonial) and one control group (Morawska et al. 2011: S1&S2).
Outcomes
The primary outcome of this review was any indicator of initial parental engagement presented by stage, recruitment, enrolment, and first attendance. In general, only one study included all three stages of initial parental engagement (Morawska et al. 2011: S2), while the rest of the studies only covered one stage (Morawska et al. 2011: S1; Salari and Backman 2016: S2) or two (Dumas et al. 2010; Gross et al. 2011; Heinrichs 2006; Salari and Backman 2016: S1; Winslow et al. 2016). In summary, only three engagement strategies showed a significant effect on one stage of initial parental engagement. A promotion-focused advertisement, monetary incentive, and engagement package showed a significant impact on recruitment, enrolment, and first attendance, respectively. All other engagement strategies showed no significant effect. Table 3 summarises the effectiveness of each engagement strategy by stages of initial engagement.
Discussion
This systematic review aimed to identify engagement strategies tested to enhance initial stages of parental engagement, particularly recruitment, enrolment, and first attendance, in the context of parenting interventions for parents of young children. Although numerous studies and reviews have highlighted the importance of engagement and the need to better understand how to enhance parental engagement in parenting interventions (Chacko et al. 2016; Ingoldsby 2010; Morawska and Sanders 2006), the current review showed that rigorous experimental studies are still scarce.
The issue of parental engagement to interventions arose in the literature in the mid-late 1990s (Dumka et al. 1997; McKay et al. 1996; Prinz and Miller 1994); however, experimental studies to test engagement strategies have only been published since 2006. Although numerous engagement strategies are currently used by researchers and practitioners when implementing parenting interventions (Ingoldsby 2010; Morawska and Sanders 2006); only a limited number of these strategies have been tested in the studies included in this review. As a result, few engagement strategies showed a significant impact on initial engagement, while most did not. None of the strategies appeared to have a significant impact on all the stages of initial parental engagement included in each study.
Our review showed that the selection of engagement strategies currently in use is not based on evidence of their effectiveness. Despite many calls in the literature to increase the focus on engagement of parents, little experimental work has been done to date to advance the field. Although monetary incentives showed some effect on enrolment (Dumas et al. 2010; Heinrichs 2006), these incentives tend to be not feasible in the context of parenting interventions where the resources are limited, and those resources can be allocated to increase programme coverage in order to allow more parents to access these evidence-based interventions (Foster et al. 2008). In addition, payment for participation may undermine parental self-regulation and personal responsibility to make informed decisions regarding their engagement in a parenting intervention. If parents are offered an intervention that is already free or low cost, receiving money for enrolling and attending that intervention may undermine their interest and how they value it (Dumas et al. 2010; Heinrichs 2006). Similarly, setting a fixed monetary incentive may underestimate the variable effort and time that parents invest in enrolling and attending a parenting intervention (Gross et al. 2011).
The engagement package used by Winslow et al. (2016) seemed to reduce the gap between parents’ intention to engage and their actual engagement in a parenting intervention. However, the effect was attributed to the package as a whole, which does not account for the potential effect that each strategy may have by itself. For instance, Morawska et al. (2011: S1&S2) found that testimonial from a parent did not show an impact on any stage of initial parental engagement, but a parent testimonial flyer was included within the engagement package by Winslow et al. (2016). This link brings the question whether the source of the testimonial or the format impacted on the engagement. Winslow et al. (2016) pointed out that the strategies included in the package varied in terms of the resources required to implement them. Thus, the cost-effectiveness of the whole package remains uncertain.
A systematic review is only as good as the quality of the included studies. The relatively low methodological quality of the studies highlighted by numerous limitations (e.g. lack of published protocols, lack of power calculations, randomisation procedures not described in sufficient detail) means that the impact of their outcomes needs to be treated with some caution.
The main limitation of the current review is that given the limited published evidence on engagement strategies we are not able to provide a definitive statement on what strategies are effective. There are other limitations relevant to address. We focused on experimental studies in order to ensure inclusion of rigorous studies. This resulted in a limited number of studies included in the analysis; however, conclusions from non-randomised controlled trials may be risky and still lead to inconclusive outcomes. This review only focused on journal articles from databases, while guidelines for systematic reviews (Higgins and Green 2008, 2011; Moher et al. 2015) suggest to include other sources of information, such as the grey literature. However, we restricted the searches to databases in order to secure the quality and validity of the search procedure and thus prioritise articles which were published after undergoing a peer-reviewed process. Even though one limitation of this review is that only two languages were included; there was only one article (Heinrichs et al. 2006) in another language that was excluded for this reason. Still, its inclusion may have contributed additional information to reported outcomes.
Several strengths emerge in this review. First, this systematic review provided existing evidence regarding the engagement strategies tested in experimental trials and their effectiveness. Given that this review was restricted to studies published in peer-reviewed journals, this review contributed outcomes based on the existing evidence, even if limited. Second, the systematic review protocol was registered before conducting the searches, which facilitated the monitoring of the planned review and how it was conducted. Third, the search procedure followed the most critical recommendations from guidelines (Higgins and Green 2008, 2011; Moher et al. 2015), including that two reviewers conducted the full-text selection, dealing with discrepancies, and measuring agreement between reviewers. Fourth, this review included multiple interdisciplinary databases focused on education, health sciences, and social sciences. This wide range of databases provided a comprehensive summary of the experimental studies that have been conducted on the topic. Lastly, this review included an assessment of risk of bias (Higgins and Green 2008, 2011), which contributed to evaluating the validity of the existing evidence. Although some existing reviews in engagement have not conducted this assessment (Becker et al. 2015, 2017; Chacko et al. 2016; Haine-Schlagel and Walsh 2015; Lindsey et al. 2014), the judgement of the risk of bias is valued as best practice when reporting outcomes of systematic reviews in order to obtain reliable conclusions (Higgins et al. 2011).
Implications
The evidence from this review suggests that engagement strategies may have a differential impact on different stages of initial parental engagement and multiple approaches across stages may be needed. This outcome supports the multistage feature of parental engagement (Eisner and Meidert 2011) and the conception that engagement changes over time (Becker et al. 2014; Chacko et al. 2012). However, it may also challenge the implementation of strategies given the particular characteristics of each stage. Following this argument, Salari and Backman (2016) pointed out that a prevention-focused advertisement initially captured parents’ attention, but a promotion-focused one inspired more parents to consider engaging in a parenting intervention. Similarly, the use of the same engagement strategies across stages of initial parental engagement may not be appropriate if stages differ from each other.
This review illustrated that very limited attention to date has been focused on empirical testing of engagement approaches, despite multiple calls for enhanced focus and attention to improving engagement (Chacko et al. 2016; Ingoldsby 2010; Morawska and Sanders 2006). Of the five engagement strategies tested, only three showed some effect on a stage of engagement. Due to the limited time and resources available for researchers and practitioners to engage parents in evidence-based parenting interventions (Salari and Backman 2016), a better understanding of how to engage parents and the mechanisms that can enhance it from early stages of a parenting intervention would facilitate to reach as many parents as possible using appropriately the resources available for that engagement process.
Future Directions
This review highlighted several remaining gaps. Although previous reviews have pointed out to the relevance of building a shared understanding of parental engagement (Chacko et al. 2016; Haine-Schlagel and Walsh 2015; Ingoldsby 2010), our review identified that it remains as a pending task. We acknowledge the theoretical advancement recently published by Piotrowska et al. (2017). This conceptual model of parental engagement provides a comprehensive approach to parental engagement. However, the attention given to initial parental engagement is insufficient to inform current practice and research. Thus, we propose that a theoretical model providing a deeper analysis of recruitment, enrolment, and first attendance would contribute to increase the understanding of initial parental engagement and thus parenting interventions would be able to reach more parents.
Given the attitudinal and behavioural nature of initial parental engagement, research needs to focus on modifiable variables and thus to understand how mechanisms of change evolve through the stages of engagement (Haine-Schlagel and Walsh 2015). To ascertain a consumer perspective (Sanders and Kirby 2012) into parental engagement, variables related to parents’ individual characteristics, programme preferences, and previous programme experiences have to be analysed in a single study to determine which parent-related variables are critical for initial parental engagement. Parents’ cognitions and their parenting practices influence their engagement throughout an intervention (Chacko et al. 2017), but the underlying processes of this influence still need to be further explored. For instance, matching parents’ individual characteristics and their preferences for certain formats have shown a positive impact on intention to participate in training, but there is no evidence if this intention translates into attending (Wymbs et al. 2015, 2016). When parents are exposed to programme content, they seem more motivated to stay in the programme (Garvey et al. 2006; Heinrichs 2006) and they are more likely to involve in a programme in the future (Chislett and Kennett 2007). Thus, some efforts have been conducted to contribute emerging evidence, but outcomes are still inconclusive in the context of initial parental engagement.
Once this consumer perspective is incorporated into the theoretical development of initial parental engagement, more rigorous experimental studies testing engagement strategies have to be conducted. These studies need to include a variety of formats, messages, and sources of information, prioritising those formats, messages, and sources suitable for wide and cost-effective implementation at a population level in order to advance in the initial engagement of parents to access and benefit from evidence-based parenting interventions. For instance, Morawska et al. (2011) used testimonial videos showing not significant effect on initial parental engagement; however, a recent study conducted by Winslow et al. (2017) reported a positive effect of this format. The engagement videos consisted of information and (parent and expert) testimonials, which integrated the social influence principles and health behaviour theories. However, this study showed some limitations in the context of the current review. The sample may not be representative of our targeted parents as this study was oriented to litigating parents referred by court mandate to the intervention, and the age range of their children was from 3 to 18 years old. Still, this study represents advancements in terms of providing further evidence on this topic using a more comprehensive approach (three experimental conditions and two control conditions) and more rigorous methodological design.
The theoretical approaches used in the design of the experimental studies included in this review did not include any of the recent theories of parental engagement, such as the integrated theory of parent involvement (McCurdy and Daro 2001), the conceptual framework of the engagement (Staudt 2007), and the model of parental engagement (Piotrowska et al. 2017). Instead, they incorporated mainly health behaviour theories, such as theory of planned behaviour, health belief theory, and other health behaviour approaches. Still, it showed that the call for more theory-driven efforts (Morawska and Sanders 2006) had been increasingly addressed in the research conducted in the last decade. Research has evaluated the impact of these health behaviour theories on engagement (Salari and Filus 2017; Spoth et al. 2000; Thornton and Calam 2011; Wellington et al. 2006), but not in experimental studies using purely the factors from those theories to design the engagement strategies. For instance, Thornton and Calam (2011) compared the predictive validity of the theory of planned behaviour and the health belief model on engagement, showing that both theories predicted intention to participate, but the theory of planned behaviour showed a greater effect. However, this kind of comparison has not been placed in an experimental setting yet. Further research needs to provide specific and clear links between the elements of these theories and the particular challenges of engaging parents in early stages of parenting in parenting interventions.
There are macro-contextual systems, such as health system, educational system, and parenting education that may have influenced the study results due to differences in the support available for parents and their acceptability of accessing this support. These variables may play a moderating role as engagement strategies are implemented in an ecological context (Morawska et al. 2011), but we still do not how they play that role. For instance, although all Swedish parents access to parenting support during the first year of life of their child, and there is a national strategy in place to offer evidence-based parenting interventions, their rates of parents’ participation in parenting programmes are still similar to other western countries, such as the USA (Salari and Filus 2017). This is surprising given that both countries have also shown cultural differences in particular values (Hofstede et al. 2010) that may incentive/prevent them from accessing support from systems external to the family network.
Conclusion
The evidence showed that there is an increasing interest to test engagement strategies to enhance parental engagement in initial stages of parental engagement in the last decade. A promotion-focused advertisement for recruitment, monetary incentive for enrolment, and engagement package for first attendance appear more promising; however, methodological flaws prohibit a clear confirmation that they are effective and we need to implement these strategies with cautious. Therefore, outcomes are not sufficient to inform researchers and practitioners regarding evidence-based engagement strategies to effectively increase recruitment, enrolment, and first attendance in parenting interventions. There is a significant need for further research oriented to provide evidence and strategies to secure the gradual access of more parents to existing evidence-based parenting interventions. More theory-driven research is needed in order to translate initial parental engagement from the least understood aspect of parental engagement (Chacko et al. 2016) to one where an effective approach can be implemented to engage parents in accessing the level of support they require.
References
Becker, K. D., Boustani, M., Gellatly, R., & Chorpita, B. F. (2017). Forty years of engagement research in children’s mental health services: Multidimensional measurement and practice elements. Journal of Clinical Child and Adolescent Psychology, 47, 1–23. https://doi.org/10.1080/15374416.2017.1326121.
Becker, K. D., Kiser, L. J., Herr, S. R., Stapleton, L. M., Barksdale, C. L., & Buckingham, S. (2014). Changes in treatment engagement of youths and families with complex needs. Children and Youth Services Review, 46, 276–284. https://doi.org/10.1016/j.childyouth.2014.09.005.
Becker, K. D., Lee, B. R., Daleiden, E. L., Lindsey, M., Brandt, N. E., & Chorpita, B. F. (2015). The common elements of engagement in children’s mental health services: Which elements for which outcomes? Journal of Clinical Child and Adolescent Psychology, 44(1), 30–43. https://doi.org/10.1080/15374416.2013.814543.
Bérubé, A., Lafantaisie, V., Dubeau, D., Coutu, S., Caron, J., & Devault, A. (2014). Using implementation evaluation to uncover a child neglect prevention program. Evaluation and Program Planning, 45, 1–8. https://doi.org/10.1016/j.evalprogplan.2014.03.001.
Bruzzese, J. M., Gallagher, R., McCann-Doyle, S., Reiss, P. T., & Wijetunga, N. A. (2009). Effective methods to improve recruitment and retention in school-based substance use prevention studies. Journal of School Health, 79(9), 400–407. https://doi.org/10.1111/j.1746-1561.2009.00427.x.
Calam, R., Miller, C., Sadhnani, V., Sanders, M. R., & Carmont, S.-A. (2008). Can technology and the media help reduce dysfunctional parenting and increase engagement with preventative parenting interventions? Child Maltreatment, 13(4), 347–361. https://doi.org/10.1177/1077559508321272.
Chacko, A., Jensen, S. A., Lowry, L. S., Cornwell, M., Chimklis, A., Chan, E., et al. (2016). Engagement in behavioral parent training: Review of the literature and implications for practice. Clinical Child and Family Psychology Review, 19(3), 204–215. https://doi.org/10.1007/s10567-016-0205-2.
Chacko, A., Wymbs, B. T., Chimiklis, A., Wymbs, F. A., & Pelham, W. E. (2012). Evaluating a comprehensive strategy to improve engagement to group-based behavioral parent training for high-risk families of children with ADHD. Journal of Abnormal Child Psychology, 40(8), 1351–1362. https://doi.org/10.1007/s10802-012-9666-z.
Chacko, A., Wymbs, B., Rajwan, E., Wymbs, F., & Feirsen, N. (2017). Characteristics of parents of children with ADHD who never attend, drop out, and complete behavioral parent training. Journal of Child and Family Studies, 26(3), 950–960. https://doi.org/10.1007/s10826-016-0618-z.
Chislett, G., & Kennett, D. J. (2007). The effects of the Nobody’s Perfect Program on parenting resourcefulness and competency. Journal of Child and Family Studies, 16(4), 473–482. https://doi.org/10.1007/s10826-006-9098-x.
Chu, J., Farruggia, S., Sanders, M., & Ralph, A. (2014). Towards a public health approach to parenting programmes for parents of adolescents. Journal of Public Health, 36(3), 522. https://doi.org/10.1093/pubmed/fdu084.
Cowan, P. A., Cowan, C. P., Pruett, K., Pruett, M. K., Wong, J. J., & LaRossa, R. (2009). Promoting fathers’ engagement with children: Preventive interventions for low-income families. Journal of Marriage and Family, 71(3), 663–679. https://doi.org/10.1111/j.1741-3737.2009.00625.x.
Cullen, S. M., Cullen, M. A., & Lindsay, G. (2016). Universal parenting programme provision in England: Barriers to parent engagement in the CANparent trial, 2012–2014. Children and Society, 30(1), 71–81. https://doi.org/10.1111/chso.12120.
De Brún, C., & Pearce-Smith, N. (2014). Searching skills toolkit: Finding the evidence (Vol. 2nd). Chichester: BMJ Books/Wiley-Blackwell.
Dittman, C., Keown, L. J., Sanders, M., Rose, D., Farruggia, S. P., & Sofronoff, K. (2011). An epidemiological examination of parenting and family correlates of emotional problems in young children. American Journal of Orthopsychiatry, 81(3), 360–371. https://doi.org/10.1111/j.1939-0025.2011.01104.x.
Dumas, J. E., Moreland, A., French, B., & Pearl, A. (2010). Effects of monetary incentives on engagement in the PACE parenting program. Journal of Clinical Child and Adolescent Psychology, 39(3), 302–313. https://doi.org/10.1080/15374411003691792.
Dumas, J. E., Nissley-Tsiopinis, J., & Moreland, A. D. (2007). From intent to enrollment, attendance, and participation in preventive parenting groups. Journal of Child and Family Studies, 16(1), 1–26. https://doi.org/10.1007/s10826-006-9042-0.
Dumka, L. E., Garza, C. A., Roosa, M. W., & Stoerzinger, H. D. (1997). Recruitment and retention of high-risk families into a preventive parent training intervention. The Journal of Primary Prevention, 18(1), 25–39. https://doi.org/10.1023/A:1024626105091.
Eisner, M., & Meidert, U. (2011). Stages of parental engagement in a universal parent training program. The Journal of Primary Prevention, 32(2), 83–93. https://doi.org/10.1007/s10935-011-0238-8.
Foster, E. M., Prinz, R. J., Sanders, M. R., & Shapiro, C. J. (2008). The costs of a public health infrastructure for delivering parenting and family support. Children and Youth Services Review, 30(5), 493–501. https://doi.org/10.1016/j.childyouth.2007.11.002.
Frank, T. J., Keown, L. J., Dittman, C. K., & Sanders, M. R. (2015a). Using father preference data to increase father engagement in evidence-based parenting programs. Journal of Child and Family Studies, 24(4), 937–947. https://doi.org/10.1007/s10826-014-9904-9.
Frank, T. J., Keown, L. J., & Sanders, M. R. (2015b). Enhancing father engagement and interparental teamwork in an evidence-based parenting intervention: A randomized-controlled trial of outcomes and processes. Behavior Therapy, 46(6), 749–763. https://doi.org/10.1016/j.beth.2015.05.008.
Garvey, C., Julion, W., Fogg, L., Kratovil, A., & Gross, D. (2006). Measuring participation in a prevention trial with parents of young children. Research in Nursing and Health, 29(3), 212–222. https://doi.org/10.1002/nur.20127.
Girvin, H., DePanfilis, D., & Daining, C. (2007). Predicting program completion among families enrolled in a child neglect preventive intervention. Research on Social Work Practice, 17(6), 674–685. https://doi.org/10.1177/1049731507300285.
Gross, D., Johnson, T., Ridge, A., Garvey, C., Julion, W., Treysman, A. B., et al. (2011). Cost-effectiveness of childcare discounts on parent participation in preventive parent training in low-income communities. The Journal of Primary Prevention, 32(5–6), 283–298. https://doi.org/10.1007/s10935-011-0255-7.
Guyll, M., Spoth, R., & Redmond, C. (2003). The effects of incentives and research requirements on participation rates for a community-based preventive intervention research study. The Journal of Primary Prevention, 24(1), 25–41. https://doi.org/10.1023/A:1025023600517.
Haine-Schlagel, R., & Walsh, N. (2015). A review of parent participation engagement in child and family mental health treatment. Clinical Child and Family Psychology Review, 18(2), 133–150. https://doi.org/10.1007/s10567-015-0182-x.
Heinrichs, N. (2006). The effects of two different incentives on recruitment rates of families into a prevention program. The Journal of Primary Prevention, 27(4), 345–365. https://doi.org/10.1007/s10935-006-0038-8.
Heinrichs, N., Bertram, H., Kuschel, A., & Hahlweg, K. (2005). Parent recruitment and retention in a universal prevention program for child behavior and emotional problems: Barriers to research and program participation. Prevention Science, 6(4), 275–286. https://doi.org/10.1007/s11121-005-0006-1.
Heinrichs, N., Krüger, S., & Guse, U. (2006). Der Einfluss von Anreizen auf die Rekrutierung von Eltern und auf die Effektivität eines präventiven Elterntrainings. [The effect of incentives on recruitment of parents and effectiveness of preventive parent training.]. Zeitschrift für Klinische Psychologie und Psychotherapie: Forschung und Praxis, 35(2), 97–108. https://doi.org/10.1026/1616-3443.35.2.97.
Higgins, J. P., Altman, D. G., Gøtzsche, P. C., Jüni, P., Moher, D., & Oxman, A. D. (2011). Cochrane Bias Methods: The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. British Medical Journal, 343(7829), 889–893. https://doi.org/10.1136/bmj.d5928.
Higgins, J., & Green, S. (2008). Cochrane handbook for systematic reviews of interventions: Cochrane book series. In J. P. T. Higgins & S. Green (Eds.), Chichester. England: Wiley.
Higgins, J., & Green, S. (2011). Cochrane handbook for systematic reviews of interventions Version 5.1. 0 [updated March 2011].
Hofstede, G., Hofstede, G. J., & Minkov, M. (2010). Cultures and organizations: Software of the mind (3rd ed.). New York: McGraw-Hill.
Ingoldsby, E. (2010). Review of interventions to improve family engagement and retention in parent and child mental health programs. Journal of Child and Family Studies, 19(5), 629–645. https://doi.org/10.1007/s10826-009-9350-2.
Lefever, J. B., Bigelow, K. M., Carta, J. J., & Borkowski, J. G. (2013). Prediction of early engagement and completion of a home visitation parenting intervention for preventing child maltreatment. NHSA Dialog, 16(1), 1–19.
Lindsey, M. A., Brandt, N. E., Becker, K. D., Lee, B. R., Barth, R. P., Daleiden, E. L., et al. (2014). Identifying the common elements of treatment engagement interventions in children’s mental health services. Clinical Child and Family Psychology Review, 17(3), 283–298. https://doi.org/10.1007/s10567-013-0163-x.
McCurdy, K., & Daro, D. (2001). Parent involvement in family support programs: An integrated theory. Family Relations, 50(2), 113–121.
McKay, M. M., McCadam, K., & Gonzales, J. J. (1996). Addressing the barriers to mental health services for inner city children and their caretakers. Community Mental Health Journal, 32(4), 353–361. https://doi.org/10.1007/BF02249453.
Miller, G. E., & Prinz, R. J. (2003). Engagement of families in treatment for childhood conduct problems. Behavior Therapy, 34(4), 517–534. https://doi.org/10.1016/S0005-7894(03)80033-3.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & Prisma Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ. British Medical Journal, 339(7716), 332–336. https://doi.org/10.1136/bmj.b2535.
Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., et al. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Reviews, 4(1), 1. https://doi.org/10.1186/2046-4053-4-1.
Morawska, A., Nitschke, F., & Burrows, S. (2011). Do testimonials improve parental perceptions and participation in parenting programmes? Results of two studies. Journal of Child Health Care, 15(2), 85–98. https://doi.org/10.1177/1367493510397625.
Morawska, A., & Sanders, M. R. (2006). A review of parental engagement in parenting interventions and strategies to promote it. Journal of Children’s Services, 1(1), 29–40. https://doi.org/10.1108/17466660200600004.
Mytton, J., Ingram, J., Manns, S., & Thomas, J. (2014). Facilitators and barriers to engagement in parenting programs: A qualitative systematic review. Health Education and Behavior, 41(2), 127–137. https://doi.org/10.1177/1090198113485755.
Ohan, J., Seward, R., Stallman, H. M., Bayliss, D., & Sanders, M. (2015). Parents’ barriers to using school psychology services for their child’s mental health problems. School Mental Health, 7(4), 287–297. https://doi.org/10.1007/s12310-015-9152-1.
Olofsson, V., Skoog, T., & Tillfors, M. (2016). Implementing group based parenting programs: A narrative review. Children and Youth Services Review, 69, 67–81. https://doi.org/10.1016/j.childyouth.2016.07.004.
Piotrowska, P. J., Tully, L. A., Lenroot, R., Kimonis, E., Hawes, D., Moul, C., et al. (2017). Mothers, fathers, and parental systems: A conceptual model of parental engagement in programmes for child mental health—Connect, Attend, Participate, Enact (CAPE). Clinical Child and Family Psychology Review, 20, 146–161. https://doi.org/10.1007/s10567-016-0219-9.
Prinz, R. J., & Miller, G. E. (1994). Family-based treatment for childhood antisocial behavior: Experimental influences on dropout and engagement. Journal of Consulting and Clinical Psychology, 62(3), 645–650. https://doi.org/10.1037/0022-006X.62.3.645.
Prinz, R. J., Sanders, M., Shapiro, C., Whitaker, D., & Lutzker, J. (2009). Population-based prevention of child maltreatment: The U.S. Triple P System Population Trial. Prevention Science, 10(1), 1–12. https://doi.org/10.1007/s11121-009-0123-3.
Salari, R., & Backman, A. (2016). Direct marketing of parenting programs: Comparing a promotion-focused and a prevention-focused strategy. European Journal of Public Health, 27(3), 489–494. https://doi.org/10.1093/eurpub/ckw149.
Salari, R., & Filus, A. (2017). Using the Health Belief Model to explain mothers’ and fathers’ intention to participate in universal parenting programs. Prevention Science, 18(1), 83–94. https://doi.org/10.1007/s11121-016-0696-6.
Sanders, M. R. (2012). Development, evaluation, and multinational dissemination of the Triple P-Positive Parenting Program. Annual Review of Clinical Psychology, 8, 345. https://doi.org/10.1146/annurev-clinpsy-032511-143104.
Sanders, M. R., & Kirby, J. N. (2012). Consumer engagement and the development, evaluation, and dissemination of evidence-based parenting programs. Behavior Therapy, 43(2), 236–250. https://doi.org/10.1016/j.beth.2011.01.005.
Sanders, M. R., & Kirby, J. (2015). Surviving or thriving: Quality assurance mechanisms to promote innovation in the development of evidence-based parenting interventions. Prevention Science, 16(3), 421–431. https://doi.org/10.1007/s11121-014-0475-1.
Sanders, M. R., Kirby, J. N., Tellegen, C. L., & Day, J. J. (2014). The Triple P-positive parenting program: A systematic review and meta-analysis of a multi-level system of parenting support. Clinical Psychology Review, 34(4), 337–357. https://doi.org/10.1016/j.cpr.2014.04.003.
Sanders, M. R., Tully, L. A., Pollard, G. E., Baade, P. D., Heywood, A. H., Lynch, M. E., et al. (1999). A survey of parenting practices in Queensland: Implications for mental health promotion. Health Promotion Journal of Australia: Official Journal of Australian Association of Health Promotion Professionals, 9(2), 105–114.
Shaffer, A., Kotchick, B. A., Dorsey, S., & Forehand, R. (2001). The past, present, and future of behavioral parent training: Interventions for child and adolescent problem behavior. The Behavior Analyst Today, 2(2), 91–105. https://doi.org/10.1037/h0099922.
Spoth, R., Redmond, C., & Shin, C. (2000). Modeling factors influencing enrollment in family-focused preventive intervention research. Prevention Science, 1(4), 213–225. https://doi.org/10.1023/A:1026551229118.
Staudt, M. (2007). Treatment engagement with caregivers of at-risk children: Gaps in research and conceptualization. Journal of Child and Family Studies, 16(2), 183–196. https://doi.org/10.1007/s10826-006-9077-2.
The Cochrane Collaboration. (2014). Review Manager (RevMan) [Computer program] (Version 5.3). Copenhagen: The Nordic Cochrane Centre.
Thornton, S., & Calam, R. (2011). Predicting intention to attend and actual attendance at a universal parent-training programme: A comparison of social cognition models. Clinical Child Psychology and Psychiatry, 16(3), 365–383. https://doi.org/10.1177/1359104510366278.
UNESCO Institute of Statistics. (2018). Education dataset. Retrieved from: http://data.uis.unesco.org/. Accessed 12 Jan 2018.
Wellington, L., White, K. M., & Liossis, P. (2006). Beliefs underlying intentions to participate in group parenting education. Australian e-Journal for the Advancement of Mental Health, 5(3), 275–283. https://doi.org/10.5172/jamh.5.3.275.
Winslow, E. B., Braver, S., Cialdini, R., Sandler, I., Betkowski, J., Tein, J. Y., et al. (2017). Video-based approach to engaging parents into a preventive parenting intervention for divorcing families: Results of a randomized controlled trial. Prevention Science. https://doi.org/10.1007/s11121-017-0791-3.
Winslow, E. B., Poloskov, E., Begay, R., Tein, J.-Y., Sandler, I., & Wolchik, S. (2016). A randomized trial of methods to engage Mexican American parents into a school-based parenting intervention. Journal of Consulting and Clinical Psychology, 84(12), 1094. https://doi.org/10.1037/ccp0000140.
World Health Organization. (2009). Preventing violence through the development of safe, stable and nurturing relationships between children and their parents and caregivers. Geneva: World Health Organization.
Wymbs, F. A., Chen, Y., Rimas, H. M., Deal, K., Waschbusch, D. A., & Pelham, W. E. (2016). Examining parents’ preferences for group parent training for ADHD when individual parent training is unavailable. Journal of Child and Family Studies. https://doi.org/10.1007/s10826-016-0588-1.
Wymbs, F. A., Cunningham, C. E., Chen, Y., Rimas, H. M., Deal, K., Waschbusch, D. A., et al. (2015). Examining parents’ preferences for group and individual parent training for children with ADHD symptoms. Journal of Clinical Child and Adolescent Psychology. https://doi.org/10.1080/15374416.2015.1004678.
Acknowledgements
We would like to thank Miranda Newell, Librarian from the University of Queensland Library, for her assistance with developing search strategy and protocol. We also thank Bao Yi Tan, who collaborated as the second reviewer for selection of articles by full text.
Funding
CG is supported by a scholarship granted by CONICYT (Comisión Nacional de Investigación Científica y Tecnológica) Becas Chile 72160251. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
CG, AM, and DH contributed to the drafting of the protocol. CG ran the searches and retrieved potentially relevant studies. CG was one of the two reviewers for selection by full text. AM was the third reviewer to deal with discrepancies. CG conducted data extraction for selected studies. CG, AM, and DH wrote the review.
Corresponding author
Ethics declarations
Conflict of interest
The Parenting and Family Support Centre is partly funded by royalties stemming from published resources of the Triple P—Positive Parenting Program, which is developed and owned by The University of Queensland (UQ). Royalties are also distributed to the Faculty of Health and Behavioural Sciences at UQ and contributory authors of published Triple P resources. Triple P International (TPI) Pty Ltd is a private company licensed by Uniquest Pty Ltd on behalf of UQ, to publish and disseminate Triple P worldwide. The authors of this report have no share or ownership of TPI. Alina Morawka and Divna M. Haslam receive royalties from TPI. TPI had no involvement in the study design, collection, analysis or interpretation of data, or writing of this report. Alina Morawska and Divna M. Haslam are employees at UQ. Carolina Gonzalez is a student at UQ.
Rights and permissions
About this article

Cite this article
Gonzalez, C., Morawska, A. & Haslam, D.M. Enhancing Initial Parental Engagement in Interventions for Parents of Young Children: A Systematic Review of Experimental Studies. Clin Child Fam Psychol Rev 21, 415–432 (2018). https://doi.org/10.1007/s10567-018-0259-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10567-018-0259-4