
Abstract
Mast cells are of paramount importance to allergies, pathogen immune responses during infections, and angiogenesis, as well as innate and adaptive immune regulations. Beyond all these roles, mast cells are now more and more being recognized as modulators of tumor microenvironment. Notwithstanding mounting evidences of mast cell accumulation in tumors, their exact role in tumor microenvironment is still incompletely understood. In this review, we discuss the significant role of mast cells in the remodeling of tumor microenvironment by either releasing various factors after activation or interacting with other cells within tumor and, as a result, the possible role of mast cell in cancer invasion and metastasis. We also discuss recent findings that mast cells actively release microparticles, which account for the transfer of membrane-type receptor signal and regulatory molecules such as microRNAs to tumor cells and immune cells. These findings on mast cells provide further insights into the complexity of tumor microenvironment remodeling.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Mast cells are derived from bone-marrow hematopoietic progenitors but migrate, whilst still immature, from vascular to peripheral tissues, where they mature and reside [1] close to blood vessels, nerves, and mucosal surfaces, such as the skin, respiratory tract, and gastrointestinal tract [2, 3], so as to be able to react quickly in the event of an attack by xenobiotics such as bacteria, parasites, viruses, and even seemingly innocuous pollen. From a physiological perspective, mast cells participate in tissue remodeling, wound healing, and angiogenesis [4–6], while from a pathological one, they are regarded as primarily IgE-mediated effectors in acute disorders and chronic allergic disorders [7], including their complex roles in autoimmune diseases [8], peripheral tolerance [9, 10], innate and adaptive immunities [11, 12].
Compelling evidence from other research highlights the association of mast cells with tumors [13, 14], opening new vistas for tumor therapies. Classical tumor pharmacotherapeutic attempts mainly targeted the tumor cells themselves. For instance, many studies focused on the oncogenes and tumor suppressor genes in order to try and reverse the malignant phenotypes. However, the primary focus of more recent research has seemingly shifted from tumor cell-centric to tumor microenvironment whose fibroblasts, endothelial cells, adipocytes, and abundant immune cells have been, albeit independently, well studied and understood [15–19]. Macrophages, DCs, lymphocytes, neutrophils, eosinophils, and mast cells, already known for their tumor-infiltrating immune properties and the parts they play in tumor-induced inflammation, are being studied anew for their roles in tumorigenesis, tumor malignant transformations, and tumor proliferation. Although much is already known about the accumulation of mast cells in tumors and their roles in tumor angiogenesis, much more particularly about mast cells and tumor microenvironment remain to be completely understood. Recent in-house studies have provided partial elucidation for the molecular and cellular mechanisms of mast cells in the remodeling of tumor microenvironment and the promotion of tumor growth [20, 21]. Furthermore, our preliminary data indicate a potential role of mast cell-derived microparticles in the signal transfer between mast cells and tumor cells within tumor microenvironment.
2 Mast cells remodel tumor microenvironment through degranulation and release of cytokines and chemokines
Mast cells are of an early infiltrating cell type prior to tumor development or at the periphery of many developing tumors, such as adenomatous polyps, skin dysplasias, malignant melanoma, breast carcinoma, and colorectal carcinoma [22]. Mast cells infiltrate into the boundary between normal tissues and tumors and express many proangiogenic compounds, which may play an early role in angiogenesis within developing tumors. Beyond their role in angiogenesis, mast cells seem to also be possessed of other functions in tumor microenvironment, many of which still are not well understood. Mast cells, for example, exert their function upon stimulatory signals. As previous in-house studies have demonstrated elsewhere, tumor cells generally produce stem cell factors (SCF), leading to the recruitment and activation of mast cells [20]. Although these in-house data identify the importance of SCF in the activation of tumor-infiltrating mast cells, other mitigating factors in tumor milieu are also potentially critical for mast cell migration and activation. It has been known, for example, that mast cells express a variety of receptors on their surfaces, such as Fc receptors [23, 24], complement receptors [25, 26], and Toll-like receptors [25, 27, 28] to sense stimuli. It is now clear that Toll-like receptors (TLRs) recognize not only pathogen-associated molecular patterns but also damage-associated molecular patterns (DAMPs) [29, 30]. Not surprisingly, there are an abundance of DAMPs in tumor microenvironment. For instance, the intracellular protein high mobility group box 1 and heat-shock protein (HSP), such as HSP60, HSP70, and HSP90 are actively released from live tumor cells or passively released from dead ones [31, 32]. These molecules, in turn, may act as TLR ligands for downstream signal transductions. Other molecules have also been identified as potential TLR ligands in tumor microenvironment, including the degraded products of extracellular matrix components [33] and nuclear materials [34].
Once activated by FcR ligands and TLR signaling, mast cells can release three classes of mediators: pre-formed mediators stored in granules, de novo synthesized lipid mediators and cytokines as well as chemokines [25]. All of these mediators can participate in the processes of tumor microenvironment remodeling, viz: (1) after secretion, tryptases and chymases (the major proteins stored in mast cell granules) promote inflammation, matrix destruction, and tissue remodeling and modulate immune responses by hydrolyzing chemokines and cytokines [35]; (2) leukotrienes, the commonly described mast cell-derived mediators, function predominantly at the local vascular endothelium, promoting the rolling and recruitment of neutrophils [36], inducing vascular permeability, triggering chemotaxis in various cells, and increasing mucus production [37]. In contrast, histamine modulates dendritic and T cell responses and promote chronic inflammatory reactions by enhancement of the secretion of pro-inflammatory cytokines such as interleukin (IL)-1β, IL-6, TNF-α as well as IL-8 [38]; and (3) mast cells may also produce immune suppressive cytokines, such as TGF-β and IL-10 [39], that favor immune suppression, and chemokines such as CCL5 and CXCL8 [40] that chemoattract additional effector immune cells, thus remodeling immune and inflammatory microenvironment. Furthermore, many of the above factors may also play a role in tumor angiogenesis. For example, degradation of the extracellular matrix, migration and proliferation and differentiation of vascular endothelial cells during angiogenesis require tryptase, heparin, vascular endothelial growth factor (VEGF), and basic fibroblast growth factor (bFGF) to be released from mast cell granules [41]. All in all, when stimulated by DAMPs or other stimuli in the tumor microenvironment, mast cells can become activated and undergo degranulation and release of cytokines and chemokines that, in turn, profoundly remodel tumor microenvironment.
3 Mast cells remodel tumor microenvironments through interaction with other cells within tumors
Complex cellular networks are integral features of tumor microenvironment, filled with an assortment of immunosuppressive and inflammatory cells. Myeloid-derived suppressor cells (MDSCs), tumor-associated macrophages, and regulatory T (Treg) cells are typical examples of such cells [42–44]. That mast cells affect effector T cells, dendritic cells, and B cells is well known. As critical cell type in tumor microenvironment, mast cells may also directly or indirectly interact with MDSCs, Tregs and others. But how mast cells affect immunosuppressive and inflammatory cells in tumor microenvironment remains largely unclear. SCF and its cognate receptor c-kit on mast cells are crucial for directing mast cell development from their hematopoietic progenitors, influencing numbers and phenotypes of mast cells [45]. Other effectors, such as IL-3, are also involved in mast cell development and survival [45, 46]. By increasing the secretion and production of VEGF and bFGF from mast cells, early studies have already demonstrated the involvement of SCF in tumor angiogenesis [47]. Clinical treatments targeting SCF that have achieved convincing therapeutic effects provide further corroboration [48, 49]. Recent in-house findings have highlighted the remodeling of tumor microenvironment by tumor cell-derived SCF [20]. The results showed that mast cell infiltration and activation in tumors were mainly mediated by tumor-derived SCF and the receptor c-kit on mast cells. Low-concentration SCF was effective in the chemotactic migration of mast cells into tumor sites, while high concentrations of SCF-activated mast cells, resulting in the synthesis of multiple pro-inflammatory factors, such as IL-6, TNF-α, VEGF, COX-2, iNOS, CCL2, and IL-17 that, in turn, have profoundly remodeled tumor inflammatory microenvironment [20, 50]. Furthermore, mast cell infiltration was found to upregulate the expression of transcription factor Foxp3, the critical marker of Tregs, concomitant with the suppression of T cell- and natural killer (NK) cell-mediated antitumor immune responses [20]. Such data suggest that mast cells may actually exacerbate tumor immunosuppressive microenvironment by regulating cytotoxic T and NK cells.
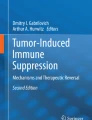
As a critical pro-inflammatory cytokine, IL-17 has recently attracted great attention and its role in allergic and autoimmune inflammation is intensively studied. IL-17 acts on a broad range of cells to induce the expression of cytokines (IL-6, IL-8, GM-CSF, G-CSF), chemokines, and metalloproteinases [51, 52]. These studies, therefore, suggest that the upregulation of IL-17 triggered by tumor-infiltrating mast cells might also be pivotal in tumor microenvironment remodeling. Interestingly, the in-house findings have shown that mast cell-induced IL-17 is not produced by Th17 cells but by MDSCs [21]. Such findings are summarized in Fig. 1, illustrating a closed loop amongst mast cells, MDSCs, and Treg cells in tumor microenvironment. Each of these components of the loop, in turn, has its own specific role it plays in the remodeling of the microenvironment: (1) mast cells promote the migration and suppressor function of tumor MDSCs by regulating the expression of CCL2 and Th2 cytokines; (2) CCL2 and other factors recruit more MDSCs to tumor microenvironment and further exacerbate tumor inflammatory microenvironment by IL-17 secretion, leading to the increased levels of CCL17 and CCL22; (3) CCL17 and CCL22, in turn, chemoattract more Tregs to tumor site; (4) IL-17 signaling upregulates CD39 and CD73 on Tregs for the enhanced suppressive function of Tregs; (5) IL-17 signaling upregulates the production of IL-9 by Tregs; and (6) IL-9 maintains the survival of mast cells in tumor microenvironment.

A model of mast cells remodeling tumor microenvironment. Under the guidance of SCF/c-kit signaling, mast cells migrate to and are activated in tumor microenvironment; the activated mast cells release a panel of factors, leading to CCL2 production and IL-17 upregulation in MDSCs; CCL2 signaling recruits more MDSCs, leading to more IL-17 production; IL-17 strengthens tumor inflammatory microenvironment, leading to the upregulation of IL-9, IL-10, IL-13, CCL17, CCL22, CD39, and CD73; IL-10 and IL-13 induce arginase 1 expression by MDSCs; CCL17 and CCL22 attract the migration of Treg cells; CD39 and CD73 enhance suppressor function of Treg cells; IL-9 produced by Treg cells maintains the survival of mast cells; MDSCs release active MMP9, through which soluble SCF is generated, thus further facilitating the migration and activation of mast cells; mast cells and/or other cells release microparticles. The latter transfer regulatory molecules such as microRNAs to proximal macrophages or others so to regulate the behavior of these cells, thus further remodeling tumor microenvironment
It is not too difficult to see from the above that mast cells, MDSCs, and Tregs form a vicious axis to develop in parallel both tumor inflammatory microenvironment and immunosuppressive microenvironment. A recent study from Khazaie's group has shown that colorectal cancer-infiltrating mast cells can contribute to systemic Treg dysfunctions [53]. They found that Tregs were unable to suppress mast cell degranulation and that the pro-inflammatory skewing of those Tregs was not dependent on either IL-17 or IL-6, suggesting the complex interaction between mast cells and Tregs in tumor microenvironment. Besides MDSCs and Treg cells, mast cells might also be communicating with other tumor infiltrating cells, such as macrophages, B cells, granulocytes, fibroblasts, adipocytes, and even tumor cells themselves. In this respect, reports from both Bentrem's and Melillo's groups have shown that crosstalk between human mast cells and cancer cells contributes to tumor progression [54, 55]. How those communications occur, however, as yet remains unclear though naturally worthy of further investigation.
4 Mast cell-derived microparticles mediate interaction of mast cells with other cells including tumor cells
Eukaryotic cells, when undergoing activation and apoptosis, may shed components of their plasma membranes encapsulating cytoplasmic elements into extracellular spaces [56, 57]. These shed vesicles vary from 100 to 1000 nm in size and are known as microparticles (MP) [58]. As a subcellular structure, MPs can be purified through centrifuging methods and detected by flow cytometric technology. Whilst plasma membrane-derived microparticles had been considered by many to be merely “cellular dust”, in-house preliminary data suggest that mast cells not only degranulate but also release MPs after activation. As components of the tumor microenvironment, mast cell-derived MPs may function at deeper levels of the tumor microenvironment and remodel tumor development from multiple aspects. Ligation of SCF to c-Kit leads to the activation of multiple pathways, including phosphatidyl-inositol-3 (PI3)-kinase, phospholipase C (PLC)-γ, Src kinase, Janus kinase (JAK)/signal transducers and activators of transcription (STAT) and mitogen-activated protein kinase pathways. Activation of these pathways results in multiple functional effects, like increased cell proliferation, differentiation, and survival [59]. Although almost all types of tumor cells are capable of producing SCF [20], most of them such as liver, breast, colon, and lung cancer cells do not express the receptor c-kit. An in-house study, as yet unpublished, has shown that when mast cell-derived MPs are added to the cultured H22 hepatocarcinoma tumor cells, MPs transfer mast cell membranes to tumor cell membranes. Since mast cells highly express c-kit, it is possible to speculate that mast cells transfer the receptor c-kit to vicinal tumor cells, enabling the tumor cells to obtain c-kit signaling in the manner of autocrine or paracrine secretion, leading to tumor cell growth and survival through the SCF/c-kit pathway. In addition to being a source of membrane receptors, MPs also function as a mediator capable of transferring intracellular components among cells. Reports have demonstrated that MPs contain parent cell mRNAs making it possible for MP-mediated mRNA to promote angiogenesis [60]. Studies conducted in-house further analyzed MPs-derived RNAs by microRNA microarray, and found that mast cells-derived MPs expressed various microRNAs that could be, in turn, transferred to phagocytes such as macrophages, DCs and, possibly even, tumor cells. In another in vitro in-house study, it was found that macrophages taking up MP-derived microRNAs were involved in the macrophage transition from M1 to M2 phenotypes. Moreover, studies conducted in-house have recently demonstrated that unstimulated mast cells are capable of taking up platelets-derived MPs that lead to the inhibition of inflammation [61]. Thus, MPs derived from mast cells and other cells might profoundly shape the biological characteristics of tumor-associated macrophages, tumor-infiltrating DCs, mast cells themselves, and even tumor cells, leading to the remodeling of tumor microenvironment. Elucidating how mast cells-derived microparticles exert their functions in tumor sites will undoubtedly expand our understanding of the remodeling of tumor microenvironment.
5 A potentially promoting effect by mast cell-remodeled tumor microenvironment on cancer invasion and metastasis
It is generally accepted that tumors are not just a problem raising from the particular tumor cells themselves but also an outcome of the microenvironment where tumor cells arise. As noted afore, mast cells play an important role in tumor progression by their remodeling tumor microenvironment. A number of contributors to the literature have demonstrated that mast cell infiltration to tumors is increased in comparison with normal tissues and accordingly appears to exert a protumor effect [62–65]. In addition to the excellent studies of the impact of mast cells on tumor angiogenesis, others have recently investigated the role of mast cells in tumor invasion and metastasis. Melillo and his colleagues found that in thyroid cancer patients, mast cells were present within the tumor and at the invasive front and tended to be positively correlated with increased invasiveness of cancer cells [55]. By using human mast cell lines HMC-1 and LAD-2 in in vitro assays, they found that mast cells increased BrdU incorporation in thyroid cancer cells and decreased the levels of serum starvation-induced apoptosis. Moreover, they found that mast cell-conditioned media facilitated thyroid cancer cell migration in Matrigel. In a similar study by Strouch et al., mast cell infiltration was showed to be significantly increased in the stroma of pancreatic cancer in comparison to adjacent normal pancreatic tissue and normal pancreatic tissue from patients with benign disease [54]. They also found that mast cell numbers were positively correlated with the advanced grade and worse median disease-specific survival in pancreatic cancer patients. Furthermore, in in vitro assays, they found that mast cells augmented the proliferation of the pancreatic ductal adenocarcinoma cell lines PANC-1 and AsPC1 and increased their invasion in Matrigel. In line with the positive effects of mast cells on human thyroid and pancreatic cancers, Xiang et al. reported that the release of tryptase by mast cells promoted the migration and invasion of breast cancer cells [66]. Mast cells seem to, therefore, be capable of promoting proliferation, survival and invasiveness of human cancer cells.
Migration and invasiveness of tumor cells are usually thought as the prerequisite of tumor metastasis. The aforementioned effect of mast cells on tumor cell motility implies a further relationship between mast cells and tumor metastasis. Furthermore, the effects of mast cells on tumor microenvironment also suggest a link between mast cells and tumor metastasis. However, to date, data on mast cells and metastasis have been scant and largely poor. Early studies have reported that not only were metastases reduced in mast cell-deficient mice [67] but when levels of mast cells were stabilized or inhibited, the metastases of rat mammary adenocarcinoma were also inhibited [68]. Recently, on the basis of the critical location of mast cells at the blood–brain barrier and the fact that mast cells can be stimulated by corticotropin-releasing hormone, secreted under stress, it has been suggested that perhaps, after stimulation mast cells release mediators such as histamine, IL-8, tryptase and VEGF to disrupt the blood–brain barrier, thus facilitating tumor cell brain metastases [69]. In addition, part clinical data have indicated a possible link of mast cells to metastasis. Yano et al. reported, for example, that mast cell numbers were higher in specimens in patients with advanced diseases and with metastases to the lymph nodes than in specimens in patients with early stages of the disease [70]. Although these studies are helpful to construct a model of tumor metastasis promotion by mast cells, the truth in mast cell promotion of metastasis may well be far more varied and much more complex. Both direct and indirect means can be employed by mast cells to facilitate metastasis. The direct means includes: (1) activated mast cells releasing proteases such as MMP9, tryptase, chymase, and cathepsin to degrade the extracellular matrix to facilitate tumor cell migration and invasion; (2) activated mast cells releasing vasoactive factors such as histamine, IL-8, VEGF, prostaglandin D, and substance P to lower endothelial barriers, thus facilitating tumor cell intravasation and extravasation; and (3) as mentioned above, transferring c-kit receptors on mast cells to tumor cells through microparticle pathways, thereby generating tentative c-kit signaling for tumor cell metastasis. The indirect means, on the other hand, includes: (1) activated mast cells releasing proangiogenic factors such as VEGF, PDGF, MMP9, and PGE2 to induce angiogenesis, thus facilitating tumor metastasis; (2) activated mast cells releasing pro-inflammatory factors such as IL-1β, TNF-α, and IL-18 to increase the interstitial fluid volume by plasma effusion and extending the distance of oxygen needed to be delivered to oxygen hungry cells, thus leading to hypoxia-induced metastasis; (3) activated mast cells releasing growth factors such as EGF, IGF, NGF, bFGF that favor tumor cell survivability, thus again facilitating metastasis; and (4) activated mast cells exacerbating tumor immunosuppression and thereby decreasing immune system destruction of tumor cells, thus facilitating metastasis. Mast cells, therefore, are advantaged in many ways that favor tumor metastasis. Which of these advantages are played probably depends on the context at that time.
The success of metastasis also depends on the survival of tumor cells in the secondary sites to which they have moved. Unpublished in-house data indicated that mast cells may be recruited to tumor cell-inoculated site as early as 2 h after inoculation, suggesting, in turn, that mast cells might play an important role in the initial survival of metastasized tumor cells at the secondary site. A key point for tumor cell survival in the secondary site is its ability to escape or ward off local immune surveillance. Unlike primary tumor site, that is full of immunosuppressive cells and molecules, distant secondary sites can be presumed to be immune competent, or at least retain their innate immunity-for example, NK cell activity being unimpaired. Mast cells probably are a critical regulator in helping tumors to overcome the dangers from the local immune system where they metastasize to. Mast cells are capable of secreting diverse biologically active products upon exposure to a variety of immunological or nonimmunological stimuli [25, 26]. After activation by tumor cell-derived SCF and other signals, mast cells can produce CCL2, not only by themselves but also by remodeling the local microenvironment [20]. As a result, MDSCs are recruited to the site via CCL2/CCR2 signaling pathway to establish a safe immune unresponsive new home for tumor cells [71]. Besides the effect on MDSCs, mast cells may also induce immunosuppression by producing inhibitory factors such as IL-10, TGF-β, and adenosine [20]. The in-house study has demonstrated that mast cells induce the inhibition of tumor-infiltrating T cells and NK cells by releasing adenosine [20]. The fact that mast cells encircle the endothelium enables mast cells to become the first responder to tumor cell invasion of the strange secondary site. Although the interaction between mast cells and the new invader can be predicted as being inevitable, the consequence of this interaction at the secondary site may be much more complicated and dependent on the context at that time.
6 Concluding remarks
Recent advances have established various important stromal cell types in regulating tumor microenvironment. But perhaps more important, than those cell types, is the observation that mast cells have a significant role in sculpting tumor microenvironment. Mast cells are present in most tumor types, and probably act as the scaffolding cell population by secreting a variety of effector molecules, interacting with other stromal cells and even tumor cells, and shedding microparticles (Fig. 1), thus guiding tumor initiation, progression and metastasis. However, to date, the real veil of tumor-infiltrating mast cells is still covered, especially in human cancers. Unveiling the complexity and complicity of mast cells in cancer should provide insights into understanding the formation and remodeling of tumor microenvironment. Hopefully this may open new avenues and novel approaches to cancer therapies or combined treatments against tumor growth and metastasis.
References
Metcalfe, D. D., Baram, D., & Mekori, Y. A. (1997). Mast cells. Physiological Reviews, 77, 1033–1079.
Heib, V., Becker, M., Taube, C., & Stassen, M. (2008). Advances in the understanding of mast cell function. British Journal Haematology, 142, 683–694.
Bauer, O., & Razin, E. (2000). Mast Cell-Nerve Interactions. News in Physiological Sciences, 15, 213–218.
Weller, K., Foitzik, K., Paus, R., Syska, W., & Maurer, M. (2006). Mast cells are required for normal healing of skin wounds in mice. The FASEB Journal, 20, 2366–2368.
Hebda, P. A., Collins, M. A., & Tharp, M. D. (1993). Mast cell and myofibroblast in wound healing. Dermatologic Clinics, 11, 685–696.
Blair, R. J., Meng, H., Marchese, M. J., Ren, S., Schwartz, L. B., Tonnesen, M. G., et al. (1997). Human mast cells stimulate vascular tube formation. Tryptase is a novel, potent angiogenic factor. The Journal of Clinical Investigation, 99, 2691–2700.
Williams, C. M., & Galli, S. J. (2000). The diverse potential effector and immunoregulatory roles of mast cells in allergic disease. The Journal of Allergy and Clinical Immunology, 105, 847–859.
Benoist, C., & Mathis, D. (2002). Mast cells in autoimmune disease. Nature, 420, 875–878.
de Vries, V., Pino-Lagos, K., Elgueta, R., & Noelle, R. J. (2009). The enigmatic role of mast cells in dominant tolerance. Current Opinion in Organ Transplantation, 14, 332–337.
Sayed, B. A., Christy, A., Quirion, M. R., & Brown, M. A. (2008). The master switch: the role of mast cells in autoimmunity and tolerance. Annual Review of Immunology, 26, 705–739.
Palker, T. J., Dong, G., & Leitner, W. W. (2010). Mast cells in innate and adaptive immunity to infection. European Journal of Immunology, 40, 13–18.
Galli, S. J., Nakae, S., & Tsai, M. (2005). Mast cells in the development of adaptive immune responses. Nature Immunology, 6, 135–142.
Conti, P., Castellani, M. L., Kempuraj, D., Salini, V., Vecchiet, J., Tete, S., et al. (2007). Role of mast cells in tumor growth. Annals of Clinical and Laboratory Science, 37, 315–322.
Johansson, A., Rudolfsson, S., Hammarsten, P., Halin, S., Pietras, K., Jones, J., et al. (2010). Mast cells are novel independent prognostic markers in prostate cancer and represent a target for therapy. The American Journal of Pathology, 177, 1031–1041.
Murdoch, C., Muthana, M., Coffelt, S. B., & Lewis, C. E. (2008). The role of myeloid cells in the promotion of tumour angiogenesis. Nature Reviews. Cancer, 8, 618–631.
Mayani, H., Guilbert, L. J., & Janowska-Wieczorek, A. (1992). Biology of the hemopoietic microenvironment. European Journal of Haematology, 49, 225–233.
Siclari, V. A., Guise, T. A., & Chirgwin, J. M. (2006). Molecular interactions between breast cancer cells and the bone microenvironment drive skeletal metastases. Cancer and Metastasis Reviews, 25, 621–633.
Noel, A., Jost, M., & Maquoi, E. (2008). Matrix metalloproteinases at cancer tumor-host interface. Seminars in Cell & Developmental Biology, 19, 52–60.
Hanna, E., Quick, J., & Libutti, S. K. (2009). The tumour microenvironment: a novel target for cancer therapy. Oral Diseases, 15, 8–17.
Huang, B., Lei, Z., Zhang, G. M., Li, D., Song, C., Li, B., et al. (2008). SCF-mediated mast cell infiltration and activation exacerbate the inflammation and immunosuppression in tumor microenvironment. Blood, 112, 1269–1279.
Yang, Z., Zhang, B., Li, D., Lv, M., Huang, C., Shen, G. X., et al. (2010). Mast cells mobilize myeloid-derived suppressor cells and Treg cells in tumor microenvironment via IL-17 pathway in murine hepatocarcinoma model. PLoS ONE, 5, e8922.
Maltby, S., Khazaie, K., & McNagny, K. M. (2009). Mast cells in tumor growth: angiogenesis, tissue remodelling and immune-modulation. Biochimica et Biophysica Acta, 1796, 19–26.
Kinet, J. P. (1999). The high-affinity IgE receptor (Fc epsilon RI): from physiology to pathology. Annual Review of Immunology, 17, 931–972.
Malbec, O., & Daeron, M. (2007). The mast cell IgG receptors and their roles in tissue inflammation. Immunological Reviews, 217, 206–221.
Marshall, J. S. (2004). Mast-cell responses to pathogens. Nature Reviews. Immunology, 4, 787–799.
Dawicki, W., & Marshall, J. S. (2007). New and emerging roles for mast cells in host defence. Current Opinion in Immunology, 19, 31–38.
Matsushima, H., Yamada, N., Matsue, H., & Shimada, S. (2004). TLR3-, TLR7-, and TLR9-mediated production of proinflammatory cytokines and chemokines from murine connective tissue type skin-derived mast cells but not from bone marrow-derived mast cells. Journal of Immunology, 173, 531–541.
Varadaradjalou, S., Feger, F., Thieblemont, N., Hamouda, N. B., Pleau, J. M., Dy, M., et al. (2003). Toll-like receptor 2 (TLR2) and TLR4 differentially activate human mast cells. European Journal of Immunology, 33, 899–906.
Piccinini, A. M., & Midwood, K. S. (2010). DAMPening Inflammation by Modulating TLR Signalling. Mediators of Inflammation, 2010.
Fischer, M., & Ehlers, M. (2008). Toll-like receptors in autoimmunity. Annals of the New York Academy of Sciences, 1143, 21–34.
Sims, G. P., Rowe, D. C., Rietdijk, S. T., Herbst, R., & Coyle, A. J. (2010). HMGB1 and RAGE in inflammation and cancer. Annual Review of Immunology, 28, 367–388.
Lu, W. J., Lee, N. P., Fatima, S., & Luk, J. M. (2009). Heat shock proteins in cancer: signaling pathways, tumor markers and molecular targets in liver malignancy. Protein and Peptide Letters, 16, 508–516.
Smiley, S. T., King, J. A., & Hancock, W. W. (2001). Fibrinogen stimulates macrophage chemokine secretion through toll-like receptor 4. Journal of Immunology, 167, 2887–2894.
Tesniere, A., Panaretakis, T., Kepp, O., Apetoh, L., Ghiringhelli, F., Zitvogel, L., et al. (2008). Molecular characteristics of immunogenic cancer cell death. Cell Death and Differentiation, 15, 3–12.
Caughey, G. H. (2007). Mast cell tryptases and chymases in inflammation and host defense. Immunological Reviews, 217, 141–154.
Datta, Y. H., Romano, M., Jacobson, B. C., Golan, D. E., Serhan, C. N., & Ewenstein, B. M. (1995). Peptido-leukotrienes are potent agonists of von Willebrand factor secretion and P-selectin surface expression in human umbilical vein endothelial cells. Circulation, 92, 3304–3311.
Boyce, J. A. (2007). Mast cells and eicosanoid mediators: a system of reciprocal paracrine and autocrine regulation. Immunological Reviews, 217, 168–185.
Mekori, Y. A., & Metcalfe, D. D. (1999). Mast cell-T cell interactions. The Journal of Allergy and Clinical Immunology, 104, 517–523.
Kim, B. G., Li, C., Qiao, W., Mamura, M., Kasprzak, B., Anver, M., et al. (2006). Smad4 signalling in T cells is required for suppression of gastrointestinal cancer. Nature, 441, 1015–1019.
Abraham, S. N., & St John, A. L. (2010). Mast cell-orchestrated immunity to pathogens. Nature Reviews. Immunology, 10, 440–452.
Josko, J., & Mazurek, M. (2004). Transcription factors having impact on vascular endothelial growth factor (VEGF) gene expression in angiogenesis. Medical Science Monitor, 10, RA89–RA98.
Qian, B. Z., & Pollard, J. W. (2010). Macrophage diversity enhances tumor progression and metastasis. Cell, 141, 39–51.
Zou, W. (2005). Immunosuppressive networks in the tumour environment and their therapeutic relevance. Nature Reviews. Cancer, 5, 263–274.
Gabrilovich, D. I., & Nagaraj, S. (2009). Myeloid-derived suppressor cells as regulators of the immune system. Nature Reviews. Immunology, 9, 162–174.
Kitamura, Y., & Fujita, J. (1989). Regulation of mast cell differentiation. Bioessays, 10, 193–196.
Tsuji, K., Nakahata, T., Takagi, M., Kobayashi, T., Ishiguro, A., Kikuchi, T., et al. (1990). Effects of interleukin-3 and interleukin-4 on the development of "connective tissue-type" mast cells: interleukin-3 supports their survival and interleukin-4 triggers and supports their proliferation synergistically with interleukin-3. Blood, 75, 421–427.
Zhang, W., Stoica, G., Tasca, S. I., Kelly, K. A., & Meininger, C. J. (2000). Modulation of tumor angiogenesis by stem cell factor. Cancer Research, 60, 6757–6762.
Finotto, S., Buerke, M., Lingnau, K., Schmitt, E., Galle, P. R., & Neurath, M. F. (2001). Local administration of antisense phosphorothioate oligonucleotides to the c-kit ligand, stem cell factor, suppresses airway inflammation and IL-4 production in a murine model of asthma. The Journal of Allergy and Clinical Immunology, 107, 279–286.
Hassan, H. T. (2009). c-Kit expression in human normal and malignant stem cells prognostic and therapeutic implications. Leukemia Research, 33, 5–10.
Kinet, J. P. (2007). The essential role of mast cells in orchestrating inflammation. Immunological Reviews, 217, 5–7.
Fossiez, F., Banchereau, J., Murray, R., Van, K. C., Garrone, P., & Lebecque, S. (1998). Interleukin-17. International Reviews of Immunology, 16, 541–551.
Sylvester, J., Liacini, A., Li, W. Q., & Zafarullah, M. (2004). Interleukin-17 signal transduction pathways implicated in inducing matrix metalloproteinase-3, -13 and aggrecanase-1 genes in articular chondrocytes. Cellular Signalling, 16, 469–476.
Blatner, N. R., Bonertz, A., Beckhove, P., Cheon, E. C., Krantz, S. B., Strouch, M., et al. (2010). In colorectal cancer mast cells contribute to systemic regulatory T-cell dysfunction. Proceedings of the National Academy of Sciences of the United States of America, 107, 6430–6435.
Strouch, M. J., Cheon, E. C., Salabat, M. R., Krantz, S. B., Gounaris, E., Melstrom, L. G., et al. (2010). Crosstalk between mast cells and pancreatic cancer cells contributes to pancreatic tumor progression. Clinical Cancer Research, 16, 2257–2265.
Melillo, R. M., Guarino, V., Avilla, E., Galdiero, M. R., Liotti, F., Prevete, N., et al. (2010). Mast cells have a protumorigenic role in human thyroid cancer. Oncogene, 29, 6203–6215.
Bode, A. P., Sandberg, H., Dombrose, F. A., & Lentz, B. R. (1985). Association of factor V activity with membranous vesicles released from human platelets: requirement for platelet stimulation. Thrombosis Research, 39, 49–61.
VanWijk, M. J., VanBavel, E., Sturk, A., & Nieuwland, R. (2003). Microparticles in cardiovascular diseases. Cardiovascular Research, 59, 277–287.
Ratajczak, J., Wysoczynski, M., Hayek, F., Janowska-Wieczorek, A., & Ratajczak, M. Z. (2006). Membrane-derived microvesicles: important and underappreciated mediators of cell-to-cell communication. Leukemia, 20, 1487–1495.
Gilfillan, A. M., & Tkaczyk, C. (2006). Integrated signalling pathways for mast-cell activation. Nature Reviews. Immunology, 6, 218–230.
Deregibus, M. C., Cantaluppi, V., Calogero, R., Lo, I. M., Tetta, C., Biancone, L., et al. (2007). Endothelial progenitor cell derived microvesicles activate an angiogenic program in endothelial cells by a horizontal transfer of mRNA. Blood, 110, 2440–2448.
Tang, K., Liu, J., Yang, Z. S., Zhang, B., Zhang, H. F., Huang, C. M., et al. (2010). Microparticles mediate enzyme transfer from platelets to mast cells: a new pathway for lipoxin A4 biosynthesis. Biochemical and Biophysical Research Communications, 400, 432–436.
Kondo, K., Muramatsu, M., Okamoto, Y., Jin, D., Takai, S., Tanigawa, N., et al. (2006). Expression of chymase-positive cells in gastric cancer and its correlation with the angiogenesis. Journal of Surgical Oncology, 93, 36–42.
Terada, T., & Matsunaga, Y. (2000). Increased mast cells in hepatocellular carcinoma and intrahepatic cholangiocarcinoma. Journal of Hepatology, 3, 961–966.
Pelosi, G., Barisella, M., Pasini, F., Leon, M. E., Veronesi, G., Spaggiari, L., et al. (2004). CD117 immunoreactivity in stage I adenocarcinoma and squamous cell carcinoma of the lung: relevance to prognosis in a subset of adenocarcinoma patients. Modern Pathology, 17, 711–721.
Ju, M. J., Qiu, S. J., Gao, Q., Fan, J., Cai, M. Y., Li, Y. W., et al. (2009). Combination of peritumoral mast cells and T-regulatory cells predicts prognosis of hepatocellular carcinoma. Cancer Science, 100, 1267–1274.
Xiang, M., Gu, Y., Zhao, F., Lu, H., Chen, S., & Yin, L. (2010). Mast cell tryptase promotes breast cancer migration and invasion. Oncology Reports, 23, 615–619.
Starkey, J. R., Crowle, P. K., & Taubenberger, S. (1988). Mast-cell-deficient W/Wv mice exhibit a decreased rate of tumor angiogenesis. International Journal of Cancer, 42, 48–52.
Dabbous, M. K., Haney, L., Nicolson, G. L., Eckley, D., & Woolley, D. E. (1991). Mast cell modulation of tumour cell proliferation in rat mammary adenocarcinoma 13762NF. British Journal of Cancer, 63, 873–878.
Theoharides, T. C., Rozniecki, J. J., Sahagian, G., Jocobson, S., Kempuraj, D., Conti, P., et al. (2008). Impact of stress and mast cells on brain metastases. Journal of Neuroimmunology, 205, 1–7.
Yano, H., Kinuta, M., Tateishi, H., Nakano, Y., Matsui, S., Monden, T., et al. (1999). Mast cell infiltration around gastric cancer cells correlates with tumor angiogenesis and metastasis. Gastric Cancer, 2, 26–32.
Huang, B., Lei, Z., Zhao, J., Gong, W., Liu, J., Chen, Z., et al. (2007). CCL2/CCR2 pathway mediates recruitment of myeloid suppressor cells to cancers. Cancer Letters, 252, 86–92.
Acknowledgments
The authors thank Dr. Yonghong Wan of McMaster University (Canada) and Dr. Yan Su of The University of Maryland (USA) for their helpful discussion and assistance in editing this article.
This work was supported by the National Natural Science Foundation of China (30871020), Funds for International Cooperation and Exchange of the National Natural Science Foundation of China (30911120482), the Program for New Century Excellent Talents in University (NCET-08-0219), Special Research Foundation for Universities affiliated with China Ministry of Education (Z2009005), Important National Science and Technology Specific Projects (2009ZX09301-014), Scientific Research Foundation of Wuhan City Human Resource for Returned Scholars.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Liu, J., Zhang, Y., Zhao, J. et al. Mast cell: insight into remodeling a tumor microenvironment. Cancer Metastasis Rev 30, 177–184 (2011). https://doi.org/10.1007/s10555-011-9276-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10555-011-9276-1