
Abstract
Mast cells are tissue-resident, innate immune cells that play a key role in the inflammatory response and tissue homeostasis. Mast cells accumulate in the tumor stroma of different human cancer types, and increased mast cell density has been associated to either good or poor prognosis, depending on the tumor type and stage. Mast cells play a multifaceted role in the tumor microenvironment by modulating various events of tumor biology, such as cell proliferation and survival, angiogenesis, invasiveness, and metastasis. Moreover, tumor-associated mast cells have the potential to shape the tumor microenvironment by establishing crosstalk with other tumor-infiltrating cells. This chapter reviews the current understanding of the role of mast cells in the tumor microenvironment. These cells have received much less attention than other tumor-associated immune cells but are now recognized as critical components of the tumor microenvironment and could hold promise as a potential target to improve cancer immunotherapy.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Tumor microenvironment
- Mast cells
- Tumor-associated mast cells
- Breast cancer
- Lung cancer
- Prostate cancer
- Colorectal cancer
- Gastric cancer
- Pancreatic cancer
- Anti-tumoral
- Pro-tumoral
- Histamine
- Tryptase
- Angiogenesis
- Lymphangiogenesis
9.1 Introduction
The mast cell (MC) is a tissue-resident, innate immune cell that plays a key role in the host defense and homeostatic response but also contributes to several immune-mediated disorders, such as allergic reactions, autoimmune diseases, and cancer.
Although MC accumulation at tumor sites has been reported for many years, there is still controversy about the contribution of this cell to tumor development. This chapter provides a review of the literature focusing on the MC role in the tumor microenvironment of different human solid cancers. After briefly reviewing new insights into MC biology, with a major focus on MC phenotype and function, as a direct consequence of the local microenvironment, we analyze the described mechanisms for MC recruitment into the tumor microenvironment. We also discuss evidence reporting MCs anti-tumoral role, as well as evidence supporting a pro-tumoral role, and the mechanisms implicated in each response. The goal of this chapter is to give insight into the multifaceted role played by MCs in the tumor microenvironment and puts forward some perspectives for future studies.
9.2 Biology of the Mast Cell
MCs are tissue-resident cells extensively distributed throughout the body, especially prominent in protective tissue barriers, such as the skin, airways, and gut mucosa. MCs differentiation into one of their distinct phenotypes and their functions are strongly determined by growth factors and cytokines present in the tissue microenvironment [1]. In rodents, MC subtypes are classified based on their tissue location in two major populations: connective tissue mast cells (CTMCs) , which reside constitutively in most connective tissues, and mucosal mast cells (MMCs), which reside in the intestinal and respiratory mucosa. MMCs arise from bone marrow-derived MC progenitors that are recruited and undergo maturation in a T cell-dependent manner. Unlike MMCs, CTMCs are seeded during embryogenesis, by MC “primitive” progenitors (derived from yolk sac) and progenitors derived from “definitive” fetal hematopoietic stem cells, and their maintenance in adult tissues occurs independently of bone marrow progenitors [2, 3]. Their human counterparts are classified based on the proteases they contain, tryptase alone (MCT), chymase alone (MCC), or both (MCTC). These subsets differ in their tissue localization and function [4]. The origin of human MCs and the factors that influence each subtype are yet to be completely understood. It is worth noting that both human and rodent MCs are highly heterogeneous and moldable, and intraspecies as well as interspecies heterogeneity has been reported [5]. MC phenotype and function are profoundly shaped by the microenvironment where they originate, mature, and reside. Indeed, MCs are endowed with a high degree of site-specific plasticity, and tissue-specific MCs display differences in granule content, cytokine expression patterns, and receptors, which provide context-related functions to these cells [4]. Even within the same tissue and under basal conditions, MC populations are phenotypically different and can generate further specific subpopulations [6, 7]. MCs also display specific activation-associated transcriptional signatures, for example, interleukin (IL)-33 activated MCs are transcriptionally and most likely functionally distinct than MCs activated via cross-linking of the high-affinity receptor for IgE (FcεRI) [8]. Therefore, the traditional classification based on the produced proteases is too simplistic and a further classification, that takes into consideration the variety of tissue-specific MC subtypes, has been proposed [4]. Supporting this idea, recent studies identified that CTMCs from distinct anatomical locations or with a different fetal origin, had considerable heterogeneity in gene profiles revealing different CTMC subsets [2, 3, 9]. Also, these studies found evidence for previously unappreciated CTMC turnover, in the absence of tissue inflammation and with tissue-specific kinetics [2, 9]. The existence of distinct CTMC subsets confirms that MC identity and function are strongly influenced by their developmental origin and microenvironment.
MCs are characterized by a cytoplasm packed with secretory granules, filled with a broad array of immunomodulatory and vasoactive mediators such as histamine, heparin, cytokines such as tumor necrosis factor-alpha (TNF-α), and different proteases. Indeed, half of the content in secretory granules of mature MCs consists of proteases, tryptase being the predominant protease in human MC [10].
MCs are notable for their extraordinary ability to respond rapidly to stimuli (Fig. 9.1). Upon activation and depending on the type of stimuli and receptor involved, MCs can release three distinct classes of bioactive molecules: granule-stored preformed mediators that are released within seconds to minutes (degranulation); de novo-synthesized lipid mediators, prostaglandins, and leukotrienes, produced within minutes; and a variety of cytokines, chemokines, and growth and angiogenic factors that are produced, following their transcription and translation, within hours [11]. MC activation is mediated by a variety of receptors expressed on their surface, the most well-known pathway of activation is mediated by the cross-linkage of their high-affinity IgE receptor (FcεRI), but MC activation can also be triggered by other receptors, such as Toll-like receptors (TLRs), complement receptors, adenosine receptor, and cytokine and chemokine receptors [5]. The nature of the MC response is dependent on the stimulating ligand.

Mast cells (MCs) express several receptors on their surface, which give them the ability to recognize a wide range of endogenous/exogenous ligands. Upon activation by diverse mechanisms, MCs can release a broad array of biologically active mediators that can be divided into two major categories: preformed mediators, stored within the MC granules and released immediately after activation (a process called degranulation) and de novo synthesized mediators, produced following activation. These mediators are directly or indirectly involved in several physiological and pathophysiological processes
MCs are multifunctional cells implicated in several physiologic and disease responses. They contribute to tissue homeostasis by promoting inflammation, angiogenesis, and wound healing [12]. They also accumulate in injured and inflamed tissue, where they can amplify or suppress inflammation. MCs also play a key role in the host defense, acting as sentinels, sensing their environment via multiple cell surface receptors to orchestrate the immune response through the fine-tuned release of their biologically active mediators [11]. MC-derived mediators can influence migration, maturation, and function of different cell types, including dendritic cells (DCs), macrophages, eosinophils, natural killer cells (NK), T cells, B cells, fibroblasts, endothelial, and epithelial cells [13]. For example, MC-derived TNF-α is required for efficient DCs and cytotoxic T cells responses, since it promotes DC maturation and migration, and boost the T-cell-priming efficiency [14]. This mediator is also a critical factor for neutrophil recruitment. Similarly, MC-derived prostaglandins and leukotrienes act mainly as proinflammatory factors [15], whereas histamine has pleiotropic effects dependent upon the receptor subtype it is bound to. Therefore, histamine not only enhances the proliferation and activation of different immune and nonimmune cells but also inhibits cell proliferation and stimulates immune cell suppressor activity. One of the most important modulatory effects of histamine is its influence on T lymphocyte function and differentiation. Specifically, through its H1 receptor, histamine influences T-cell development into Th1 and leads to a decrease of T cell suppressor activity, but through its H2 receptor, histamine stimulates T lymphocyte suppressor activity and inhibits cytolytic activity [15]. It is worth to note that the effector functions of MCs could be different depending on the tissue in which the response occurs, and then the same MC-derived mediator can induce different effects.
Under physiological conditions, MCs can induce and enhance angiogenesis through the production of a variety of pro-angiogenic factors, such as vascular endothelial growth factor (VEGF), fibroblast growth factor 2 (FGF2), tryptase, and other proteases [16]. These molecules also contribute to cancer progression. Indeed, one of the main MC effects on tumor growth is related to their pro-angiogenic function.
9.3 Tumor-Associated Mast Cells (TAMCs)
Increased understanding of the relationship between cancer cells and their microenvironment has shed light on how tumors evolve as complex systems, involving dynamic interactions between tumor cells and different cell types, including infiltrating immune cells. The interaction of tumor cells with the immune cells in their microenvironment is essential for determining the tumor fate [17].
MC infiltration is commonly found in different human cancer types, and their accumulation, either at the peri-tumoral or intra-tumoral level, has been associated with both promotion and suppression of tumor growth [16].
TAMCs may arise in tumor microenvironment either by recruitment of neighboring tissue-resident MCs and/or MC progenitors (MCP) via healthy vasculature close to the tumor site or by the proliferation of both mature tissue-resident MCs and MCPs. MCs could be recruited by various inflammatory stimuli within the tumor microenvironment, including hypoxia, cellular injury, and tissue ischemia. MCs could also be recruited by soluble factors secreted from the tumor cells and noncancerous stromal cells. So far, the precise molecular mechanisms involved in the MC accumulation in tumors remain poorly studied.
In healthy tissue, stem cell factor (SCF) is the most characterized chemotactic factor for MC recruitment. Similarly, MC infiltration in tumors is mainly mediated by tumor-derived SCF and its receptor c-kit in MC [18,19,20]. Experiments using cancer cells from clear cell renal cell carcinoma (ccRCC), the most common histological subtype of renal cell carcinoma (RCC), identified SCF as a key mediator of MC recruitment. Additionally, assays using 3D coculture models showed that hypoxia inducible factor (HIF-2α) expression in these cancer cells was responsible for inducing SCF secretion and subsequently MC recruitment [20]. In vitro evidence showed that colon cancer cells recruited MCs by releasing SCF, and this effect was mediated via bidirectional crosstalk [21]. This study also demonstrated that MC recruitment, rather than local proliferation, was the determinant factor for the increased mast cell density (MCD) observed in colorectal cancer (CRC). Besides SCF, other growth factors produced by noncancerous stromal cells, such as FGF-2, VEGF, and platelet-derived endothelial cell growth factor (PD-ECGF) mediated MC recruitment both in vivo and in vitro [22, 23].
Recently, chemokines were described as important factors for MC recruitment to the tumor microenvironment. For instance, experiments using cell culture supernatants from gastric cancer (GC) tissues, demonstrated the importance of CXCL12 and its receptor CXCR4 in MC recruitment [24]. These experiments indicated that the CXCL12-CXCR4 chemotactic axis could be one of the mechanisms for MC recruitment to the tumor microenvironment, in gastric cancer in vivo, since high MC infiltration correlated with high CXCL12 levels in tumor tissues. Moreover, TAMCs were preferably located intratumorally, and their numbers increased with tumor progression, showing a positive correlation between MCD and increased advanced lymphatic invasion, tumor size, and tumor stage, in tissues from patients with this disease [24, 25]. Another study reported that CCL15, a chemokine constitutively secreted by colon cancer cells, was as an important chemotactic factor for MCs in vitro, eventually promoting MCs migration [21].
9.4 Mast Cells’ Functions in the Tumor Microenvironment
It is clear that mast cells infiltrate tumors of different types of cancer, but what is the role of tumor-associated mast cells?
Although MCs have been long recognized as early and persistent tumor-infiltrating cells, they remain less studied than other components of the tumor microenvironment [26]. Undeniably, MCs can influence directly or indirectly the tumor biology and fate, but their functions in the tumor microenvironment are complex and still poorly understood.
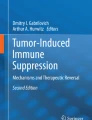
MCs are a rich source of diverse biologically active mediators (cytokines, chemokines, growth factors, matrix metalloproteinases, and proteases), with pro-inflammatory, immunoregulatory, and angiogenic properties. Similar to its physiological functions, MCs can exert diverse functions during cancer development and progression (Fig. 9.2). Depending largely on the microenvironmental stimuli, MCs can inhibit or promote several processes of tumor biology, such as proliferation and survival, angiogenesis, lymphangiogenesis, tissue remodeling, disruption of the extracellular matrix, invasion, and metastatic spread [16]. Therefore, TAMCs could be either pro-tumorigenic, anti-tumorigenic, or innocent bystander cells.

Multifaceted effects of mast cells in the tumor microenvironment. Mast cells (MCs) accumulate in the tumor microenvironment either by the proliferation of local tissue-resident MCs or via recruitment of neighboring tissue-resident MCs and/or MC progenitors, by tumor-derived factors such as SCF, CXCL12, and CCL15. MCs could also be recruited and activated by various inflammatory stimuli within the tumor microenvironment. Activated MCs can exert antitumor effects through direct tumor cell lysis, or indirectly through the release of mediators that promote recruitment and maturation of immune effector cells in the tumor microenvironment. MCs can also contribute to the antitumor microenvironment by decreasing tumor angiogenesis through the inhibition of vascular permeability via MC production of prostaglandin D2 (PGD2). On the other side, activated MCs can also exert pro-tumor effects. In particular, MC-derived histamine can enhance tumor cell proliferation through binding to its H4 receptor. Tumor derived-adrenomedullin (ADM) stimulates MCs to produce IL-17, which in turn suppresses cancer cell apoptosis contributing to cancer growth. Besides, MCs contribute to angiogenesis in the tumor microenvironment by secreting several angiogenesis-promoting factors. Tryptase, a MC-specific protease, enhances angiogenesis directly by stimulating endothelial cell proliferation and vascular tube formation, or indirectly by activating matrix-metalloproteases (MMPs) and plasminogen activator (PA), which in turn degrade extracellular-matrix components to provide space for neovascular growth. MC-derived factors are also potent promoters of lymphangiogenesis. Moreover, MCs also contribute to the development of tumor-favoring microenvironment by suppressing T-lymphocytes function, via MC secretion of IL-10 and TGF-β or by recruitment of myeloid-derived suppressor cells (MDSC) via secretion of CCL-2 and leukotriene B4 (LTB4). Tumor-derived TNF-α upregulates PD-L1 expression in the MC, which represents a mechanism of immune suppression via direct interaction between MCs and T lymphocytes in a PDL1-dependent manner. MCs can also exacerbate the immunosuppressive tumor microenvironment by establishing crosstalk with MDSC through CD40:CD40L axis. IMCs immature myeloid cells, MEC microvascular endothelial cells, PD-L1 programmed death-ligand 1
In this chapter, we discuss the role of MCs as a potential prognostic marker in cancer, as well as some anti- and pro-tumor mechanisms by which MCs potentially modulate the tumor microenvironment.
9.4.1 Anti-Tumoral Role of Mast Cells
9.4.1.1 Tumor-Associated Mast Cells as a Good Prognostic Marker
The prognostic value of TAMCs in human solid tumors is still unclear and controversial. Some clinical studies have considered TAMCs as indicators of better prognosis in certain human cancers, such as breast, prostate, and lung cancer (Table 9.1). In this context, MC infiltration in breast cancer has been considered a favorable prognostic factor, and in some cases, this good prognosis was independent of age, tumor grade, and molecular cancer subtype [27,28,29,30,31,32]. Similarly, in nonsmall-cell lung cancer (NSCLC) , high MC infiltration was considered an indicator of good prognosis, independently of tumor stage [33, 34]. In another study, high MCD was linked to a better prognosis in stage I NSCLC but not in stage II [35]. Interestingly, in prostate cancer, an experimental study in mice found that TAMCs exerted different functions according to tumor stage and that MC inactivation promoted the occurrence of highly malignant neuroendocrine cancers [36]. Clinical studies in humans have shown that in prostate cancer, the prognostic role of TAMCs depends not only on the tumor stage but also on the MC location within tumor tissue. So far, the results obtained indicate that intra-tumoral and peri-tumoral MCs have opposing effects on prostate cancer outcome. Therefore, high intra-tumoral but not peri-tumoral MC numbers were associated with a favorable prognosis [37,38,39,40].
Few studies have investigated the role of specific MC subtypes in cancer. From this perspective, a recent study found that both MCT and MCTC phenotypes were associated with less aggressive breast cancer and that increased numbers of any of the MC subtypes correlated with a better prognosis [32]. This is consistent with another study reporting that both MCT and MCTC phenotypes correlated with improved survival in NSCLC [34]. In colon cancer, only one study has associated high MCD to longer overall survival in patients [41]. Together, these data indicate that MCs may contribute to the anti-tumor response in these cancer types; however, more high-quality clinical studies and standardization of methods are needed before MCD can be considered a biomarker of prognosis for routine use in clinical practice.
9.4.1.2 Mast Cells’ Potential to Exert Anti-tumor Effects
Little has been studied about the mechanisms implicated in the anti-tumor activity of MCs (Fig. 9.2). Through microscopic analysis of breast cancer tissues, one study reported that peri-tumoral MCs showed cytolytic activity against tumor cells [29]. Another study, using a mouse model of lung carcinoma, demonstrated that MCs decreased angiogenesis and vascular permeability in the tumor microenvironment, through the production of prostaglandin D2 (PGD2) . Additionally, this study showed that MC-derived PGD2 reduced TNF-α synthesis, and then limited the pro-tumor response in the tumor microenvironment [42]. This work identified MC-derived PGD2 as an anti-angiogenic factor in lung carcinoma. Besides, analysis in an experimental model of chemical skin carcinogenesis, in MC-deficient KitW/KitW-v mice, demonstrated that the absence of MCs led to an increased tumor incidence and growth. This observation was associated with reduced infiltration of Gr-1+ granulocytes, F4/80+ macrophages, B220+ B cells, and CD8+ T cells in sites of skin carcinogenesis. The authors suggested that MCs contributed to the anti-tumor response indirectly by promoting the recruitment of immune cells and immunosurveillance in the tumor microenvironment. This finding was supported by demonstrating that local adoptive transfer of MCs restored cell infiltration, leading to an active immune response that did not allow tumor establishment [43]. The potential of MCs to stimulate the anti-tumor immune response was also demonstrated using a model of murine melanoma. TLR2-activated MCs were able to inhibit tumor growth in vivo, by recruitment of NK and T cells to tumor sites and reduction of angiogenesis. MC-derived IL-6 but not TNF-α was required for tumor growth inhibition after TLR2-mediated MC activation [44]. Comparably to the effect observed in melanoma, TLR2-activated MCs also inhibited the growth of lung cancer in vivo, and this effect was also associated with mononuclear cell infiltration and decreased angiogenesis. In vitro experiments also showed that tumor cell proliferation decreased in the presence of TLR2-activated MCs supernatants, indicating direct MCs anti-tumor effects. Furthermore, in vitro chemotaxis experiments using CCL3−/− murine-derived MCs demonstrated a clear role for CCL3 in mediating MC-dependent recruitment of immune effector cells [44]. Similarly, another study using a model of murine melanoma demonstrated that TLR7-activated dermal MCs secreted CCL2, resulting in skin inflammation and recruitment of plasmacytoid DCs to tumor sites, which after transformation into a subset of killer DCs directly eliminated tumor cells [45]. Overall, these studies indicated that TLR-mediated activation could harness MCs to exert tumor inhibitory functions, such as the recruitment of immune effector cells to tumor sites and the boost of cancer immunosurveillance.
9.4.2 Pro-tumoral Role of Mast Cells
9.4.2.1 Tumor-Associated Mast Cells as a Poor Prognostic Marker
Several scientific studies support MCs pro-tumoral function and association of TAMCs with a poor clinical prognosis of various solid tumors (Table 9.1). Mostly in colon [46,47,48,49,50,51,52], gastric [53,54,55,56], and pancreatic cancer [57,58,59,60], a growing number of clinical studies have associated high TAMC numbers with tumor progression and worse prognosis in patients. A similar association, though controversial, have been reported for breast [26, 61,62,63,64,65], lung [35, 66, 67], and prostate cancer [38, 68].
The mechanisms that potentially mediate MCs pro-tumoral functions include stimulation of tumor cells growth, induction of an immunosuppressive tumor microenvironment, promotion of angiogenesis and lymphangiogenesis, and facilitation of invasion and metastasis (Fig. 9.2).
9.4.2.2 Mast Cells as Promoters of Tumor Cell Proliferation and Survival
MCs can induce proliferation of tumor cells either by direct cell–cell contact or through the release of mediators that directly or indirectly stimulate proliferation and survival. Studies using MC-deficient mice demonstrated that MCs were an essential hematopoietic component for the development and growth of preneoplastic polyps [69]. Moreover, MC-secreted mediators promoted tumor growth by stimulation of colon cancer cell proliferation, through bidirectional communication between MCs and cancer cells, without the need of cell–cell contact [21]. A recent study showed that adrenomedullin, an acid peptide amide in supernatants from cancerous gastric tissue, stimulated MC production of IL-17A, which in turn promoted proliferation by suppressing apoptosis in GC cells, contributing to cancer growth and progression [25]. These data were supported by histopathological results showing that increased numbers of intra-tumoral MCs correlated with tumor progression and poor survival in GC patients [25]. An in vitro study showed that MCs, in coculture with lung cancer cells, released high levels of histamine, β-hexosaminidase, and tryptase. Interestingly, histamine was the only MC-derived mediator capable of inducing cancer cell proliferation through its H4 receptor [70]. Although some studies have demonstrated that tryptase can induce proteinase-activated receptor 2 (PAR-2)-mediated proliferation of some types of cancer cells, here it was demonstrated that this protease did not directly affect lung cancer cell proliferation.
9.4.2.3 Mast Cells’ Contribution to Tumor Angiogenesis and Lymphangiogenesis
MCs can be potent inductors of angiogenesis because of their ability to synthesize and release several common angiogenic components, such as FGF, IL-8, transforming growth factor (TGF-β), TNF-α, and VEGF, as well as noncommon angiogenic components, such as tryptase. Currently, a great amount of evidence has shown that mast cell density (MCD) is strongly correlated to angiogenesis in different human cancers, and among the proangiogenic factors released by MCs tryptase, it is one of the most powerful [23]. A relationship between microvascular density (MVD) and MCD has been shown in various human tumors. A recent paper showed a positive correlation between the MCD and MVD in oral squamous cell carcinoma (OSCC) [71]. Also, in gastric cancer, MCD correlates with angiogenesis, growth, and cancer progression [54]. In patients with breast cancer, high levels of tryptase in serum correlated with high TAMCs numbers and strongly with MVD, supporting the involvement of MC-derived tryptase in tumor angiogenesis [61]. Moreover, experimental data using MC-deficient mice have also provided strong evidence for a positive correlation between the MCD in mammary tumors and angiogenesis. Histological examination of tumors in MC-deficient mice that spontaneously develop breast cancer revealed a marked decrease in angiogenesis compared to control mice, thus supporting the fact that MCs contribution to angiogenesis was strongly due to their ability to promote tumor vascularization [72].
Recent evidence showed a positive relationship between TAMCs and lymphatic vessels (LV), suggesting that MCs may also contribute to the formation of LV in the tumor microenvironment [63, 73]. Analysis of the association between TAMCs and lymphangiogenesis in different molecular subtypes of breast cancer, showed a significant correlation between a high number of peri-tumoral MCs and newly formed LV, in the luminal A-type and the basal-like subtypes [73]. Interestingly, the basal-like subtype exhibited a particular behavior concerning TAMCs and LV density (LVD). This subtype was the only one that showed a significant correlation between the overall MCD (peri-tumoral and intra-tumoral MC count) and LVD. These findings indicated that TAMCs response was specific for each molecular subtype of breast cancer, and this could influence lymphovascular invasion dependent on each molecular tumor subtype [73].
Although MC association with cancer angiogenesis and lymphangiogenesis has been widely demonstrated, the specific mechanisms and factors implicated are only partially characterized, and the MC role in these events seems to be tumor type-dependent.
9.4.2.4 Mast Cells as Promoters of Invasion and Metastasis
In addition to releasing their specific proteases tryptase and chymase, MCs can release different matrix metalloproteases, which degrade components of the extracellular matrix (ECM), and have a key role in cancer progression [16]. Some studies have demonstrated the potential role of MCs in favoring cancer invasion and metastasis. In a cohort of patients with breast cancer, MCs were detected in all metastatic lymph nodes, but not in reactive lymph nodes, which indicated a specific MC role in nodal metastasis of breast cancer [63]. Another study showed that increased tryptase expression, in tumor tissues of breast cancer, was associated with a higher tumor grade and greater lymph node metastasis [74]. Supporting this, in vitro assays showed that tryptase promoted the invasion and migration of the breast cancer cell line MDA-MB-231, along with activation of matrix metalloproteinase-2, which could facilitate vascular invasion and accelerate metastatic spread [74]. Recently, a meta-analysis of cohort studies evaluating the prognostic role of MC, in different human solid tumors, found that increased tryptase + MC infiltration was significantly associated with lymph node metastasis in NSCLC, hepatocellular, and colorectal cancer [75].
9.4.2.5 Mast Cells Contribute to an Immunosuppressive Tumor Microenvironment
MCs can contribute to the generation of a tumor-favoring microenvironment by disrupting the anti-tumor immunity (Fig. 9.2). A recent study found that intra-tumoral MCs, in samples from patients with gastric cancer, expressed a significantly higher level of immunosuppressive molecule PD-L1. Since crosstalk between PD-L1 and PD-1 is one of the main mechanisms leading to immunosuppression of T cells, this result suggested that MCs may play a role to directly modulate effector function in the tumor microenvironment [24]. This study also demonstrated that TNF-α produced by tumor cell cultures significantly upregulated PD-L1 expression in MCs by activating the nuclear factor-κB (NF-κB) signaling pathway. Through experimental evidence, the authors showed that TAMC inhibited the normal T-cell function in a PD-L1-dependent manner. The results also indicated a significant negative correlation between MC numbers and CD8+ T cells. Additionally, the percentage of MC was significantly increased in patients with advanced stages of GC, suggesting that MC contributes to tumor growth and GC progression via PD-L1 [24]. Besides, in colorectal cancer, CD8+ T-cell infiltration was negatively correlated with MC infiltration. Likewise, Th1-type chemokines CXCL9 and CXCL10, which recruit and promote cytotoxicity of T and natural killer (NK) cells, were highly upregulated in low MCD tumors, suggesting that tumors with less MCs infiltration had a more intense immune response, which could explain the better prognosis in such patients. Importantly, the authors showed that patients with a lower MCD had better survival rates after receiving adjuvant chemotherapy [52]. Using gene set enrichment analysis, it was reported that tumor-infiltrating MC in ccRCC promoted an immunosuppressive environment through suppression of CD8+ T-cell function, via secretion of IL-10 and TGF-β. Furthermore, the expression of characteristic genes of the adaptive immune system and cytotoxic functions [interferon-γ (IFN-γ) and granzyme B (GZMB)] were markedly downregulated in tumors with a high MCD [20].
MCs also contribute to immune suppression through the recruitment of myeloid-derived suppressor cells (MDSCs) and boost their suppressor activity (Fig. 9.2). In a murine model of hepatocarcinoma, activated MCs modified the tumor microenvironment by upregulating CCL2, and the Th2 cytokines IL-10 and IL-13. Moreover, MCs induced IL-17 expression in MDSCs, which in turn regulated the infiltration and enhanced the suppressive function of Treg cells in the tumor microenvironment [76]. In a mouse model of colon cancer, MCs were required to enhance MDSC-mediated immune suppression, through a mechanism involving IFN-γ and nitric oxide production. In the same study, in vitro migration assays showed that activated MCs induced the migration of MDSCs, partly through MC-derived leukotrienes [77]. Also, crosstalk between MCs and MDSCs through the CD40:CD40L axis was responsible for shaping the MC-derived proinflammatory microenvironment (CCL2, IL-6, and TNF-α), that could further support MDSC activation, resulting in a tumor-promoting microenvironment [77]. The fact that MDSCs selectively increased the production of proinflammatory mediators by MCs when cocultured, highlighted the existence of a bidirectional modulation between these two cell populations in the tumor microenvironment.
9.4.2.6 Mast Cells’ Role in Cancer Therapeutic Resistance
In addition to the pro-tumoral functions described above, MCs may also modulate the response of cancer cells to therapy. In vitro assays demonstrated that MC culture supernatants blocked gemcitabine (GEM)/nabpaclitaxel (NAB)-induced apoptosis in pancreatic cancer cell lines, through the activation of TGF-β1 signaling. Furthermore, these MC-derived supernatants reduced the anti-invasive activity of GEM/NAB. These data showed a functional interplay between MCs and pancreatic cancer cells, which induced resistance to GEM/NAB. This observation was supported by the finding that unresponsiveness to GEM/NAB correlated with increased levels of tryptase and TGF-β1 in the blood of pancreatic ductal adenocarcinoma patients. Thus, MCs seem to play a crucial role in tumor resistance to GEM/NAB [60]. Analysis of tumor tissue of inflammatory breast cancer (IBC), an aggressive form of breast cancer characterized by the clinical appearance of inflammation, showed that the MCD was significantly associated with poor response to neoadjuvant chemotherapy in all disease stages and molecular subtypes of IBC. Moreover, MCs were located within range for direct or paracrine interactions with CD8+ T cells, as well as CD163+ macrophages and tumor cells. The authors suggested that interaction of MCs with these immune cells might be exerting an inhibitory effect in IBC, through suppressing CD8+ T cells, enhancing immunosuppressive CD163+ macrophages, and directly promoting tumor cell growth [65]. This study indicated that MCs could represent a possible therapeutic target to enhance the response to chemotherapy.
9.5 Concluding Remarks
Despite recent advances in understanding the mast cell role in tumor biology, we still have limited knowledge of the molecular mechanisms driving mast cells functions in the tumor microenvironment. Most studies agree that mast cells are tumor-infiltrating cells of different human cancers; however, conflicting data exist about the role played by these cells. Also, in specific cancer types, there is a discrepancy in the correlation between the mast cell density and cancer prognosis.
The role of mast cells in the tumor microenvironment might be more complex than suggested by the studies reviewed here, and mast cells functions could rely heavily on the poorly described role of tumor microenvironment in shaping the mast cell response.
Similar to other cell constituents of the tumor microenvironment, such as macrophages, mast cells are extremely moldable and can change their phenotype and functions in response to a changing microenvironment. While tumor-associated macrophages (TAMs) have been extensively studied, and distinct specialized TAMs subpopulations have been well described [78], mast cells have received much less attention, and mast cell diversity and function in distinct tumor microenvironments have not been described up to now. Elucidation of how mast cell plasticity impacts on mechanisms orchestrating a pro-tumor or anti-tumor milieu could explain the contradictory findings regarding the mast cell function in the tumor microenvironment.
In general, cancer is a highly heterogeneous disease with a great variety of genetic and histological clinical subtypes, with each subtype also exhibiting a high heterogeneity within itself. The landscape is made even more complex by the intrinsic mast cell heterogeneity and plasticity, making it possible that within each cancer subtype a variety of tumor associated-mast cell subpopulations exists. Consequently, mast cell contribution, either positive or negative, could be specific to certain cancer subtypes or tumor microenvironments, which could dictate context-dependent functions to the mast cell.
The interaction of mast cells with other tumor-associated stromal cell types, in addition to immune cells, such as fibroblasts, pericytes, endothelial cells, and adipocytes, should be investigated. These stromal cells are key components of the tumor microenvironment, which support tumor growth. Specifically, endothelial cells and pericytes participate in tumor angiogenesis [79]. Therefore, crosstalk between these stromal cells and mast cells may occur within the tumor microenvironment.
More work is needed to understand the intricate crosstalk between mast cells and the tumor microenvironment. Uncovering the mechanisms orchestrating this reciprocal communication will allow mast cell inclusion in future therapeutic approaches.
References
Moon TC, St Laurent CD, Morris KE, Marcet C, Yoshimura T, Sekar Y, Befus AD (2010) Advances in mast cell biology: new understanding of heterogeneity and function. Mucosal Immunol 3(2):111–128. https://doi.org/10.1038/mi.2009.136
Gentek R, Ghigo C, Hoeffel G, Bulle MJ, Msallam R, Gautier G, Launay P, Chen J, Ginhoux F, Bajenoff M (2018) Hemogenic endothelial fate mapping reveals dual developmental origin of mast cells. Immunity 48(6):1160–1171. e1165. https://doi.org/10.1016/j.immuni.2018.04.025
Li Z, Liu S, Xu J, Zhang X, Han D, Liu J, Xia M, Yi L, Shen Q, Xu S, Lu L, Cao X (2018) Adult connective tissue-resident mast cells originate from late erythro-myeloid progenitors. Immunity 49(4):640–653. e645. https://doi.org/10.1016/j.immuni.2018.09.023
Frossi B, Mion F, Sibilano R, Danelli L, Pucillo CEM (2018) Is it time for a new classification of mast cells? What do we know about mast cell heterogeneity? Immunol Rev 282(1):35–46. https://doi.org/10.1111/imr.12636
Huber M, Cato ACB, Ainooson GK, Freichel M, Tsvilovskyy V, Jessberger R, Riedlinger E, Sommerhoff CP, Bischoff SC (2019) Regulation of the pleiotropic effects of tissue-resident mast cells. J Allergy Clin Immunol. https://doi.org/10.1016/j.jaci.2019.02.004
Cildir G, Pant H, Lopez AF, Tergaonkar V (2017) The transcriptional program, functional heterogeneity, and clinical targeting of mast cells. J Exp Med 214(9):2491–2506. https://doi.org/10.1084/jem.20170910
Espinosa E, Valitutti S (2018) New roles and controls of mast cells. Curr Opin Immunol 50:39–47. https://doi.org/10.1016/j.coi.2017.10.012
Chhiba KD, Hsu CL, Berdnikovs S, Bryce PJ (2017) Transcriptional heterogeneity of mast cells and basophils upon activation. J Immunol 198(12):4868–4878. https://doi.org/10.4049/jimmunol.1601825
Dwyer DF, Barrett NA, Austen KF, Immunological Genome Project C (2016) Expression profiling of constitutive mast cells reveals a unique identity within the immune system. Nat Immunol 17(7):878–887. https://doi.org/10.1038/ni.3445
Meyer N, Zenclussen AC (2018) Mast cells-good guys with a bad image? Am J Reprod Immunol 80(4):e13002. https://doi.org/10.1111/aji.13002
Abraham SN, St John AL (2010) Mast cell-orchestrated immunity to pathogens. Nat Rev Immunol 10(6):440–452. https://doi.org/10.1038/nri2782
Dudeck A, Koberle M, Goldmann O, Meyer N, Dudeck J, Lemmens S, Rohde M, Roldan NG, Dietze-Schwonberg K, Orinska Z, Medina E, Hendrix S, Metz M, Zenclussen AC, von Stebut E, Biedermann T (2018) Mast cells as protectors of health. J Allergy Clin Immunol. https://doi.org/10.1016/j.jaci.2018.10.054
Krystel-Whittemore M, Dileepan KN, Wood JG (2015) Mast cell: a multi-functional master cell. Front Immunol 6:620. https://doi.org/10.3389/fimmu.2015.00620
Dudeck J, Ghouse SM, Lehmann CH, Hoppe A, Schubert N, Nedospasov SA, Dudziak D, Dudeck A (2015) Mast-cell-derived TNF amplifies CD8(+) dendritic cell functionality and CD8(+) T cell priming. Cell Rep 13(2):399–411. https://doi.org/10.1016/j.celrep.2015.08.078
Branco A, Yoshikawa FSY, Pietrobon AJ, Sato MN (2018) Role of histamine in modulating the immune response and inflammation. Mediat Inflamm 2018:9524075. https://doi.org/10.1155/2018/9524075
Varricchi G, Galdiero MR, Loffredo S, Marone G, Iannone R, Marone G, Granata F (2017) Are mast cells MASTers in cancer? Front Immunol 8:424. https://doi.org/10.3389/fimmu.2017.00424
Turley SJ, Cremasco V, Astarita JL (2015) Immunological hallmarks of stromal cells in the tumour microenvironment. Nat Rev Immunol 15(11):669–682. https://doi.org/10.1038/nri3902
Khazaie K, Blatner NR, Khan MW, Gounari F, Gounaris E, Dennis K, Bonertz A, Tsai FN, Strouch MJ, Cheon E, Phillips JD, Beckhove P, Bentrem DJ (2011) The significant role of mast cells in cancer. Cancer Metastasis Rev 30(1):45–60. https://doi.org/10.1007/s10555-011-9286-z
Huang B, Lei Z, Zhang GM, Li D, Song C, Li B, Liu Y, Yuan Y, Unkeless J, Xiong H, Feng ZH (2008) SCF-mediated mast cell infiltration and activation exacerbate the inflammation and immunosuppression in tumor microenvironment. Blood 112(4):1269–1279. https://doi.org/10.1182/blood-2008-03-147033
Xiong Y, Liu L, Xia Y, Qi Y, Chen Y, Chen L, Zhang P, Kong Y, Qu Y, Wang Z, Lin Z, Chen X, Xiang Z, Wang J, Bai Q, Zhang W, Yang Y, Guo J, Xu J (2019) Tumor infiltrating mast cells determine oncogenic HIF-2alpha-conferred immune evasion in clear cell renal cell carcinoma. Cancer Immunol Immunother 68(5):731–741. https://doi.org/10.1007/s00262-019-02314-y
Yu Y, Blokhuis B, Derks Y, Kumari S, Garssen J, Redegeld F (2018) Human mast cells promote colon cancer growth via bidirectional crosstalk: studies in 2D and 3D coculture models. Onco Targets Ther 7(11):e1504729. https://doi.org/10.1080/2162402X.2018.1504729
Ronca R, Tamma R, Coltrini D, Ruggieri S, Presta M, Ribatti D (2017) Fibroblast growth factor modulates mast cell recruitment in a murine model of prostate cancer. Oncotarget 8(47):82583–82592. https://doi.org/10.18632/oncotarget.19773
Ribatti D, Crivellato E (2012) Mast cells, angiogenesis, and tumour growth. Biochim Biophys Acta 1822(1):2–8. https://doi.org/10.1016/j.bbadis.2010.11.010
Lv Y, Zhao Y, Wang X, Chen N, Mao F, Teng Y, Wang T, Peng L, Zhang J, Cheng P, Liu Y, Kong H, Chen W, Hao C, Han B, Ma Q, Zou Q, Chen J, Zhuang Y (2019) Increased intratumoral mast cells foster immune suppression and gastric cancer progression through TNF-alpha-PD-L1 pathway. J Immunother Cancer 7(1):54. https://doi.org/10.1186/s40425-019-0530-3
Lv YP, Peng LS, Wang QH, Chen N, Teng YS, Wang TT, Mao FY, Zhang JY, Cheng P, Liu YG, Kong H, Wu XL, Hao CJ, Chen W, Zhu J, Han B, Ma Q, Li K, Zou Q, Zhuang Y (2018) Degranulation of mast cells induced by gastric cancer-derived adrenomedullin prompts gastric cancer progression. Cell Death Dis 9(10):1034. https://doi.org/10.1038/s41419-018-1100-1
Aponte-Lopez A, Fuentes-Panana EM, Cortes-Munoz D, Munoz-Cruz S (2018) Mast cell, the neglected member of the tumor microenvironment: role in breast cancer. J Immunol Res 2018:2584243. https://doi.org/10.1155/2018/2584243
Dabiri S, Huntsman D, Makretsov N, Cheang M, Gilks B, Bajdik C, Gelmon K, Chia S, Hayes M (2004) The presence of stromal mast cells identifies a subset of invasive breast cancers with a favorable prognosis. Mod Pathol 17(6):690–695. https://doi.org/10.1038/modpathol.3800094
Amini RM, Aaltonen K, Nevanlinna H, Carvalho R, Salonen L, Heikkila P, Blomqvist C (2007) Mast cells and eosinophils in invasive breast carcinoma. BMC Cancer 7:165. https://doi.org/10.1186/1471-2407-7-165
della Rovere F, Granata A, Familiari D, D’Arrigo G, Mondello B, Basile G (2007) Mast cells in invasive ductal breast cancer: different behavior in high and minimum hormone-receptive cancers. Anticancer Res 27(4B):2465–2471
Rajput AB, Turbin DA, Cheang MC, Voduc DK, Leung S, Gelmon KA, Gilks CB, Huntsman DG (2008) Stromal mast cells in invasive breast cancer are a marker of favourable prognosis: a study of 4,444 cases. Breast Cancer Res Treat 107(2):249–257. https://doi.org/10.1007/s10549-007-9546-3
Sang J, Yi D, Tang X, Zhang Y, Huang T (2016) The associations between mast cell infiltration, clinical features and molecular types of invasive breast cancer. Oncotarget 7(49):81661–81669. https://doi.org/10.18632/oncotarget.13163
Glajcar A, Szpor J, Pacek A, Tyrak KE, Chan F, Streb J, Hodorowicz-Zaniewska D, Okon K (2017) The relationship between breast cancer molecular subtypes and mast cell populations in tumor microenvironment. Virchows Arch 470(5):505–515. https://doi.org/10.1007/s00428-017-2103-5
Welsh TJ, Green RH, Richardson D, Waller DA, O’Byrne KJ, Bradding P (2005) Macrophage and mast-cell invasion of tumor cell islets confers a marked survival advantage in non-small-cell lung cancer. J Clin Oncol 23(35):8959–8967. https://doi.org/10.1200/JCO.2005.01.4910
Shikotra A, Ohri CM, Green RH, Waller DA, Bradding P (2016) Mast cell phenotype, TNFalpha expression and degranulation status in non-small cell lung cancer. Sci Rep 6:38352. https://doi.org/10.1038/srep38352
Carlini MJ, Dalurzo MC, Lastiri JM, Smith DE, Vasallo BC, Puricelli LI, Lauria de Cidre LS (2010) Mast cell phenotypes and microvessels in non-small cell lung cancer and its prognostic significance. Hum Pathol 41(5):697–705. https://doi.org/10.1016/j.humpath.2009.04.029
Pittoni P, Tripodo C, Piconese S, Mauri G, Parenza M, Rigoni A, Sangaletti S, Colombo MP (2011) Mast cell targeting hampers prostate adenocarcinoma development but promotes the occurrence of highly malignant neuroendocrine cancers. Cancer Res 71(18):5987–5997. https://doi.org/10.1158/0008-5472.CAN-11-1637
Fleischmann A, Schlomm T, Kollermann J, Sekulic N, Huland H, Mirlacher M, Sauter G, Simon R, Erbersdobler A (2009) Immunological microenvironment in prostate cancer: high mast cell densities are associated with favorable tumor characteristics and good prognosis. Prostate 69(9):976–981. https://doi.org/10.1002/pros.20948
Johansson A, Rudolfsson S, Hammarsten P, Halin S, Pietras K, Jones J, Stattin P, Egevad L, Granfors T, Wikstrom P, Bergh A (2010) Mast cells are novel independent prognostic markers in prostate cancer and represent a target for therapy. Am J Pathol 177(2):1031–1041. https://doi.org/10.2353/ajpath.2010.100070
Hempel HA, Cuka NS, Kulac I, Barber JR, Cornish TC, Platz EA, De Marzo AM, Sfanos KS (2017) Low intratumoral mast cells are associated with a higher risk of prostate cancer recurrence. Prostate 77(4):412–424. https://doi.org/10.1002/pros.23280
Zhao SG, Lehrer J, Chang SL, Das R, Erho N, Liu Y, Sjostrom M, Den RB, Freedland SJ, Klein EA, Karnes RJ, Schaeffer EM, Xu M, Speers C, Nguyen PL, Ross AE, Chan JM, Cooperberg MR, Carroll PR, Davicioni E, Fong L, Spratt DE, Feng FY (2019) The immune landscape of prostate cancer and nomination of PD-L2 as a potential therapeutic target. J Natl Cancer Inst 111(3):301–310. https://doi.org/10.1093/jnci/djy141
Mehdawi L, Osman J, Topi G, Sjolander A (2016) High tumor mast cell density is associated with longer survival of colon cancer patients. Acta Oncol 55(12):1434–1442. https://doi.org/10.1080/0284186X.2016.1198493
Murata T, Aritake K, Matsumoto S, Kamauchi S, Nakagawa T, Hori M, Momotani E, Urade Y, Ozaki H (2011) Prostagladin D2 is a mast cell-derived antiangiogenic factor in lung carcinoma. Proc Natl Acad Sci U S A 108(49):19802–19807. https://doi.org/10.1073/pnas.1110011108
Siebenhaar F, Metz M, Maurer M (2014) Mast cells protect from skin tumor development and limit tumor growth during cutaneous de novo carcinogenesis in a Kit-dependent mouse model. Exp Dermatol 23(3):159–164. https://doi.org/10.1111/exd.12328
Oldford SA, Haidl ID, Howatt MA, Leiva CA, Johnston B, Marshall JS (2010) A critical role for mast cells and mast cell-derived IL-6 in TLR2-mediated inhibition of tumor growth. J Immunol 185(11):7067–7076. https://doi.org/10.4049/jimmunol.1001137
Drobits B, Holcmann M, Amberg N, Swiecki M, Grundtner R, Hammer M, Colonna M, Sibilia M (2012) Imiquimod clears tumors in mice independent of adaptive immunity by converting pDCs into tumor-killing effector cells. J Clin Invest 122(2):575–585. https://doi.org/10.1172/JCI61034
Gulubova M, Vlaykova T (2009) Prognostic significance of mast cell number and microvascular density for the survival of patients with primary colorectal cancer. J Gastroenterol Hepatol 24(7):1265–1275. https://doi.org/10.1111/j.1440-1746.2007.05009.x
Elezoglu B, Tolunay S (2012) The relationship between the stromal mast cell number, microvessel density, c-erbB-2 staining and survival and prognostic factors in colorectal carcinoma. Turk Patoloji Derg 28(2):110–118. https://doi.org/10.5146/tjpath.2012.01109
Wu X, Zou Y, He X, Yuan R, Chen Y, Lan N, Lian L, Wang F, Fan X, Zeng Y, Ke J, Wu X, Lan P (2013) Tumor-infiltrating mast cells in colorectal cancer as a poor prognostic factor. Int J Surg Pathol 21(2):111–120. https://doi.org/10.1177/1066896912448836
Ammendola M, Sacco R, Sammarco G, Donato G, Montemurro S, Ruggieri E, Patruno R, Marech I, Cariello M, Vacca A, Gadaleta CD, Ranieri G (2014) Correlation between serum tryptase, mast cells positive to tryptase and microvascular density in colo-rectal cancer patients: possible biological-clinical significance. PLoS One 9(6):e99512. https://doi.org/10.1371/journal.pone.0099512
Suzuki S, Ichikawa Y, Nakagawa K, Kumamoto T, Mori R, Matsuyama R, Takeda K, Ota M, Tanaka K, Tamura T, Endo I (2015) High infiltration of mast cells positive to tryptase predicts worse outcome following resection of colorectal liver metastases. BMC Cancer 15:840. https://doi.org/10.1186/s12885-015-1863-z
Chen Y, Yuan R, Wu X, He X, Zeng Y, Fan X, Wang L, Wang J, Lan P, Wu X (2016) A novel immune marker model predicts oncological outcomes of patients with colorectal cancer. Ann Surg Oncol 23(3):826–832. https://doi.org/10.1245/s10434-015-4889-1
Mao Y, Feng Q, Zheng P, Yang L, Zhu D, Chang W, Ji M, He G, Xu J (2018) Low tumor infiltrating mast cell density confers prognostic benefit and reflects immunoactivation in colorectal cancer. Int J Cancer 143(9):2271–2280. https://doi.org/10.1002/ijc.31613
Ammendola M, Marech I, Sammarco G, Zuccala V, Luposella M, Zizzo N, Patruno R, Crovace A, Ruggieri E, Zito AF, Gadaleta CD, Sacco R, Ranieri G (2015) Infiltrating mast cells correlate with angiogenesis in bone metastases from gastric cancer patients. Int J Mol Sci 16(2):3237–3250. https://doi.org/10.3390/ijms16023237
Micu GV, Staniceanu F, Sticlaru LC, Popp CG, Bastian AE, Gramada E, Pop G, Mateescu RB, Rimbas M, Archip B, Bleotu C (2016) Correlations between the density of tryptase positive mast cells (DMCT) and that of new blood vessels (CD105+) in patients with gastric cancer. Rom J Intern Med 54(2):113–120. https://doi.org/10.1515/rjim-2016-0016
Ribatti D, Guidolin D, Marzullo A, Nico B, Annese T, Benagiano V, Crivellato E (2010) Mast cells and angiogenesis in gastric carcinoma. Int J Exp Pathol 91(4):350–356. https://doi.org/10.1111/j.1365-2613.2010.00714.x
Ammendola M, Sacco R, Zuccala V, Luposella M, Patruno R, Gadaleta P, Zizzo N, Gadaleta CD, De Sarro G, Sammarco G, Oltean M, Ranieri G (2016) Mast cells density positive to tryptase correlate with microvascular density in both primary gastric cancer tissue and loco-regional lymph node metastases from patients that have undergone radical surgery. Int J Mol Sci 17(11). https://doi.org/10.3390/ijms17111905
Strouch MJ, Cheon EC, Salabat MR, Krantz SB, Gounaris E, Melstrom LG, Dangi-Garimella S, Wang E, Munshi HG, Khazaie K, Bentrem DJ (2010) Crosstalk between mast cells and pancreatic cancer cells contributes to pancreatic tumor progression. Clin Cancer Res 16(8):2257–2265. https://doi.org/10.1158/1078-0432.CCR-09-1230
Chang DZ, Ma Y, Ji B, Wang H, Deng D, Liu Y, Abbruzzese JL, Liu YJ, Logsdon CD, Hwu P (2011) Mast cells in tumor microenvironment promotes the in vivo growth of pancreatic ductal adenocarcinoma. Clin Cancer Res 17(22):7015–7023. https://doi.org/10.1158/1078-0432.CCR-11-0607
Cai SW, Yang SZ, Gao J, Pan K, Chen JY, Wang YL, Wei LX, Dong JH (2011) Prognostic significance of mast cell count following curative resection for pancreatic ductal adenocarcinoma. Surgery 149(4):576–584. https://doi.org/10.1016/j.surg.2010.10.009
Porcelli L, Iacobazzi RM, Di Fonte R, Serrati S, Intini A, Solimando AG, Brunetti O, Calabrese A, Leonetti F, Azzariti A, Silvestris N (2019) CAFs and TGF-beta signaling activation by mast cells contribute to resistance to gemcitabine/nabpaclitaxel in pancreatic cancer. Cancers (Basel) 11(3). https://doi.org/10.3390/cancers11030330
Marech I, Ammendola M, Sacco R, Capriuolo GS, Patruno R, Rubini R, Luposella M, Zuccala V, Savino E, Gadaleta CD, Ribatti D, Ranieri G (2014) Serum tryptase, mast cells positive to tryptase and microvascular density evaluation in early breast cancer patients: possible translational significance. BMC Cancer 14:534. https://doi.org/10.1186/1471-2407-14-534
Fakhrjou A, Naghavi-Behzad M, Montazeri V, Karkon-Shayan F, Norouzi-Panahi L, Piri R (2016) The relationship between histologic grades of invasive carcinoma of breast ducts and mast cell infiltration. South Asian J Cancer 5(1):5–7. https://doi.org/10.4103/2278-330X.179699
Keser SH, Kandemir NO, Ece D, Gecmen GG, Gul AE, Barisik NO, Sensu S, Buyukuysal C, Barut F (2017) Relationship of mast cell density with lymphangiogenesis and prognostic parameters in breast carcinoma. Kaohsiung J Med Sci 33(4):171–180. https://doi.org/10.1016/j.kjms.2017.01.005
Carpenco E, Ceausu RA, Cimpean AM, Gaje PN, Saptefrati L, Fulga V, David V, Raica M (2019) Mast cells as an indicator and prognostic marker in molecular subtypes of breast cancer. In Vivo 33(3):743–748. https://doi.org/10.21873/invivo.11534
Reddy SM, Reuben A, Barua S, Jiang H, Zhang S, Wang L, Gopalakrishnan V, Hudgens CW, Tetzlaff MT, Reuben JM, Tsujikawa T, Coussens LM, Wani K, He Y, Villareal L, Wood A, Rao A, Woodward WA, Ueno NT, Krishnamurthy S, Wargo JA, Mittendorf EA (2019) Poor response to neoadjuvant chemotherapy correlates with mast cell infiltration in inflammatory breast cancer. Cancer Immunol Res 7(6):1025–1035. https://doi.org/10.1158/2326-6066.CIR-18-0619
Imada A, Shijubo N, Kojima H, Abe S (2000) Mast cells correlate with angiogenesis and poor outcome in stage I lung adenocarcinoma. Eur Respir J 15(6):1087–1093. https://doi.org/10.1034/j.1399-3003.2000.01517.x
Takanami I, Takeuchi K, Naruke M (2000) Mast cell density is associated with angiogenesis and poor prognosis in pulmonary adenocarcinoma. Cancer 88(12):2686–2692
Nonomura N, Takayama H, Nishimura K, Oka D, Nakai Y, Shiba M, Tsujimura A, Nakayama M, Aozasa K, Okuyama A (2007) Decreased number of mast cells infiltrating into needle biopsy specimens leads to a better prognosis of prostate cancer. Br J Cancer 97(7):952–956. https://doi.org/10.1038/sj.bjc.6603962
Gounaris E, Erdman SE, Restaino C, Gurish MF, Friend DS, Gounari F, Lee DM, Zhang G, Glickman JN, Shin K, Rao VP, Poutahidis T, Weissleder R, McNagny KM, Khazaie K (2007) Mast cells are an essential hematopoietic component for polyp development. Proc Natl Acad Sci U S A 104(50):19977–19982. https://doi.org/10.1073/pnas.0704620104
Stoyanov E, Uddin M, Mankuta D, Dubinett SM, Levi-Schaffer F (2012) Mast cells and histamine enhance the proliferation of non-small cell lung cancer cells. Lung Cancer 75(1):38–44. https://doi.org/10.1016/j.lungcan.2011.05.029
Kabiraj A, Jaiswal R, Singh A, Gupta J, Singh A, Samadi FM (2018) Immunohistochemical evaluation of tumor angiogenesis and the role of mast cells in oral squamous cell carcinoma. J Cancer Res Ther 14(3):495–502. https://doi.org/10.4103/0973-1482.163693
He L, Zhu Z, Chen S, Wang Y, Gu H (2016) Mammary tumor growth and metastasis are reduced in c-Kit mutant Sash mice. Cancer Med 5(6):1292–1297. https://doi.org/10.1002/cam4.696
Raica M, Cimpean AM, Ceausu R, Ribatti D, Gaje P (2013) Interplay between mast cells and lymphatic vessels in different molecular types of breast cancer. Anticancer Res 33(3):957–963
Xiang M, Gu Y, Zhao F, Lu H, Chen S, Yin L (2010) Mast cell tryptase promotes breast cancer migration and invasion. Oncol Rep 23(3):615–619. https://doi.org/10.3892/or_00000676
Hu G, Wang S, Cheng P (2018) Tumor-infiltrating tryptase(+) mast cells predict unfavorable clinical outcome in solid tumors. Int J Cancer 142(4):813–821. https://doi.org/10.1002/ijc.31099
Yang Z, Zhang B, Li D, Lv M, Huang C, Shen GX, Huang B (2010) Mast cells mobilize myeloid-derived suppressor cells and Treg cells in tumor microenvironment via IL-17 pathway in murine hepatocarcinoma model. PLoS One 5(1):e8922. https://doi.org/10.1371/journal.pone.0008922
Danelli L, Frossi B, Gri G, Mion F, Guarnotta C, Bongiovanni L, Tripodo C, Mariuzzi L, Marzinotto S, Rigoni A, Blank U, Colombo MP, Pucillo CE (2015) Mast cells boost myeloid-derived suppressor cell activity and contribute to the development of tumor-favoring microenvironment. Cancer Immunol Res 3(1):85–95. https://doi.org/10.1158/2326-6066.CIR-14-0102
Bolli E, Movahedi K, Laoui D, Van Ginderachter JA (2017) Novel insights in the regulation and function of macrophages in the tumor microenvironment. Curr Opin Oncol 29(1):55–61. https://doi.org/10.1097/CCO.0000000000000344
Birbrair A, Zhang T, Wang ZM, Messi ML, Olson JD, Mintz A, Delbono O (2014) Type-2 pericytes participate in normal and tumoral angiogenesis. Am J Physiol Cell Physiol 307(1):C25–C38. https://doi.org/10.1152/ajpcell.00084.2014
Lin C, Liu H, Zhang H, Cao Y, Li R, Wu S, Li H, He H, Xu J, Sun Y (2017) Tryptase expression as a prognostic marker in patients with resected gastric cancer. Br J Surg 104(8):1037–1044. https://doi.org/10.1002/bjs.10546
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 The Editor(s) (if applicable) and The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Aponte-López, A., Muñoz-Cruz, S. (2020). Mast Cells in the Tumor Microenvironment. In: Birbrair, A. (eds) Tumor Microenvironment. Advances in Experimental Medicine and Biology, vol 1273. Springer, Cham. https://doi.org/10.1007/978-3-030-49270-0_9
Download citation
DOI: https://doi.org/10.1007/978-3-030-49270-0_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-49269-4
Online ISBN: 978-3-030-49270-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)