
Abstract
Purpose
Radiotherapy (RT) after breast-conserving surgery for early-stage breast cancer patients has similar survival benefits with whole breast RT (WBRT) or accelerated partial breast irradiation (APBI). However, the impact of RT type and side-effects severity on change in quality of life (QOL) is unknown. We examined changes in RT side-effects severity and QOL by RT type.
Methods
We analyzed data from a cohort of 285 newly diagnosed early-stage breast cancer patients with tumor size ≤3.0 cm and lymph node-negative disease. Patients (93 [32.6%] stage 0; 49 [17.2%] non-white; mean age = 59.3 years) completed four interviews (6 weeks, 6, 12, and 24 months) after definitive surgical treatment. We measured severity of RT side effects, fatigue and skin irritation, using a 5-point scale (1 “not at all” to 5 “all the time”) and measured QOL using the Functional Assessment of Cancer Therapy-Breast (FACT-B) and RAND 36-item Health Survey Vitality subscale. Repeated-measures analysis of covariance of each outcome controlled for demographic, clinical/treatment, and psychosocial factors.
Results
Patients initiated RT by 6 months (113 received APBI; 172 received WBRT) and completed RT by 12 months. Patients receiving WBRT (vs. APBI) reported greater increase in fatigue and skin irritation severity from 6-week to 6-month interviews (each P < 0.001). Improvement in neither total FACT-B nor Vitality differed significantly by RT type over 2-year follow-up.
Conclusions
Findings suggest that early-stage breast cancer patients can benefit from less-severe, short-term side effects of APBI with no differential impact on QOL change within 2-year follow-up.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Standard of care for early-stage breast cancer is breast-conserving surgery (BCS) plus radiation (RT) for women under age 70 and, for those over age 70, BCS with or without RT [1,2,3,4]. Recent studies demonstrate that accelerated partial breast irradiation (APBI) provides, in shorter time, similar rates of local control and similar breast cancer-specific and overall survival outcomes as treatment with whole breast radiation therapy (WBRT) in early-stage breast cancer patients [5,6,7,8,9,10]. However, a number of systematic reviews reported a lack of evidence about short-term RT side effects and their impact on changes in quality of life (QOL) [11,12,13,14]. One review of randomized clinical trials comparing PBI/APBI and conventional or hypo-fractionated WBRT found that no studies reported on the relative effects of PBI/APBI and WBRT on QOL [15].
Although RT may negatively impact patients’ QOL [16, 17], favorable QOL outcomes have been reported in breast cancer patients receiving ABPI [18,19,20], but these studies did not directly compare QOL to patients who received WBRT. Other studies directly comparing fatigue [21], skin toxicity [22], and cosmetic outcomes [5, 23] in breast cancer patients treated with either WBRT or ABPI did not measure QOL as an outcome of interest. Several other studies explored QOL outcomes in breast cancer patients who received RT with either APBI or WBRT [24,25,26,27,28,29,30,31,32]. However, these studies were limited by small patient samples [25, 28,29,30,31], using a cross-sectional design [28, 29, 32], using stratified analyses without directly comparing QOL by RT type [25,26,27], or did not examine the impact of RT side effects on change in QOL [24]. Using data from an early-stage breast cancer cohort study, we examined changes in QOL by type of RT (WBRT or APBI), controlling for the severity RT-related side effects as well as demographic, clinical, treatment, and psychosocial correlates of QOL.
Methods
Participants
Between October 2003 and June 2007, early-stage breast cancer patients treated at the Siteman Cancer Center at Barnes-Jewish Hospital and Washington University School of Medicine and at Saint Louis University School of Medicine were prospectively recruited for a cohort study evaluating QOL changes and similarities/differences in aspects of QOL in 549 women with and 547 same-aged women without a breast cancer history [33,34,35]. Eligibility criteria included English fluency, age 40 and older (based on screening mammography recommendations [36, 37]), no prior breast-cancer history, no receipt of neoadjuvant chemotherapy, and no evidence of cognitive impairment on the Orientation-Memory-Concentration Test [38] administered to all women 65 years of age or older. Participants were recruited 2-3 weeks after a first primary stage 0-IIA breast-cancer diagnosis determined by surgical pathology (patients) or after a negative/benign screening mammogram (controls). This study was approved by the Institutional Review Board at each university.
Specially trained interviewers obtained informed consent from all study participants and conducted computer-assisted telephone interviews 6 weeks (Time1), 6 months (Time2), 1 year (Time3), and 2 years (Time4) following definitive surgical treatment (patients) or screening mammogram (controls), with routine follow-up quality-assurance checks for randomly selected 10% of participants. By interview, we administered newly developed and previously validated measures of QOL, and other variables hypothesized to be associated with QOL in breast cancer patients.
Measures
We conducted a secondary analysis of data from this cohort study, analyzing data for patients who reported receiving RT at either Time1 or Time2, as self-reported RT is a reliable alternative to the medical record [39,40,41,42]. Patients were included if they received BCS and met clinical criteria to receive either APBI or WBRT, including a diagnosis of node-negative disease and a primary tumor size ≤3.0 cm by surgical pathology [43, 44].
We collected patient demographics and measured QOL at each interview using the FACT-B [45] and the Vitality subscale of the RAND 36-Item Health Survey 1.0 [46]. The FACT-B is a multidimensional measure of QOL that asks patients to indicate how true each item was for them “during the past 7 days” using a 5-point scale (“not at all” to “very much”). Total scores range from 0 to 144 with higher scores reflecting better QOL. The RAND Vitality subscale measures patient’s energy and fatigue with four items asking how they felt “during the past 4 weeks” using a 5-point scale (“none of the time” to “all the time”); standardized scores range from 0 to 100 with higher scores reflecting more Vitality.
To measure severity of two common RT side effects, fatigue and skin irritation [47,48,49,50], we asked patients who reported receipt of RT at Time1 and/or Time2 to indicate how much they were bothered by these side effects in the last month: “You have (or had) burns/dried skin/itchy skin from radiation,” and “You are (or were) very tired after radiation.” Patients responded to each item using a 5-point scale from “not at all” (1) to “all the time” (5); higher scores indicate greater severity of each RT side effect.
As potential covariates of RT side-effects severity and QOL, we used validated measures of patients’ perceived availability of social support (19-item Medical Outcomes Study Social Support Survey [51]), comorbidity [52] (using the Charlson Comorbidity Index scoring algorithm [53]), and state anxiety (21-item Beck Anxiety Inventory ® [54]). Higher scores indicate greater availability of social support, comorbidity, and state anxiety. History of depression at Time1 was measured by an affirmative response to either, “Has a doctor ever told you that you had depression?” or “Have you ever been treated for depression with medication or psychotherapy?” We used a previously validated, 8-item questionnaire [34, 35] to measure severity of surgical side effects; higher mean scores indicate more severe surgical side effects.
Patients’ clinical data, including cancer stage (ductal carcinoma in situ [55], stage I/IIA), tumor size, lymph node positivity, estrogen receptor status (positive/negative), and type of definitive surgical treatment (BCS, mastectomy), were determined by surgical pathology. Receipt of RT (yes/no), type of RT received (APBI, WBRT), receipt of chemotherapy (yes/no), and endocrine therapy (yes/no) were obtained by interview and the medical record.
Data analysis
Using analysis of variance (ANOVA) and Pearson product-moment correlations, we identified covariates of each RT side-effects-severity measure (i.e., fatigue and skin irritation) and of each QOL measure (i.e., total FACT-B and RAND Vitality subscale). Chi square tests examined associations among categorical variables. Cohen’s kappa [56] measured agreement between medical record data and patients’ self-reported receipt of RT, chemotherapy, and endocrine therapy (yes, no) and type of RT (APBI, WBRT). Analysis of covariance (ANCOVA) tested differences in RT side-effects severity by RT type, controlling for covariates significantly associated with RT side-effects severity and/or QOL at Time1. We analyzed changes in each of fatigue and skin irritation severity from Time1 to Time2 in those patients who reported receiving RT at both time points as well as changes in each QOL measure (i.e., total FACT-B and RAND Vitality subscale) from Time1-Time4 using repeated-measures ANCOVAs (RM-ANCOVAs) grouping by RT type and adjusting for RT side-effects severity and other covariates. All analyses were performed using IBM SPSS Statistics version 23.0 (IBM Corp., Armonk, NY).
Results
Of 772 patients invited to participate in the larger cohort study, 549 (71%) enrolled and completed the first interview between October 2003 and July 2007. Participants and non-participants did not differ significantly by pathologic cancer stage (P = 0.837), surgery type (BCS vs. mastectomy; P = 0.095), or marital status (married vs. non-married; P = 0.072). However, compared with non-participants, participants were younger (mean [SD], 58.3 [10.6] vs. 60.6 [12.6] years; P = 0.011) and were more likely to be White (79.2 vs. 63.8%; P < 0.001).
Of the 549 patients, we excluded 212 patients who would not have been eligible to receive APBI, including 193 patients who received a mastectomy, and 19 patients who received BCS who had a primary tumor size >3.0 cm or had positive nodes. We also excluded 22 patients who reported they did not receive RT, 12 patients who did not report the type of RT received, 8 patients who dropped out of the study after Time1, and 10 patients who initiated RT between Time2 and Time3, and therefore could not have answered the two RT side-effects-severity items asked during the first two interviews. Patient characteristics by RT type for the 285 patients in the study sample are shown in Table 1. Retention was high, with 275 patients (96%) in this sample completing all four interviews.
Telephone interviews were completed a mean 6.5 weeks (Time1) and 6.2 (Time2), 12.3 (Time3), and 24.5 (Time4) months following definitive surgical treatment. Since we collected more complete treatment data by interview than by medical record review, we examined agreement between the medical record and patient-reported treatment data. At Time1, 121 patients (43%) reported at least initiating RT; at Time2, all 285 patients reported at least initiating RT (Table 1), which was confirmed for all patients by medical record review. For the 258 patients whose type of RT was found in the medical record, we observed near-perfect agreement (kappa = 0.81–1.00) [56] between the medical record and patient-reported type of RT (kappa = 0.98). Of the 110 patients confirmed to have received APBI per the medical record, 94 patients received brachytherapy (34 [36.2%] interstitial, 37 [39.4%] intracavitary, and 23 [24.5%] not otherwise specified [NOS]), 12 patients received a regional dose of 3600 cGy, two received a regional dose of 3400 cGy, and two were treated with “external beam NOS.” We observed near-perfect agreement between the medical record and patient-reported receipt of chemotherapy (kappa = 0.97) and endocrine therapy (kappa = 0.94), as we observed for RT.
Of 25 patients who had initiated chemotherapy at Time1, only one patient also had initiated RT at Time1. By Time2, 53 patients had initiated chemotherapy, and the proportions of patients who received APBI and WBRT did not differ significantly (20/113 [17.7%] vs. 33/172 [19.2%], respectively; P = 0.752). All patients had completed chemotherapy and RT by Time3.
Of 53 patients who had initiated endocrine therapy at Time1, 35 patients also had initiated RT. At Time2, 169 patients had initiated endocrine therapy, and the proportions who received APBI and WBRT did not differ significantly (69/113 [61.1%] vs. 100/172 [58.1%], respectively, P = 0.848). Similarly, the proportions of patients receiving endocrine therapy at Time3 (n = 198) and Time4 (n = 184) also did not differ significantly by RT type (results not shown).
Patients who received WBRT reported significantly greater severity of fatigue (P = 0.001) and skin irritation (P < 0.001) than patients who received APBI at Time2 only (Table 2). Younger age, greater severity of surgical side effects, greater state anxiety, and worse QOL on the FACT-B were significantly correlated with greater severity of both fatigue and skin irritation side effects at Time2 (Table 3; each P < 0.05).
Patients who received WBRT reported worse QOL on the total FACT-B measure than patients who received APBI at Time1 only (Table 4), but we did not observe any QOL differences by RT type in Vitality (Table 5). In the RM-ANCOVA models testing change in RT side-effects severity and QOL by RT type, all variables significantly associated with RT side-effects severity and/or QOL shown in Tables 2, 3, 4 and 5 (age, education, employment status, marital status, social support, surgical side effects, state anxiety, history of depression, BMI) were included as covariates. We also included as covariates receipt of chemotherapy at Time2 and a binary variable for receipt of endocrine therapy at any interview (yes/no), as all patients included had at least initiated RT and chemotherapy by Time2 and the number of patients reporting use of endocrine therapy varied over the course of the study (Tables 4, 5 footnote). We included severity of RT-related fatigue and skin irritation side effects at Time2 as covariates in the models testing change in QOL by RT type, as these variables were associated with worse QOL at Time2 (Table 3). To avoid overfitting the data, we did not adjust for cancer stage, which was associated with both RT type (Table 1) and receipt of chemotherapy (P < 0.001), nor did we adjust for income, which was associated with patients’ education and employment status (each P < 0.001) and reported by fewer participants (8.4% did not respond). We did not adjust for comorbidity as patients reported few comorbid conditions and comorbidity was positively associated with age and BMI (Table 3).
In separate RM-ANCOVA models for change in RT side-effects severity among women who responded to these items at both Time1 and Time2 (Figs. 1, 2), women who received WBRT reported increasingly more severe RT-related fatigue and skin irritation compared with women who received APBI (each P < 0.001). Side-effects severity at Time2 was significantly higher for patients who received WBRT compared with APBI for both fatigue (P = 0.007) and skin irritation (P < 0.001).

Repeated-measures analysis of covariance of severity of fatigue at Time1 and Time2 by type of radiation therapy (RT)—whole breast radiation therapy (WBRT) or accelerated partial breast irradiation (APBI)—for those 120 patients who had initiated RT at Time1, adjusting for all covariates. Higher scores indicate greater severity of fatigue. Women who received WBRT reported a greater increase in fatigue at Time2 than women who received APBI (P < 0.001)

Repeated-measures analysis of covariance of severity of skin irritation at Time1 and Time2 by type of radiation therapy (RT)—whole breast radiation therapy (WBRT) or accelerated partial breast irradiation (APBI)—for those 120 patients who had initiated RT at Time1, adjusting for all covariates. Higher scores indicate greater severity of skin irritation. Women who received WBRT reported a greater increase in skin irritation at Time2 (P < 0.001) than women who received APBI
In the RM-ANCOVA models for change in QOL controlling for severity of RT-related fatigue and skin irritation side effects and all other covariates, we did not observe a significant improvement in either the RAND Vitality subscale (Fig. 3) or total FACT-B score (Fig. 4) over 2-year follow-up across all patients. The change in these QOL measures also did not differ significantly by RT type (i.e., the time-by-RT type interaction was not significant).

Repeated-measures analysis of covariance of RAND 36-item health survey vitality subscale scores over time by type of radiation therapy (RT)—whole breast radiation therapy (WBRT) or accelerated partial breast irradiation (APBI)—adjusting for all covariates (N = 268). Higher scores indicate greater vitality. Change over time was not statistically significant regardless of type of RT

Repeated-measures analysis of covariance of total FACT-B scores over time by type of radiation therapy (RT)—whole breast radiation therapy (WBRT) or accelerated partial breast irradiation (APBI)—adjusting for all covariates (N = 267). Higher scores indicate better quality of life. Change over time was not statistically significant regardless of type of RT
Discussion
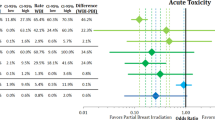
This cohort study of early-stage breast cancer patients with similar tumor size (≤3.0 cm) and node-negative disease [44] contributes to the limited knowledge about changes in QOL and RT side-effects severity over time by type of RT received. We observed that patients treated with APBI reported less severe RT-related side effects (both fatigue and skin irritation) than patients treated with WBRT at the 6-month interview following definitive surgical treatment. Eligible patients may elect to receive APBI over WBRT because of the convenience and targeted nature of APBI [57] or the inherent advantage of APBI to complete treatment quickly. Some studies have reported that breast cancer patients who received APBI report satisfaction with treatment [58] and good cosmetic outcomes [5, 22, 59], while other studies reported unacceptable cosmetic outcomes following APBI [60, 61]. In a systematic review of published and unpublished trials, PBI/APBI was associated with lower likelihood of acute, but not late, skin toxicity compared with WBRT, although cosmetic outcome and local recurrence-free survival appeared to be worse with PBI/APBI in the studies reviewed [15].
Radiation-related fatigue [47, 62] and skin irritation [48] are commonly reported RT side effects [50]. The frequency of reporting these side effects increases throughout treatment [47, 48], and fatigue in patients who received RT is reported to worsen over time compared with patients who did not receive RT [16]. Studies comparing women receiving tamoxifen with or without WBRT following BCS have reported similar QOL outcomes (physical functioning, general health, pain, and breast symptoms) at 12-month follow-up [63], and few adverse events of RT-related fatigue and skin erythema were reported at 5-year follow-up [64]. However, greater breast symptoms have been reported by older patients treated (vs. not treated) with RT at 5-year follow-up [65]. We found that patients treated with WBRT reported more severe fatigue and skin irritation than patients treated with APBI at 6-month follow-up, and among those patients who had initiated RT by the first interview, patients treated with WBRT reported a greater increase in the severity of fatigue and skin irritation at 6-month follow-up than patients treated with APBI (Figs. 1, 2). Patients in our sample who received WBRT might have had worse prognosis, as they were more likely to have received chemotherapy at Time1 and less likely to have had estrogen receptor-positive tumors, which also may offer better prognosis in some subsets of patients [66, 67]. Interestingly, using Surveillance Epidemiology and End Results program data, Liu et al. [68] found that patients with estrogen receptor-positive tumors were more likely to receive brachytherapy compared with WBRT.
We did not observe a significant improvement in QOL across all patients in this subsample over time nor did we observe that improvement in QOL differed by type of RT in either the Vitality or FACT-B models over the 2-year follow-up (Figs. 3, 4). Our findings expand upon the few studies that examined QOL outcomes after RT [24,25,26,27,28,29,30,31,32], each of which had notable limitations, e.g., having small samples [25, 28,29,30,31], a cross-sectional design [28, 29, 32], not directly comparing QOL outcomes by RT type [25,26,27], or not examining the impact of RT side-effects severity on change in QOL [24]. To the best of our knowledge, no previous studies have reported change in the severity of RT-related side effects in relation to both APBI and WBRT, and none have examined, as we have done here, changes in QOL over time by type of RT, adjusting for the severity of RT-related side effects as well as demographic, clinical, treatment, and psychosocial factors. The National Surgical Adjuvant Breast and Bowel Project (NSABP) B-39/Radiation Therapy Oncology Group (RTOG) 0413 Phase III randomized trial [69] is comparing survival and QOL outcomes in stage 0–II breast cancer patients treated with conventional WBRT versus partial breast RT. The results of this large, multicenter trial will be able to compare the impact of APBI and WBRT on RT-related side effects as well as on QOL and fill in some notable gaps in knowledge to help inform treatment decision-making.
At 6-month follow-up, we observed less severe RT-related fatigue and skin irritation side effects with APBI compared with WBRT, which may be expected given the abbreviated course of treatment and more focused RT exposure using APBI. However, since breast cancer patients treated with RT report persistent fatigue years after completing treatment [49, 70] and cancer-related fatigue is associated with worse QOL in long-term breast cancer survivors [70], future research is warranted to determine if less severe RT-related side effects in the short term are associated with improved long-term QOL in breast cancer survivors. Jeffe et al. reported that the adverse effect of chemotherapy on total FACT-B scores was more prominent in early-stage breast cancer patients who received BCS than mastectomy, suggesting that this finding was potentially due to the cumulative effects of RT following BCS [71]. Findings reported here suggest further that the negative cumulative effect of RT on change in both Vitality and the FACT-B total scores over two-year follow-up occurs regardless of type of RT received after definitive surgical treatment. As APBI was associated with less severe RT-related side effects than WBRT in the short term within six months of surgery, and more severe RT-related side effects were associated with poorer QOL outcomes (Table 3), these findings may be especially important for early-stage breast cancer patients who also may require adjuvant chemotherapy following BCS, as RT options associated with less severe side effects (at least in the short term) may be preferred.
This study has some strengths and limitations. While we benefited from a relatively large, prospective cohort of early-stage breast cancer patients meeting much of the criteria set forth by the American Society for Radiation Oncology (ASTRO) for “suitable” and “cautionary” patient groups considered for treatment with APBI [44], we did not conduct a randomized controlled trial, which could have eliminated potential sources of bias resulting from unmeasured confounders and limited our ability to make causal inferences. Such a trial, the large, multi-site NSABP B-39/RTOG 0413 study [69], began recruiting in 2005, 2 years after we began recruiting for our cohort study and their results comparing the effects of WBRT and APBI on QOL have not yet been reported [69]. We could not account for the timing of initiation or duration of RT or the type of APBI received, which could have had an impact on RT side-effects severity and QOL changes over time, as this information was not available for all patients in the medical record. We could not confirm self-reported RT type for 27 patients or type of APBI reported by three patients, although near-perfect agreement was observed between the medical record and self-reported RT type by 258 patients. Additionally, our cohort study was not powered based on the aims of the secondary analysis reported here. An appropriately designed study specifically to examine the type, timing, and duration of RT on QOL outcomes is still needed. We also did not know whether all patients who met the ASTRO criteria for “suitable” and “cautionary” use of APBI [44] had been offered a choice between WBRT and APBI and, if they were offered a choice, which patients elected to receive WBRT over APBI. Although hypofractionated WBRT is now recommended treatment in breast cancer patients meeting specific criteria [72, 73], we could not compare between patients receiving conventional and hypofractionated WBRT, as our study began enrollment in 2003 before this treatment recommendation was made. As with all self-reported data, social desirability bias has been reported in both telephone [74] and face-to-face interviews [75]. However, other research supports using telephone surveys, even where sensitive health information is being collected [76]. As we recruited women 40 years of age or older from a National Cancer Institute-designated comprehensive cancer center and another academic medical center in St. Louis, MO, our results may not be generalizable to younger breast cancer patients, who often report worse QOL than older patients [77,78,79], or to patients receiving treatment in rural or community settings. Although the racial/ethnic composition of our sample was representative of the St. Louis metropolitan area, few non-white participants were Hispanic or Asian, further limiting generalizability.
In conclusion, early-stage breast cancer patients can benefit from less-severe, short-term side effects of APBI with no differential impact on QOL improvements in the first two years after diagnosis. Rigorously designed and implemented longitudinal studies examining late-effects of treatment and long-term QOL outcomes in early-stage breast cancer survivors are warranted given the expected longevity of this group of survivors [80].
References
National Comprehensive Cancer Network (2008) NCCN clinical practice guidelines in oncology: Breast cancer, v. 2.2008. http://www.nccn.org/professionals/physician_gls/PDF/breast.pdf. Accessed 4 Feb 2008
Hughes KS, Schnaper LA, Berry D, Cirrincione C, McCormick B, Shank B, Wheeler J, Champion LA, Smith TJ, Smith BL, Shapiro C, Muss HB, Winer E, Hudis C, Wood W, Sugarbaker D, Henderson IC, Norton L (2004) Lumpectomy plus tamoxifen with or without irradiation in women 70 years of age or older with early breast cancer. N Engl J Med 351(10):971–977. doi:10.1056/NEJMoa040587
Hughes KS, Schnaper LA, Bellon JR, Cirrincione CT, Berry DA, McCormick B, Muss HB, Smith BL, Hudis CA, Winer EP, Wood WC (2013) Lumpectomy plus tamoxifen with or without irradiation in women age 70 years or older with early breast cancer: long-term follow-up of CALGB 9343. J Clin Oncol 31(19):2382–2387. doi:10.1200/jco.2012.45.2615
Kunkler IH, Williams LJ, Jack WJL, Cameron DA, Dixon JM (2015) Breast-conserving surgery with or without irradiation in women aged 65 years or older with early breast cancer (PRIME II): a randomised controlled trial. Lancet Oncol 16(3):266–273. doi:10.1016/S1470-2045(14)71221-5
Polgár C, Fodor J, Major T, Németh G, Lövey K, Orosz Z, Sulyok Z, Takácsi-Nagy Z, Kásler M (2007) Breast-conserving treatment with partial or whole breast irradiation for low-risk invasive breast carcinoma—5-year results of a randomized trial. Int J Radiat Oncol Biol Phy 69(3):694–702
Livi L, Meattini I, Marrazzo L, Simontacchi G, Pallotta S, Saieva C, Paiar F, Scotti V, De Luca Cardillo C, Bastiani P, Orzalesi L, Casella D, Sanchez L, Nori J, Fambrini M, Bianchi S (2015) Accelerated partial breast irradiation using intensity-modulated radiotherapy versus whole breast irradiation: 5-year survival analysis of a phase 3 randomised controlled trial. Eur J Cancer 51(4):451–463. doi:10.1016/j.ejca.2014.12.013
Wobb JL, Shah C, Chen PY, Wallace M, Ye H, Jawad MS, Grills IS (2015) Brachytherapy-based accelerated partial breast irradiation provides equivalent 10-year outcomes to whole breast irradiation: a matched-pair analysis. Am J Clin Oncol. doi:10.1097/coc.0000000000000082
Antonucci JV, Wallace M, Goldstein NS, Kestin L, Chen P, Benitez P, Dekhne N, Martinez A, Vicini F (2009) Differences in patterns of failure in patients treated with accelerated partial breast irradiation versus whole-breast irradiation: a matched-pair analysis with 10-year follow-up. Int J Radiat Oncol Biol Phys 74(2):447–452. doi:10.1016/j.ijrobp.2008.08.025
Shah C, Wilkinson JB, Lyden M, Mbah A, Keisch M, Beitsch P, Vicini FA (2012) Comparison of survival and regional failure between accelerated partial breast irradiation and whole breast irradiation. Brachytherapy 11(4):311–315. doi:10.1016/j.brachy.2012.01.008
Ferraro D, Garsa A, DeWees T, Margenthaler J, Naughton M, Aft R, Gillanders W, Eberlein T, Matesa M, Zoberi I (2012) Comparison of accelerated partial breast irradiation via multicatheter interstitial brachytherapy versus whole breast radiation. Radiat Oncol 7(1):53
Goodwin A, Parker S, Ghersi D, Wilcken N (2009) Post-operative radiotherapy for ductal carcinoma in situ of the breast. Cochrane Database Syst Rev. doi:10.1002/14651858.CD000563.pub5
James ML, Lehman M, Hider PN, Jeffery M, Hickey BE, Francis DP (2010) Fraction size in radiation treatment for breast conservation in early breast cancer. Cochrane Database Systematic Rev. doi:10.1002/14651858.CD003860.pub3
Goodwin A, Parker S, Ghersi D, Wilcken N (2013) Post-operative radiotherapy for ductal carcinoma in situ of the breast. Cochrane Database Syst Rev. doi:10.1002/14651858.CD000563.pub7
Hickey BE, James ML, Lehman M, Hider PN, Jeffery M, Francis DP (2016) Fraction size in radiation therapy for breast conservation in early breast cancer. Cochrane Database Syst Rev. doi:10.1002/14651858.CD003860.pub4
Hickey BE, Lehman M, Francis DP (2016) Partial breast irradiation for early breast cancer (Review). Cochrane Database Syst Rev. doi:10.1002/14651858.CD007077.pub3
Whelan TJ, Levine M, Julian J, Kirkbride P, Skingley P (2000) The effects of radiation therapy on quality of life of women with breast carcinoma: results of a randomized trial. Ontario Clinical Oncology Group. Cancer 88(10):2260–2266
Hau E, Browne L, Capp A, Delaney GP, Fox C, Kearsley JH, Millar E, Nasser EH, Papadatos G, Graham PH (2013) The impact of breast cosmetic and functional outcomes on quality of life: long-term results from the St. George and Wollongong randomized breast boost trial. Breast Cancer Res Treat 139(1):115–123. doi:10.1007/s10549-013-2508-z
Garsa AA, Ferraro DJ, DeWees TA, Deshields TL, Margenthaler JA, Cyr AE, Naughton M, Aft R, Gillanders W, Eberlein T, Matesa MA, Ochoa LL, Zoberi I (2013) A prospective longitudinal clinical trial evaluating quality of life after breast-conserving surgery and high-dose-rate interstitial brachytherapy for early-stage breast cancer. Int J Radiat Oncol Biol Phys 87(5):1043–1050
Belkacemi Y, Chauvet M, Giard S, Villette S, Lacornerie T, Bonodeau F, Baranzelli M, Bonneterre J, Lartigau E (2009) Partial breast irradiation as sole therapy for low risk breast carcinoma: early toxicity, cosmesis and quality of life results of a MammoSite brachytherapy phase II study. Radiother Oncol 90(1):23–29
Lemanski C, Azria D, Gourgon-Bourgade S, Gutowski M, Rouanet P, Saint-Aubert B, Ailleres N, Fenoglietto P, Dubois JB (2010) Intraoperative radiotherapy in early-stage breast cancer: results of the montpellier phase II trial. Int J Radiat Oncol Biol Phys 76(3):698–703. doi:10.1016/j.ijrobp.2009.02.039
Taunk N, Haffty B, Chen S, Khan A, Nelson C, Pierce D, Goyal S (2011) Comparison of radiation-induced fatigue across 3 different radiotherapeutic methods for early stage breast cancer. Cancer 117(18):4116–4124
Meattini I, Saieva C, Marrazzo L, Di Brina L, Pallotta S, Mangoni M, Meacci F, Bendinelli B, Francolini G, Desideri I, De Luca Cardillo C, Scotti V, Furfaro IF, Rossi F, Greto D, Bonomo P, Casella D, Bernini M, Sanchez L, Orzalesi L, Simoncini R, Nori J, Bianchi S, Livi L (2015) Accelerated partial breast irradiation using intensity-modulated radiotherapy technique compared to whole breast irradiation for patients aged 70 years or older: subgroup analysis from a randomized phase 3 trial. Breast Cancer Res Treat 153(3):539–547. doi:10.1007/s10549-015-3565-2
Wadasadawala T, Sarin R, Budrukkar A, Jalali R, Munshi A, Badwe R (2009) Accelerated partial-breast irradiation vs conventional whole-breast radiotherapy in early breast cancer: a case-control study of disease control, cosmesis, and complications. J Cancer Res Ther 5(2):93–101
Flynn C, Wallace M, Balasubramaniam M, Kestin L, Chen PY (2006) An assessment of quality of life for patients undergoing radiotherapy with whole breast irradiation compared to accelerated partial breast irradiation. Int J Radiat Oncol Biol Phys 66(3):S134. doi:10.1016/j.ijrobp.2006.07.274
Flynn C, Hardy M, Mitchell C, Wallace M, Vicini F, Martinez A (2003) A comparison of quality of life (QOL) for patients with early stage breast cancer treated with whole breast irradiation versus targeted partial breast brachytherapy. Int J Radiat Oncol Biol Phys 57(2):S310. doi:10.1016/s0360-3016(03)01180-5
Flynn CJ, Mitchell C, Boyea G, Vicini F, Martinez A (2007) A comparison of quality of life for early stage breast cancer examining various treatment modalities and no chemotherapy. Int J Radiat Oncol Biol Phys 69(3):S583–S584. doi:10.1016/j.ijrobp.2007.07.1870
Flynn CJ, Mitchell C, Limbacher A, Vicini F, Martinez A (2010) A comparison of quality of life for early stage breast cancer examining whole breast imrt versus accelerated partial breast irradiation. Int J Radiat Oncol Biol Phys 78(3):S609–S610. doi:10.1016/j.ijrobp.2010.07.1419
He Z-Y, Tong Q, Wu S-G, Li F-Y, Lin H-X, Guan X-X (2012) A comparison of quality of life of early breast cancer patients treated with accelerated partial breast irradiation versus whole breast irradiation in China. Breast Cancer Res Treat 133(2):545–552. doi:10.1007/s10549-011-1793-7
Wadasadawala T, Budrukkar A, Chopra S, Badwe R, Hawaldar R, Parmar V, Jalali R, Sarin R (2009) Quality of life after accelerated partial breast irradiation in early breast cancer: matched pair analysis with protracted whole breast radiotherapy. Clin Oncol 21(9):668–675. doi:10.1016/j.clon.2009.07.014
Albuquerque K, Janusek L, Mathews H, Millbrandt L, Gabram S (2010) Short-term quality of life following partial breast irradiation with balloon brachytherapy- comparison with whole breast irradiation. Breast J 16(3):325–326. doi:10.1111/j.1524-4741.2009.00895.x
Albuquerque K, Tell D, Lobo P, Millbrandt L, Mathews H, Witek Janusek L (2012) Impact of partial versus whole breast radiation therapy on fatigue, perceived stress, quality of life and natural killer cell activity in women with breast cancer. BMC Cancer 12(1):1–12. doi:10.1186/1471-2407-12-251
Welzel G, Boch A, Sperk E, Hofmann F, Kraus-Tiefenbacher U, Gerhardt A, Suetterlin M, Wenz F (2013) Radiation-related quality of life parameters after targeted intraoperative radiotherapy versus whole breast radiotherapy in patients with breast cancer: results from the randomized phase III trial TARGIT-A. Radiat Oncol 8:9. doi:10.1186/1748-717x-8-9
Jeffe DB, Pérez M, Liu Y, Collins KK, Aft RL, Schootman M (2012) Quality of life changes over time in women diagnosed with ductal carcinoma in situ, early-stage invasive breast cancer, and age-matched controls. Breast Cancer Res Treat 134:379–391
Pérez M, Liu Y, Schootman M, Aft R, Schechtman K, Gillanders W, Jeffe D (2010) Changes in sexual problems over time in women with and without early-stage breast cancer. Menopause 17(5):924–937
Collins K, Liu Y, Schootman M, Aft R, Yan Y, Dean G, Eilers M, Jeffe D (2011) Effects of breast cancer surgery and surgical side effects on body image over time. Breast Cancer Res Treat 126(1):167–176
Leitch AM, Dodd GD, Costanza M, Linver M, Pressman P, McGinnis L, Smith RA (1997) American cancer society guidelines for the early detection of breast cancer: update 1997. CA 47:150–153
Carrera C, Payne S (1999) Ductal carcinoma in situ (DCIS) of the breast: the need for psychosocial research. Psychooncology 8:538–545
Katzman R, Brown T, Fuld P, Peck A, Schechter R, Schimmel H (1983) Validation of a short orientation-memory-concentration test of cognitive impairment. Am J Psychiatry 140:734–739
Schootman M, Jeffe DB, West MM, Aft R (2005) Elderly patients’ self-reports of receipt of some breast cancer treatments was an acceptable alternative to SEER-registry data. J Clin Epidemiol 58:1316–1319
Gupta V, Gu K, Chen Z, Lu W, Shu XO, Zheng Y (2011) Concordance of self-reported and medical chart information on cancer diagnosis and treatment. BMC Med Res Methodol 11:72. doi:10.1186/1471-2288-11-72
Barisic A, Glendon G, Weerasooriya N, Andrulis IL, Knight JA (2012) Accuracy of self-reported breast cancer information among women from the Ontario site of the Breast Cancer Family Registry. J Cancer Epidemiol 2012:310804. doi:10.1155/2012/310804
Yen TW, Sparapani RA, Guo C, Neuner JM, Laud PW, Nattinger AB (2010) Elderly breast cancer survivors accurately self-report key treatment information. J Am Geriatr Soc 58(2):410–412. doi:10.1111/j.1532-5415.2009.02714.x
Arthur DW, Vicini FA, Kuske RR, Wazer DE, Nag S (2003) Accelerated partial breast irradiation: an updated report from the American Brachytherapy Society. Brachytherapy 2(2):124–130. doi:10.1016/S1538-4721(03)00107-7
Smith BD, Arthur DW, Buchholz TA, Haffty BG, Hahn CA, Hardenbergh PH, Julian TB, Marks LB, Todor DA, Vicini FA, Whelan TJ, White J, Wo JY, Harris JR (2009) Accelerated partial breast irradiation consensus statement from the American Society for Radiation Oncology (ASTRO). Int J Radiat Oncol Biol Phys 74(4):987–1001. doi:10.1016/j.ijrobp.2009.02.031
Brady MJ, Cella DF, Mo F, Bonomi AE, Tulsky DS, Lloyd SR, Deasy S, Cobleigh M, Shiomoto G (1997) Reliability and validity of the functional assessment of cancer therapy-breast quality of life instrument. J Clin Oncol 15:974–986
Hays RD, Sherbourne CD, Mazel RM (1993) The RAND 36-item health survey 1.0. Health Econ 2:217–227
Schwartz AL, Nail LM, Chen RNS, Meek P, Barsevick AM, King ME, Jones LS (2000) Fatigue patterns observed in patients receiving chemotherapy and radiotherapy. Cancer Investig 18(1):11–19. doi:10.3109/07357900009023057
Hickok JT, Morrow GR, Roscoe JA, Mustian K, Okunieff P (2005) Occurrence, severity, and longitudinal course of twelve common symptoms in 1129 consecutive patients during radiotherapy for cancer. J Pain Symptom Manag 30(5):433–442. doi:10.1016/j.jpainsymman.2005.04.012
Noal S, Levy C, Hardouin A, Rieux C, Heutte N, Ségura C, Collet F, Allouache D, Switsers O, Delcambre C, Delozier T, Henry-Amar M, Joly F (2011) One-year longitudinal study of fatigue, cognitive functions, and quality of life after adjuvant radiotherapy for breast cancer. Int J Radiat Oncol Biol Phys 81(3):795–803
Schnur JB, Ouellette SC, Bovbjerg DH, Montgomery GH (2009) Breast cancer patients’ experience of external-beam radiotherapy. Qual Health Res 19(5):668–676. doi:10.1177/1049732309334097
Sherbourne CD, Stewart AL (1991) The MOS social support survey. Soc Sci Med 32(6):705–714
Katz JN, Chang LC, Sangha O, Fossel AH, Bates DW (1996) Can comorbidity be measured by questionnaire rather than medical record review? Med Care 34(1):73–84
Charlson ME, Pompei P, Ales K, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Beck AT, Epstein N, Brown G, Steer RA (1988) An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol 56:893–897
Houghton J, George WD, Cuzick J, Duggan C, Fentiman IS, Spittle M, UK Coordinating Committee on Cancer Research, Ductal Carcinoma in situ Working Party, DCIS trialists in the UK A, and New Zealand (2003) Radiotherapy and tamoxifen in women with completely excised ductal carcinoma in situ of the breast in the UK, Australia, and New Zealand: randomised controlled trial. The Lancet 362:95–102
Landis J, Koch G (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Dragun AE, Harper JL, Taylor CE, Jenrette JM (2008) Patient satisfaction and quality of life after MammoSite breast brachytherapy. Am J Surg 196(4):545–548. doi:10.1016/j.amjsurg.2008.06.014
Chafe S, Moughan J, McCormick B, Wong J, Pass H, Rabinovitch R, Arthur DW, Petersen I, White J, Vicini FA (2013) Late toxicity and patient self-assessment of breast appearance/satisfaction on RTOG 0319: a phase 2 trial of 3-dimensional conformal radiation therapy-accelerated partial breast irradiation following lumpectomy for stages I and II breast cancer. Int J Radiat Oncol Biol Phys 86(5):854–859. doi:10.1016/j.ijrobp.2013.04.005
Garsa AA, Ferraro DJ, DeWees T, Margenthaler JA, Naughton M, Aft R, Gillanders WE, Eberlein T, Matesa MA, Zoberi I (2013) Cosmetic analysis following breast-conserving surgery and adjuvant high-dose-rate interstitial brachytherapy for early-stage breast cancer: a prospective clinical study. Int J Radiat Oncol Biol Phys 85(4):965–970. doi:10.1016/j.ijrobp.2012.08.027
Jagsi R, Abrahamse P, Morrow M, Hawley ST, Griggs JJ, Graff JJ, Hamilton AS, Katz SJ (2010) Patterns and correlates of adjuvant radiotherapy receipt after lumpectomy and after mastectomy for breast cancer. J Clin Oncol 28(14):2396–2403. doi:10.1200/jco.2009.26.8433
Hepel JT, Tokita M, MacAusland SG, Evans SB, Hiatt JR, Price LL, DiPetrillo T, Wazer DE (2009) Toxicity of three-dimensional conformal radiotherapy for accelerated partial breast irradiation. Int J Radiat Oncol Biol Phys 75(5):1290–1296. doi:10.1016/j.ijrobp.2009.01.009
Back M, Ahern V, Delaney G, Graham P, Steigler A, Wratten C, for the New South Wales Breast Radiation Oncology Group (2005) Absence of adverse early quality of life outcomes of radiation therapy in breast conservation therapy for early breast cancer. Australas Radiol 49(1):39–43. doi:10.1111/j.1440-1673.2005.01392.x
Rayan G, Dawson LA, Bezjak A, Lau A, Fyles AW, Yi Q-L, Merante P, Vallis KA (2003) Prospective comparison of breast pain in patients participating in a randomized trial of breast-conserving surgery and tamoxifen with or without radiotherapy. Int J Radiat Oncol Biol Phys 55(1):154–161. doi:10.1016/S0360-3016(02)03826-9
Fyles AW, McCready DR, Manchul LA, Trudeau ME, Merante P, Pintilie M, Weir LM, Olivotto IA (2004) Tamoxifen with or without breast irradiation in women 50 years of age or older with early breast cancer. N Engl J Med 351(10):963–970. doi:10.1056/NEJMoa040595
Williams LJ, Kunkler IH, King CC, Jack W, van der Pol M (2011) A randomised controlled trial of post-operative radiotherapy following breast-conserving surgery in a minimum-risk population. Quality of life at 5 years in the PRIME trial. Health Technol Asses 15(12):i–xi, 1–57. doi:10.3310/hta15120
Fisher B, Redmond C, Fisher ER, Caplan R (1988) Relative worth of estrogen or progesterone receptor and pathologic characteristics of differentiation as indicators of prognosis in node negative breast cancer patients: findings from National Surgical Adjuvant Breast and Bowel Project Protocol B-06. J Clin Oncol 6(7):1076–1087
Yu KD, Wu J, Shen ZZ, Shao ZM (2012) Hazard of breast cancer-specific mortality among women with estrogen receptor-positive breast cancer after five years from diagnosis: implication for extended endocrine therapy. J Clin Endocrinol Metab 97(12):E2201–E2209. doi:10.1210/jc.2012-2423
Liu Y, Schloemann DT, Lian M, Colditz GA (2015) Accelerated partial breast irradiation through brachytherapy for ductal carcinoma in situ: factors influencing utilization and risks of second breast tumors. Breast Cancer Res Treat 151(1):199–208. doi:10.1007/s10549-015-3389-0
NRG Oncology website NSABP Clinical Trials Overview: Protocol B-39/RTOG 0413http://www.nsabp.pitt.edu/B-39.asp. Accessed 24 Jul 2016
Schmidt M, Chang-Claude J, Vrieling A, Heinz J, Flesch-Janys D, Steindorf K (2012) Fatigue and quality of life in breast cancer survivors: temporal courses and long-term pattern. J Cancer Surviv 6(1):11–19
Jeffe DB, Pérez M, Cole EF, Liu Y, Schootman M (2016) The effects of surgery type and chemotherapy on early-stage breast cancer patients’ quality of life over 2-year follow-up. Ann Surg Oncol 23(3):735–743. doi:10.1245/s10434-015-4926-0
Whelan TJ, Pignol J-P, Levine MN, Julian JA, MacKenzie R, Parpia S, Shelley W, Grimard L, Bowen J, Lukka H, Perera F, Fyles A, Schneider K, Gulavita S, Freeman C (2010) Long-term results of hypofractionated radiation therapy for breast cancer. N Engl J Med 362(6):513–520. doi:10.1056/NEJMoa0906260
Kacprowska A, Jassem J (2012) Hypofractionated radiotherapy for early breast cancer: review of phase III studies. Rep Pract Oncol Radiother 17(2):66–70. doi:10.1016/j.rpor.2011.10.003
Maguire KB (2009) Does mode matter? A comparison of telephone, mail, and in-person treatments in contingent valuation surveys. J Environ Manag 90(11):3528–3533
Turner AN, De Kock AE, Meehan-Ritter A, Blanchard K, Sebola MH, Hoosen AA, Coetzee N, Ellertson C (2009) Many vaginal microbicide trial participants acknowledged they had misreported sensitive sexual behavior in face-to-face interviews. J Clin Epidemiol 62(7):759–765
Kramer JR, Chan G, Kuperman S, Bucholz KK, Edenberg HJ, Schuckit MA, Polgreen LA, Kapp ES, Hesselbrock VM, Nurnberger JI, Bierut LI (2009) A comparison of diagnoses obtained from in-person and telephone interviews, using the semi-structured assessment for the genetics of alcoholism (SSAGA). J Stud Alcohol Drugs 70(4):623–627
Arora NK, Gustafson DH, Hawkins RP, McTavish F, Cella DF, Pingree S, Mendenhall JH, Mahvi DM (2001) Impact of surgery and chemotherapy on the quality of life of younger women with breast carcinoma: a prospective study. Cancer 92(5):1288–1298
Avis NE, Crawford S, Manuel J (2004) Psychosocial problems among younger women with breast cancer. Psychooncology 13(5):295–308
Bloom JR, Stewart SL, Oakley-Girvan I, Banks PJ, Shema S (2012) Quality of life of younger breast cancer survivors: persistence of problems and sense of well-being. Psychooncology 21:655–665
US Department of Health and Human Services, National Institutes of Health National Cancer Institute. Living beyond cancer: finding a new balance. President’s Cancer Panel: 2003–2004 Annual Report. http://deainfo.nci.nih.gov/advisory/pcp/annualReports/pcp03-04rpt/Survivorship.pdf. Accessed 25 Jul 2016
Acknowledgements
This study was supported by a Grant from the National Cancer Institute (NCI) and Breast Cancer Stamp Fund (R01 CA102777; PI: Jeffe, DB). Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the NCI or Breast Cancer Stamp Fund. We thank our participants, the interviewers, and services provided by Ms. Lori Grove in Oncology Data Services and the Health Behavior, Communication and Outreach Core, which were supported, in part, by the National Cancer Institute Cancer Center Support Grant to the Alvin J. Siteman Cancer Center at Barnes-Jewish Hospital and Washington University School of Medicine in St. Louis, Missouri (P30 CA091842; PI: Timothy Eberlein). We also thank the physicians who helped us recruit their patients for this study, including Drs. Barbara Monsees, Jill Dietz, Julie Margenthaler, Virginia Herrmann, Timothy Eberlein, Matthew Ellis, Imran Zoberi, Marie Taylor, Michael Naughton, Antonella Rastelli, Donald Lombardi, Cynthia Ma, Loren Michel, and Rama Suresh at Washington University School of Medicine and Dr. Eddie Hsueh and Pam Hunborg, RN, at Saint Louis University School of Medicine. The Beck Anxiety Inventory ® and BAI ® (copyright 1990, 1993 by Aaron T. Beck), are trademarks of The Psychological Corporation, a Harcourt Assessment Company. The BAI ® was adapted and used by permission of the publisher, The Psychological Corporation. All rights reserved.
Funding
This study was funded by a grant from the National Cancer Institute (NCI) and Breast Cancer Stamp Fund (R01 CA102777; PI: Jeffe, DB) and by the NCI Cancer Center Support Grant to the Alvin J. Siteman Cancer Center at Barnes-Jewish Hospital and Washington University School of Medicine in St. Louis, Missouri (P30 CA091842; PI: Timothy Eberlein), for services provided by the Health Behavior, Communication and Outreach Core.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest, financial or otherwise.
Ethical approval
The IRBs at both Washington University and Saint Louis University approved this study. All procedures performed were in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments and the institutional review boards (IRBs) at both Washington University and Saint Louis University.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Pérez, M., Schootman, M., Hall, L.E. et al. Accelerated partial breast irradiation compared with whole breast radiation therapy: a breast cancer cohort study measuring change in radiation side-effects severity and quality of life. Breast Cancer Res Treat 162, 329–342 (2017). https://doi.org/10.1007/s10549-017-4121-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-017-4121-z