
Abstract
Sexual minority women are at an elevated risk for depression compared to heterosexual women, yet less is known about how gender roles affect the mental health of sexual minority women. Existing studies examining the role of self-esteem in the relationship between gender roles and depression are scarce and have predominantly focused on heterosexual populations. Using a cross-sectional survey of Chinese lesbians in Hong Kong (N = 438), the study tested the direct and indirect effects of different types of gender roles (masculine, feminine, and androgynous) on depression through the mediating factor of self-esteem. We found that masculinity and androgyny were positively associated with self-esteem, while femininity was negatively associated with self-esteem. More importantly, self-esteem fully mediated the inverse relationship between masculinity and depression and that between androgyny and depression. The positive relationship between femininity and depression was also fully mediated by self-esteem. By examining different types of gender roles and incorporating gender roles, self-esteem, and depression into a unified framework, the research highlighted the particularly protective effect of androgyny, which had the strongest positive direct effect on self-esteem and indirect effect on depression through the mediation of self-esteem compared to the effects of other types of gender roles. Our results illuminate the importance of understanding how individual differences in gender roles relate to the mental health of sexual minority women in future research and interventions. Implications for interventions that help Chinese lesbians cope with gender expectations and improve their mental health are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sexual minority individuals, including lesbians and gay men, are at a higher risk for mental health problems, including depression, compared to their heterosexual counterparts (Everett, Talley, Hughes, Wilsnack, & Johnson, 2016; King et al., 2008). Meanwhile, the heterogeneity within sexual minority populations, which involve people with different biological sex, sexual orientations, and gender roles, requires concentrated research attention (Li, Pollitt, & Russell, 2016; Ross et al., 2018). With a focus on gender-related traits, research has shown that lesbians tend to describe themselves as more masculine than heterosexual women, and gay men more feminine than heterosexual men (Lippa, 2000, 2002). The observed sexual orientation differences in self-ascribed masculinity–femininity are considerably larger for women than for men in both Chinese and Western contexts due in part to the fact that it is less socially undesirable for lesbians to cross gender boundaries compared to gay men (Lippa, 2005, 2008; Zheng, Lippa, & Zheng, 2011). Nevertheless, previous studies have rarely examined the reasons why and the conditions under which masculinity and femininity affect the mental health of sexual minority people. The current research fills this gap by examining the mechanism through which different gender roles affect the mental health of lesbians in the Hong Kong Chinese context.
Gender Roles (Based on Gender-Stereotypical Personality Traits) and Mental Health
Given gender polarization (treating femininity and masculinity as polar opposites) in many cultures, individuals gradually develop ideas about what it means to be masculine or feminine, or in Bem’s (1981) terms, gender schemas. People tend to associate masculinity with instrumental roles such as assertiveness and leadership and to associate femininity with communal roles such as compassion and nurturance (Bem, 1974; Hill & Lynch, 1983; Spence & Helmreich, 1978, 1980). The social construction of these binary gender roles (masculinity and femininity) prescribes how men and women are expected to act, respectively. Any deviation from the socially defined content of gender schemas is considered a violation of the norms in a heteronormative society (Bem, 1981).
To date, little attention has been paid to assess gender roles and their association with mental health among sexual minority people, who are often perceived to have challenged both heterosexual norms and traditional gender expectations (Starr & Zurbriggen, 2017). The majority of previous studies have examined sexual minority people’s gender expressions and behaviors, which often do not conform to traditional gender norms in childhood and/or adulthood (Bailey & Zucker, 1995; Li et al., 2016; Rieger & Savin-Williams, 2012; Rosario, Schrimshaw, & Hunter, 2008). There is evidence that lesbians and gay men who demonstrate explicit gender nonconforming behaviors in childhood and/or adolescence are often stigmatized and rejected by others and thus are subject to an elevated level of depression (Collier, Van Beusekom, Bos, & Sandfort, 2013; Rieger & Savin-Williams, 2012; Roberts, Rosario, Slopen, Calzo, & Austin, 2013). The focus on observable behaviors may, however, overlook the roles of masculine and feminine personality traits in sexual minority individuals. These personality traits, although less visible, are a significant aspect of gender that substantially impacts one’s mental health.
Evidence has shown that displaying gender nonconforming physical appearance, gestures, and behaviors is perceived as violating gender norms and thus makes people prone to stigmatization (Baams, Beek, Hille, Zevenbergen, & Bos, 2013; Roberts et al., 2013); whether endorsing cross-gender personality traits is associated with poorer mental health is still open to debate. Psychological androgyny, a term used to denote flexible engagement in both masculinity and femininity within a single individual (Bem, 1974), has stimulated considerable research (Dean & Tate, 2017; Keener & Mehta, 2017). Theoretically, the notion of psychological androgyny indicates that the endorsement of both masculine and feminine personality traits is linked to better mental health because of cognitive flexibility inherent in androgyny which allows individuals to freely and effectively engage in activities regardless of masculine or feminine stereotypes (Bem, 1981; Martin, Cook, & Andrews, 2017). In contrast, gender-typed individuals with a strong self-concept as one gender would avoid activities that are stereotypically prescribed for the other gender and thus limit their own adaptability and lead to poorer mental health (Barrett & White, 2002; Whitley, 1985).
Attempts to test Bem’s notion of psychological androgyny have yielded mixed results. Research has found that androgynous personality traits are associated with higher levels of self-esteem, lower levels of depressive symptoms, and optimal mental health among men and women (Buckley & Carter, 2005; Juster et al., 2016; Lefkowitz & Zeldow, 2006). Other studies have shown that it is the strong effect of masculinity, rather than a joint effect of masculinity and femininity, that contributes to mental health (Kopper & Epperson, 1996; Whitley, 1985). Research has found that masculine traits are more consistently associated with better mental health, such as self-esteem and decreased symptoms of depression, than are feminine traits (Carlson & Steuer, 1985; Gonzalez, Bockting, Beckman, & Durán, 2012; Leung & Moore, 2003). Some studies in the U.S. have shown that femininity is associated with higher levels of depression and lower levels of self-esteem (Helgeson, 1994; Kreiger & Dumka, 2006; Mosher & Danoff-Burg, 2008; Whitley, 1985), whereas others have found femininity to be associated with better interpersonal and marital functioning (Aube, Norcliffe, Craig, & Koestner, 1995; Kurdek & Schmitt, 1986).
Despite inconsistent results concerning the association between different types of gender roles and mental health, Bem’s (1974) theorization of gender, coupled with the construction of the Bem Sex Role Inventory (BSRI), plays a significant role in psychological studies of gender because it challenges the traditional polarized view of gender. It asserts that masculinity and femininity exist on two separate continua rather than on a single bipolar dimension and can be seen in one single individual. Drawing on Bem’s (1974, 1981) theoretical perspective, our present research extended current discussions which have predominantly focused on heterosexual populations and examined lesbians’ gender roles using the BSRI (Bem, 1974). The BSRI measures the extent to which an individual possesses personality traits that are stereotypically masculine or feminine. It categorizes respondents into four gender role categories: masculine, feminine, androgynous (high levels of both masculinity and femininity), and undifferentiated (low levels of both masculinity and femininity). In the present study, such categorization offered insight into the ways in which lesbians perceived the world and their self-concepts through the lens of gender schemas.
This study focused on lesbians and identified risk factors associated with depression with the aim of contributing to a better understanding of mental health disparities within sexual minority populations. As shown in one study (Marshal et al., 2013), sexual minority youth reported higher rates of depression and suicidality in early adolescence than did their heterosexual counterparts and, more importantly, these observed disparities were the largest for girls and bisexual-identified youth over time. Recent research has highlighted the urgent need for in-depth analyses of mental health disparities among sexual minority individuals (Li et al., 2016; Plöderl & Tremblay, 2015). Therefore, with a focus on gender roles, the current study attempted to describe and understand the mental health status of lesbians as a vulnerable subgroup of sexual minority populations.
Self-Esteem as a Mediator in the Relationship Between Gender Roles and Depression
Although gender roles and self-esteem are considered key factors that contribute to depression (Orth, Robins, & Roberts, 2008; Ryu et al., 2006), studies of sexual minority people rarely integrate these two variables into a unified framework to provide additional insights into the complex phenomenon of depression. Informed by both theories and prior empirical research, our research tested the mediating role of self-esteem in the relationship between gender roles and depression.
Drawing on the theoretical insights into the notion of self provided by social identity theory (Tajfel & Turner, 1979; Turner, Hogg, Oakes, Reicher, & Wetherell, 1987) and gender schema theory (Bem, 1981, 1993), the present study used the BSRI to assess the extent to which social categories of masculinity and femininity were reflected in lesbians’ self-definitions of their gendered sense of self (Bem, 1974). Social identity theory posits that social identities are shaped by individuals’ self-identification with certain social groups or categories. People tend to integrate positive attributes associated with self-relevant groups or categories into their self-concepts and determine their personal feelings of worth (Wood & Eagly, 2015). The gendered self plays a key role, among other important identities, in an individual’s global feelings of self-worth (Wood & Eagly, 2015), which is referred to as self-esteem (Rosenberg, 1965). Based on the above-mentioned theories and empirical results of the association between gender roles and self-esteem (Buckley & Carter, 2005; Whitley, 1985), we hypothesized the relationship between the two variables in our mediation model.
In addition, theory and empirical studies have indicated that low levels of self-esteem lead to depression (Beck, 1967; Orth et al., 2008; Trzesniewski et al., 2006), informing our hypothesis that gender roles would be associated with depression through the mediating role of self-esteem. The vulnerability model of depression serves as a prominent theoretical model which suggests that low self-esteem causally influences the onset and maintenance of depression (Beck, 1967; Metalsky, Joiner, Hardin, & Abramson, 1993). In other words, a negative view of self is a key predictor of depression (Beck, 1967). Empirical findings also consistently support the vulnerability model (Orth et al., 2008; Trzesniewski et al., 2006). For instance, results from a 23-year longitudinal study in Germany showed that not only low levels of self-esteem but also a decline in levels of self-esteem during adolescence predicted depression in adulthood two decades later (Steiger, Allemand, Robins, & Fend, 2014). Using a sample of gay men and lesbians in the U.S., Otis and Skinner (1996) found that self-esteem was the strongest predictor of depression among other predictors, including victimization, social support, external stress, and internalized homophobia.
Furthermore, empirical evidence from the 1980s has documented the mediating role of self-esteem in the relationship between gender roles and depression (e.g., Feather, 1985; Lu & Wu, 1998; Whitley & Gridley, 1993). For instance, Lu and Wu (1998) tested the mediating effect of self-esteem with a sample of 300 clinical nurses who worked in six different hospitals in Taiwan. Their study demonstrated that self-esteem fully mediated the effects of gender roles (i.e., masculinity and femininity, respectively) on depression. On the other hand, using a sample of 200 students enrolled in a psychology class in the U.S., Whitley and Gridley (1993) found that self-esteem had a significant mediating effect on the inverse relationship between masculinity and depression, but femininity had no significant relationship with self-esteem and depression. Similarly, a study of Korean male high school students undertaken by Choi, Kim, Hwang, and Heppner (2010) found that masculinity, which was labeled instrumentality, did not directly influence depression, but had indirect effects on depression through the mediation of self-esteem. While these studies have yielded significant but slightly different results across various settings and countries, they have predominantly focused on heterosexual populations but neglected sexual minority people.
The Current Study
Building on the above-mentioned theories and previous studies that have assessed the mediating role of self-esteem in the relationship between gender roles and depression using heterosexual samples (Choi et al., 2010; Lu & Wu, 1998; Whitley & Gridley, 1993), our study tested the extent to which these findings were consistent with lesbians in the Hong Kong Chinese context.
Drawing from the literature review, the study had three hypotheses: (1a) masculinity and androgyny would each be positively associated with self-esteem and negatively associated with depression; (1b) femininity would be negatively associated with self-esteem and positively associated with depression; (2) each type of gender role would be associated with depression through the mediation of self-esteem. Specifically, masculinity and androgyny would each have a significant association with high levels of self-esteem, which would, in turn, be associated with low levels of depression. In contrast, femininity would have a significant association with low levels of self-esteem, which would, in turn, be associated with high levels of depression; and (3) there would be impact differences in direct and indirect effects of each type of gender role on depression.
Method
Participants
We recruited participants between December 2014 and March 2015 mainly through local lesbian, gay, bisexual, and trans (LGBT) organizations and the University of Hong Kong. The ethics research committee of the University of Hong Kong approved the study.
Five local LGBT organizations facilitated the online dissemination of the survey to their members through their mailing lists and social networks. The survey was also distributed online through the e-mail delivery system of the university to all students, staff, alumni, and faculty of all disciplines (27,933 students and 10,965 staff in the 2014–2015 academic year). Similar to nonprobability procedures of prior research that recruited sexual minority respondents (Meyer & Wilson, 2009), the study utilized snowball sampling to reach personal networks of people who were informed about the study so as to recruit an adequate sample of Chinese lesbians in Hong Kong.
The first page of the online survey provided potential participants with a clear description of the research and allowed them to complete an informed consent form and to confirm that they met the inclusion criteria of the research. Hong Kong female citizens aged between 18 and 35 who identified themselves as lesbians and were able to read and speak Chinese were eligible for the study. The current sample was restricted to women who were ethnically Chinese in order to avoid potential confounding differences in cultural background. No compensation was directly given to participants except, upon completion of the survey, they were entered into a lottery draw with a prize worth HK$500 (around US$64).
A total of 438 self-identified lesbians completed the online survey. Respondents ranged in age from 18 to 35 years with a mean of 24.67 years (SD = 4.60). More than half of the respondents had a full-time job (54.3%), while a significant number of respondents were full-time students (35.6%), and fewer were employed part-time (5.5%), unemployed (3.0%), or had “other” types of employment status (1.6%). Most respondents were undergoing or had completed university education (82.2%), while some had had high school or diploma education (17.8%). Most were currently in a same-sex relationship (55.3%), while a significant number of respondents were single (39.0%), fewer were engaged to their same-sex partner (4.6%), and only 1.1% were married to their same-sex partner. Most respondents reported no religious affiliation (73.1%), but a significant number of respondents identified as Protestant (12.8%), and fewer identified as either Catholic (7.3%), as Buddhist (3.9%) or as having “other” types of religion (2.9%).
Measures
Gender Roles
The Bem Sex Role Inventory (BSRI) (Bem, 1974) was used to assess respondents’ endorsement of gender-stereotypical personality traits. It consists of 20 masculine gender role items (e.g., independent, forceful, and ambitious) and 20 feminine gender role items (e.g., shy, affectionate, and tender). Respondents were asked to rate the degree to which these stereotypically masculine and feminine traits described their personality on a 7-point Likert scale, ranging from 1 (never or almost never true) to 7 (always or almost always true). Consequently, the BSRI yielded a masculinity score (average of 20 masculine gender role items) and a femininity score (average of 20 feminine gender role items) for each respondent, with higher scores indicating more of the masculine or feminine personality traits. This instrument has been validated and widely used with Chinese samples (Lau & Wong, 1992; Wang & Creedon, 1989; Zhang, Norvilitis, & Jin, 2001; Zheng et al., 2011). In the current study, both the Masculinity subscale (α = .84) and Femininity subscale (α = .78) showed good internal consistency.
With our focus on gender-stereotypical personality traits, the current study followed the categorization of gender roles suggested by Bem (1981), characterizing personality traits as masculine, feminine, androgynous, or undifferentiated. In order to test the mediation models, this study used dummy variables to create each gender role category with reference to the median scores of the Masculinity subscale and Femininity subscale, respectively. Specifically, respondents classified as masculine scored above the median on the Masculinity subscale and below the median on the Femininity subscale. Similarly, respondents classified as feminine scored above the median on the Femininity subscale and below the median on the Masculinity subscale. The third gender role category, androgyny, was the result of scoring above the median on both the Masculinity subscale and Femininity subscale, whereas the undifferentiated gender role category was the result of scoring below the median on both subscales.
Self-Esteem
The Rosenberg Self-Esteem Scale (RSES) (Rosenberg, 1965) is a 10-item measure designed to assess respondents’ feelings of global, personal esteem. The items (e.g., “All in all, I am inclined to feel that I am a failure” (reverse coded) and “I feel that I have a number of good qualities”) were rated on a 4-point Likert scale from 1 (strongly disagree) to 4 (strongly agree). Item scores were averaged to form a self-esteem score for each respondent, with higher scores indicating higher levels of self-esteem. The RSES is one of the most frequently used measures for assessing self-esteem and has been translated into many different languages. Satisfactory reliability and validity of the scale have been reported by numerous studies with Chinese samples (e.g., Cheung, 2006; Yu & Xie, 2008). This study adopted a Chinese version of the RSES tested by Leung and Wong (2008). Internal reliability was supported with Cronbach alpha of .89 in the current study.
Depression
Depression was assessed using the Hospital Anxiety and Depression Scale (HADS) developed by Zigmond and Snaith (1983), a measure with 7 out of 14 items that assess the presence and severity of depressive symptoms. The 7 items assessing depression (e.g., “I still enjoy the things I used to enjoy” (reverse coded) and “I feel as if I am slowed down”) were rated on a 4-point Likert scale, ranging from 0 (never or rarely in the preceding week) to 3 (most of the time or all of the time in the preceding week). Item scores were summed, with higher scores indicating higher levels of depression. The HADS has been validated and widely used across culturally diverse groups, including Chinese populations (e.g., Chan, Leung, Fong, Leung, & Lee, 2010; Martin, Thompson, & Chan, 2004). The Cronbach alpha for the depression items in the current study was .76.
Data Analysis
We conducted an ANOVA to test the differences in self-esteem and depression among groups with different gender roles (masculinity, femininity, androgyny, and undifferentiated). Tukey was used as a post hoc test.
Afterward, we conducted structural equation modeling (SEM) using Mplus 7.0 to test a measurement model and a path model. First, we tested a measurement model to ensure that the observed items of the latent constructs (self-esteem and depression) were valid indicators. The overall model fit was estimated using goodness-of-fit indices: (1) Akaike information criterion (AIC), (2) chi-square (χ2), (3) comparative fit index (CFI), (4) Tucker Lewis Index (TLI), and (5) root mean square error of approximation (RMSEA). The AIC compares the fit of different competing models. The lower values are indicative of better fit (Kelloway, 2015). The chi-square with a nonsignificant p value indicates satisfactory model fit (Bollen, 1989). Values of .96 for the CFI and TLI indicate great fit (Hu & Bentler, 1999). The RMSEA refers to a standardized measure of the lack of fit in the population data and the model, and values of less than .06 indicate good fit (Hu & Bentler, 1999). In addition, based on the results of the measurement model, the factor loadings of each latent variable were estimated and indicators with a factor loading lower than the recommended value of .50 were removed from the original model (Hair, Black, Babin, Anderson, & Tatham, 2006). After removing the items with factor loadings lower than .50, we allowed specific items in the measurement model to covary based on the information from the modified model fit indices. The model fit indices of the original model and post hoc model with the reduced items of the latent variables (self-esteem and depression) and covariances were reported.
After testing the measurement model, the path model was tested to assess direct and indirect associations among variables (gender roles, self-esteem, and depression) in the proposed model. Specifically, by using the undifferentiated gender role as a reference group, the model assessed the direct and indirect effects of each type of gender role (masculinity, femininity, and androgyny) on depression through the mediation of self-esteem among Chinese lesbians in Hong Kong. Age was used as a control variable because previous research has suggested that age tends to affect one’s self-esteem (Tate, Bettergarcia, & Brent, 2015).
Results
Differences in Self-Esteem and Depression Based on Gender Roles
As shown in Table 1, the results from the ANOVA showed significant mean differences in self-esteem (F[3, 419] = 9.24, p < .001) and depression (F[3, 421] = 15.97, p < .001) among groups. According to the post hoc test (Tukey), respondents with strong masculine and androgynous traits reported higher levels of self-esteem than those with strong feminine and undifferentiated traits. In addition, respondents with strong undifferentiated traits showed higher levels of depression than those with strong feminine, masculine, and androgynous traits.
Measurement Model
Results from the final measurement model showed good model fit for the observed data (χ2= 96.92, df = 73, CFI = .99, TLI = .99, RMSEA = .03). The TLI and CFI values were both above .99, suggesting an excellent fit of the model to the data. The RMSEA value of .03 met the criteria for a good model.
When estimating the factor loadings of each latent variable (self-esteem and depression), all indicators had a factor loading greater than .50, except Item 8 for self-esteem and Item 5 for depression (see Table 2). Therefore, Item 8 for self-esteem and Item 5 for depression were not included in the final model. The model fit of the measurement model was also improved by allowing several items to covary based on the information from the modified model fit indices. The reduced number of items based on the information of factor loadings and the incorporation of the error covariance made an improvement in model fit. This post hoc model showed good model fit (AIC = 11,023.82 vs 13,272.18, difference = 2248.36) compared to the original model (χ2[118] = 417.85, p < .001, CFI = .90, TLI = .88, RMSEA = .08) (see Table 3). Overall, the composite reliability of each latent construct was greater than .70 (self-esteem = .90, depression = .78).
Path Model
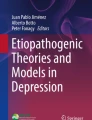
The results of the path model are shown in Fig. 1. The path model explains both direct and indirect effects of each type of gender role on depression through the mediation of self-esteem. The path model also had excellent model fit (χ2 = 148.21, df = 112, CFI = .99, TLI = .98, RMSEA = .03) as described in Fig. 1. The following direct and indirect path results partially supported our hypotheses.

Path diagram. *p < .05; **p < .01; ***p < .001. Note Model fit: χ2 = 148.21, df = 112, CFI = .99, TLI = .98, RMSEA = .03; undifferentiated gender role was used as a reference group
Direct Effects
A total of seven direct paths were tested. The results showed that four of these were statistically significant (see Table 4). Specifically, respondents’ strong masculine traits were significantly associated with higher levels of self-esteem (β = .17, p < .01). Likewise, respondents’ androgynous traits were significantly associated with higher levels of self-esteem (β = .22, p < .001). On the other hand, respondents’ strong feminine traits were significantly associated with lower levels of self-esteem (β = − .17, p < .01). Moreover, lower levels of self-esteem were significantly associated with higher levels of depressive symptoms (β = − .75, p < .001). Among the significant direct effects of gender role on self-esteem, the impact of androgynous gender role on self-esteem (β = .22) was greater than that of masculinity (β = .17) and femininity (β = − .17), respectively.
Indirect Effects
The path results also showed three significant indirect mediating effects: (1) self-esteem significantly mediated the relationship between masculinity and depression (β = − .07, p < .01); (2) self-esteem significantly mediated the relationship between femininity and depression (β = .07, p < .01); (3) self-esteem also significantly mediated the relationship between androgynous gender role and depression (β = − .14, p < .001). The results demonstrated that respondents’ strong masculine and androgynous traits were significantly associated with higher levels of self-esteem, which in turn led to lower levels of depression. However, respondents’ strong feminine traits were significantly associated with lower levels of self-esteem and then the lower levels of self-esteem were significantly associated with higher levels of depression. Among significant indirect effects of gender role on depression through the mediation of self-esteem, the indirect impact of androgynous gender role on depression (β = − .14) was greater than that of masculinity (β = − .07) and femininity (β = .07), respectively.
Discussion
Our study signifies the first important step to provide insights into the mechanism through which gender roles affect the mental health of lesbians in the Hong Kong Chinese context. After controlling for age, the current study found that masculinity and androgyny were associated with higher levels of self-esteem, which were, in turn, associated with lower levels of depression. The positive relationship between femininity and depression was also fully mediated by self-esteem. By attending to the diversity among Chinese lesbians with a major focus on different types of gender roles, the current study provides a better understanding of protective and risk factors associated with depression among this group of sexual minority women.
Our findings suggest that possessing high levels of both masculine and feminine personality traits was psychologically healthy for Chinese lesbians. The findings support our hypotheses and Bem’s (1974) notion of psychological androgyny, which posits that the endorsement of both masculine and feminine traits can be seen as an adaptive form of flexibility that is conducive to psychological adjustment. As shown by the ANOVA results, respondents who were classified as androgynous not only reported significantly higher levels of self-esteem than respondents who were classified as feminine and undifferentiated, but they also had lower levels of depression than those who were classified as undifferentiated. More importantly, the results of the mediation model suggested that androgyny provided a buffer against depression by boosting one’s self-esteem in our sample. One of the possible explanations might be that the integration of both masculinity and femininity into one’s self-concept could endow an individual with flexibility and freedom to develop a strong sense of self (Skoe, 1995). Furthermore, taking respondents’ marginalized position as Chinese sexual minority women in a predominantly heteronormative environment into account (Chow & Cheng, 2010; Kwok & Wu, 2015), transcending gender boundaries might allow lesbians to perceive themselves as capable of performing different gender roles and coping with difficult circumstances with great flexibility. As a result, androgynous personality traits played a particularly protective role in their mental health. In recent years, a considerable number of scholars have called for more research into the extent to which it is psychologically healthy to be androgynous (Dean & Tate, 2017; Keener & Mehta, 2017). It is important to continue this line of enquiry and investigate the role of androgyny among both heterosexual and sexual minority populations across different contexts.
Additionally, our results support our hypothesis that femininity was associated with lower levels of self-esteem, which were, in turn, associated with higher levels of depression among Chinese lesbians. They were consistent with previous studies showing the inverse relationship between femininity and self-esteem and positive relationship between femininity and depression in the U.S. general population (Helgeson, 1994; Kreiger & Dumka, 2006; Mosher & Danoff-Burg, 2008; Whitley, 1985). As suggested by gender schema theory (Bem, 1981, 1993) and the notion of psychological androgyny (Bem, 1974), gender-schematic people, who associate their personality traits more strongly with either gender, tend to be less psychologically healthy than gender-aschematic people with androgynous personality traits due to the tendency of the former to perceive their sense of self and their surroundings too much in terms of stereotypical masculinity or femininity. Given that China still faces more severe gender inequality than many Western countries (World Economic Forum, 2017), Chinese women tend to be socialized in a culture where traditional and polarized gender roles remain the norm (Zheng et al., 2011). It was thus unsurprising to find that endorsing personality traits that were stereotypically feminine was harmful to respondents’ self-esteem, which played a mediating role in increasing levels of depression. In other words, respondents with stereotypically feminine traits were more likely to see themselves in a negative light in the Chinese context where gender inequality persists.
Moreover, when juxtaposing this finding with some recent Western research on lesbians’ gender roles and mental health (Balsam, Beadnell, & Molina, 2012; Lehavot & Simoni, 2011), our attention is drawn to the specific role of femininity among sexual minority women. There is evidence that a feminine (or femme) role is associated with higher levels of internalized homophobia and identity concealment compared with a masculine (or butch) role (Lehavot & Simoni, 2011). Due to their feminine personality and behavior, femme lesbians are likely to “pass” or be perceived as heterosexual women and thus they have greater difficulty resolving negative internalized beliefs about their sexual identity and acknowledging their sexual identity than do butch lesbians (Levitt, Gerrish, & Hiestand, 2003). Although the present research did not test these interpersonal factors but focused more on the gendered and global sense of self, our results were consistent with previous Western research in the sense that they both highlighted the potentially adverse and restrictive role of femininity in lesbians’ affirmation of their self-concepts, which, in turn, hampered their mental health. Future research should continue to examine the effect of femininity on various domains of individual experiences, including interpersonal functioning, among sexual minority people across cultures.
Another interesting finding was that androgyny, rather than masculinity, had the strongest positive direct effect on self-esteem and strongest indirect effect on depression through the mediation of self-esteem compared to the effects of other gender role categories. Masculine traits are generally found to serve as a protective factor for both gay and heterosexual men and women (Carlson & Steuer, 1985; Whitley, 1985). One of the possible explanations is that most Western societies emphasize success and goal attainment and thus highly value stereotypically masculine personality traits, which denote one’s inclination to be assertive and to achieve goals (Whitley, 1985; Wolfram, Mohr, & Borchert, 2009). Also, a recent study found that the positive relationship between masculinity measured via the BSRI and self-esteem had a larger effect size for queer women and men compared to their heterosexual counterparts in the U.S. (Tate et al., 2015). Tate et al. attributed the particularly crucial role of masculinity in queer respondents’ self-esteem to its instrumental role in combating minority stress, which arises from one’s marginalized position as a member of a sexual minority group (Meyer, 2003). These two lines of reasoning may explain why respondents with masculine personality traits had significantly higher levels of self-esteem compared to respondents who were categorized as feminine and undifferentiated as shown by our ANOVA results. In support of our hypotheses, our findings also showed that masculinity had a positive direct effect on self-esteem and an indirect effect on depression through the mediation of self-esteem. The smaller effect sizes of masculinity compared to that of androgyny, however, suggested that androgyny was of greater value to Chinese lesbians’ self-concepts and mental health.
The ways in which gender roles affect mental health outcomes have to be understood in the context of societal gender norms (Bem, 1985; Smagur, Bogat, & Levendosky, 2017). One possible explanation for the greater importance of androgyny compared to masculinity was that the positive effect of masculine personality traits might be offset by the negative effect of the violation of gender norms in the Chinese context. Research has shown that lesbians who do not follow traditional gender roles and adopt a more masculine/butch role are likely to be subjected to harassment and discrimination (Herek, 1995; Levitt & Hiestand, 2004). Given the deep-rooted heteronormative culture in Chinese society in particular (Chow & Cheng, 2010; Kwok & Wu, 2015), sexual minority women are likely to be subjected to not only more stigma and discrimination against their sexual identity but also stronger gender-polarized expectations than their counterparts in many Western countries (Stotzer & Lau, 2013; Zheng et al., 2011). As the reality is still far from Bem’s (1985) hope of a “gender-aschematic” society where gender is no longer a central social category, our findings suggested that androgyny, rather than masculinity, served as the best alternative for Chinese lesbians to organize their lives through the lens of gender scehmas. In practical terms, having personality traits that belong in both social categories of masculinity and femininity would allow them to have a greater repertoire of behavioral responses and coping strategies to fit in or deviate from normative gender expectations in various situations (Bem, 1974; Huang, Zhu, Zheng, Zhang, & Shiomi, 2012; Smagur et al., 2017; Stake, 1997). Also, existing social identification literature has shown that individuals who report having fewer social identities are more likely to develop depression because social identities serve as valuable psychological resources (Jetten, Haslam, Haslam, Dingle, & Jones, 2014; Jones & Jetten, 2011). In other words, it is reasonable to believe that seeing oneself as both masculine and feminine may allow Chinese lesbians to draw on psychological resources when facing challenges, especially in a gender-polarized culture. Thus, androgyny had a stronger protective role in lesbians’ mental health compared to masculinity in our study. Nevertheless, as our explanation based on sociocultural factors remains speculative, further research, particularly qualitative research, is needed to explore the unique meanings and roles of masculinity, femininity, and androgyny among lesbians across cultural contexts, including but not limited to their self-perceptions of gender ideology and the ways in which they perceive their own gender roles in relation to societal gender expectations.
Limitations and Suggestions for Future Research
Several limitations in this study deserve attention. First, given the snowball sampling method, we were unable to determine to what extent our results could be generalizable to the lesbian population in Hong Kong. It is noteworthy that neither census data identifying the Chinese lesbian and gay population nor studies using a random sample of Chinese lesbian and gay people are currently available in the literature due to the fact that sexual minority people remain stigmatized and thus hidden in Hong Kong (Chong, Zhang, Mak, & Pang, 2015; Lo, Chan, & Chan, 2016). Nevertheless, our study represents the first important attempt to focus on Chinese lesbians and investigate the mechanisms through which gender roles influence their mental health.
Second, although this research built on existing theories and empirical studies to test if the established mediation model concerning the relationship between gender roles, self-esteem, and depression could be replicated, our cross-sectional design still limited the ability to make causal arguments regarding the observed relationships among the three variables. For instance, lesbians who were depressed might be more likely to report lower levels of self-esteem than those who were not depressed. Future longitudinal research is needed to test the directionality of the relationships over time.
Third, our novel findings about the predictive pathways of the effects of gender roles on depression among Chinese lesbians were confined to one of the dimensions of gender roles–gender-stereotypical personality traits measured via the BSRI. There has been ongoing debate as to what extent gender roles measured via the BSRI, which focuses on positive aspects of gendered personality traits, actually capture the wide and shifting spectrum of masculine and feminine attributes across cultural and historical contexts (Berger & Krahé, 2013; Donnelly & Twenge, 2017; Tate et al., 2015). While the goal of our study was not to reassess the reliability and validity of the BSRI, we caution that our findings need to be viewed with the potential limitations of the BSRI in mind and call for continued research to improve this widely used instrument. Future research should also continue to examine gender roles manifested in other domains, namely those in body image, intimate relationships, and behaviors, to expand on our model and develop culturally sensitive and effective interventions for the improvement in mental health among sexual minority individuals.
Implications
This study highlights the importance of including different types of gender roles and self-esteem in both theoretical frameworks and interventions aimed at diminishing depression. It shows that self-esteem was an important and necessary factor to which mental health professionals should pay attention so as to reduce Chinese lesbians’ levels of depression. It also indicates that mental health professionals need to be sensitized to different types of gender roles among Chinese lesbians so as to enable them to carry out gender-specific interventions. In particular, mental health professionals should shed traditional gender assumptions and understand the positive effects of androgyny and masculinity on lesbians. They should encourage lesbians to transcend established gender boundaries and not to cling to the conventional gender belief that they ought to be feminine as women.
Conclusion
Our study marks a major step forward in investigating the predictive pathways of the effects of gender roles on depression among Chinese lesbians in Hong Kong. Whereas androgyny and masculinity were associated with decreased levels of depression through the mediation of self-esteem, femininity was associated with increased levels of depression through the mediation of self-esteem. This specific relationship between gender roles, self-esteem, and depression had the largest effect size for respondents with androgynous personality traits, suggesting the particularly important role of androgyny in Chinese lesbians’ mental health. By attending to different gender-typed groups of lesbians and their self-esteem, the present study has provided the lead for developing a more comprehensive and cross-cultural understanding of the complex phenomenon of depression among sexual minority women.
References
Aube, J., Norcliffe, H., Craig, J. A., & Koestner, R. (1995). Gender characteristics and adjustment-related outcomes: Questioning the masculinity model. Personality and Social Psychology Bulletin, 21, 284–295.
Baams, L., Beek, T., Hille, H., Zevenbergen, F. C., & Bos, H. M. (2013). Gender nonconformity, perceived stigmatization, and psychological well-being in Dutch sexual minority youth and young adults: A mediation analysis. Archives of Sexual Behavior, 42, 765–773.
Bailey, J. M., & Zucker, K. J. (1995). Childhood sex-typed behavior and sexual orientation: A conceptual analysis and quantitative review. Developmental Psychology, 31, 43–55.
Balsam, K. F., Beadnell, B., & Molina, Y. (2012). The Daily Heterosexist Experiences Questionnaire: Measuring minority stress among lesbian, gay, bisexual, and transgender adults. Measurement and Evaluation in Counseling and Development, 46, 3–25.
Barrett, A. E., & White, H. R. (2002). Trajectories of gender role orientations in adolescence and early adulthood: A prospective study of the mental health effects of masculinity and femininity. Journal of Health and Social Behavior, 43, 451–468.
Beck, A. T. (1967). Depression: Causes and treatment. Philadelphia: University of Pennsylvania Press.
Bem, S. L. (1974). The measurement of psychological androgyny. Journal of Consulting and Clinical Psychology, 42, 155–162.
Bem, S. L. (1981). Gender schema theory: A cognitive account of sex typing. Psychological Review, 88, 354–364.
Bem, S. L. (1985). Androgyny and gender schema theory: A conceptual and empirical integration. In T. B. Sonderegger (Ed.), Psychology and gender: Nebraska symposium on motivation (pp. 179–226). Lincoln, NE: University of Nebraska Press.
Bem, S. L. (1993). The lenses of gender: Transforming the debate on sexual inequality. New Haven: Yale University Press.
Berger, A., & Krahé, B. (2013). Negative attributes are gendered too: Conceptualizing and measuring positive and negative facets of sex-role identity. European Journal of Social Psychology, 43, 516–531.
Bollen, K. A. (1989). A new incremental fit index for general structural equation models. Sociological Methods & Research, 17, 303–316.
Buckley, T. R., & Carter, R. T. (2005). Black adolescent girls: Do gender role and racial identity impact their self-esteem? Sex Roles, 53, 647–661.
Carlson, H. M., & Steuer, J. (1985). Age, sex-role categorization, and psychological health in American homosexual and heterosexual men and women. Journal of Social Psychology, 125, 203–211.
Chan, Y. F., Leung, D. Y., Fong, D. Y., Leung, C. M., & Lee, A. M. (2010). Psychometric evaluation of the Hospital Anxiety and Depression Scale in a large community sample of adolescents in Hong Kong. Quality of Life Research, 19, 865–873.
Cheung, H. Y. (2006). Factors affecting the state anxiety level of higher education students in Macau: The impact of trait anxiety and self-esteem. Assessment and Evaluation in Higher Education, 31, 709–725.
Choi, H., Kim, J. H., Hwang, M. H., & Heppner, M. J. (2010). Self-esteem as a mediator between instrumentality, gender role conflict and depression in male Korean high school students. Sex Roles, 63, 361–372.
Chong, E. S. K., Zhang, Y., Mak, W. W. S., & Pang, I. H. Y. (2015). Social media as social capital of LGB individuals in Hong Kong: Its relations with group membership, stigma, and mental well-being. American Journal of Community Psychology, 55, 228–238.
Chow, K. Y., & Cheng, S. T. (2010). Shame, internalized heterosexism, lesbian identity and coming out to others: A comparative study of lesbians in Mainland China and Hong Kong. Journal of Counseling Psychology, 57, 92–104.
Collier, K. L., Van Beusekom, G., Bos, H. M., & Sandfort, T. G. (2013). Sexual orientation and gender identity/expression related peer victimization in adolescence: A systematic review of associated psychosocial and health outcomes. Journal of Sex Research, 50, 299–317.
Dean, M. L., & Tate, C. C. (2017). Extending the legacy of Sandra Bem: Psychological androgyny as a touchstone conceptual advance for the study of gender in psychological science. Sex Roles, 76, 643–654.
Donnelly, K., & Twenge, J. M. (2017). Masculine and feminine traits on the Bem Sex-Role Inventory, 1993–2012: A cross-temporal meta-analysis. Sex Roles, 76, 556–565.
Everett, B. G., Talley, A. E., Hughes, T. L., Wilsnack, S. C., & Johnson, T. P. (2016). Sexual identity mobility and depressive symptoms: A longitudinal analysis of moderating factors among sexual minority women. Archives of Sexual Behavior, 45, 1731–1744.
Feather, N. T. (1985). Masculinity, femininity, self-esteem, and subclinical depression. Sex Roles, 12, 491–500.
Gonzalez, C. A., Bockting, W. O., Beckman, L. J., & Durán, R. E. (2012). Agentic and communal personality traits: Their associations with depression and resilience among transgender women. Sex Roles, 67, 528–543.
Hair, J. F., Black, W. C., Babin, B. J., Anderson, R. E., & Tatham, R. L. (2006). Multivariate data analysis (6th ed.). Upper Saddle River, NJ: Pearson Prentice Hall.
Helgeson, V. S. (1994). Relation of agency and communion to well- being: Evidence and potential explanations. Psychological Bulletin, 116, 412–428.
Herek, G. M. (1995). Psychological heterosexism in the United States. In A. R. d’Augelli & C. Patterson (Eds.), Lesbian, gay, and bisexual identities over the lifespan: Psychological perspectives (pp. 321–346). Oxford: Oxford University Press.
Hill, J., & Lynch, M. (1983). The intensification of gender-related role expectations during early adolescence. In J. Brooks-Gunn & A. Petersen (Eds.), Girls at puberty: Biological and psychosocial perspectives (pp. 201–228). New York: Plenum Press.
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6, 1–55.
Huang, X., Zhu, X., Zheng, J., Zhang, L., & Shiomi, K. (2012). Relationships among androgyny, self-esteem, and trait coping style of Chinese university students. Social Behavior and Personality, 40, 1005–1014.
Jetten, J., Haslam, C., Haslam, S. A., Dingle, G., & Jones, J. M. (2014). How groups affect our health and well-being: The path from theory to policy. Social Issues and Policy Review, 8, 103–130.
Jones, J. M., & Jetten, J. (2011). Recovering from strain and enduring pain: Multiple group memberships promote resilience in the face of physical challenges. Social Psychological and Personality Science, 2, 239–244.
Juster, R. P., Pruessner, J. C., Desrochers, A. B., Bourdon, O., Durand, N., Wan, N., & Lupien, S. J. (2016). Sex and gender roles in relation to mental health and allostatic load. Psychosomatic Medicine, 78, 788–804.
Keener, E., & Mehta, C. (2017). Sandra Bem: Revolutionary and generative feminist psychologist. Sex Roles, 76, 525–528.
Kelloway, K. E. (2015). Using Mplus for structural equation modelling (2nd ed.). Thousand Oaks, CA: Sage.
King, M., Semlyen, J., Tai, S. S., Killaspy, H., Osborn, D., Popelyuk, D., & Nazareth, I. (2008). A systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay and bisexual people. BMC Psychiatry, 8, 70. https://doi.org/10.1186/1471-244X-8-70.
Kopper, B. A., & Epperson, D. L. (1996). The experience and expression of anger: Relationships with gender, gender role socialization, depression, and mental health functioning. Journal of Counseling Psychology, 43, 158–165.
Kreiger, T. C., & Dumka, L. E. (2006). The relationships between hypergender, gender, and psychological adjustment. Sex Roles, 54, 777–785.
Kurdek, L. A., & Schmitt, J. P. (1986). Interaction of sex role self-concept with relationship quality and relationship beliefs in married, heterosexual cohabiting, gay, and lesbian couples. Journal of Personality and Social Psychology, 51, 365–370.
Kwok, D. K., & Wu, J. (2015). Chinese attitudes towards sexual minorities in Hong Kong: Implications for mental health. International Review of Psychiatry, 27, 444–454.
Lau, S., & Wong, A. (1992). Value and sex-role orientation of Chinese adolescents. International Journal of Psychology, 27, 3–17.
Lefkowitz, E. S., & Zeldow, P. B. (2006). Masculinity and femininity predict optimal mental health: A belated test of the androgyny hypothesis. Journal of Personality Assessment, 87, 95–101.
Lehavot, K., & Simoni, J. M. (2011). The impact of minority stress on mental health and substance use among sexual minority women. Journal of Consulting and Clinical Psychology, 79, 159–170.
Leung, C., & Moore, S. (2003). Individual and cultural gender roles: A comparison of Anglo-Australians and Chinese in Australia. Current Research in Social Psychology, 8, 21–24.
Leung, S., & Wong, P. (2008). Validity and reliability of Chinese Rosenberg Self-Esteem Scale. New Horizons in Education, 56, 62–69.
Levitt, H. M., Gerrish, E. A., & Hiestand, K. R. (2003). The misunderstood gender: A model of modern femme identity. Sex Roles, 48, 99–113.
Levitt, H. M., & Hiestand, K. R. (2004). A quest for authenticity: Contemporary butch gender. Sex Roles, 50, 605–621.
Li, G., Pollitt, A. M., & Russell, S. T. (2016). Depression and sexual orientation during young adulthood: Diversity among sexual minority subgroups and the role of gender nonconformity. Archives of Sexual Behavior, 45, 697–711.
Lippa, R. A. (2000). Gender-related traits in gay men, lesbian women, and heterosexual men and women: The virtual identity of homosexual–heterosexual diagnosticity and gender diagnosticity. Journal of Personality, 68, 899–926.
Lippa, R. A. (2002). Gender-related traits of heterosexual and homosexual men and women. Archives of Sexual Behavior, 31, 83–98.
Lippa, R. A. (2005). Sexual orientation and personality. Annual Review of Sex Research, 16, 119–153.
Lippa, R. A. (2008). The relation between childhood gender nonconformity and adult masculinity–femininity and anxiety in heterosexual and homosexual men and women. Sex Roles, 59, 684–693.
Lo, I. P. Y., Chan, C. H. Y., & Chan, T. H. Y. (2016). Perceived importance of childbearing and attitudes toward assisted reproductive technology among Chinese lesbians in Hong Kong: Implications for psychological well-being. Fertility and Sterility, 106, 1221–1229.
Lu, L., & Wu, H. L. (1998). Gender-role traits and depression: Self-esteem and control as mediators. Counselling Psychology Quarterly, 11, 95–107.
Marshal, M. P., Dermody, S. S., Cheong, J., Burton, C. M., Friedman, M. S., Aranda, F., & Hughes, T. L. (2013). Trajectories of depressive symptoms and suicidality among heterosexual and sexual minority youth. Journal of Youth and Adolescence, 42, 1243–1256.
Martin, C. L., Cook, R. E., & Andrews, N. C. Z. (2017). Reviving androgyny: A modern day perspective on flexibility of gender identity and behavior. Sex Roles, 76, 592–603.
Martin, C. R., Thompson, D. R., & Chan, D. S. (2004). An examination of the psychometric properties of the Hospital Anxiety and Depression Scale in Chinese patients with acute coronary syndrome. Psychiatry Research, 129, 279–288.
Metalsky, G. I., Joiner, T. E., Hardin, T. S., & Abramson, L. Y. (1993). Depressive reactions to failure in a naturalistic setting: A test of the hopelessness and self-esteem theories of depression. Journal of Abnormal Psychology, 102, 101–109.
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129, 674–697.
Meyer, I. H., & Wilson, P. A. (2009). Sampling lesbian, gay, and bisexual populations. Journal of Counseling Psychology, 56, 23–31.
Mosher, C. E., & Danoff-Burg, S. (2008). Agentic and communal personality traits: Relations to disordered eating behavior, body shape concern, and depressive symptoms. Eating Behaviors, 9, 497–500.
Orth, U., Robins, R. W., & Roberts, B. W. (2008). Low self-esteem prospectively predicts depression in adolescence and young adulthood. Journal of Personality and Social Psychology, 95, 695–708.
Otis, M. D., & Skinner, W. F. (1996). The prevalence of victimization and its effect on mental well-being among lesbian and gay people. Journal of Homosexuality, 30, 93–121.
Plöderl, M., & Tremblay, P. (2015). Mental health of sexual minorities. A systematic review. International Review of Psychiatry, 27, 367–385.
Rieger, G., & Savin-Williams, R. C. (2012). Gender nonconformity, sexual orientation, and psychological well-being. Archives of Sexual Behavior, 41, 611–621.
Roberts, A. L., Rosario, M., Slopen, N., Calzo, J. P., & Austin, S. B. (2013). Childhood gender nonconformity, bullying victimization, and depressive symptoms across adolescence and early adulthood: An 11-year longitudinal study. Journal of the American Academy of Child and Adolescent Psychiatry, 52, 143–152.
Rosario, M., Schrimshaw, E. W., & Hunter, J. (2008). Butch/femme differences in substance use and abuse among young lesbian and bisexual women: Examination and potential explanations. Substance Use and Misuse, 43, 1002–1015.
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton, NJ: Princeton University Press.
Ross, L. E., Salway, T., Tarasoff, L. A., MacKay, J. M., Hawkins, B. W., & Fehr, C. P. (2018). Prevalence of depression and anxiety among bisexual people compared to gay, lesbian, and heterosexual individuals: A systematic review and meta-analysis. Journal of Sex Research, 55, 435–456.
Ryu, E., Seo, J., Ham, M., Park, Y., Moon, S., & Nam, B. (2006). Sex role identity in adolescents and its relation to anxiety, depression and suicidal ideation. Journal of Korean Academy of Psychiatric and Mental Health Nursing, 15, 136–143.
Skoe, E. E. (1995). Sex role orientation and its relationship to the development of identity and moral thought. Scandinavian Journal of Psychology, 36, 235–245.
Smagur, K. E., Bogat, G. A., & Levendosky, A. A. (2017). Gender role and gender as predictors of behavior problems in children exposed to intimate partner violence. Journal of Family Violence, 32, 157–168.
Spence, J. T., & Helmreich, R. L. (1978). Masculinity and femininity: Their psychological dimensions, correlates, and antecedents. Austin: University of Texas Press.
Spence, J. T., & Helmreich, R. L. (1980). Masculine instrumentality and feminine expressiveness: Their relationships with sex role attitudes and behaviors. Psychology of Women Quarterly, 5, 147–163.
Stake, J. E. (1997). Integrating expressiveness and instrumentality in real- life settings: A new perspective on the benefits of androgyny. Sex Roles, 37, 541–564.
Starr, C. R., & Zurbriggen, E. L. (2017). Sandra Bem’s gender schema theory after 34 years: A review of its reach and impact. Sex Roles, 76, 566–578.
Steiger, A. E., Allemand, M., Robins, R. W., & Fend, H. A. (2014). Low and decreasing self-esteem during adolescence predict adult depression two decades later. Journal of Personality and Social Psychology, 106, 325–338.
Stotzer, R. L., & Lau, H. (2013). Sexual orientation-based violence in Hong Kong. Asian-Pacific Law & Policy Journal, 14, 84–107.
Tajfel, H., & Turner, J. C. (1979). An integrative theory of intergroup conflict. In W. G. Austin & S. Worchel (Eds.), The social psychology of intergroup relations (pp. 33–47). Monterey, CA: Brooks-Cole.
Tate, C. C., Bettergarcia, J. N., & Brent, L. M. (2015). Re-assessing the role of gender-related cognitions for self-esteem: The importance of gender typicality for cisgender adults. Sex Roles, 72, 221–236.
Trzesniewski, K. H., Donnellan, M. B., Moffit, T. E., Robins, R. W., Poulton, R. P., & Caspi, A. (2006). Low self-esteem during adolescence predicts poor health, criminal behavior, and limited economic prospects during adulthood. Developmental Psychology, 42, 381–390.
Turner, J. C., Hogg, M. A., Oakes, P. J., Reicher, S. D., & Wetherell, M. S. (1987). Rediscovering the social group: A self-categorization theory. Oxford, England: Blackwell.
Wang, T., & Creedon, C. (1989). Sex role orientations, attributions for achievement, and personal goals of Chinese youth. Sex Roles, 20, 473–486.
Whitley, B. E. (1985). Sex-role orientation and psychological well-being: Two meta-analyses. Sex Roles, 12, 207–225.
Whitley, B. E., & Gridley, B. E. (1993). Sex role orientation, self-esteem, and depression: A latent variables analysis. Personality and Social Psychology Bulletin, 19, 363–369.
Wolfram, H. J., Mohr, G., & Borchert, J. (2009). Gender role self-concept, gender role conflict, and well-being in male primary school teachers. Sex Roles, 60, 114–127.
Wood, W., & Eagly, A. H. (2015). Two traditions of research on gender identity. Sex Roles, 73, 461–473.
World Economic Forum. (2017). The global gender gap report 2017. Retrieved December 1, 2018, from http://www3.weforum.org/docs/WEF_GGGR_2017.pdf.
Yu, L., & Xie, D. (2008). The relationship between desirable and undesirable gender role traits, and their implications for psychological well-being in Chinese culture. Personality and Individual Differences, 44, 1517–1527.
Zhang, J., Norvilitis, J., & Jin, S. (2001). Measuring gender orientation with the Bem Sex Role Inventory in Chinese culture. Sex Roles, 44, 237–251.
Zheng, L., Lippa, R. A., & Zheng, Y. (2011). Sex and sexual orientation differences in personality in China. Archives of Sexual Behavior, 40, 533–541.
Zigmond, A. S., & Snaith, R. P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67, 361–370.
Acknowledgements
This study was funded by the Research Committee of the University of Hong Kong (Grant Number: 201409176248).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lo, I.P.Y., Kim, Y.K., Small, E. et al. The Gendered Self of Chinese Lesbians: Self-Esteem as a Mediator Between Gender Roles and Depression. Arch Sex Behav 48, 1543–1554 (2019). https://doi.org/10.1007/s10508-019-1402-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10508-019-1402-0