
Abstract
Sexual minority identity (bisexual, lesbian) is a known risk factor for depression in women. This study examined a facet of minority stress prevalent among women—sexual identity mobility—as an identity-related contributor to higher levels of depressive symptoms. We used three waves of data from the Chicago Health and Life Experiences of Women study, a longitudinal study of sexual minority women (N = 306). Random effects OLS regression models were constructed to examine the effect of sexual identity changes on depressive symptoms. We found that 25.6 % of the sample reported a sexual identity change between Wave I and Wave II, and 24.9 % reported a sexual identity change between Waves II and III. Women who reported a change in sexual identity also reported more depressive symptoms subsequent to identity change. This effect was moderated by the number of years participants had reported their baseline identity and by whether the participant had initiated a romantic relationship with a male partner.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Previous research has documented that sexual minority-identified (e.g., lesbian, bisexual, and mostly heterosexual) women report higher rates of depressive disorders compared to heterosexual women (Bostwick, 2012; Cochran, Greer, & Mays, 2003; Diamant & Wold, 2003; Marshal et al., 2011). Minority stress theory posits that disparities in mental health among sexual minorities are due to exposure to stigma-related stressors (Hatzenbuehler, Phelan, & Link, 2013; Meyer, 1995, 2003). Sources of sexual minority stress include victimization, discrimination, and negative feelings regarding one’s own sexual orientation (i.e., internalized homophobia) (Burgess, Tran, Lee, & van Ryn, 2007; Feinstein, Goldfried, & Davila, 2012; Hatzenbuehler, McLaughlin, Keyes, & Hasin, 2010; Herek, Gillis, & Cogan, 1999). Studies have shown that, among sexual minorities, these sources of stress are associated with poorer mental health outcomes; however, sexual orientation disparities in mental health often persist even after adjusting for these factors (Burton, Marshal, Chisolm, Sucato, & Friedman, 2013; Marshal et al., 2011; Matthews, Hughes, Johnson, Razzano, & Cassidy, 2002; McLaughlin, Hatzenbuehler, Xuan, & Conron, 2012; Russell & Joyner, 2001).
This study focuses on an understudied aspect of minority stress prevalent among women—sexual identity mobility—as a potentially important factor that contributes to depressive symptoms. Sexual identity mobility is defined as “changes in self-reported sexual orientation” (Ott, Corliss, Wypij, Rosario, & Austin, 2011, p. 520), which includes changes to a more same-gender/sex-oriented identity or to a less same-gender/sex-oriented identity.Footnote 1 Changes in sexual identity appear to be much more common among women than among men (Everett, 2015; Mock & Eibach, 2012; Ott et al., 2011; Savin-Williams, Joyner, & Rieger, 2012), and women are more likely than men to report changes in their sexual identity later in life (Calzo, Antonucci, Mays, & Cochran, 2011).
Although previous research has examined mental health outcomes following identity disclosure or “coming-out” among sexual minorities (Chaudoir & Fisher, 2010; Maguen, Floyd, Bakeman, & Armistead, 2002), fewer studies have examined the impact of sexual identity mobility on sexual minority women’s mental health. Further, extant research investigating the relationship between identity mobility and mental health has relied almost exclusively on samples of adolescents and young adults; thus results may not be generalizable to individuals in other life stages (Everett, 2015; Needham, 2012).
Although not uncommon among women (Diamond, 2000, 2008), sexual identity mobility that is reported in middle and older adulthood falls outside normative expectations for when sexual identity development is typically reported to occur, i.e., in adolescence or young adulthood (Floyd & Bakeman, 2006; Rosario, Hunter, Maguen, Gwadz, & Smith, 2001; Valentine, Skelton, & Butler, 2003). Changes outside the expected period of sexual orientation development may therefore have a greater impact on women’s mental health. Sexual identity changes in adulthood may be further complicated by longer periods of identifying with a baseline identity and higher levels of identity disclosure to friends and family members, making such changes more psychologically distressing. This study addresses an important gap in the literature by examining the impact of sexual identity mobility on depressive symptoms using a longitudinal sample of adult sexual minority women. Moreover, we examine whether the impact of identity change varies according to other important identity-related characteristics, including the number of years spent identifying with the most recent baseline sexual identity, level of identity disclosure to family members, and initiation of romantic relationships with male and female partners.
Sexual Identity Development
Early theories of sexual identity development, largely put forth in the 1980s, suggested that sexual orientation development is a linear process whereby individuals become aware of their same-gender/sex attraction in early adolescence, begin to engage in same-gender/sex romantic and sexual relationships, and eventually come to identify with a lesbian identity in early adulthood (Cass, 1979; Coleman, 1982; Troiden, 1988). These theories characterize transition periods that involve identity change as being particularly distressing, given that individuals may experience high levels of cognitive dissonance (e.g., the stress associated with incongruence between identity and behavior) before they self-ascribed a lesbian identity. Increasingly, however, researchers (Diamond, 2007; Savin-Williams et al., 2012) have criticized these early models on a number of grounds. For example, early-stage process models do not account for high levels of documented sexual fluidity across the life course (see e.g., Diamond, 2008). In addition, the models do not account for subsequent changes toward more heterosexually oriented identities.
Stage process models also do not adequately account for bisexual identity development among persons who maintain attractions to both men and women over time as an end-stage identity. Traditional stage-based models largely ignore women who do not identify as exclusively heterosexual or exclusively lesbian. Indeed, bisexual women’s sexuality is often seen as invalid or temporary. As such bisexual women often face high levels of stigma and exclusion, not only from heterosexual populations but also from gay and lesbian populations and organizations—factors that are believed to be linked to bisexual women’s poorer mental health profiles (Mulick & Wright, 2002). More recently researchers have articulated the need for recognizing bisexual women as a distinct sexual minority group, separate from lesbians—not only because of the large number of women who identify with these labels, but also because a growing body of research has shown that bisexual and mostly heterosexual women report higher rates of risk behaviors and poorer mental health (Bostwick, Boyd, Hughes, & McCabe, 2010; Cochran & Mays, 2009; Fredriksen-Goldsen, Hyun-Jun, Barkan, Balsam, & Mincer, 2010; Hughes, Wilsnack, & Kristjanson, 2015; McCabe, Hughes, & Boyd, 2004).
In response to limitations of stage process models, new theories of sexual orientation development have been proposed which emphasize that personal experiences and the social environment influence the timing and pattern of an individual’s sexual identity development (Horowitz & Newcomb, 2002; Rosario, Schrimshaw, & Hunter, 2008; Savin-Williams, 2011). For example, in outlining Sexual Configurations Theory, van Anders (2015) argues that sexuality scholars should adopt a “fundamentally dynamic perspective where change is central rather than peripheral, irrelevant, or aberrant” (p. 1179). Additionally, Diamond’s (2003) bio-behavioral model of sexual orientation emphasizes that sexual orientation is not only based solely on sexual desire, but also on romantic desire; individuals may develop romantic feelings for persons whose gender/sex is congruent or incongruent with their sexual orientation identity. This is particularly true of women, who show greater flexibility in their sexual and emotional responses (Chivers, Rieger, Latty, & Bailey, 2004) and are more likely than men to form romantic relationships with friends (Diamond, 2003). For women, high levels of sexual identity mobility may be linked to changes in romantic relationships and the gender/sex of their partners rather than to changes in sexual attraction or desire.
Identity Change and Mental Health
Identity theory emphasizes the importance of internal and external alignment in identity standards, which are defined by the set of meanings attached to an identity and an individual’s perceptions of how they are performing an identity (Burke, 1980, 1991; Burke & Tully, 1977; Stryker & Burke, 2000). Social identities and their corresponding identity standards are known before individuals self-ascribed them and are often adopted by persons as a strategy to validate their internal evaluation of whom they perceive themselves to be. Performing up to the standards of one’s in-group allows an individual to feel validated as a “good” group member. Additionally, social identities are an important organizing feature of social life: they connect individuals to other individuals, help them to identify support networks, and validate in-group norms (Haslam, Jetten, Postmes, & Haslam, 2008). The validation of in-group norms is of particular importance for marginalized groups such as sexual minorities, who are often confronted with external sources of stigma and discrimination that may threaten their identities (Mossakowski, 2003; Ramirez-Valles, Kuhns, Campbell, & Diaz, 2010; Rosario, Schrimshaw, Hunter, & Braun, 2006). Important for the current work, misalignments between the external identity standard and individuals’ internal evaluations of their performance of the identity are believed to result in psychological distress (Burke, 2006).
Identity control theory (Burke, 2006) suggests that changes in identity are often precipitated by high levels of cognitive dissonance between an identity standard and an individual’s internal evaluation of how they are performing relative to that standard. Periods of heightened dissonance are hypothesized to be associated with psychological distress. As a result, individuals who are unable or unwilling to maintain identity standards may decide to redefine their identity to reduce dissonance and psychological distress. Although in the long-term these changes may improve an individual’s mental health, in the short-term, such identity changes are associated with cognitive and emotional disruptions as individuals attempt to navigate the reconfiguration of self-relevant schemas and related social support networks. Previous research has shown that, in general, changes in identity status are associated with poorer mental health outcomes compared to individuals who maintain stable identities (Bonanno, Papa, & O’Neill, 2001; Haslam et al., 2008; Iyer & Jetten, 2011).
According to social identity theory (Tajfel & Turner, 1979, 2004), the impact of identity changes on mental health may be dependent upon the amount of time an individual has identified in a particular way, as well as the extent to which an individual has externally committed to that identity. Although the extant literature suggests that identity commitments and stability are generally protective (Iyer, Jetten, Tsivrikos, Postmes, & Haslam, 2009; Schnittker & McLeod, 2005; Sellers, Caldwell, Schmeelk-Cone, & Zimmerman, 2003; Sellers, Copeland-Linder, Martin, & Lewis, 2006), the longer individuals have spent committed to a particular identity, the more disruptive an identity transition may be. Identity transitions from long-held identity commitments are likely to involve more extensive reconfigurations of self-relevant schemas. Moreover, individuals who report higher levels of external identity commitment may find that identity transitions are met with higher levels of rejection from in-group members. Social rejection resulting in a loss of social support may also precipitate reconfigurations related to a sense of self. Social rejection in and of itself is known to contribute to psychosocial distress (e.g., Twenge, Catanese, & Baumeister, 2003).
Identity Change and Sexual Orientation
For sexual minority women, the stress associated with changes in identity may be exacerbated by the unique social position of lesbian and bisexual women in the larger social structure. For sexual minorities, sexual orientation often develops within a larger heterosexist and homophobic cultural context (Hatzenbuehler et al., 2013). In addition, sexual minority women are often vulnerable to additional risk exposures (e.g., victimization) pertinent for psychological functioning that have been shown to influence the timing and pattern of sexual identity development (Rosario et al., 2008). Moreover, changes in sexual identity may be met with rejection from peers, friends, and/or family members, regardless of whether the change is toward a more same-gender/sex-oriented identity (D’Augelli, Hershberger, & Pilkington, 1998; Floyd & Bakeman, 2006) or a less same-gender/sex-oriented identity (Diamond, 2003; Tabatabai & Linders, 2011). To be sure, sexual minorities as a group continue to face high levels of stigma and discrimination and yet persist in demanding social recognition and legitimization of their identities and relationships. Because of that demand, transitioning from a more same-sex-oriented identity toward a more opposite-gender/sex one may be viewed as reinforcing negative stereotypes about sexual minorities and resulted in social rejection from both in-group peers and out-group members. Formerly bisexual and lesbian-identified women who reported changes in identity toward less same-sex-oriented identities indicated stress related to the perception that their identity change was validating negative stereotypes that their same-gender/sex sexuality was “just a phase” (Diamond, 2003; Tabatabai & Linders, 2011). Thus, although changes toward less same-gender/sex-oriented identities may result in fewer instances of discrimination and stigma from out-group members (i.e., heterosexuals), such changes may be associated with increased rejection from sexual minority in-group peers, particularly for individuals who have identified as sexual minority for extended periods of time and/or those with high levels of external identity commitment to their long-held sexual minority identity.
The motivations for changes in sexual identity have been hard to characterize (Diamond, 2008); however, one possible predictor may be changes in relationship status. Identity theory acknowledges that although individuals maintain multiple identities, each with different degrees of salience at any given time, interactions with one’s primary social network are a motivator of identity stability versus change (Stryker & Serpe, 1982). Moreover, changes in social networks can sometimes be catalysts of identity change (McFarland & Pals, 2005). Specifically, change in the gender/sex of an individual’s romantic partner may be a strong predictor of sexual identity mobility because such a change is motivated by the desire to reduce cognitive dissonance. Because changes in the gender/sex of relationship partners are readily observable, it may be that such changes are more likely to spur identity changes than are variations in covert aspects of sexual orientation, such as the gender/sex of persons to which an individual is typically attracted. By reducing cognitive dissonance, these changes therefore may be protective and work to improve mental health, rather than detrimental. Regardless, self-ascribed changes in sexual identity may be ultimately protective for cognitive consistency and facilitate improved mental health.
Regardless of the precipitating factors influencing change, transitions in sexual identity may impact mental health, either via a temporary cognitive interruption and subsequent adjustment period or via a potentially longer-lasting and more damaging major loss in social support. The effect of identity change on mental health functioning, however, may differ depending on the amount of time spent identifying as a sexual minority member and the level of external commitment to that identity. Therefore, based on prior research and theory, we posit that the greater the time spent identifying as a sexual minority, the higher the levels of external commitment to a sexual minority identity will be, resulting in greater psychological distress if a change is reported. One important indicator of external commitment is sexual orientation disclosure to friends and family. Disclosure is seen as a vital step in minority sexual identity integration (Floyd & Bakeman, 2006; Floyd & Stein, 2002; Maguen et al., 2002). Disclosure, in particular to family members, may be considered an important marker of external identity commitment due to the documented risks of rejection when informing family members of one’s lesbian or bisexual identity (Corrigan & Matthews, 2003; D’Augelli & Grossman, 2001; D’Augelli et al., 1998). Thus, when changes are toward less same-gender/sex-oriented identities, sexual minority persons who have disclosed their sexual identity to many people may experience greater psychological distress. For individuals who report changes toward more same-gender/sex-oriented identities, higher levels of disclosure may be protective and ease the transition to an exclusively or mostly lesbian identity.
To date, research that has examined the relationship between sexual identity mobility and psychological distress has focused entirely on the developmental period of adolescence and emerging adulthood. For example, in a longitudinal study of attraction trajectories in adolescence, Needham (2012) found that girls who reported stable bisexual/lesbian attractions and those that transitioned to bisexual/lesbian attractions had higher levels of depressive symptoms at baseline than girls who reported stable heterosexual attractions, but that these differences did not increase over time. By contrast, no differences were found between stable heterosexual and lesbian/bisexual-attracted girls who transitioned to heterosexual attraction (Needham, 2012). Rosario, Schrimshaw, and Hunter (2011), however, found that variations in adolescent sexual identity development were ultimately unrelated to reports of depressive symptoms, anxiety, or self-esteem. Nevertheless, changes toward greater identity integration were associated with better psychological adjustment and youth who consistently reported high levels of identity integration reported lower corresponding levels of psychological distress (Rosario et al., 2011). Finally, a recent study of identity change in emerging adulthood (Everett, 2015) found that, during the transition from adolescence-to-young adulthood, changes toward more same-sex-oriented identities were linked to higher levels of depressive symptoms, but that there were no negative effects for identity shifts toward less same-gender/sex-oriented identities.
To our knowledge, no research has examined the effects of identity mobility among adult sexual minority women. This gap in the literature is particularly problematic given that identity shifts that occur outside of adolescence or young adulthood violate normative expectations for the development of sexual orientation and thus may be particularly distressing. The longitudinal data used in the study affords a unique opportunity to examine the impact of other important identity-related characteristics (e.g., identity commitment, disclosure, and relationship status) on the expected association between sexual identity mobility and depressive symptoms. Given the high likelihood of identity changes over the life course among sexual minority women, understanding relations among identity transitions and mental health outcomes may yield important insights into transition periods of greater risk for poorer mental health. Using data from the Chicago Health and Life Experiences of Women (CHLEW) longitudinal study of adult sexual minority women, this study investigated the relationship between sexual identity mobility and psychological distress using depressive symptoms as the mental health indicator. We tested the following hypotheses: (1) Adult sexual minority women who report sexual identity mobility, regardless of the direction of change, will report higher subsequent levels of depressive symptoms; (2) The negative effect of change toward more same-gender/sex-oriented identities will be weaker among women with higher levels of external identity commitment, measured via sexual identity disclosure, whereas negative effects of change toward less same-gender/sex-oriented identities will be stronger among women with higher external identity commitment; (3) Women will report greater psychological distress as a result of identity change as the number of years they identified with their previous sexual identity increases; and (4) Sexual minority women reporting a recent identity change and a new romantic relationship with a male partner will report greater psychological distress than women who report a recent identity change and a new romantic relationship with a female partner.
Method
Participants
The CHLEW is a 3-wave 10-year longitudinal study of adult sexual minority women. Data collection began in the greater Chicago metropolitan area in 2000, using a broad range of recruitment sources and strategies to enroll a diverse sample of 447 English-speaking women, ages 18 and older, who self-identified as lesbian (exclusively or mostly) at baseline. Extensive efforts were made to maximize CHLEW sample representativeness by including subgroups of lesbians underrepresented in most studies of lesbian health (i.e., aged under 25 and over 50, high school education or less, racial/ethnic minority). The study was advertised in local newspapers, on Internet listservs, and on flyers posted in churches and bookstores; information about the study was also distributed to individuals and organizations via formal and informal social events and social networks. Other recruitment sources included clusters of social networks (e.g., formal community-based organizations and informal community social groups) and individual social networks, including those of women who participated in the study. Interested women were invited to call the project office to complete a short telephone interview. Participants who reported being heterosexual, mostly heterosexual, bisexual, or transgender at Wave I were not eligible to participate. Although bisexual women were screened out in the telephone interview, a small minority of the sample self-identified as bisexual in subsequent baseline interviews. The baseline sample included women ages 18–82 years; less than one-half of the baseline sample was white. The CHLEW Wave II survey (2004–2005) had a response rate of 86 %, and the Wave III survey (2011–2012) a response rate of 79 %. The current sample was restricted to women who were interviewed at all three waves of data collection and did not have missing data on key variables. The final sample size was 306 participants.
Measures
Sexual Identity Mobility
A measure of sexual identity mobility was created using responses to the sexual orientation question in the three waves of data. At each assessment, participants were asked whether they identify as “exclusively heterosexual, mostly heterosexual, bisexual, mostly lesbian, or exclusively lesbian.” Responses were used to construct three dichotomous variables that captured whether participants reported change toward (a) a more same-gender/sex-oriented identity between Waves I and II; (b) a less same-gender/sex-oriented identity between Waves I and II; or (c) a stable identity across Waves I and II (referent). A similar variable was created for changes between Waves II and III: participants were coded as reporting change toward (a) a more same-gender/sex-oriented identity between Waves II and III, (b) a less same-gender/sex-oriented identity between Waves II and III, or (c) a stable identity between Waves II and III (referent).
Dependent Variables
Questions about depressive symptoms were asked of participants at all three waves of the survey. The questions were from the Major Depressive Episode section of the National Institute of Mental Health Diagnostic Interview Schedule (Robins, Helzer, Croughan, & Ratcliff, 1981). The questions asked “Since your last interview, have there been two weeks or more during which you (1) felt sad, blue, depressed, or when you lost all interest and pleasure in things you usually cared about; (2) you lost your appetite, whether or not you continued to eat the same amount of food; (3) you lost weight without trying—as much as two pounds a week for several weeks, or as much as ten pounds or more altogether; (4) you gained as much as two pounds a week for several weeks, or ten pounds or more altogether; (5) when nearly every night you had trouble with sleeping: waking up too early, or sleeping too much, not staying asleep, or trouble falling asleep; (6) when you felt tired all the time even when you had not been working very hard; (7) when nearly every day you had to be moving all the time; that is, you couldn’t sit still, and paced up and down; (8) when you talked or moved more slowly than is normal for you; (9) when your interest in sex was a lot less than usual; (10) when you felt worthless, sinful, or guilty; (11) when nearly every day your thoughts came much slowly than usual or seemed mixed up, or you had a lot more trouble concentrating than is usual for you?” Participants responded “yes” or “no” to each question, and “yes” responses were summed into a scale that ranged from 0 to 11. Cronbach’s alpha for this scale ranged from .82 to .85 across waves of data collection.
We also created a dichotomous measure following clinical guidelines for major depressive episode in the DSM-5 (American Psychiatric Association, 2013). Participants who met the criteria reported (1) at least five depressive symptoms in a two-week period; (2) one of these indicators was having felt sad, blue, depressed, or having lost interest in things they usually cared about; and (3) these symptoms interfered with the participant’s daily life. Participants who met the criteria were coded as 1 and those who did not were coded as 0.
Moderating Variables
We examined the effect of several moderating variables to assess whether the effect of identity mobility varied by levels of external commitment (number of people to whom the participant had disclosed their identity), age, number of years the participant’s baseline identity was maintained, and change in the reported gender/sex of relationship partners.
The number of years participants had maintained their most recent reported sexual identity (at baseline) was included for both the Wave I-to-II and Wave II-to-III sub-samples. At Wave I, this measure was created using a survey item that asked, “How old were you when you first identified as [identity reported at time of interview]?” Participants’ responses were subtracted from their age at Wave I; years ranged from 0 to 53. At Wave II, this variable was created from a survey item that asked participants, “How long have you identified as [reported identity at time of interview]?” The range at Wave 2 was 0 to 58 years. Variables were then mean centered; the resulting range was from −23.42 to 36.94.
Sexual orientation disclosure to family members was measured at Waves I and II using a series of questions that asked participants to report whether their mother (living or not living) knew that they were lesbian/mostly lesbian/bisexual and whether their father (living or not living) knew that they were lesbian/mostly lesbian/bisexual. Participants were also asked how many siblings they had and the number who knew that they were lesbian/mostly lesbian/bisexual. Because family size varied among participants, this item was coded as the total proportion of family members to whom the participant had disclosed their identity and ranged from 0 to 1. This variable was then mean centered and ranged from −.75 to .24.
Initiating a romantic relationship with a man or woman was measured using responses to a series of questions that asked, “Since the time of the last interview, have you experienced a change in your relationship status?” Participants were coded as initiating a new romantic relationship if they reported that since the last interview they began “living with a partner in a committed relationship that lasted at least one year” or were in a “committed relationship that had lasted at least one year, but not living with partner.” Participants were also asked to identify the gender/sex of the committed relationship partner. Two dummy variables were created, one that captured whether a participant initiated a relationship with a woman between study waves and another that indicated if a participant initiated a relationship with a man between study waves.
Controls
We controlled for sexual orientation identity at Wave I. Because participants were recruited into the study based on minority sexual identity, all participants in the current analyses identified as exclusively gay/lesbian, mostly gay/lesbian, or bisexual (referent) at baseline. We controlled for age at Wave 1 of the survey, which ranged from 18 to 82 years. Race/ethnicity was coded as a series of dummy variables to indicate whether participants’ self-reported race/ethnicity was white (referent), black, Latina, or something else. Education was coded as a series of dummy variables that captured whether participants reported their highest level of education was a high school degree or less, some college, or a college degree or greater (referent). We also controlled for cohabitation status at Waves I and II using a series of dummy variables that captured whether participants were single, in a non-cohabiting committed relationship, or in a cohabiting relationship (referent).
Analytic Plan
First, we present descriptive statistics for the overall sample. Second we present descriptive information for our measures of psychological distress separately for participants whose sexual orientation identity remained stable and, alternatively, those whose identity changed over time (sexual identity mobility).
Third, we used multi-level, random effects OLS regression models to examine the association between identity change and depressive symptoms. To account for non-independence of error terms, waves of data collection were nested within individuals. Because the independent variable captures change in identity status between waves, despite collecting three waves of data, there are only two time points at which the independent variable (identity change) is observed. To ensure the correct time-ordering effects, all baseline moderating variables and covariates were time-lagged to predict subsequent levels of depressive symptoms at the following wave. As a result, although there are three waves of data, only two data points were used in the models, resulting in 612 observations across 306 participants. Furthermore, although measured longitudinally, only depressive symptoms from Waves II and III were used in the model; thus, we adjust for depressive symptoms reported at Wave I. All models were analyzed using the “XT” commands in Stata 14.0.
We used a model-building strategy to assess the influence of sexual identity mobility on depressive symptoms. In Model 1, we included measures of identity mobility and prior reports of depressive symptoms (i.e., at baseline) to examine subsequent levels of depressive symptoms. Model 2 adjusted for age, race/ethnicity, education, and baseline sexual orientation identity. Model 3 included variables reflecting disclosure to family members, number of years baseline identity was maintained, and changes in gender/sex of committed partners. To examine whether the effect of identity mobility on depressive symptoms varied by number of years in baseline identity in Model 4, we examined interactions between identity-change status and the number of years participants had identified with their baseline sexual identity. In Model 5, we examined interactions between identity-change status and the proportion of family members to whom the participant had disclosed their baseline identity. Finally, Model 6 examined whether initiating a new romantic relationship with a male partner moderated the effect of identity-change status when compared to not having initiated a relationship with a male.
Finally, we present the predicted probabilities from lagged, random-effect logistic regression models for major depressive episode clinical cutoffs using the “XTlogit” and “Margins” commands in Stata 14. Predicted probabilities are derived from two models. The first model includes all simple associations, including sociodemographic characteristics, sexual identity mobility indicators, prior depressive symptoms, number of years with most recent self-ascribed sexual identity, disclosure to family members, and changes in the gender/sex of relationship partners. The second model presents predicted probabilities by sexual identity mobility status and number of years with baseline self-ascribed sexual identity, adjusting for all other covariates in the first model.Footnote 2
Results
Table 1 presents descriptive statistics for the analytic sample. Between Wave I and II, 12 % of participants reported a change toward a more same-gender/sex-oriented identity and 13 % of participants reported a change toward a less same-gender/sex-oriented identity. In contrast, from Wave II to Wave III, just 7 % of participants reported a more same-gender/sex-oriented identity and 18 % reported a less same-gender/sex-oriented identity. The percent of exclusively lesbian-identified participants was 70 % at both waves. On average, participants reported that they had disclosed their sexual identity to 75 % of their family at Wave I and 80 % at Wave III. On average, participants indicated that they had identified with the sexual identity reported at Wave I for 16 years, and with the identity reported at Wave II for the previous 18 years.
Between Waves I and II and Waves II and III, respectively, the percentage of women who began a new relationship with a male partner was much smaller than those who began a new relationship with a female partner: compared to 34 and 40 % of women who began a relationship with a woman, 5 and 7 % of women began a relationship with a man between Waves I and II and between Waves II and III, respectively.
Table 2 presents mean scores for depressive symptoms and the percent of participants who met criteria for a major depressive episode according to their sexual identity mobility status. Women who reported changes toward more same-sex-oriented identities reported significantly higher levels of depressive symptoms (M = 5.54) than women who reported a stable sexual identity (M = 4.51, p < .05). By contrast, women who reported changes toward less same-sex-oriented identities reported levels of depressive symptoms (M = 5.21) that were not statistically different from either other sexual identity mobility group. Forty percent of the women in the sample who reported a stable sexual identity over time met the clinical cutoff for a major depressive episode, compared to about 51 % of women who reported a shift toward more same-sex-oriented identities and about 54 % of women who reported less same-sex-oriented identities. Thus, both groups of women who reported changes in their sexual identity were at greater risk of reporting a major depressive episode than those who reported a stable sexual identity.
Differences in Depressive Symptoms by Sexual identity Mobility
Table 3 presents coefficients for sexual identity mobility and other covariates derived from OLS regressions for prospective associations with depressive symptomatology.
Results from Model 1 show that changes toward more (B = 0.76, p < .05) same-sex-oriented identities were associated with a greater number of depressive symptoms in subsequent waves. This finding holds and in fact, becomes stronger (B = 0.98, p < .05) after adjustments for other sociodemographic characteristics are included in Model 2. Model 3 includes sociodemographic characteristics and adjusts for other measures (the number of years the participant identified with the baseline identity, disclosure to family members, and change in gender/sex of partner). These additional measures were not significantly related to depressive symptoms in Model 3. Participants who reported shifts toward more same-gender/sex-oriented identities report more depressive symptoms compared to those with stable identities (B = 0.95, p < .05)
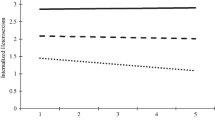
Models 4–6 tested interaction hypotheses. Model 4 includes all previous covariates and an interaction between the number of years that participants identified with their baseline identity and identity-mobility status. These results show that as the number of years a woman spent identifying with her baseline identity increased the more punitive the identity change was for mental health (see Fig. 1). The results, in Model 5, that tested an interaction between identity change status and the number of family members to whom a participant disclosed their sexual identity was not significant.

Predicted depressive symptoms by years identified
Model 6 included an interaction between identity-mobility status and initiating a romantic relationship with a male partner. Findings show that shifts towards more same-gender/sex-oriented identities were associated with an increase in depressive symptoms (B = 1.05, p < .05). For women who reported changes toward a less same-gender/sex-oriented identity, initiating a new relationship with a male partner was not associated with similar risk for an increase in depressive symptoms (B = 0.57 + 0.21 − 2.74). Rather, these participants showed an overall reduction of depressive symptoms (see Fig. 2). There were no women who reported a more same-gender/sex-oriented identity and had initiated a relationship with a male between waves.

Depressive symptoms by relationship status
Table 4 presents predicted probabilities for scoring above the major depressive disorder cutoff based on identity-mobility status and years spent identifying with most recent identity. The results showed that as the number of years increased for persons who did not report changes in sexual identity, the probability of experiencing a major depressive disorder actually decreased. For example, women who reported having identified with their baseline identity for 0–4 years had a 48.5 % chance of exceeding cutoffs indicating a subsequent depressive episode, compared with 42.2 % for women who had identified for 15–19 years, and 34.1 % for women who had identified for 35 or more years.
In direct contrast, among women who reported any change in sexual identity, the longer they had reported identifying with their most recent sexual identity, the higher their likelihood of meeting criteria for a major depressive episode subsequent to that change. For example, women who reported changes to more same-sex-oriented identities yet had only self-ascribed their baseline sexual identity for 0–4 years, had a 40.3 % probability of meeting criteria for a major depressive episode, compared to a 61.2 % probability for women who reported changes to more same-sex-oriented identities yet had self-ascribed their baseline identity for 35 or more years. Similarly, women who reported changes to less same-sex-oriented identities, yet had only identified with their baseline sexual identity for 0–4 years, had a 42.1 % probability of meeting criteria for a depressive episode, compared to a 59.8 % probability for women who reported changes to less same-sex-oriented identities yet had self-ascribed their most recent sexual identity for 35 or more years.
Discussion
These results provide new insights into an understudied contributor to adult sexual minority women’s mental health. In our sample, it was relatively common for adult sexual minority women to report a change in sexual identity over time: 25 % of the sample reported a change in identity between Waves I and II; similarly, 25 % of the sample reported a change in identity between Waves II and III. This finding is consistent with other research indicating that sexual identity change may be relatively common, especially among women (Diamond, 2000; Mock & Eibach, 2012; Ott et al., 2011; Savin-Williams et al., 2012). Unfortunately, studies and narratives that have documented sexual fluidity in women’s lives have included little information about the consequences of sexual fluidity for women’s health and well-being.
Extant research has focused almost exclusively on adolescent and young adult populations and has provided mixed results on the relationship between sexual fluidity and mental health: some studies have suggested no difference in the mental health outcomes of individuals who have reported changes in attraction (Needham, 2012), whereas others have shown that only shifts toward same-gender/sex-oriented identities were linked to depressive symptoms (Everett, 2015). Our results are consistent with the finding from Everett (2015) that shifts toward more same-gender/sex-oriented identities were associated with higher levels of depressive symptoms. Importantly, however, we extend previous research by showing that in some contexts, adult sexual minority women who shift toward less same-gender/sex-oriented identities are also at risk for elevated depressive symptoms and depressive episodes (i.e., based on years spent self-ascribing a particular sexual identity).
Findings of the present study suggest that the effect of sexual identity mobility on depressive symptoms is dependent on at least two key identity-relevant characteristics: number of years an identity is maintained and initiation of a committed relationship with an opposite-gender/sex partner. Indeed, the negative effects of identity change are concentrated among women who had maintained their identity for many years. This is true for both women who report changes toward more same-gender/sex-oriented identities and those who report changes toward less same-gender/sex-oriented identities. We argue that the presumption that sexual identity is an intrinsic, stable, and binary quality, which persists in the larger society (in both heterosexual and gay/lesbian populations), may be an egregious contributor to mental health problems among women who report attractions to or engage in behaviors with both men and women as well as among those who report changes in their sexual identity over time. This interpretation is supported by qualitative research findings that lesbian and bisexual women whose sexual identity changes in the direction of less same-gender/sex-oriented identities often face criticism from both heterosexual and gay communities (Diamond, 2003; Tabatabai & Linders, 2011). Such women expressed concerns about fulfilling heterosexist stereotypes about lesbians (e.g., that they were not really lesbian or bisexual, or that their same-gender/sex sexuality was “just a phase”). Further, new results from Katz-Wise and Hyde (2014) show that women who are sexually fluid are more likely to have positive attitudes about bisexuality and sexual fluidity as a process, compared with women who do not report fluidity (see also Parent, Talley, Schwartz, & Hancock, 2015). Efforts to reduce stigma surrounding sexual fluidity and identity change in the lives of women may be an important step in eliminating or reducing mental health disparities based on sexual orientation.
The current findings that any change in identity status was associated with risk of psychological distress stands in contrast to the recent study using the National Longitudinal Study of Adolescent to Adult Health by Everett (2015) which found that only shifts toward more same-gender/sex-oriented identities were associated with depressive symptoms. The mean age of this sample was 28.77 at the follow-up period. These contrasting findings may be explained by differences in age between the CHLEW sample and Everett’s (2015) study samples. The mean age of the CHLEW sample was 38 years at Wave I and 48 years at Wave III. Thus, sexual identity transitions reported in this current study necessarily occurred after adolescence, a developmental period in which a certain amount of fluidity and/or stress is expected during sexual identity development (Floyd & Bakeman, 2006; Rosario et al., 2001; Valentine et al., 2003). Similar to other research on sexual fluidity among samples of adult sexual minority women (Diamond, 2000, 2008), we observed that a substantial proportion of sexual minority women in our sample reported sexual identity changes well into adulthood.
In addition to the sample age differences, Everett’s (2015) study sample did not assess length of time participants had maintained their baseline identity. Given the comparatively young age of the sample, it is possible that many of the study participants had not spent many years identifying as bisexual or lesbian and thus the negative effects of sexual identity changes were not pronounced. Many of the women in the CHLEW sample had identified as sexual minority for an extended period of time and may have been in long-term, same-gender/sex romantic relationships. Such individuals typically develop many social relationships in which sexual orientation is a defining feature, and they are often deeply integrated into sexual minority communities. Thus, identity change for women transitioning toward less same-gender/sex-oriented identities may be fraught with anxieties similar to those previously encountered by women who moved toward more same-gender/sex-oriented identities.
Interestingly, women’s level of disclosure to family members did not affect the relation between identity change and depressive symptoms. This may be because the women in the CHLEW are adults who live independently and disclosure to family members may be less important or less necessary at their stage of life.
Our findings also suggest that, among sexual minority women who begin a relationship with a male partner, a corresponding change in sexual identity may be protective for mental health, as it likely reduces cognitive dissonance. That is, our findings showed that sexual minority women who began a committed relationship with a man and also reported a corresponding change toward a less same-gender/sex-oriented identity between waves subsequently reported reduced depressive symptoms. Thus, shifts in identity do not appear to be universally detrimental for mental health, especially if such changes alleviate cognitive dissonance.
Competing group memberships are problematic for identity development and stability (Stryker & Burke, 2000). In the context of sexual orientation, previous research has found that casual sexual encounters with men are not a strong driver of sexual identity change among sexual minority women (Diamond, 2003). However, a lesbian-identified woman in a long-term, committed relationship with a male partner may find that her lesbian identity and her identity as a woman in a relationship with a male partner are not sustainable, co-existing identities—which may motivate identity change. For a bisexual woman, the challenge of aligning her sexual identity with the gender/sex of her relationship partner may be a consistent source of stress and, in part, explain the robust finding that bisexual women have poorer mental health than either lesbian or heterosexual women (e.g., Bostwick et al., 2010). Indeed, it is difficult in the context of a single romantic or sexual partnership to externally validate a bisexual identity, given that most modern, romantic couplings are dyads.
Interestingly, our results show no differences between exclusively lesbian women and “mostly” lesbian or bisexual identified women. Supplementary analyses examining whether the effect of identity change varied by baseline sexual identity were not significant. This is likely due to very few women identifying as bisexual in the initial sample recruitment (n = 10, 3 %). Given the differential stigma reported by bisexual women, perceived from both their heterosexual and gay/lesbian peers, it is possible that their experiences of sexual identity mobility are different from the experiences of other women. More research is necessary to investigate how different trajectories of sexual identity development impact diverse sexual minority sub-populations.
Several limitations of this research should be noted. First, the CHLEW study used non-probability sampling methods to recruit sexual minority women in one geographic area (Chicago metropolitan). Thus, the results are limited in their generalizability. Second, we were unable to capture the degree or magnitude of sexual identity changes that may have occurred before participants were interviewed in Wave I or between study waves. For example, some women may have changed identity multiple times and in different directions between waves; thus, our indicators of identity change may not accurately reflect the heterogeneity in mobility among participants. This would be a conservative bias, however, given that it would likely result in underestimates of the degree of identity mobility experienced by the women in the sample. Third, the sample is limited to women who identified as sexual minorities at the time of recruitment—therefore, heterosexual women who may have previously identified as lesbian or bisexual were not included. Fourth, while we focus on several identity-relevant moderating characteristics, there may be other changes in social circumstances that alter associations between sexual identity mobility and mental health. Changes in social environment and changes in the cultural acceptance of LGBT persons over time, for example, may both influence the timing and pattern of sexual identity development. It is possible that individuals may change their sexual identities based on perceived shifts in expectations for identity standards. Finally, sample size limited the statistical power of our analyses. The results presented here are conservative estimates of the effects of identity change on depressive symptoms. It should also be noted that only 21–28 % of variance was accounted for in our models, indicating that other variables likely contribute to the processes examined in our analyses. Finally, our sample is restricted to women. Future research should investigate whether changes in sexual identity have similar effects on depressive symptoms among men.
Despite these limitations, this research provides new evidence for understanding mental health disparities among sexual minority women. Our study is the first to use longitudinal data from a large sample of adult women to examine the relationship between sexual identity change and depressive symptoms and its moderating factors. Nearly 25 % of the current sample reported a change in identity over approximately 5-year intervals, and these changes had important implications for mental health. Moreover, this study investigated the circumstances under which identity changes are most, and least, likely to impact women’s mental health. More research is needed to understand factors that contribute to women’s health and well-being during periods of identity change.
When working with sexual minority women, clinicians and health care providers should familiarize themselves with clients’ sexual orientation development histories to the extent they have relevance for current mental health functioning. In particular, it should be noted that changes in sexual identity are not uncommon for a subset of this population and are not necessarily indicative of underlying pathology. Indeed, Diamond (2008, 2012) argued that transitions in sexual identity may reflect attempts to accurately represent and resolve fluctuations in sexual experiences and desires over time. Thus, providers should take care to ask detailed questions about the context in which such identity changes occur, as it possible that some changes in sexual identity precipitate improved mental health.
New theories, such as Sexual Configurations Theory (van Anders, 2015), are encouraging researchers to grapple with the multidimensional and dynamic aspects of sexuality. While far from a formal test of this theory, by creating space for variation in both identity and sexual behavior over the life course, this study is a step forward in acknowledging the complexity of women’s sexuality and the implications of such complexities for mental health. Future research should examine the impact of identity mobility on sexual orientation disparities in mental health using population-level data. Efforts to reduce the stigma surrounding sexual identity changes, including changes toward less same-gender/sex-oriented identities, may be key to improving the mental health of sexual minority women. Emphasizing the normative nature of sexual identity transitions in the lives of women, rather than viewing transitions as unusual or deviant, may be an important first step for public health interventionists and clinicians working to improve the health and well-being of sexual minority women.
Notes
Because the effects of gender versus sex are often difficult to disentangle, following van Anders (2015), we use the term “gender/sex” throughout the paper.
Supplementary analyses were conducted that interacted identity mobility with disclosure and change in relationship status. These interactions were not significant and are therefore not presented in the paper but are available from the corresponding author upon request.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
Bonanno, G. A., Papa, A., & O’Neill, K. (2001). Loss and human resilience. Applied and Preventive Psychology, 10(3), 193–206.
Bostwick, W. B. (2012). Assessing bisexual stigma and mental health status: A brief report. Journal of Bisexuality, 12(2), 214–222.
Bostwick, W. B., Boyd, C. J., Hughes, T. L., & McCabe, S. E. (2010). Dimensions of sexual orientation and the prevalence of mood and anxiety disorders in the United States. American Journal of Public Health, 100(3), 468–475.
Burgess, D., Tran, A., Lee, R., & van Ryn, M. (2007). Effects of perceived discrimination on mental health and mental health services utilization among gay, lesbian, bisexual and transgender persons. Journal of LGBT Health Research, 3(4), 1–14.
Burke, P. J. (1980). The self: Measurement requirements from an interactionist perspective. Social Psychology Quarterly, 43(1), 18–29.
Burke, P. J. (1991). Identity processes and social stress. American Sociological Review, 56(6), 836–849.
Burke, P. J. (2006). Identity change. Social Psychology Quarterly, 69(1), 81–96.
Burke, P. J., & Tully, J. C. (1977). The measurement of role identity. Social Forces, 55(4), 881–897.
Burton, C. M., Marshal, M. P., Chisolm, D. J., Sucato, G. S., & Friedman, M. S. (2013). Sexual minority-related victimization as a mediator of mental health disparities in sexual minority youth: A longitudinal analysis. Journal of Youth and Adolescence, 42(3), 394–402.
Calzo, J. P., Antonucci, T. C., Mays, V. M., & Cochran, S. D. (2011). Retrospective recall of sexual orientation identity development among gay, lesbian, and bisexual adults. Developmental Psychology, 47(6), 1658–1673.
Cass, V. C. (1979). Homosexuality identity formation: A theoretical model. Journal of Homosexuality, 4(3), 219–235.
Chaudoir, S. R., & Fisher, J. D. (2010). The disclosure processes model: Understanding disclosure decision making and postdisclosure outcomes among people living with a concealable stigmatized identity. Psychological Bulletin, 136(2), 236–256.
Chivers, M. L., Rieger, G., Latty, E., & Bailey, J. M. (2004). A sex difference in the specificity of sexual arousal. Psychological Science, 15(11), 736–744.
Cochran, S. D., Greer, J., & Mays, V. M. (2003). Prevalence of mental disorders, psychological distress, and mental health services use among lesbian, gay, and bisexual adults in the United States. Journal of Consulting and Clinical Psychology, 71(1), 53–61.
Cochran, S. D., & Mays, V. M. (2009). Burden of psychiatric morbidity among lesbian, gay, and bisexual individuals in the California Quality of Life Survey. Journal of Abnormal Psychology, 118(3), 647–658.
Coleman, E. (1982). Developmental stages of the coming out process. Journal of Homosexuality, 7(2–3), 31–43.
Corrigan, P., & Matthews, A. (2003). Stigma and disclosure: Implications for coming out of the closet. Journal of Mental Health, 12(3), 235–248.
D’Augelli, A. R., & Grossman, A. H. (2001). Disclosure of sexual orientation, victimization, and mental health among lesbian, gay, and bisexual older adults. Journal of Interpersonal Violence, 16(10), 1008–1027.
D’Augelli, A. R., Hershberger, S. L., & Pilkington, N. W. (1998). Lesbian, gay, and bisexual youth and their families: Disclosure of sexual orientation and its consequences. American Journal of Orthopsychiatry, 68(3), 361–371.
Diamant, A. L., & Wold, C. (2003). Sexual orientation and variation in physical and mental health status among women. Journal of Women’s Health, 12(1), 41–49.
Diamond, L. M. (2000). Sexual-identity, attractions, and behavior among young sexual-minority women over a 2-year period. Developmental Psychology, 36(2), 241–250.
Diamond, L. M. (2003). Was it a phase? Young women’s relinquishment of lesbian/bisexual identities over a 5-year period. Journal of Personality and Social Psychology, 84(2), 352–364.
Diamond, L. M. (2007). A dynamical systems approach to the development and expression of female same-sex sexuality. Perspectives on Psychological Science, 2(2), 142–161.
Diamond, L. M. (2008). Female bisexuality from adolescence to adulthood: Results from a 10-year longitudinal study. Developmental Psychology, 44(1), 5–14.
Diamond, L. M. (2012). The desire disorder in research on sexual orientation in women: Contributions of dynamical systems theory. Archives of Sexual Behavior, 41, 73–83.
Everett, B. G. (2015). Sexual orientation identity change and depressive symptoms: A longitudinal analysis. Journal of Health and Social Behavior, 56(1), 37–58.
Feinstein, B. A., Goldfried, M. R., & Davila, J. (2012). The relationship between experiences of discrimination and mental health among lesbians and gay men: An examination of internalized homonegativity and rejection sensitivity as potential mechanisms. Journal of Consulting and Clinical Psychology, 80(5), 917–927.
Floyd, F. J., & Bakeman, R. (2006). Coming-out across the life course: Implications of age and historical context. Archives of Sexual Behavior, 35(3), 287–296.
Floyd, F. J., & Stein, T. S. (2002). Sexual orientation identity formation among gay, lesbian, and bisexual youths: Multiple patterns of milestone experiences. Journal of Research on Adolescence, 12(2), 167–191.
Fredriksen-Goldsen, K. I., Hyun-Jun, K., Barkan, S. E., Balsam, K. F., & Mincer, S. L. (2010). Disparities in health-related quality of life: A comparison of lesbians and bisexual women. American Journal of Public Health, 100(11), 2255–2261.
Haslam, A., Jetten, J., Postmes, T., & Haslam, C. (2008). Maintaining group memberships: Social identity continuity predicts well-being after stroke. Neuropsychological Rehabilitation, 18(5/6), 671–691.
Hatzenbuehler, M. L., McLaughlin, K. A., Keyes, K. M., & Hasin, D. S. (2010). The impact of institutional discrimination on psychiatric disorders in lesbian, gay, and bisexual populations: A prospective study. American Journal of Public Health, 100(3), 452.
Hatzenbuehler, M. L., Phelan, J. C., & Link, B. G. (2013). Stigma as a fundamental cause of population health inequalities. American Journal of Public Health, 103(5), 813–821.
Herek, G. M., Gillis, J. R., & Cogan, J. C. (1999). Psychological sequelae of hate-crime victimization among lesbian, gay, and bisexual adults. Journal of Consulting and Clinical Psychology, 67(6), 945–951.
Horowitz, J. L., & Newcomb, M. D. (2002). A multidimensional approach to homosexual-identity. Journal of Homosexuality, 42(2), 1–19.
Hughes, T. L., Wilsnack, S. C., & Kristjanson, A. F. (2015). Substance use and related problems among U.S. women who identify as mostly heterosexual. BMC Public Health, 15, 803.
Iyer, A., & Jetten, J. (2011). What’s left behind: Identity continuity moderates the effect of nostalgia on well-being and life choices. Journal of Personality and Social Psychology, 101(1), 94–108.
Iyer, A., Jetten, J., Tsivrikos, D., Postmes, T., & Haslam, S. A. (2009). The more (and the more compatible) the merrier: Multiple group memberships and identity compatibility as predictors of adjustment after life transitions. British Journal of Social Psychology, 48(4), 707–733.
Katz-Wise, S., & Hyde, J. S. (2014). Sexual fluidity and related attitudes and beliefs among young adults with a same-gender orientation. Archives of Sexual Behavior, 44(5), 1459–1470.
Maguen, S., Floyd, F. J., Bakeman, R., & Armistead, L. (2002). Developmental milestones and disclosure of sexual orientation among gay, lesbian, and bisexual youths. Journal of Applied Developmental Psychology, 23(2), 219–233.
Marshal, M. P., Dietz, L. J., Friedman, M. S., Stall, R., Smith, H. A., et al. (2011). Suicidality and depression disparities between sexual minority and heterosexual youth: A meta-analytic review. Journal of Adolescent Health, 49(2), 115–123.
Matthews, A. K., Hughes, T. L., Johnson, T., Razzano, L. A., & Cassidy, R. (2002). Prediction of depressive distress in a community sample of women: The role of sexual orientation. American Journal Public Health, 92(7), 1131–1139.
McCabe, S. E., Hughes, T. L., & Boyd, C. J. (2004). Substance use and misuse: Are bisexual women at greater risk? Journal of Psychoactive Drugs, 36(2), 217–225.
McFarland, D., & Pals, H. (2005). Motives and contexts of identity change: A case for network effects. Social Psychology Quarterly, 68(4), 289–315.
McLaughlin, K. A., Hatzenbuehler, M. L., Xuan, Z., & Conron, K. J. (2012). Disproportionate exposure to early-life adversity and sexual orientation disparities in psychiatric morbidity. Child Abuse and Neglect, 36(9), 645–655.
Meyer, I. H. (1995). Minority stress and mental health in gay men. Journal of Health and Social Behavior, 36(1), 38–56.
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674.
Mock, S. E., & Eibach, R. P. (2012). Stability and change in sexual orientation identity over a 10-year period in adulthood. Archives of Sexual Behavior, 41(3), 641–648.
Mossakowski, K. N. (2003). Coping with perceived discrimination: Does ethnic identity protect mental health? Journal of Health and Social Behavior, 44, 318–331.
Mulick, P. S., & Wright, L. W. (2002). Examining the existence of biphobia in the heterosexual and homosexual populations. Journal of Bisexuality, 2(4), 45–64.
Needham, B. L. (2012). Sexual attraction and trajectories of mental health and substance use during the transition from adolescence to adulthood. Journal of Youth and Adolescence, 41(2), 179–190.
Ott, M. Q., Corliss, H. L., Wypij, D., Rosario, M., & Austin, S. B. (2011). Stability and change in self-reported sexual orientation identity in young people: Application of mobility metrics. Archives of Sexual Behavior, 40(3), 519–532.
Parent, M. C., Talley, A. E., Schwartz, E. N., & Hancock, D. W. (2015). I want your sex: The role of sexual exploration in fostering positive sexual self-concepts for heterosexual and sexual minority women. Psychology of Sexual Orientation and Gender Diversity, 2, 199–204.
Ramirez-Valles, J., Kuhns, L. M., Campbell, R. T., & Diaz, R. M. (2010). Social integration and health: Community involvement, stigmatized identities, and risk in Latino sexual minorities. Journal of Health and Social Behavior, 51(1), 30–47.
Robins, L. N., Helzer, J. E., Croughan, J., & Ratcliff, K. S. (1981). National Institute of Mental Health Diagnostic Interview schedule: Its history, characteristics, and validity. Archives of General Psychiatry, 38(4), 381–389.
Rosario, M., Hunter, J., Maguen, S., Gwadz, M., & Smith, R. (2001). The coming-out process and its adaptational and health-related associations among gay, lesbian, and bisexual youths: Stipulation and exploration of a model. American Journal of Community Psychology, 29(1), 133–160.
Rosario, M., Schrimshaw, E. W., & Hunter, J. (2008). Predicting patterns of sexual identity development over time among lesbian, gay, and bisexual youths: A cluster analytic approach. American Journal of Community Psychology, 42, 266–282.
Rosario, M., Schrimshaw, E. W., & Hunter, J. (2011). Different patterns of sexual identity development over time: Implications of the psychological adjustment of lesbian, gay, and bisexual youths. Journal of Sex Research, 48(1), 3–15.
Rosario, M., Schrimshaw, E. W., Hunter, J., & Braun, L. (2006). Sexual-identity development among lesbian, gay, and bisexual youths: Consistency and change over time. Journal of Sex Research, 43(1), 46–58.
Russell, S. T., & Joyner, K. (2001). Adolescent sexual orientation and suicide risk: Evidence from a national study. American Journal of Public Health, 91(8), 1276–1281.
Savin-Williams, R. C. (2011). Identity development among sexual-minority youth. In S. J. Schwartz, K. Luyckx, & V. L. Vignoles (Eds.), Handbook of identity theory and research (pp. 671–689). New York: Springer.
Savin-Williams, R. C., Joyner, K., & Rieger, G. (2012). Prevalence and stability of self-reported sexual orientation identity during young adulthood. Archives of Sexual Behavior, 41(1), 103–110.
Schnittker, J., & McLeod, J. D. (2005). The social psychology of health disparities. Annual Review of Sociology, 31, 75–103.
Sellers, R. M., Caldwell, C. H., Schmeelk-Cone, K. H., & Zimmerman, M. A. (2003). Racial identity, racial discrimination, perceived stress, and psychological distress among African American young adults. Journal of Health and Social Behavior, 44(3), 302–317.
Sellers, R. M., Copeland-Linder, N., Martin, P. P., & Lewis, R. L. (2006). Racial identity matters: The relationship between racial discrimination and psychological functioning in African American adolescents. Journal of Research on Adolescence, 16(2), 187–216.
Stryker, S., & Burke, P. J. (2000). The past, present, and future of an identity theory. Social Psychology Quarterly, 63(4), 284–297.
Stryker, S., & Serpe, R. T. (1982). Commitment, identity salience, and role behavior: Theory and research example. In W. Ickes & E. S. Knowles (Eds.), Personality, roles, and social behavior (pp. 199–218). New York: Springer.
Tabatabai, A., & Linders, A. (2011). Vanishing act: Non-straight identity narratives of women in relationships with women and men. Qualitative Sociology, 34(4), 583–599.
Tajfel, H., & Turner, J. C. (1979). An integrative theory of intergroup conflict. In G. A. William & S. Worchel (Eds.), The social psychology of intergroup relations (pp. 33–47). Monterey, CA: Brooks-Cole.
Tajfel, H., & Turner, J. C. (2004). The social identity theory of intergroup behavior. In J. T. Jost & J. Sidanius (Eds.), Political psychology: Key readings (pp. 276–293). New York: Psychology Press.
Troiden, R. R. (1988). Homosexual-identity development. Journal of Adolescent Health Care, 9(2), 105–113.
Twenge, J. M., Catanese, K. R., & Baumeister, R. F. (2003). Social exclusion and the deconstructed state: Time perception, meaninglessness, lethargy, lack of emotion, and self-awareness. Journal of Personality and Social Psychology, 85(3), 409.
Valentine, G., Skelton, T., & Butler, R. (2003). Coming out and outcomes: Negotiating lesbian and gay identities with, and in, the family. Environment and Planning, 21(4), 479–500.
van Anders, S. M. (2015). Beyond sexual orientation: Integrating gender/sex and diverse sexualities via sexual configurations theory. Archives of Sexual Behavior, 44(5), 1177–1213.
Acknowledgments
This study was supported by the National Institutes of Health and Office of Research on Women’s Health (ORWH) Grant K12HD055892, and by the National Institute of Alcohol Abuse and Alcoholism (NIAAA) Grant R01 AA13328-01 and NIAAA Grant AA019974.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Everett, B.G., Talley, A.E., Hughes, T.L. et al. Sexual Identity Mobility and Depressive Symptoms: A Longitudinal Analysis of Moderating Factors Among Sexual Minority Women. Arch Sex Behav 45, 1731–1744 (2016). https://doi.org/10.1007/s10508-016-0755-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10508-016-0755-x