
Abstract
One of the four national HIV prevention goals is to incorporate combinations of effective, evidence-based approaches to prevent HIV infection. In fields of public health, techniques that alter environment and affect choice options are effective. Structural approaches may be effective in preventing HIV infection. Existing frameworks for structural interventions were lacking in breadth and/or depth. We conducted a systematic review and searched CDC’s HIV/AIDS Prevention Research Synthesis Project’s database for relevant interventions during 1988–2013. We used an iterative process to develop the taxonomy. We identified 213 structural interventions: Access (65%), Policy/Procedure (32%), Mass Media (29%), Physical Structure (27%), Capacity Building (24%), Community Mobilization (9%), and Social Determinants of Health (8%). Forty percent targeted high-risk populations (e.g., people who inject drugs [12%]). This paper describes a comprehensive, well-defined taxonomy of structural interventions with 7 categories and 20 subcategories. The taxonomy accommodated all interventions identified.
Resumen
Uno de los cuatro objetivos nacionales de prevención del VIH es usar combinaciones de enfoques los cuales son eficaces y basadas en evidencia para prevenir la infección por el VIH. En los campos de la salud pública, técnicas que alteran el medio ambiente y afectan opciones son eficaces. Enfoques estructurales pueden ser eficaces en la prevención de la infección por VIH. Los marcos existentes para las intervenciones estructurales carecían en amplitude, en profundidad, o en ambos. Se realizó una revisión sistemática y búsquedas en la base de datos del proyecto Síntesis de los VIH/SIDA Prevención Investigaciónes de los Centros para el Control y la Prevención de Enfermedades para intervenciones pertinentes publicado durante 1988-2013. Utilizamos un proceso iterativo para desarrollar la taxonomía. Se identificaron 213 intervenciones estructurales: Acceso (65%), Política o procedimiento (32%), Medios de comunicación (29%), Estructura física (27%), Capacitación (24%), Movilización de la comunidad (9%) y Determinantes sociales de la salud (8%). Cuarenta por ciento había concentrado en poblaciones de alto riesgo (por ejemplo, personas que se inyectan drogas [12%]). Este artículo describe una taxonomía completa y bien definida de intervenciones estructurales con 7 categorías y 20 subcategorías. La taxonomía acomodado todas las intervenciones identificadas.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
National HIV prevention goals [1] include the expansion of efforts to prevent HIV infection by using a combination of effective, evidence-based strategies. An updated, national goal [1] calls for adoption of structural approaches to reduce HIV infections and improve health outcomes in communities with high rates of infection as one of the steps to reducing HIV-related disparities and health inequities. Many public health outcomes are partly determined by individuals’ behaviors. Public health efforts to reduce the consequences of such behaviors often rely on appeals to individuals to change their behavior. However, other approaches have been developed and these strategies, one of which is referred to as “structural,” alter the environment in ways that facilitate or promote safer behaviors, or reduce risk in ways that do not rely on individual behavior change. Historically, major structural public health interventions have had large impacts.
Several HIV specialists have developed frameworks for classifying structural interventions for HIV prevention. However, they all consisted of a set of categories designed to be illustrative, rather than comprehensive. Sweat and Denison [2] proposed that behavior change interventions can produce change at any of four causal levels—individual, environmental, structural, and “superstructural”—and gave examples and change mechanisms for each. For example, superstructural interventions were defined as “macrosocial and political arrangements, resources, and power differences that result in unequal advantages.” Examples of such interventions might include “national and international social movements, revolution, land redistribution, war, and empowerment of disenfranchised populations.” Structural interventions were defined as “laws, policies, and standard operating procedures.”
Blankenship and colleagues [3] reviewed the literature available at the time and proposed nine categories of structural interventions based on contextual factors of availability, acceptability (e.g., campaigns shaming people committing unacceptable behavior, such as drug use), and accessibility. Similarly to the Sweat and Denison analysis, these authors gave examples of each at the individual, organizational, and environmental levels.
In the context of a special issue of AIDS resulting from a consultation organized by scientists (including the senior author of the current manuscript) at the Centers for Disease Control and Prevention (CDC), Sumartojo and colleagues [4] presented a table listing types of structural interventions (economic resources, policy supports, societal conditions, and organizational structures and functions) crossed with types of institutions (government, service organizations, private business, workforce organization, faith community, justice system, media, educational system, and the health care system) that could be a barrier or provide support. Again, these examples were not based on the extant literature, nor meant to be comprehensive.
In 2000, Cohen and Scribner [5] described four categories of structural interventions: Availability, Physical Structures, Social Structures, and Media Messages. In a later exposition by Blankenship and colleagues [6], structural interventions were categorized into four types: community mobilization, integration of HIV services, contingent funding, and economic and educational interventions; these four were largely mutually exclusive of the four specified by Cohen et al. [5]. Another such effort was undertaken by Tsai [7] who described structural interventions as existing along two dimensions: implementation intensity, and dependence of the effects on user agency. However, only a few examples were provided. Lastly, Kaufman and colleagues [8] noted stigma as an important factor that may influence HIV-related behavior. Other efforts at structural interventions to date have suffered the same issue of lacking comprehensiveness [9,10,11,12,13]. Moreover, a systematic process to categorize existing structural interventions was not attempted.
As we became immersed in the literature, we found the need for an all-inclusive framework to organize the different types of structural interventions. Therefore, we conducted a systematic review of the literature on structural interventions addressing HIV and developed a detailed and comprehensive taxonomy to enable categorization of every identified structural intervention. The purpose of this paper is to describe this new taxonomy in detail and to apply it to organize interventions identified through the systematic review.
Research Questions
This review addressed the following research questions:
-
1.
What types of HIV prevention structural interventions are currently in the literature?
-
2.
What are the outcomes of HIV prevention structural interventions?
-
3.
Are there patterns in types of HIV prevention structural interventions? (Do certain types go together?)
-
4.
What are the study designs of HIV prevention structural interventions?
-
5.
Has the mix of HIV prevention structural interventions changed across time in terms of location, structural intervention type, research design, and population groups?
Methods
Search Strategy
To identify structural interventions in HIV prevention, we used CDC’s Prevention Research Synthesis (PRS) Project’s cumulative database (PRS database) of citations relating to HIV, AIDS and STI prevention literature from 1988 to 2013. Citations in this database are coded for a variety of variables related to populations, settings, interventions and outcomes. At the time of this project in 2013, the database contained more than 64,000 unique citations that were coded according to topics, target populations and types of interventions. This database is updated annually with automated searches [14] designed and tailored to four research areas: (1) HIV, AIDS, or STI behavioral prevention; (2) linkage to, retention in, and re-engagement in HIV care; (3) HIV, AIDS, antiretroviral therapy (ART) treatment and adherence; and (4) systematic reviews on HIV and AIDS. The automated searches use six electronic bibliographic databases to retrieve relevant published literature: CAB Global Health (OVID), CINAHL (EBSCOhost), EMBASE (OVID), PsycINFO (OVID), MEDLINE (OVID), Sociological Abstracts (ProQuest) [15,16,17,18]. In addition, there is a supplemental manual search, which includes a quarterly hand search of 52 journals, requesting publications from experts in the field and reviewing other sources, such as electronic mail lists, clinical trial databases (e.g., Cochrane Library, CRISP database), conference proceedings, and references harvested from relevant HIV behavioral prevention research literature [14]. Full search strategy details of databases searched, MEDLINE search strategy, and a list of hand-searched journals are provided in the online Supplementary Materials A, B, and C, respectively. Citations identified through automated and manual searches were downloaded and deduplicated in the PRS database before conducting title/abstract screening and full report coding.
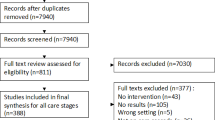
To obtain citations for this project specific to structural interventions, the PRS database was searched for citations published between 1988 and March 2013 that were coded as (1) “structural intervention,” yield = 135 citations; or (2) “policy intervention,” yield = 38 citations; or (3) “structural change mechanism,” yield = 100 citations. A second search was conducted after the taxonomy was developed and included terms that were not in the original search. These coded terms included (1) “capacity building,” yield = 33 citations, (2) “community mobilization,” yield = 37 citations, and (3) “social marketing/mass media,” yield = 97 citations. The total citation yield from the PRS database was 440 citations, last searched on May 3, 2017. In addition, authors hand-searched reference lists of related reports and systematic reviews and identified 63 more citations. Thus, 503 potential papers were identified (see Fig. 1).

Flow chart showing number of papers identified, duplicates, reasons for exclusion, and total number of included studies
Inclusion Criteria
To be included in this review, studies were required to meet the following criteria:
-
Evaluation of an intervention that included at least one structural component not controlled by the individual, affecting recipients’ behavior or other aspects of HIV risk
-
Reported data on at least one of the specified outcomes (see list below in Outcome Measures)
-
Published in English in a peer-reviewed journal
-
Research design including a comparison condition, specifically:
-
RCTs, cluster RCTs
-
quasi-experimental, cluster quasi-experimental (defined here as comparison trials where treatment assignment is not random but also not self-selected)
-
time series (requiring two or more observations before and after the intervention)
-
prospective cohort studies
-
retrospective cohort studies
-
case–control studies
-
before/after comparisons (including comparisons against a baseline of zero)
-
Exclusion Criteria
-
Interventions delivered at the community level unless there was an explicit structural component. Interventions were considered community level and not structural if the activity focused on individual participation or transactions, such as small group empowerment meetings or one-to-one conversations.
-
Exposure analysis (i.e., only comparing people reporting exposure versus no exposure to an intervention)
Variables Abstracted
The following variables were abstracted: first author name, year of publication, years and location of implementation, target population, type of structural intervention, study design, outcomes measured, and description of intervention.
Outcome Measures
Studies were eligible for this review if they reported results on at least one of the following outcome measures:
-
Sexual risk behaviors associated with HIV infection or STI (e.g., condomless sex, number of sex partners)
-
Injection drug use behaviors (e.g., uptake of sterile syringes, frequency of injection drug use)
-
HIV testing (e.g., number of people tested for HIV)
-
HIV infection
-
STI when used as a proxy for behavior change (i.e., excluding improved surveillance)
-
HIV stigma
-
ART prescriptions, when an outcome of provider interventions
-
Adherence to HIV medication
-
Engagement in HIV primary medical care (including health care utilization, linkage to and retention in care)
We excluded certain outcomes that we considered more distal to HIV infection. The outcomes excluded, or that did not qualify a citation for the review, were:
-
Number of condoms distributed/taken
-
Attitudes other than stigma
-
Cognition including knowledge
-
Communication
Procedure
We developed a definition for structural interventions through an iterative procedure of literature review and workgroup discussion. In 2010–2011, a team of experts reviewed the first 87 citations and developed an initial definition and taxonomy. In 2012, two coders were added to the project and independently coded the 87 citations by using the categories developed in the first step. The categories and corresponding definitions were further refined. All citations were coded by pairs of independent coders. Discrepancies were resolved through discussion by all team members.
Statistical Methods
Taxonomy categories and subcategories were analyzed using descriptive statistics and cross-tabulations. We used logistic regression to examine changes across time in the proportion of studies that featured various characteristics, specifically type of structural intervention, location (high versus middle/low income economies), type of study population, and study design quality (stronger versus weaker designs). In each model, the dependent variable was presence or absence of the characteristic of interest. The independent variable was year, so that the odds ratio (OR) represents the annual increase in odds that a study includes the characteristic of interest. For graphic presentation we grouped the 26-year review period into one group of 6 years followed by four groups of 5 years. SAS version 9.3 was used for the analyses.
Results
Structural Intervention Definition and Taxonomy Development
We defined structural interventions as:
An intervention that affects risk and/or behavioral choices by changing something that is external to the individual and not under his/her control.
The definition is broad enough to include interventions that operate in two distinct ways along separate continua to reduce risk: intervention target and proximity to HIV infection. The first dimension refers to whether an intervention targets changes in individuals versus environment. When the intervention alters the environment (e.g., storefront HIV testing centers) or uses strategies to alter the choice structure (e.g., routine opt-out HIV testing in clinical settings), these are outside the individual’s control. The second dimension refers to whether an intervention alters social determinants of the epidemic (e.g., microfinance interventions or reducing societal homophobia). We categorized all interventions along these two dimensions as illustrated in Fig. 2. Interventions are considered structural if they meet one or both criteria of being distal to the infection (e.g., social determinants of health) or targeting the environment. Thus, structural interventions fall into three of the four quadrants.

Two dimensions and four quadrants useful in distinguishing structural interventions from other types of interventions. Interventions are considered structural if they target the environment and/or address determinants of health that are distal to HIV infection. Quadrant 1 is not considered to be structural
Interventions in Quadrant 1 are typically focused on changing individual behavior, knowledge, and awareness, and focused on proximal causes; these meet neither criterion, thus are considered not structural. Interventions in Quadrant 4 are considered structural as they meet both criteria (i.e., they target the environment rather than the individual and are focused on distal causes). Those in Quadrants 2 and 3 meet only one of the two criteria to affect change; however, these types of interventions were considered to be structural as well.
We next developed a taxonomy of structural interventions and refined definitions for each category in the taxonomy (Access, Policy/Procedure, Physical Structure, Capacity Building, Mass Media, Community Mobilization, and Social Determinants). Most of the categories had subcategories; all are defined below.
Taxonomy Definitions
Access
Provision of a health product or service or actions that make such products or services more readily available to the intended users. Access can be modified in ways that include, but are not limited to, physical changes. Examples include locating a storefront HIV testing site in a neighborhood or expanding its hours of operation. Condom distribution counts as access only if condoms are available widely and do not require enrollment into a program to procure. Subcategories of Access include HIV testing, Condoms, STI testing, Sterile injection equipment, HIV Health Care, and Drug treatment.
Policy/Procedure
Policy is formal guidance, principal, or rule adopted to bring about change. Procedure is the implementation of a policy and typically specifies a process. It is important to note that virtually all interventions require some policy or procedural change in order to be instantiated. Both are decided at an organizational or higher level that do require input at the individual level. Often, policy/procedure interventions are ones in which the change is the intervention itself.
-
Institutional policy/procedure Policies enacted by a nonjudicial entity such as a clinic, school, or workplace that affect risk and/or behavioral choices (e.g., opt-out testing in an ER).
-
Governmental policy For interventions in this category, there may not be legal consequences for infractions and they may be issued from a municipal, state, or national body (e.g., CDC guidelines on preexposure prophylaxis).
-
Legislation Involves change in law that affect risk and/or behavioral choices (e.g., syringe access laws). Such changes have the authority of the polity behind them.
Mass Media
Widely disseminated interventions via a large-scale communication medium other than person-to-person.
-
Social marketing The promotion of some positive social objective by employing marketing techniques used commercially; often disseminated via mass media (e.g., radio or TV spots delivering a crafted message). A requirement is that the information channel can be said to saturate the environment, so that exposure is largely outside the control of the individual (e.g., video shown to large waiting room; large posters displayed in multiple locations in a neighborhood). Small communication channels, such as letters, brochures, newsletters, and videos delivered to individuals or small groups, do not qualify as mass media.
-
Narrative interventions Interventions focused on a storyline included in the media (e.g., soap operas, podcast serial dramas).
Physical Structure
Any physical form that affects risk directly or the ease with which healthy behaviors can be performed (e.g., creating new clinics, integrating services in one location, building a road, using a mobile van to deliver services).
-
Integration of services Services or products are brought together (i.e., co-located) for the sake of the convenience of the intended user and the efficiency of service provision. This is an important subset of physical structure interventions.
-
New physical structures Development of structures that did not exist previously, at least in the present location (e.g. clinics, vans, doors on bathhouse rooms).
-
Service provided in nontraditional setting Health services made available to people in a particular setting (e.g., homes, workplaces, prisons, schools) and the original service provided in the setting is not related to health or located in a health setting.
Capacity-Building
Change that improves an agency’s ability to provide services or programs.
-
Provider/supervisor training Training of health care or other staff to help them use more effective procedures with patients/clients.
-
Technology Using tools to increase productivity.
-
Hiring staff/funding Adding personnel to start interventions or increase productivity or securing monies to implement or enhance interventions.
-
Staff incentives Providing inducements, either monetary or nonmonetary, to increase productivity.
Community Mobilization
A process of change involving multiple stakeholders within a community, including people who live in the community. A key criterion is that the community becomes involved through interaction with each other and the resulting change includes emergent properties, such as collective efficacy (e.g., commercial sex workers who unite together to demand condom use from clients). A substantial amount of the change is generated by community members who play a role in developing and implementing the intervention.
Social Determinants of Health Interventions
Interventions addressing survival or acceptance and respect.
-
Survival Interventions that address factors having to do with basic necessities, such as money, food, and shelter, rather than, or in addition to, addressing HIV-related risk behavior directly.
-
Acceptance and Respect Interventions that address prejudice, discrimination, HIV stigma, or homophobia in the social environment of those whose health and/or health behaviors are affected by them. Interventions aimed at reducing internalized prejudice do not necessarily count as structural interventions because they may directly influence only the affected individuals.
The categories are mutually exclusive with the exception of the Access category. Often, interventions in other categories provided access to things by their very nature, such as condoms, HIV testing, or sterile syringes, and thus meet the definition of the Access category. On the other hand, interventions can also be classified in more than one category when they have multiple components, such as an intervention that includes community mobilization of commercial sex workers in addition to a policy of 100% condom use. Most of the interventions in these categories fit into quadrants 3 or 4 in Fig. 2. Only interventions in the social determinants of health category may fit into quadrant 2 or 4.
Characteristics of Structural Interventions and Categorization using the New Taxonomy
Sample of Studies
From the 503 citations identified by the search, 213 intervention studies published between 1988 and 2013 met criteria and are therefore included in this review (Fig. 1, Appendix Table 6). The interventions were conducted between 1984 and 2010; more than half began in 2001 or later.
Type of Structural Intervention
The majority of interventions were categorized as Access (65%, n = 139) (Table 1); the most common Access types were HIV testing (n = 52), condoms (n = 48), and STI testing and treatment (n = 34). The next largest category was Policy/Procedure (32%, n = 68) with 51 studies employing institutional policies/procedures and 18 employing governmental. Twenty-nine percent of the interventions were developed as Mass Media interventions (n = 62), most of which included social marketing campaigns (n = 56). Five of the social marketing studies also included narrative interventions while six were narrative interventions only.
Twenty-seven percent of studies were categorized as a Physical Structure (n = 58), either by providing services in a nontraditional setting (n = 23), integrating services (n = 22), or developing a new physical structure (n = 20). Twenty-four percent of the studies featured Capacity Building (n = 51), most frequently through provider or supervisor training (n = 42) or new technology (n = 12). Nine percent of studies were categorized as Community Mobilization (n = 20) and eight percent of studies were considered to be Social Determinants of Health (n = 16).
There was a significant increase across time in the proportion of studies that included three SI types (Fig. 3). The proportion including Physical Structure increased from 13% in 1988–1993 to 33% in 2009–2013 (OR per year = 1.08, 95% CI 1.02, 1.14). The proportion including Policy and Procedure increased from 27 to 44% (OR 1.06, 95% CI 1.01, 1.11). The proportion including Social Determinants of Health increased from 0 to 14% (OR 1.24, 95% CI 1.06, 1.46). There was a significant decrease across time in the proportion of studies that included Mass Media from 47 to 14% (OR 0.91, 95% CI 0.88, 0.97). There was no significant change across time in the proportion of studies that included Access, Capacity Building, or Community Mobilization.

Changes over time in proportion of studies by type of structural intervention, 1998–2013
Intervention Location
The interventions were located in countries around the world (Table 2). The largest proportion (49%, n = 104) of studies were conducted in the Americas, most of them in the United States (n = 84); within the United States, the largest numbers were from the West (n = 30), Southeast (n = 16) and Northeast (n = 15). Twenty-four percent of studies were conducted in Africa (n = 52), including nine from Tanzania, eight from South Africa, and six from Uganda. Seventeen percent of the studies were conducted in Asia (n = 36) including nine each from China, India, and Thailand. Eight percent were conducted in Europe (n = 18), including nine studies from the United Kingdom and two each from France, Italy, and the Netherlands. Three studies were from Australia. In analyses examining change over time, there was no significant change in the proportion of interventions conducted in high income economies versus middle/low economies (OR 0.99, 95% CI 0.95, 1.04).
Target Population
Table 3 summarizes the target populations across the interventions. Forty percent of the structural interventions focused on high-risk populations, including 32 studies targeting commercial sex workers, 26 studies targeting individuals who inject drugs (PWID), and 17 studies targeting men who have sex with men (MSM). Several studies focused on females (n = 47), persons living with HIV (n = 32), youth (n = 30), people residing in urban/inner city areas (n = 26), young adults (n = 20), HIV clinic patients (n = 16), blacks or African Americans (n = 12), and Hispanics/Latinos (n = 8).
Fewer studies targeted homeless persons (n = 4), non-injection drug users (n = 4), pregnant females (n = 4), incarcerated persons (n = 4), or sexually active youth (n = 3). Only one study focused on transgender persons. There was a significant increase over time in the proportion of interventions focusing on persons living with HIV, from 7% in 1988–1993 to 30% in 2009-2013 (OR = 1.17, 95% CI 1.06, 1.28), and a significant decrease in the proportion of interventions targeting PWID, from 53 to 7% (OR 0.89, 95% CI 0.84, 0.95). There was no significant change across time in the proportion of studies focusing on commercial sex workers (OR 0.97, 95% CI 0.91, 1.03) or MSM (OR 1.00, 95% CI 0.92, 1.08).
Outcome
Sex behavior outcomes constituted the largest category of outcomes (50%, n = 106); condom use was the most frequent outcome in this category (n = 81) (Table 4). Testing or treatment outcomes were the next largest category (40%, n = 86); HIV testing (n = 60) was the most frequent type of testing/treatment, followed by retention in care (n = 13) and antiretroviral adherence (n = 11). Twenty-five percent of the interventions reported biologic outcomes (n = 53), which consisted predominantly of STI (n = 31) and HIV infection (n = 26). Other biologic outcomes included viral load/suppression, CD4 counts and AIDS mortality. There was a smaller proportion of drug injection behavior outcomes (13%, n = 28); among these, sharing of equipment or injection drug use were reported most frequently. There were only 5 studies with stigma outcomes (2%).
Type of Research Design
The majority of interventions was evaluated using before/after research design, either one group or cross-sectional (57%, n = 121), but other research designs of randomized controlled trials, quasi-experimental, and serial cross-sectional designs were also employed (Table 5). There was no significant change over time in proportion of high-quality study designs (i.e., RCT, cluster RCT, quasi-experimental and cluster quasi-experimental) versus low-quality study design (e.g., before/after designs or after-only designs) (OR 1.01, 95% CI 0.96, 1.06).
Discussion
Overall HIV incidence in the United States has remained stable despite increasing prevalence [19]. Several federal initiatives have been used to maintain or reduce new HIV diagnoses, the most recent of which is High Impact Prevention [20], a strategy to allocate resources on activities found to have the greatest impact in HIV prevention. Moving forward, the national HIV prevention goals [1] emphasize structural interventions as a way to reduce new HIV infections, thus it is timely to have a comprehensive framework for structural interventions. In this study, we developed a taxonomy of structural interventions comprising 7 categories and 20 subcategories, and classified 213 structural interventions into the new taxonomy. The new taxonomy is parsed similarly to Cohen et al. [5] and Blankenship et al. [6], but is more comprehensive than either taken singly and also includes social determinants of health (survival and acceptance). Blankenship et al. [6] included “community mobilization” and “integration of services,” which are also part of our own taxonomy. “Contingent funding,” while being sparse in the literature at the time we conducted our review, would be an example of using Social Determinants of Health-Survival, as would “economic development programs.” The category of “educational interventions” has more to do with site of delivery than type of intervention per se, and therefore does not appear in our taxonomy.
In earlier work, Blankenship and colleagues [3] proposed “availability” and “accessibility” categories, which are similar to our access category. Sumartojo and colleagues [4] included “economic resources,” which is similar to our category of social determinants of health-survival; “policy supports” is similar to our policy/process; and both “societal conditions” and “organizational structures and functions” encompass more than a single category in our taxonomy. Tsai [7], on the other hand, gave a few examples but none of them overlap with our categories. In summary, our taxonomy encompassed every structural intervention identified from the systematic review in HIV prevention and was built to be inclusive and comprehensive of interventions beyond the systematic review. Each category and subcategory has detailed definitions that were tested and refined during an iterative process. Moreover, since this taxonomy is broad, it is useful in presenting a wide variety of options to consider when choosing strategies that will best address the specific needs of a community.
Access, Policy/Procedures, Mass Media, and Physical Structure were the most common structural interventions identified in the literature. By contrast, interventions addressing social determinants of health were infrequently found in the HIV prevention and treatment literature. The largest proportion of the interventions were conducted in the United States but it is important to note that many of the interventions in low-middle–income countries were conducted by researchers from high-income countries. In general, the evaluation of the interventions consisted of before/after research designs and the rigor did not increase over time, possibly because it is often not feasible to randomly allocate structural interventions or study them in controlled situations.
While nearly 40% of the structural interventions focused on high-risk populations, interventions targeting MSM were relatively few compared to PWID and commercial sex workers.
Some structural interventions—namely, those addressing social determinants of health (both survival-related and tolerance/acceptance-related)—have the potential to influence multiple health conditions. Poverty, for example, is related to many health outcomes [21]. While conducting a microfinance intervention to address HIV risk alone may appear to be prohibitively expensive, a study assessing its effects on multiple health outcomes may demonstrate cost-effectiveness. Unfortunately, the disease-specific silos around which health promotion and illness prevention funding are organized make it difficult to conduct such studies. Thus, most interventions target intermediate structural factors associated with HIV and do not address fundamental contributors to health disparities, such as poverty, housing, and education. These contributors are termed frequently as “social determinants of health” and, for many health conditions, generally account for more variance in health than most factors and arguably more than individual behaviors [21]. Agencies that are capable of addressing these major structural determinants, such as US Departments of Housing and Urban Development (HUD), Labor (DOL) or Education (ED), do not necessarily focus on public health, but their programs are likely to have great impact on health outcomes. Evaluation of programmatic or policy interventions directed towards employment generation, school retention, or housing stability can be designed to examine effects on HIV and other health outcomes. It is often considered outside the reach of public health to intervene on these domains due to narrow organizational missions and vertical funding streams. However, with shrinking public health dollars, an HIV epidemic characterized by extreme disparities driven by social conditions, and the syndemic nature of infectious disease, chronic illness, substance abuse, and mental health, meaningful action-oriented collaborations that alter the fundamental causes of HIV and other health outcomes are needed urgently. Given the lack of integration between the health care system and other key non-health care systems, more of these collaborations from different arenas will be necessary.
It was a challenge to develop a definition for identifying that an intervention was truly structural and then to create a taxonomy that was able to encompass all structural interventions identified in our review. Our definition of structural interventions necessitates that exposure to the intervention is outside of the control of the person affected. For example, small-group interventions are not considered structural, as people self-select into group interventions and are thus in control of the receipt of the intervention. The distinction is that of personal agency (i.e., individuals controlling their own actions). We did include interventions that required some personal agency, as in the case of individuals using syringe exchange programs, because the environment is changed in a way that is not under the control of the involved person. By contrast, an example that would be excluded is a community-level intervention with no structural components. Even though these interventions are delivered in community settings, most also feature significant one-on-one transactions (e.g., Popular Opinion Leader and Community PROMISE) or small group risk-reduction meetings (e.g., Voices/Voces) [22,23,24]. Thus, interventions with a large reach do not necessarily meet the criteria as structural interventions unless the intervention entails an environmental change. Lastly, small communication media, such as brochures or pamphlets, even if they have a large reach, do not translate to structural change unless they change the environment.
Limitations
Our taxonomy may not be broad enough to apply to structural interventions reported for other health conditions. While we were highly inclusive in allowing less rigorously evaluated studies to be included, there are many interventions that are structural in nature that have not been evaluated. On the other hand, there may be some structural intervention evaluations not included in this study that report outcomes not directly related to HIV, but in theory could impact HIV risk. Lastly, we did not quantify the effectiveness of these interventions, nor did we assess in detail the quality of studies. Examining these dimensions in future studies will enhance the usefulness of the findings reported here.
Conclusions
To our knowledge, this is the first time a framework for structural interventions in HIV prevention has yielded a comprehensive, well-defined taxonomy of structural interventions. The taxonomy may move the field toward a more precise and shared language for discussing these types of interventions. It can be used to develop further generalizations about different types of interventions, as well as providing insight into the gaps in research in various categories within the taxonomy.
References
Office of National AIDS Policy. National HIV/AIDS Strategy for the United States: Updated to 2020.2015 cited November 9, 2015]. https://www.aids.gov/federal-resources/national-hiv-aids-strategy/nhas-update.pdf.
Sweat MD, Denison JA. Reducing HIV incidence in developing countries with structural and environmental interventions. AIDS. 1995;9(Suppl A):S251–7.
Blankenship KM, Bray SJ, Merson MH. Structural interventions in public health. AIDS. 2000;14(Suppl 1):S11–21.
Sumartojo E. Structural factors in HIV prevention: concepts, examples, and implications for research. AIDS. 2000;14(Suppl 1):S3–10.
Cohen DA, Scribner R. An STD/HIV prevention intervention framework. AIDS Patient Care STDS. 2000;14(1):37–45.
Blankenship KM, Friedman SR, Dworkin S, Mantell JE. Structural interventions: concepts, challenges and opportunities for research. J Urban Health. 2006;83(1):59–72.
Tsai AC. A typology of structural approaches to HIV prevention: a commentary on Roberts and Matthews. Soc Sci Med. 2012;75(9):1562–7 discussion 8–71.
Kaufman MR, Cornish F, Zimmerman RS, Johnson BT. Health behavior change models for HIV prevention and AIDS care: practical recommendations for a multi-level approach. J Acquir Immune Defic Syndr. 2014;66(Suppl 3):S250–8.
Adimora AA, Auerbach JD. Structural interventions for HIV prevention in the United States. J Acquir Immune Defic Syndr. 2010;55(Suppl 2):S132–5.
Des Jarlais DC. Structural interventions to reduce HIV transmission among injecting drug users. AIDS. 2000;14(Suppl 1):S41–6.
Gupta GR, Parkhurst JO, Ogden JA, Aggleton P, Mahal A. Structural approaches to HIV prevention. Lancet. 2008;372(9640):764–75.
Parker RG, Easton D, Klein CH. Structural barriers and facilitators in HIV prevention: a review of international research. AIDS. 2000;14(Suppl 1):S22–32.
Parkhurst JO. HIV prevention, structural change and social values: the need for an explicit normative approach. J Int AIDS Soc. 2012;15(Suppl 1):1–10.
DeLuca JB, Mullins MM, Lyles CM, Crepaz N, Kay K, Thadiparthi S. Developing a comprehensive search strategy for evidence based systematic reviews. Evid Based Libr Inf Pract. 2008;3(1):3–32.
PsycINFO. Wolters Kluwer. 1988 [cited November 9, 2015]. http://www.ovid.com/site/.
EMBASE. Wolters Kluwer. 1988 [cited November 9, 2015]. http://www.ovid.com/site/?cmpid=Database%2520Landing:%2520RecomendMedicine%2520-%2520Embase.
MEDLINE. Wolters Kluwer. 1988 [cited November 9, 2015]. http://gateway.ovid.com/autologin.html.
Sociological Abstracts. ProQuest. 2012 [cited November 9, 2015]. http://www.proquest.com/products-services/socioabs-set-c.html.
Centers for Disease Control and Prevention. Diagnoses of HIV infection in the United States and dependent areas, 2013. HIV Surveill Rep. 2013;25:1–82.
Purcell DW, McCray E, Mermin J. The shift to high-impact HIV prevention by health departments in the United States. Public Health Rep. 2016;131(1):7–10.
Frieden TR. A framework for public health action: the health impact pyramid. Am J Public Health. 2010;100(4):590–5.
Centers for Disease Control and Prevention. (CDC) AIDS Community Demonstration Projects Research Group. Community-level HIV intervention in 5 cities: final outcome data from the CDC AIDS Community Demonstration Projects. Am J Public Health. 1999;89(3):336–45.
Kelly JA, Murphy DA, Sikkema KJ, McAuliffe TL, Roffman RA, Solomon LJ, et al. Randomised, controlled, community-level HIV-prevention intervention for sexual-risk behaviour among homosexual men in US cities. Community HIV prevention research collaborative. Lancet. 1997;350(9090):1500–5.
Neumann MS, O’Donnell L, Doval AS, Schillinger J, Blank S, Ortiz-Rios E, et al. Effectiveness of the VOICES/VOCES sexually transmitted disease/human immunodeficiency virus prevention intervention when administered by health department staff: does it work in the “real world”? Sex Transm Dis. 2011;38(2):133–9.
Ajuwon A, Funmilayo F, Oladepo O, Osungbade K, Asuzu M. Effects of training programme on HIV/AIDS prevention among primary health care workers in Oyo State, Nigeria. Health Educ. 2008;108(6):463–74.
Alamo ST, Wagner GJ, Sunday P, Wanyenze RK, Ouma J, Kamya M, et al. Electronic medical records and same day patient tracing improves clinic efficiency and adherence to appointments in a community based HIV/AIDS care program, Uganda. AIDS Behav. 2012;16(2):368–74.
Alstead M, Campsmith M, Halley CS, Hartfield K, Goldbaum G, Wood RW. Developing, implementing, and evaluating a condom promotion program targeting sexually active adolescents. AIDS Educ Prev. 1999;11(6):497–512.
Anderko L, Robertson JF, Uscian MM. The effectiveness of a rural nursing center in improving health care access in a three-county area. J Rural Health. 2000;16(2):177–84.
Baird SJ, Garfein RS, McIntosh CT, Ozler B. Effect of a cash transfer programme for schooling on prevalence of HIV and herpes simplex type 2 in Malawi: a cluster randomised trial. Lancet. 2012;379(9823):1320–9.
Bardsley J, Turvey J, Blatherwick J. Vancouver’s needle exchange program. Can J Public Health. 1990;81(1):39–45.
Basu I, Jana S, Rotheram-Borus MJ, Swendeman D, Lee S, Newman P, et al. HIV prevention among sex workers in India. J Acquir Immune Defic Syndr. 2004;36(3):845–52.
Batavia AS, Balaji K, Houle E, Parisaboina S, Ganesh AK, Mayer KH, et al. Adherence to antiretroviral therapy in patients participating in a graduated cost recovery program at an HIV care center in South India. AIDS Behav. 2010;14(4):794–8.
Blake SM, Ledsky R, Goodenow C, Sawyer R, Lohrmann D, Windsor R. Condom availability programs in Massachusetts high schools: relationships with condom use and sexual behavior. Am J Public Health. 2003;93(6):955–62.
Blank S, Gallagher K, Washburn K, Rogers M. Reaching out to boys at bars: utilizing community partnerships to employ a wellness strategy for syphilis control among men who have sex with men in New York City. Sex Transm Dis. 2005;32(10 Suppl):S65–72.
Blankenship KM, West BS, Kershaw TS, Biradavolu MR. Power, community mobilization, and condom use practices among female sex workers in Andhra Pradesh. India. AIDS. 2008;22(Suppl. 5):S109–16.
Bollen LJ, Anartati AS, Morineau G, Sulami S, Prabawanti C, Silfanus FJ, et al. Addressing the high prevalence of gonorrhoea and chlamydia among female sex workers in Indonesia: results of an enhanced, comprehensive intervention. Sex Transm Infect. 2010;86(1):61–5.
Bortolotti F, Stivanello A, Noventa F, Forza G, Pavanello N, Bertolini A. Sustained AIDS education campaigns and behavioural changes in Italian drug abusers. Eur J Epidemiol. 1992;8(2):264–7.
Boulay M, Tweedie I, Fiagbey E. The effectiveness of a national communication campaign using religious leaders to reduce HIV-related stigma in Ghana. Afr J AIDS Res. 2008;7(1):133–41.
Bowles KE, Clark HA, Tai E, Sullivan PS, Song B, Tsang J, et al. Implementing rapid HIV testing in outreach and community settings: results from an advancing HIV prevention demonstration project conducted in seven U.S. cities. Public Health Rep. 2008;123(Suppl 3):78–85.
Brooks L, Rietmeijer CA, McEwen D, Subiadur JA, Mettenbrink CJ. Normalizing HIV testing in a busy urban sexually transmitted infections clinic. Sex Transm Dis. 2009;36(3):127–8.
Brown NL, Luna V, Ramirez MH, Vail KA, Williams CA. Developing an effective intervention for IDU women: a harm reduction approach to collaboration. AIDS Educ Prev. 2005;17(4):317–33.
Brown J, Shesser R, Simon G, Bahn M, Czarnogorski M, Kuo I, et al. Routine HIV screening in the emergency department using the new US Centers for Disease Control and Prevention Guidelines: results from a high-prevalence area. J Acquir Immune Defic Syndr. 2007;46(4):395–401.
Buchanan D, Kee R, Sadowski LS, Garcia D. The health impact of supportive housing for HIV-positive homeless patients: a randomized controlled trial. Am J Public Health. 2009;99(Suppl 3):S675–80.
Bull SS, Posner SF, Ortiz C, Beaty B, Benton K, Lin L, et al. POWER for reproductive health: results from a social marketing campaign promoting female and male condoms. J Adolesc Health. 2008;43(1):71–8.
Busza J, Baker S. Protection and participation: an interactive programme introducing the female condom to migrant sex workers in Cambodia. AIDS Care. 2004;16(4):507–18.
Casalino E, Bernot B, Bouchaud O, Alloui C, Choquet C, Bouvet E, et al. Twelve months of routine HIV screening in 6 emergency departments in the Paris area: results from the ANRS URDEP study. PLoS ONE. 2012;7(10):e46437.
Centers for Disease Control and Prevention. (CDC) AIDS Community Demonstration Projects Research Group. Community-level HIV intervention in 5 cities: final outcome data from the CDC AIDS Community Demonstration Projects. Am J Public Health. 1999;89(3):336–45.
Cervantes RC, Kappos B, Duenas N, Arellano D. Culturally focused HIV prevention and substance abuse treatment for Hispanic women. Addict Disord Their Treat. 2003;2(3):69–77.
Chan AK, Mateyu G, Jahn A, Schouten E, Arora P, Mlotha W, et al. Outcome assessment of decentralization of antiretroviral therapy provision in a rural district of Malawi using an integrated primary care model. Trop Med Int Health. 2010;15(Suppl 1):90–7.
Charalambous S, Innes C, Muirhead D, Kumaranayake L, Fielding K, Pemba L, et al. Evaluation of a workplace HIV treatment programme in South Africa. AIDS. 2007;21(Suppl. 3):S73–8.
Chiao C, Morisky DE, Ksobiech K, Malow RM. Promoting HIV testing and condom use among Filipina commercial sex workers: findings from a quasi-experimental intervention study. AIDS Behav. 2009;13(5):892–901.
Chipfakacha V. Prevention of sexually transmitted disease: the Shurugwi sex-workers project. S Afr Med J. 1993;83(1):40–1.
Christopoulos KA, Kaplan B, Dowdy D, Haller B, Nassos P, Roemer M, et al. Testing and linkage to care outcomes for a clinician-initiated rapid HIV testing program in an urban emergency department. AIDS Patient Care STDS. 2011;25(7):439–44.
Cohen DA, Farley TA, Bedimo-Etame JR, Scribner R, Ward W, Kendall C, et al. Implementation of condom social marketing in Louisiana, 1993 to 1996. Am J Public Health. 1999;89(2):204–8.
Conkling M, Shutes EL, Karita E, Chomba E, Tichacek A, Sinkala M, et al. Couples voluntary counseling and testing and nevirapine use in antenatal clinics in two African capitals: a prospective cohort study. J Int AIDS Soc. 2010;13:10.
Cunningham CO, Shapiro S, Berg KM, Sacajiu G, Paccione G, Goulet JL. An evaluation of a medical outreach program targeting unstably housed HIV-infected individuals. J Health Care Poor Underserved. 2005;16(1):127–38.
Davila JA, Miertschin N, Sansgiry S, Schwarzwald H, Henley C, Giordano TP. Centralization of HIV services in HIV-positive African-American and Hispanic youth improves retention in care. AIDS Care. 2013;25(2):202–6.
de Vroome EM, Paalman ME, Sandfort TG, Sleutjes M, de Vries KJ, Tielman RA. AIDS in The Netherlands: the effects of several years of campaigning. Int J STD AIDS. 1990;1(4):268–75.
Dennison B, Kennedy J, Tilling K, Wolfe CD, Chrystie IL, Banatvala JE. Feasibility of named antenatal HIV screening in an inner city population. AIDS Care. 1998;10(3):259–65.
Du P, Camacho F, Zurlo J, Lengerich EJ. Human immunodeficiency virus testing behaviors among US adults: the roles of individual factors, legislative status, and public health resources. Sex Transm Dis. 2011;38(9):858–64.
Egger M, Pauw J, Lopatatzidis A, Medrano D, Paccaud F, Smith GD. Promotion of condom use in a high-risk setting in Nicaragua: a randomised controlled trial. Lancet. 2000;355(9221):2101–5.
Elkins D, Maticka-Tyndale E, Kuyyakanond T, Miller P, Haswell-Elkins M. Toward reducing the spread of HIV in northeastern Thai villages: evaluation of a village-based Intervention. AIDS Educ Prev. 1997;9(1):49–69.
Eloundou-Enyegue PM, Meekers D, Calves AE. From awareness to adoption: the effect of AIDS education and condom social marketing on condom use in Tanzania (1993-1996). J Biosoc Sci. 2005;37(3):257–68.
Feldman J, Miner M, Millis M. Training family practice residents in HIV care. AIDS Patient Care STDS. 2004;18(7):395–404.
Figueroa JP, Weir SS, Byfield L, Hall A, Cummings SM, Suchindran CM. The challenge of promoting safe sex at sites where persons meet new sex partners in Jamaica: results of the Kingston PLACE randomized controlled trial. Trop Med Int Health. 2010;15(8):945–54.
Fisher JD, Amico KR, Fisher WA, Cornman DH, Shuper PA, Trayling C, et al. Computer-based intervention in HIV clinical care setting improves antiretroviral adherence: the LifeWindows Project. AIDS Behav. 2011;15(8):1635–46.
Ford K, Wirawan DN, Fajans P, Meliawan P, MacDonald K, Thorpe L. Behavioral interventions for reduction of sexually transmitted disease/HIV transmission among female commercial sex workers and clients in Bali, Indonesia. AIDS. 1996;10(2):213–22.
Fraze JL, Uhrig JD, Davis KC, Taylor MK, Lee NR, Spoeth S, et al. Applying core principles to the design and evaluation of the ‘Take Charge. Take the Test’ campaign: what worked and lessons learned. Public Health. 2009;123(Suppl 1):e23–30.
Fuller CM, Galea S, Caceres W, Blaney S, Sisco S, Vlahov D. Multilevel community-based intervention to increase access to sterile syringes among injection drug users through pharmacy sales in New York City. Am J Public Health. 2007;97(1):117–24.
Futterman DC, Peralta L, Rudy BJ, Wolfson S, Guttmacher S, Rogers AS. The ACCESS (adolescents connected to care, evaluation, and special services) Project: social marketing to promote HIV testing to adolescents, methods and first year results from a six city campaign. J Adolesc Health. 2001;29(3 Suppl. 1):19–29.
Gao MY, Wang S. Participatory communication and HIV/AIDS prevention in a Chinese marginalized (MSM) population. AIDS Care. 2007;19(6):799–810.
Garcia PJ, Holmes KK, Carcamo CP, Garnett GP, Hughes JP, Campos PE, et al. Prevention of sexually transmitted infections in urban communities (Peru PREVEN): a multicomponent community-randomised controlled trial. Lancet. 2012;379(9821):1120–8.
Ghys PD, Diallo MO, Ettiegne-Traore V, Kale K, Tawil O, Carael M, et al. Increase in condom use and decline in HIV and sexually transmitted diseases among female sex workers in Abidjan, Cote d’Ivoire, 1991–1998. AIDS. 2002;16(2):251–8.
Gibson DR, Zhang G, Cassady D, Pappas L, Mitchell J, Kegeles SM. Effectiveness of HIV prevention social marketing with injecting drug users. Am J Public Health. 2010;100(10):1828–30.
Godin G, Naccache H, Cote F, Leclerc R, Frechette M, Alary M. Promotion of safe sex: evaluation of a community-level intervention programme in gay bars, saunas and sex shops. Health Educ Res. 2008;23(2):287–97.
Goetz MB, Hoang T, Bowman C, Knapp H, Rossman B, Smith R, et al. A system-wide intervention to improve HIV testing in the Veterans Health Administration. J Gen Intern Med. 2008;23(8):1200–7.
Goetz MB, Hoang T, Henry SR, Knapp H, Anaya HD, Gifford AL, et al. Evaluation of the sustainability of an intervention to increase HIV testing. J Gen Intern Med. 2009;24(12):1275–80.
Golden MR, Rompalo AM, Fantry L, Bein M, Perkins T, Hoover DR, et al. Early intervention for human immunodeficiency virus in Baltimore sexually transmitted diseases clinics: impact on gonorrhea incidence in patients infected with HIV. Sex Transm Dis. 1996;23(5):370–7.
Gomez CA, Hernandez M, Faigeles B. Sex in the new world: an empowerment model for HIV prevention in Latina immigrant women. Health Educ Behav. 1999;26(2):200–12.
Grabbe KL, Menzies N, Taegtmeyer M, Emukule G, Angala P, Mwega I, et al. Increasing access to HIV counseling and testing through mobile services in Kenya: strategies, utilization, and cost-effectiveness. J Acquir Immune Defic Syndr. 2010;54(3):317–23.
Gray J. Operating needle exchange programmes in the hills of Thailand. AIDS Care. 1995;7(4):489–99.
Greenwald JL, Hall J, Skolnik PR. Approaching the CDC’s guidelines on the HIV testing of inpatients: physician-referral versus nonreferral-based testing. AIDS Patient Care STDS. 2006;20(5):311–7.
Gregson S, Adamson S, Papaya S, Mundondo J, Nyamukapa CA, Mason PR, et al. Impact and process evaluation of integrated community and clinic-based HIV-1 control: a cluster-randomised trial in eastern Zimbabwe. PLoS Med. 2007;4(3):e102.
Griffith DM, Pichon LC, Campbell B, Allen JO. YOUR Blessed Health: a faith-based CBPR approach to addressing HIV/AIDS among African Americans. AIDS Educ Prev. 2010;22(3):203–17.
Grimes RM, Courtney CC, Vindekilde J. A collaborative program between a school of public health and a local health department to increase HIV testing of pregnant women. Public Health Rep. 2001;116(6):585–9.
Grosskurth H, Mosha F, Todd J, Mwijarubi E, Klokke A, Senkoro K, et al. Impact of improved treatment of sexually transmitted diseases on HIV infection in rural Tanzania: randomised controlled trial [see comment]. Lancet. 1995;346(8974):530–6.
Guttmacher S, Lieberman L, Ward D. Does access to condoms influence adolescent sexual behavior? AIDS Reader. 1998;8(4):201–5.
Guy R, Goller J, Leslie D, Thorpe R, Grierson J, Batrouney C, et al. No increase in HIV or sexually transmissible infection testing following a social marketing campaign among men who have sex with men. J Epidemiol Community Health. 2009;63(5):391–6.
Guydish J, Bucardo J, Young M, Woods W, Grinstead O, Clark W. Evaluating needle exchange: are there negative effects? AIDS. 1993;7(6):871–6.
Hagan H, Des Jarlais DC, Purchase D, Friedman SR, Reid T, Bell TA. An interview study of participants in the Tacoma, Washington, syringe exchange. Addiction. 1993;88(12):1691–7.
Hammett TM, Kling R, Johnston P, Liu W, Ngu D, Friedmann P, et al. Patterns of HIV prevalence and HIV risk behaviors among injection drug users prior to and 24 months following implementation of cross-border HIV prevention interventions in Northern Vietnam and Southern China. AIDS Educ Prev. 2006;18(2):97–115.
Handy P, Pattman RS, Richards J. ‘I’m OK?’ Evaluation of a new walk-in quick-check clinic [see comment]. Int J STD AIDS. 2006;17(10):677–80.
Hanenberg RS, Rojanapithayakorn W, Kunasol P, Sokal DC. Impact of Thailand’s HIV-control programme as indicated by the decline of sexually transmitted diseases. Lancet. 1994;344(8917):243–5.
Harris JB, Hatwiinda SM, Randels KM, Chi BH, Kancheya NG, Jham MA, et al. Early lessons from the integration of tuberculosis and HIV services in primary care centers in Lusaka, Zambia. Int J Tuberc Lung Dis. 2008;12(7):773–9.
Hart GJ, Carvell A, Woodward N, Johnson AM, Williams P, Parry JV. Evaluation of needle exchange in central London: behaviour change and anti-HIV status over one year. AIDS. 1989;3(5):261–5.
Harte D, Hamill M, Edwards SG, Copas AJ, Minton J, Jones VL, et al. Evaluation of a home-delivery service for HIV-infected patients attending an inner London HIV treatment centre. Int J STD AIDS. 2008;19(8):533–5.
Haukoos JS, Hopkins E, Eliopoulos VT, Byyny RL, Laperriere KA, Mendoza MX, et al. Development and implementation of a model to improve identification of patients infected with HIV using diagnostic rapid testing in the emergency department. Acad Emerg Med. 2007;14(12):1149–57.
Henderson KC, Hindman J, Johnson SC, Valuck RJ, Kiser JJ. Assessing the effectiveness of pharmacy-based adherence interventions on antiretroviral adherence in persons with HIV. AIDS Patient Care STDS. 2011;25(4):221–8.
Henry SR, Goetz MB, Asch SM. The effect of automated telephone appointment reminders on HIV primary care no-shows by veterans. J Assoc Nurses AIDS Care. 2012;23(5):409–18.
Herbert R, Ashraf A, Yates T, Spriggs K, Malinnag M, Durward-Brown E, et al. Nurse-delivered universal point-of-care testing for HIV in an open-access returning traveller clinic. HIV Med. 2012;13(8):499–504.
Hightow-Weidman LB, Smith JC, Valera E, Matthews DD, Lyons P. Keeping them in “STYLE”: finding, linking, and retaining young HIV-positive Black and Latino men who have sex with men in care. AIDS Patient Care STDS. 2011;25(1):37–45.
Hirsch JD, Rosenquist A, Best BM, Miller TA, Gilmer TP. Evaluation of the first year of a pilot program in community pharmacy: HIV/AIDS medication therapy management for Medi-Cal beneficiaries. J Manag Care Pharm. 2009;15(1):32–41.
Hogben M, Chesson H, Aral SO. Sexuality education policies and sexually transmitted disease rates in the United States of America. Int J STD AIDS. 2010;21(4):293–7.
Holman S, Sorin MD, Crossette J, LaChance-McCullough ML. State program for postpartum HIV counseling and testing. Public Health Rep. 1994;109(4):521–9.
Hsieh YH, Jung JJ, Shahan JB, Pollack HA, Hairston HS, Moring-Parris D, et al. Outcomes and cost analysis of 3 operational models for rapid HIV testing services in an academic inner-city emergency department. Ann Emerg Med. 2011;58(1 Suppl. 1):S133–9.
Jacob Arriola KR, Braithwaite RL, Holmes NE, Fortenberry RM. Post-release case management services and health-seeking behavior among HIV-infected ex-offenders. J Health Care Poor Underserved. 2007;18(3):665–74.
Jana S, Bandyopadhyay N, Mukherjee S, Dutta N, Basu I, Saha A. STD/HIV intervention with sex workers in West Bengal, India. AIDS. 1998;12:S101–8.
Javanbakht M, Murphy R, Harawa NT, Smith LV, Hayes M, Chien M, et al. Sexually transmitted infections and HIV prevalence among incarcerated men who have sex with men, 2000-2005. Sex Transm Dis. 2009;36(Suppl. 2):S17–21.
Kagimu M, Marum E, Wabwire-Mangen F, Nakyanjo N, Walakira Y, Hogle J. Evaluation of the effectiveness of AIDS health education interventions in the Muslim community in Uganda. AIDS Educ Prev. 1998;10(3):215–28.
Kamali A, Quigley M, Nakiyingi J, Kinsman J, Kengeya-Kayondo J, Gopal R, et al. Syndromic management of sexually-transmitted infections and behaviour change interventions on transmission of HIV-1 in rural Uganda: a community randomised trial. Lancet. 2003;361(9358):645–52.
Keating J, Meekers D, Adewuyi A. Assessing effects of a media campaign on HIV/AIDS awareness and prevention in Nigeria: results from the VISION Project. BMC Public Health. 2006;6:123.
Keene J, Stimson GV, Jones S, Parry-Langdon N. Evaluation of syringe-exchange for HIV prevention among injecting drug users in rural and urban areas of Wales. Addiction. 1993;88(8):1063–70.
Kegeles SM, Hays RB, Coates TJ. The Mpowerment Project: a community-level HIV prevention intervention for young gay men. Am J Public Health. 1996;86:1129–36.
Keitz SA, Box TL, Homan RK, Bartlett JA, Oddone EZ. Primary care for patients infected with human immunodeficiency virus: a randomized controlled trial. J Gen Intern Med. 2001;16(9):573–82.
Kennedy MG, Mizuno Y, Seals BF, Myllyluoma J, Weeks-Norton K. Increasing condom use among adolescents with coalition-based social marketing. AIDS. 2000;14(12):1809–18.
Kerr T, Small W, Buchner C, Zhang R, Li K, Montaner J, et al. Syringe sharing and HIV incidence among injection drug users and increased access to sterile syringes. Am J Public Health. 2010;100(8):1449–53.
Kerrigan D, Moreno L, Rosario S, Gomez B, Jerez H, Barrington C, et al. Environmental-structural interventions to reduce HIV/STI risk among female sex workers in the Dominican Republic. Am J Public Health. 2006;96(1):120–5.
Kerrigan D, Telles P, Torres H, Overs C, Castle C. Community development and HIV/STI-related vulnerability among female sex workers in Rio de Janeiro, Brazil. Health Educ Res. 2008;23(1):137–45.
Khumalo-Sakutukwa G, Morin SF, Fritz K, Charlebois ED, Rooyen HV, Chingono A, et al. Project Accept (HPTN 043): a community-based intervention to reduce HIV incidence in populations at risk for HIV in sub-saharan Africa and Thailand. J Acquir Immune Defic Syndr. 2008;49(4):422–31.
Klepp KI, Ndeki SS, Leshabari MT, Hannan PJ, Lyimo BA. AIDS education in Tanzania: promoting risk reduction among primary school children. Am J Public Health. 1997;87(12):1931–6.
Knittel AK, Wren PA, Gore L. Lessons learned from a peri-urban needle exchange. Harm Reduct J. 2010;7:8.1–7.
Ko NY, Lee HC, Hung CC, Chang JL, Lee NY, Chang CM, et al. Effects of structural intervention on increasing condom availability and reducing risky sexual behaviours in gay bathhouse attendees. AIDS Care. 2009;12(12):1499–507.
Kyaddondo D, Wanyenze RK, Kinsman J, Hardon A. Home-based HIV counseling and testing: client experiences and perceptions in Eastern Uganda. BMC Public Health. 2012;12:966.
Landon BE, Wilson IB, McInnes K, Landrum MB, Hirschhorn L, Marsden PV, et al. Effects of a quality improvement collaborative on the outcome of care of patients with HIV infection: the EQHIV study. Ann Intern Med. 2004;140(11):887–96.
Larke N, Cleophas-Mazige B, Plummer ML, Obasi AI, Rwakatare M, Todd J, et al. Impact of the MEMA kwa Vijana adolescent sexual and reproductive health interventions on use of health services by young people in rural Mwanza, Tanzania: results of a cluster randomized trial. J Adolesc Health. 2010;47(5):512–22.
Lauby JL, Smith PJ, Stark M, Person B, Adams J. A community-level HIV prevention intervention for inner-city women: results of the women and infants demonstration projects. Am J Public Health. 2000;90(2):216–22.
Laukamm-Josten U, Mwizarubi BK, Outwater A, Mwaijonga CL, Valadez JJ, Nyamwaya D, et al. Preventing HIV infection through peer education and condom promotion among truck drivers and their sexual partners in Tanzania, 1990–1993. AIDS Care. 2000;12(1):27–40.
Liambila W, Askew I, Mwangi J, Ayisi R, Kibaru J, Mullick S. Feasibility and effectiveness of integrating provider-initiated testing and counselling within family planning services in Kenya. AIDS. 2009;23(Suppl. 1):S115–21.
Lipovsek V, Mukherjee A, Navin D, Marjara P, Sharma A, Roy KP. Increases in self-reported consistent condom use among male clients of female sex workers following exposure to an integrated behaviour change programme in four states in southern India. Sex Transm Infect. 2010;86(Suppl 1):i25–32.
Liu B, Sullivan SG, Wu Z. An evaluation of needle exchange programmes in China. AIDS. 2007;21(Suppl. 8):S123–8.
Lowndes CM, Alary M, Labbe AC, Gnintoungbe C, Belleau M, Mukenge L, et al. Interventions among male clients of female sex workers in Benin, West Africa: an essential component of targeted HIV preventive interventions. Sex Transm Infect. 2007;83(7):577–81.
Luque-Fernandez MA, Van Cutsem G, Goemaere E, Hilderbrand K, Schomaker M, Mantangana N, et al. Effectiveness of patient adherence groups as a model of care for stable patients on antiretroviral therapy in Khayelitsha, Cape Town, South Africa. PLoS ONE. 2013;8(2):e56088.
Macgowan R, Margolis A, Richardson-Moore A, Wang T, Lalota M, French PT, et al. Voluntary rapid human immunodeficiency virus (HIV) testing in jails. Sex Transm Dis. 2009;36(2 Suppl):S9–13.
Magnus M, Jones K, Phillips G II, Binson D, Hightow-Weidman LB, Richards-Clarke C, et al. Characteristics associated with retention among African American and Latino adolescent HIV-positive men: results from the outreach, care, and prevention to engage HIV-seropositive Young MSM of Color Special Project of National Significance Initiative. J Acquir Immune Defic Syndr. 2010;53(4):529–36.
Marcus JL, Bernstein KT, Klausner JD. Updated outcomes of partner notification for human immunodeficiency virus, San Francisco, 2004–2008. AIDS. 2009;23(8):1024–6.
Martinez-Donate AP, Hovell MF, Zellner J, Sipan CL, Blumberg EJ, Carrizosa C. Evaluation of two school-based HIV prevention interventions in the border city of Tijuana, Mexico. J Sex Res. 2004;41(3):267–78.
Martinez-Donate AP, Zellner JA, Sanudo F, Fernandez-Cerdeno A, Hovell MF, Sipan CL, et al. Hombres Sanos: evaluation of a social marketing campaign for heterosexually identified Latino men who have sex with men and women. Am J Public Health. 2010;100(12):2532–40.
Marum E, Morgan G, Hightower A, Ngare C, Taegtmeyer M. Using mass media campaigns to promote voluntary counseling and HIV-testing services in Kenya. AIDS. 2008;22(15):2019–24.
Matovu JK, Kigozi G, Nalugoda F, Wabwire-Mangen F, Gray RH. The Rakai Project counselling programme experience. Trop Med Int Health. 2002;7(12):1064–7.
McCoy HV, Dodds S, Rivers JE, McCoy CB. Case management services for HIV-seropositive IDUs. In: Ashery RS, editor. Progress and issues in case management. Rockville: National Institute on Drug Abuse; 1992. p. 181–207.
McDonald D. The evaluation of a trial of syringe vending machines in Canberra, Australia. Int J Drug Policy. 2009;20(4):336–9.
McOwan A, Gilleece Y, Chislett L, Mandalia S. Can targeted HIV testing campaigns alter health-seeking behaviour? AIDS Care. 2002;14(3):385–90.
Meekers D. The effectiveness of targeted social marketing to promote adolescent reproductive health: the case of Soweto, South Africa. J HIV/AIDS Prev Educ Adolesc Children. 2000;3(4):73–92.
Meekers D, Agha S, Klein M. The impact on condom use of the “100% Jeune” social marketing program in Cameroon. J Adolesc Health. 2005;36(6):530.
Metsch LR, Feaster DJ, Gooden L, Matheson T, Mandler RN, Haynes L, et al. Implementing rapid HIV testing with or without risk-reduction counseling in drug treatment centers: results of a randomized trial. Am J Public Health. 2012;102(6):1160–7.
Meyer L, Job-Spira N, Bouyer J, Bouvet E, Spira A. Prevention of sexually transmitted diseases: a randomised community trial. J Epidemiol Community Health. 1991;45(2):152–8.
Mollen C, Lavelle J, Hawkins L, Ambrose C, Ruby B. Description of a novel pediatric emergency department-based HIV screening program for adolescents. AIDS Patient Care STDS. 2008;22(6):505–12.
Morisky DE, Chiao C, Stein JA, Malow RM. Impact of social and structural influence interventions on condom use and sexually transmited infections among establishment-based female bar workers in the Philippines. J Psychol Human Sex. 2005;17(1–2):45–63.
Morris CN, Cheevers EJ. A package of care for HIV in the occupational setting in Africa: results of a pilot intervention. AIDS Patient Care STDS. 2001;15(12):633–40.
Muñoz M, Bayona J, Sanchez E, Arevalo J, Sebastian JL, Arteaga F, et al. Matching social support to individual needs: a community-based intervention to improve HIV treatment adherence in a resource-poor setting. AIDS Behav. 2011;15(8):1454–64.
Myers JJ, Modica C, Dufour MS, Bernstein C, McNamara K. Routine rapid HIV screening in six community health centers serving populations at risk. J Gen Intern Med. 2009;24(12):1269–74.
Nelson KE, Celentano DD, Eiumtrakol S, Hoover DR, Beyrer C, Suprasert S, et al. Changes in sexual behavior and a decline in HIV infection among young men in Thailand. N Engl J Med. 1996;335(5):297–303.
Ng’weshemi JZ, Boerma JT, Pool R, Barongo L, Senkoro K, Maswe M, et al. Changes in male sexual behaviour in response to the AIDS epidemic: evidence from a cohort study in urban Tanzania. AIDS. 1996;10(12):1415–20.
Nigro L, Casciaro A, Matalone M, Aloisio P, Bruno S, Unit Operators G. Feasibility in needle exchange programme: an evaluation of a pilot programme in Catania, Sicily. Int J Drug Policy. 2000;11(4):299–303.
Odek WO, Busza J, Morris CN, Cleland J, Ngugi EN, Ferguson AG. Effects of micro-enterprise services on HIV risk behaviour among female sex workers in Kenya’s urban slums. AIDS Behav. 2009;13(3):449–61.
O’Leary A, Jemmott LS, Goodhart F, Gebelt J. Effects of an institutional AIDS prevention intervention: moderation by gender. AIDS Educ Prev. 1996;8(6):516–28.
O’Leary A, Kennedy M, Pappas-DeLuca KA, Nkete M, Beck V, Galavotti C. Association between exposure to an HIV story line in The Bold and the Beautiful and HIV-related stigma in Botswana. AIDS Educ Prev. 2007;19(3):209–17.
Olshefsky AM, Zive MM, Scolari R, Zuniga M. Promoting HIV risk awareness and testing in Latinos living on the U.S.-Mexico border: the Tu No Me Conoces social marketing campaign. AIDS Educ Prev. 2007;19(5):422–35.
Papaevangelou G, Roumeliotou A, Kallinikos G, Papoutsakis G, Trichopoulou E, Stefanou T. Education in preventing HIV infection in Greek registered prostitutes. J Acquir Immune Defic Syndr. 1988;1(4):386–9.
Parry MF, Stewart J, Wright P, McLeod GX. Collaborative management of HIV infection in the community: an effort to improve the quality of HIV care. AIDS Care. 2004;16(6):690–9.
Pauw J, Ferrie J, Rivera Villegas R, Medrano Martinez J, Gorter A, Egger M. A controlled HIV/AIDS-related health education programme in Managua, Nicaragua. AIDS. 1996;10(5):537–44.
Peak A, Rana S, Maharjan SH, Jolley D, Crofts N. Declining risk for HIV among injecting drug users in Kathmandu, Nepal: the impact of a harm-reduction programme. AIDS. 1995;9(9):1067–70.
Peltzer K, Seoka P. Evaluation of HIV/AIDS prevention intervention messages on a rural sam- ple of South African youth’s knowledge, attitudes, beliefs and behaviours over a period of 15 months. J Child Adolesc Ment Health. 2004;16(2):93–102.
Pfeiffer J, Montoya P, Baptista AJ, Karagianis M, Pugas MD, Micek M, et al. Integration of HIV/AIDS services into African primary health care: lessons learned for health system strengthening in Mozambique—a case study. J Acquir Immune Defic Syndr. 2010;13:3.1–9.
Proeschold-Bell RJ, Belden CM, Parnell H, Cohen S, Cromwell M, Lombard F. A randomized controlled trial of health information exchange between human immunodeficiency virus institutions. J Public Health Manag Pract. 2010;16(6):521–8.
Pronyk PM, Hargreaves JR, Kim JC, Morison LA, Phetla G, Watts C, et al. Effect of a structural intervention for the prevention of intimate-partner violence and HIV in rural South Africa: a cluster randomised trial. Lancet. 2006;368(9551):1973–83.
Reza-Paul S, Beattie T, Syed HU, Venukumar KT, Venugopal MS, Fathima MP, et al. Declines in risk behaviour and sexually transmitted infection prevalence following a community-led HIV preventive intervention among female sex workers in Mysore, India. AIDS. 2008;22(Suppl. 5):S91–100.
Richardson JL, Milam J, McCutchan A, Stoyanoff S, Bolan R, Weiss J, et al. Effect of brief safer-sex counseling by medical providers to HIV-1 seropositive patients: a multi-clinic assessment. AIDS. 2004;18(8):1179–86.
Richter K, Phillips SC, McInnis AM, Rice DA. Effectiveness of a multi-country workplace intervention in sub-Saharan Africa. AIDS Care. 2011;24(2):180–5.
Robbins GK, Lester W, Johnson KL, Chang Y, Estey G, Surrao D, et al. Efficacy of a clinical decision-support system in an HIV practice: a randomized trial. Ann Intern Med. 2012;157(11):757–66.
Robles RR, Colon HM, Matos TD, Finlinson HA, Munoz A, Marrero CA, et al. Syringe and needle exchange as HIV/AIDS prevention for injection drug users in Puerto Rico. Health Policy. 1998;45(3):209–20.
Rose CD, Courtenay-Quirk C, Knight K, Shade SB, Vittinghoff E, Gomez C, et al. HIV intervention for providers study: a randomized controlled trial of a clinician-delivered HIV risk-reduction intervention for HIV-positive people. J Acquir Immune Defic Syndr. 2010;55(5):572–81.
Rosenberg MS, Seavey BK, Jules R, Kershaw TS. The role of a microfinance program on HIV risk behavior among Haitian women. AIDS Behav. 2011;15(5):911–8.
Ross MW, Chatterjee NS, Leonard L. A community level syphilis prevention programme: outcome data from a controlled trial. Sex Transm Infect. 2004;80(2):100–4.
Ross DA, Changalucha J, Obasi AI, Todd J, Plummer ML, Cleophas-Mazige B, et al. Biological and behavioural impact of an adolescent sexual health intervention in Tanzania: a community-randomized trial. AIDS. 2007;21(14):1943–55.
Rosser BRS. The effects of using fear in public AIDS education on the behaviour of homosexually active men. J Psychol Human Sex. 1991;4(3):123–34.
Sakondhavat C, Sittitrai W, Soontharapa S, Veerawatanatrakul Y, Aryuvatana D, Kukieattikool P. AIDS prevention strategies for rural families in northeastern Thailand. J Med Assoc Thai. 2000;83(10):1175–86.
Sakondhavat C, Werawatanakul Y, Bennett A, Kuchaisit C, Suntharapa S. Promoting condom-only brothels through solidarity and support for brothel managers. Int J STD AIDS. 1997;8(1):40–3.
Schuster MA, Bell RM, Berry SH, Kanouse DE. Impact of a high school condom availability program on sexual attitudes and behaviors. Fam Plann Perspect. 1998;30(2):67–88.
Scott VF, Sitapati A, Martin S, Summers P, Washington M, Daniels F, et al. The Howard University Hospital experience with routineized HIV screening: a progress report. Trans Am Clin Climatol Assoc. 2009;120:429–34.
Sellers DE, McGraw SA, McKinlay JB. Does the promotion and distribution of condoms increase teen sexual activity? Evidence from an HIV prevention program for Latino youth. Am J Public Health. 1994;84(12):1952–9.
Servegev B, Oparina TR, Volkanevskii VL, Broadhead RS, Heckathorn DD, Madray H. HIV prevention in Yaroslavl, Russia: a peer-driven intervention and needle exchange. J Drug Issues. 1999;29(4):777–804.
Shagufta Z, Mahto M. Uptake of HIV testing in a genitourinary medicine clinic following opt-out screening method and uptake rate by individual clinicians. Int J STD AIDS. 2007;18(9):650–1.
Sherer R, Gui X, Zhan F, Teter C, Ping DL, Wykoff RF. Rapid antiretroviral therapy scale-up in Hubei Province, China. Health Affairs. 2008;27(4):1140–7.
Sikkema KJ, Kelly JA, Winett RA, Solomon LJ, Cargill VA, Roffman RA, et al. Outcomes of a randomized community-level HIV prevention intervention for women living in 18 low-income housing developments. Am J Public Health. 2000;90(1):57–63.
Sikkema KJ, Meade CS, Doughty-Berry JD, Zimmerman SO, Kloos B, Snow DL. Community-level HIV prevention for persons with severe mental illness living in supportive housing programs: a pilot intervention study. J Prev Interv Community. 2007;33(1–2):121–35.
Silva A, Glick NR, Lyss SB, Hutchinson AB, Gift TL, Pealer LN, et al. Implementing an HIV and sexually transmitted disease screening program in an emergency department. Ann Emerg Med. 2007;49(5):564–72.
Sirotin N, Strathdee SA, Lozada R, Abramovitz D, Semple SJ, Bucardo J, et al. Effects of government registration on unprotected sex amongst female sex workers in Tijuana, Mexico. Int J Drug Policy. 2010;21(6):466–70.
Sitapati AM, Limneos J, Bonet-Vazquez M, Mar-Tang M, Qin H, Mathews WC. Retention: building a patient-centered medical home in HIV primary care through PUFF (Patients Unable to Follow-up Found). J Health Care Poor Underserved. 2012;23(3 Suppl):81–95.
Smith S, Robinson J, Hollyer J, Bhatt R, Ash S, Shaunak S. Combining specialist and primary health care teams for HIV positive patients: retrospective and prospective studies. BMJ. 1996;312(7028):416–20.
Sood S, Singh PK, Sarwal R. Reaching the underserved: measuring the impact of a community media intervention, Uttar Pradesh, India. Int Q Community Health Educ. 2004;23(2):117–38.
Ssali A, Butler LM, Kabatesi D, King R, Namugenyi A, Kamya MR, et al. Traditional healers for HIV/AIDS prevention and family planning, Kiboga District, Uganda: evaluation of a program to improve practices. AIDS Behav. 2005;9(4):485–93.
Stoltz JA, Wood E, Small W, Li K, Tyndall M, Montaner J, et al. Changes in injecting practices associated with the use of a medically supervised safer injection facility. J Public Health (Oxford). 2007;29(1):35–9.
Sturtevant D, Preiksaitis J, Singh A, Houston S, Gill J, Predy G, et al. The feasibility of using an ‘opt-out’ approach to achieve universal HIV testing of tuberculosis patients in Alberta. Can J Public Health. 2009;100(2):116–20.
Sundaram V, Lazzeroni LC, Douglass LR, Sanders GD, Tempio P, Owens DK. A randomized trial of computer-based reminders and audit and feedback to improve HIV screening in a primary care setting. Int J STD AIDS. 2009;20(8):527–33.
Swaddiwudhipong W, Nguntra P, Chaovakiratipong C, Koonchote S, Lerdlukanavonge P, Chandoun C. Effect of health education and condom promotion on behavioral change among low socioeconomic prostitutes in Mae Sot, Tak, Thailand. Southeast Asian J Trop Med Public Health. 1990;21(3):453–7.
Swendeman D, Basu I, Das S, Jana S, Rotheram-Borus MJ. Empowering sex workers in India to reduce vulnerability to HIV and sexually transmitted diseases. Soc Sci Med. 2009;69(8):1157–66.
Sznitman S, Stanton BF, Vanable PA, Carey MP, Valois RF, Brown LK, et al. Long term effects of community-based STI screening and mass media HIV prevention messages on sexual risk behaviors of African American adolescents. AIDS Behav. 2011;15(8):1755–63.
Tambashe BO, Speizer IS, Amouzou A, Djangone AM. Evaluation of the PSAMAO “Roulez Protege” mass media campaign in Burkina Faso. Prevention du SIDA sur les Axes Migratoires de l’Afrique de l’Ouest. AIDS Educ Prev. 2003;15(1):33–48.
Thielman NM, Chu HY, Ostermann J, Itemba DK, Mgonja A, Mtweve S, et al. Cost-effectiveness of free HIV voluntary counseling and testing through a community-based AIDS service organization in Northern Tanzania. Am J Public Health. 2006;96(1):114–9.
Topp SM, Chipukuma JM, Chiko MM, Wamulume CS, Bolton-Moore C, Reid SE. Opt-out provider-initiated HIV testing and counselling in primary care outpatient clinics in Zambia. Bull World Health Organ. 2011;89(5):328–35.
Topp SM, Li MS, Chipukuma JM, Chiko MM, Matongo E, Bolton-Moore C, et al. Does provider-initiated counselling and testing (PITC) strengthen early diagnosis and treatment initiation? Results from an analysis of an urban cohort of HIV-positive patients in Lusaka, Zambia. J Int AIDS Soc. 2012;15(2):17352.
Torres GW, Heffelfinger JD, Pollack HA, Barrera SG, Rothman RE. HIV screening programs in US emergency departments: a cross-site comparison of structure, process, and outcomes. Ann Emerg Med. 2011;58(1 Suppl. 1):S104–13.
Tripiboon D. A HIV/AIDS prevention program for married women in rural northern Thailand. Aust J Prim Health. 2001;7(3):83–91.
Tyden T, Bjorkelund C, Odlind V, Olsson SE. Increased use of condoms among female university students: a 5-year follow-up of sexual behavior. Acta Obstet Gynecol Scand. 1996;75(6):579–84.
Ubaidullah M. Social vaccine for HIV prevention: a study on truck drivers in South India. Soc Work Health Care. 2004;39(3–4):399–414.
Underwood C, Hachonda H, Serlemitsos E, Bharath-Kumar U. Reducing the risk of HIV transmission among adolescents in Zambia: psychosocial and behavioral correlates of viewing a risk-reduction media campaign. J Adolesc Health. 2006;38(1):55.
Uys L, Chirwa M, Kohi T, Greeff M, Naidoo J, Makoae L, et al. Evaluation of a health setting-based stigma intervention in five African countries. AIDS Patient Care STDS. 2009;23(12):1059–66.
Van der Bij AK, Dukers NH, Coutinho RA, Fennema HS. Low HIV-testing rates and awareness of HIV infection among high-risk heterosexual STI clinic attendees in The Netherlands. Eur J Pub Health. 2008;18(4):376–9.
Van Rossem R, Meekers D. An evaluation of the effectiveness of targeted social marketing to promote adolescent and young adult reproductive health in Cameroon. AIDS Educ Prev. 2000;12(5):383–404.
Vaughan PW, Rogers EM, Singhal A, Swalehe RM. Entertainment-education and HIV/AIDS prevention: a field experiment in Tanzania. J Health Commun. 2000;5(Suppl):81–100.
Vernon R, Ojeda G, Murad R. Incorporating AIDS prevention activities into a family planning organization in Colombia. Stud Fam Plann. 1990;21(6):335–43.
Virga PH, Jin B, Thomas J, Virodov S. Electronic health information technology as a tool for improving quality of care and health outcomes for HIV/AIDS patients. Int J Med Inform. 2012;81(10):e39–45.
Visrutaratna S, Lindan CP, Sirhorachai A, Mandel JS. ‘Superstar’ and ‘model brothel’: developing and evaluating a condom promotion program for sex establishments in Chiang Mai, Thailand. AIDS. 1995;9(Suppl. 1):S69–75.
Visser MJ, Schoeman JB, Perold JJ. Evaluation of HIV/AIDS prevention in South African schools. J Health Psychol. 2004;9(2):263–80.
Vu Thuong N, Van Nghia K, Phuc Hau T, Thanh Long N, Van Thi Bao C, Hoang Duc B, et al. Impact of a community sexually transmitted infection/HIV intervention project on female sex workers in five border provinces of Vietnam. Sex Transm Infect. 2007;83(5):376–82.
Wackett J. A theory-based initiative to reduce the rates of Chlamydia trachomatis infection among young adults in the Yukon. Can J Human Sex. 1998;7(4):347–56.
Walton DA, Farmer PE, Lambert W, Leandre F, Koenig SP, Mukherjee JS. Integrated HIV prevention and care strengthens primary health care: lessons from rural Haiti. J Public Health Policy. 2004;25(2):137–58.
Wang D, Operario D, Hong Q, Zhang H, Coates TJ. Intervention to train physicians in rural China on HIV/STI knowledge and risk reduction counseling: preliminary findings. AIDS Care. 2009;21(4):468–72.
Wang B, Wang QQ, Yin YP, Liang GJ, Jiang N, Gong XD, et al. The effect of a structural intervention for syphilis control among 3597 female sex workers: a demonstration study in South China. J Infect Dis. 2012;206(6):907–14.
Warner L, Klausner JD, Rietmeijer CA, Malotte K, O’Donnell L, Margolis AD, et al. Effect of a brief video intervention on incident infection among patients attending sexually transmitted disease clinics. PLoS Med. 2008;5(6):e135.
Watters JK, Estilo MJ, Clark GL, Lorvick J. Syringe and needle exchange as HIV/AIDS prevention for injection drug users [see comment]. JAMA. 1994;271(2):115–20.
Waxman MJ, Kimaiyo S, Ongaro N, Wools-Kaloustian KK, Flanigan TP, Carter EJ. Initial outcomes of an emergency department rapid HIV testing program in western Kenya. AIDS Patient Care STDS. 2007;21(12):981–6.
Weaver MR, Myaya M, Disasi K, Regoeng M, Matumo HN, Madisa M, et al. Routine HIV testing in the context of syndromic management of sexually transmitted infections: outcomes of the first phase of a training programme in Botswana. Sex Transm Infect. 2008;84(4):259–64.
Wechsberg WM, Smith FJ, Harris-Adeeyo T. AIDS education and outreach to injecting drug users and the community in public housing. Psychol Addict Behav. 1992;6(2):107–13.
Whiters DL, Santibanez S, Dennison D, Clark HW. A case study in collaborating with Atlanta-based African-American churches: a promising means for reaching inner-city substance users with rapid HIV testing. J Evid Based Soc Work. 2010;7(1):103–14.
Williams BG, Taljaard D, Campbell CM, Gouws E, Ndhlovu L, Van Dam J, et al. Changing patterns of knowledge, reported behaviour and sexually transmitted infections in a South African gold mining community. AIDS. 2003;17(14):2099–107.
Wolitski RJ, Kidder DP, Pals SL, Royal S, Aidala A, Stall R, et al. Randomized trial of the effects of housing assistance on the health and risk behaviors of homeless and unstably housed people living with HIV. AIDS Behav. 2010;14(3):493–503.
Wood E, Tyndall MW, Montaner JS, Kerr T. Summary of findings from the evaluation of a pilot medically supervised safer injecting facility [see comment]. CMAJ. 2006;175(11):1399–404.
Wu Z, Detels R, Ji G, Xu C, Rou K, Ding H, et al. Diffusion of HIV/AIDS knowledge, positive attitudes, and behaviors through training of health professionals in China. AIDS Educ Prev. 2002;14(5):379–90.
Wu F, Zhang KL, Shan GL. An HIV/AIDS intervention programme with Buddhist aid in Yunnan Province. Chin Med J (Engl). 2010;123(8):1011–6.
Xiaoming S, Yong W, Choi K, Lurie P, Mandel J. Integrating HIV prevention education into existing family planning services: results of a controlled trial of a community-level intervention for young adults in rural China. AIDS Behav. 2000;4(1):103–10.
Yoder PS, Hornik R, Chirwa BC. Evaluating the program effects of a radio drama about AIDS in Zambia. Stud Fam Plann. 1996;27(4):188–203.
Zetola NM, Grijalva CG, Gertler S, Hare CB, Kaplan B, Dowling T, et al. Simplifying consent for HIV testing is associated with an increase in HIV testing and case detection in highest risk groups, San Francisco January 2003–June 2007. PLoS ONE. 2008;3(7):e2591.1–e.9.
Zhongdan C, Schilling RF, Shanbo W, Caiyan C, Wang Z, Jianguo S. The 100% Condom Use Program: a demonstration in Wuhan, China. Eval Program Plann. 2008;31(1):10–21.
Zimmerman MA, Ramirez-Valles J, Suarez E, de la Rosa G, Castro MA. An HIV/AIDS prevention project for Mexican homosexual men: an empowerment approach. Health Educ Behav. 1997;24(2):177–90.
Zimmerman RS, Palmgreen PM, Noar SM, Lustria ML, Lu HY, Horosewski ML. Effects of a televised two-city safer sex mass media campaign targeting high-sensation-seeking and impulsive-decision-making young adults. Health Educ Behav. 2007;34(5):810–26.
Acknowledgements
We thank Lyle McCormick for data analysis; Mary Mullins and Julia DeLuca for conducting the original search in the PRS database and assisting with writing the search strategy section; and Tom Painter, Linda Kay, Juarlyn Gaiter who were involved in early process of defining structural interventions and operationalizing taxonomy. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the U.S. Centers for Disease Control and Prevention.
Funding
This study was supported by the Prevention Research Branch, Division of HIV/AIDS Prevention at the U.S. Centers for Disease Control and Prevention and was not funded by any other organization.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
All the authors declare no conflict of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors as part of the current study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix
Rights and permissions
About this article

Cite this article
Sipe, T.A., Barham, T.L., Johnson, W.D. et al. Structural Interventions in HIV Prevention: A Taxonomy and Descriptive Systematic Review. AIDS Behav 21, 3366–3430 (2017). https://doi.org/10.1007/s10461-017-1965-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-017-1965-5