
Abstract
Pancreatic cancer is one of the most lethal malignancies worldwide. Although the standard of care in pancreatic cancer has improved, prognoses for patients remain poor with a 5-year survival rate of < 5%. Angiogenesis, namely, the formation of new blood vessels from pre-existing vessels, is an important event in tumor growth and hematogenous metastasis. It is a dynamic and complex process involving multiple mechanisms and is regulated by various molecules. Inhibition of angiogenesis has been an established therapeutic strategy for many solid tumors. However, clinical outcomes are far from satisfying for pancreatic cancer patients receiving anti-angiogenic therapies. In this review, we summarize the current status of angiogenesis in pancreatic cancer research and explore the reasons for the poor efficacy of anti-angiogenic therapies, aiming to identify some potential therapeutic targets that may enhance the effectiveness of anti-angiogenic treatments.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pancreatic cancer is one of the most devastating malignancies and ranks fourth among all causes of cancer death in the United States [1]. In 2018, there will be an estimated 55,440 new cases of pancreatic cancer and 44,330 pancreatic cancer-related deaths [2]. Despite wide applications of surgical resection, chemotherapy, and chemoradiotherapy, the long-term prognosis of pancreatic cancer patients remains poor with a median survival time of < 6 months and a 5-year survival of < 5% [3]. Moreover, pancreatic cancer is forecast to surpass prostate, breast, and colorectal cancers to become the second leading cause of cancer death by 2030 [4].
According to different tissue origins, pancreatic cancer can be divided into two major types: those that arise from pancreatic duct epithelium and those that are not pancreatic duct epithelium-derived [5]. The former type mainly refers to pancreatic ductal adenocarcinoma (PDAC) and its variants, including adenosquamous carcinoma, colloid carcinoma, signet ring carcinoma, undifferentiated carcinoma, and undifferentiated carcinoma with osteoclast-like giant cells. They represent over 85% of all pancreatic neoplasms, which we mainly emphasized in this review. The latter type includes acinar cell carcinoma, serous cystadenocarcinoma, mucinous cystadenocarcinoma, intraductal papillary-mucinous carcinoma, pancreatoblastoma, and solid-pseudopapillary carcinoma [5].
PDAC is a mucin-producing and gland-forming tumor that easily invades the lymphovascular system and metastasizes to organs such as the liver [6]. A major pathological feature of PDAC is the abundant deposition of fibrotic stroma caused by intense desmoplasia reaction [7]. This induces elevated interstitial pressure of PDAC and inevitably compresses the blood vessels in the stroma, which renders PDAC with a hypovascular and hypoxic microenvironment. In addition, blood vessel compression inhibits effective drug penetration and uptake, contributing to the lack of efficiency of conventional chemotherapies in PDAC treatment [8]. However, insulinoma is a major type of pancreatic neuroendocrine tumors (PNETs). PNETs originate from mature pancreatic endocrine cells or multipotent stem cells that can differentiate into endocrine cells in the pancreas [9]. Different from PDAC, PNETs exhibit dense vasculature and overexpression of pro-angiogenic factors. This enhanced vascularity is associated with the aggressive behavior of PNETs and makes them more susceptible to vessel-targeted therapies [10]. High response rates and disease control have been observed in patients with PNETs who received vascular targeted drugs such as sunitinib, which suggests possible treatments for pancreatic cancer [11].
Angiogenesis, the process by which new capillaries grow from pre-existing blood vessels, is essential for growth and metastasis of many solid tumors including pancreatic cancer [12]. Angiogenesis is activated when pro-angiogenic molecules predominate over anti-angiogenic molecules [13]. Among the already identified pro-angiogenic molecules, vascular endothelial growth factor A (VEGF-A) is considered as a key mediator of the regulation of pathological blood vessel growth and maintenance. VEGF-A functions as a mitogen for vascular endothelial cells and regulates endothelial cell survival. It is also a potent inducer of vascular permeability and can enhance the mobilization of bone marrow-derived endothelial precursor cells. VEGF-A mediates its pro-angiogenic effects via interactions with vascular endothelial growth factor receptor 1 and 2 (VEGFR-1 and VEGFR-2) and their co-receptors neuropilin-1 and 2 (NRP-1 and NRP-2). Although VEGFR-1 has a 10-fold higher binding affinity to VEGF-A, its subsequent kinase activity in promoting angiogenesis is less than that of VEGFR-2. Therefore, the VEGF-A/VEGFR-2 signaling pathway is commonly regarded as the most important mechanism in vessel formation [14]. VEGF-B and placental growth factor (PGF) are also VEGF family members that both bind to VEGFR-1. The ability of VEGF-B to induce angiogenesis in most tissues is weak. It acts more as a pro-survival, rather than pro-angiogenic, factor. PGF, however, promotes stronger angiogenic responses in multiple tissues. This is somewhat confusing as both growth factors interact with the same type of receptor. However, the specific roles of these growth factors in tumor angiogenesis and progression remain to be validated [15]. VEGF-C and VEGF-D preferentially mediate lymphangiogenesis, rather than angiogenesis, by binding to VEGFR-3. Compared with other VEGF family members, they have received less attention in terms of their roles in tumor vessel formation [16].
As neovascularization is associated with the aggressive nature of malignancies, it is reasonable to retard tumor growth and metastasis by inhibiting angiogenesis. The successes of anti-VEGF therapy in colorectal cancer and other tumor types provide hope for the application of this anti-angiogenic strategy in the treatment of pancreatic cancer [17,18,19]. This article reviews the current understanding of angiogenesis in pancreatic cancer, and further suggests some promising anti-angiogenic therapeutic targets.
Pathways of vessel formation in pancreatic cancer
Sprouting angiogenesis
Sprouting angiogenesis is a ubiquitous mechanism of vessel formation in which a sprout arises from a pre-existing vessel and elongates to form a new vessel. It is a common hallmark in the development of most cancers, including pancreatic cancer [20]. Two basic cell types have been recognized in sprouting angiogenesis, i.e., tip cells and stalk cells. Tip cells are located at the vascular forefront and navigate the microenvironment for angiogenic stimuli with their motile filopodia. Stalk cells align behind the tip cells and proliferate at high rates, by which the sprouting branch is elongated and the process of lumenization is started [20].
The differentiation of tip cells and stalk cells is under tight control by VEGF-A and Notch signaling. As stated above, VEGF-A binds to VEGFR-1 and VEGFR-2 with different affinities and these two receptors exhibit different abilities in promoting angiogenesis. Therefore, different endothelial cells dynamically compete for the tip cell position by changing their relative expressions of VEGFR-1 and VEGFR-2 [21]. Once a tip cell is selected, it then upregulates the expression of Delta-like ligand 4 (DLL4), which binds to Notch receptors in neighboring endothelial cells and suppresses their potential to become new tip cells. When tip cells from two distinct sprouts meet, they communicate with each other through their filopodia and anastomose to form a new vessel branch [21].
Mechanical forces are important in promoting sprouting angiogenesis. Fluid shear stress is a crucial parameter in regulating angiogenic sprouting and continuous blood flow is needed to prevent the already formed vessels from retracting [22].
Intussusceptive angiogenesis
Tumor neovascularization does not occur solely by sprouting angiogenesis, but also through an alternative pattern termed intussusceptive angiogenesis. A typical characteristic of intussusceptive angiogenesis is the formation of an intraluminal pillar [23]. Paku et al. have elucidated a possible mechanism of intraluminal pillar formation consisting of four main steps. (1) Endothelial cells from opposing vascular walls contact with each other and form a transluminal endothelial bridge. (2) Basement membranes on the abluminal side of the bridge-formed endothelial cells are locally degraded and a nearby collagen bundle adheres to the endothelial cell. (3) The collagen bundle extends and reaches the other side of the lumen. (4) Pericytes and myofibroblasts migrate into the collagen pillar and generate connective tissues that promote maturation of the pillar [24]. Following these four steps, the pillar increases in girth and finally splits up the initial vessel forms into two new vessels. This process does not depend primarily on endothelial cell proliferation, and is, therefore, a rapid mechanism for generating new vessels and increasing microvessel density (MVD). Some studies have reported a switch from sprouting to intussusceptive angiogenesis after anti-angiogenic or radiation therapy, which may represent a dynamic adjustment of vessel formation under the stress of the tumor microenvironment [25, 26].
Similar with sprouting angiogenesis, hemodynamic forces, such as increased blood flow and shear stress, play key roles in triggering intussusceptive angiogenesis [27,28,29]. To date, however, the underlying molecular mechanisms involved in this process are poorly understood. VEGF-A is currently the best described pro-angiogenic growth factor and its overexpression has been demonstrated to promote intussusceptive rather than sprouting angiogenesis in the skeletal muscle [30]. In addition, Notch signaling seems to be a negative regulator of intussusceptive angiogenesis as two experiments have collectively shown that disruption of this signaling induces rapid augmentation of vasculature predominantly by intussusceptive angiogenesis [31, 32].
Vessel co-option
Apart from sprouting and intussusceptive angiogenesis, some non-angiogenic types of vascularization have been described in pancreatic cancer. For example, vessel co-option is a mechanism in which tumor cells obtain their blood supply by hijacking and moving along the pre-existing vasculature of the host organ. This mechanism frequently occurs in hypervascular organs such as brain and liver [33, 34]. Using a RIP1-TAG2 pancreatic neuroendocrine tumor mouse model, Franco et al. found that tumors refractory to anti-angiogenic treatment contained blood vessels with abundant α-smooth muscle actin (α-SMA) positive pericytes surrounding them. This subtype of blood vessels was likely to be derived from co-opted vessels, as they were predominantly observed on the tumor/normal pancreas border [35]. To our knowledge, this is the only report that investigated vessel co-option status in pancreatic tumors. In recent years, vessel co-option has been demonstrated to be a prevailing mechanism in different metastatic lesions of tumors regardless of their origins, and it mediates resistance to conventional anti-angiogenic therapies [36, 37]. This partially explains why anti-angiogenic therapy is not as beneficial as we had previously anticipated and emphasizes the necessity of combined inhibition of angiogenesis and vessel co-option in treatment of cancer.
Vasculogenic mimicry (VM)
VM is another non-angiogenic pattern of tumor vascularization. Different from classical endothelium-dependent angiogenesis, VM refers to the highly aggressive and genetically dysregulated cancer cells can mimic endothelial cells and directly form vessel-like fluid-conducting channels due to their high plasticity [38]. VM was first introduced in a melanoma research report [39] and has subsequently been detected in different tumor types [40,41,42,43,44]. Overexpression of VM in pancreatic cancer correlates with poor tumor differentiation, late clinical stage, lymph node metastasis, and is a predictor of poor prognosis [42]. Several molecules have been identified in promoting VM, among which VE-cadherin is the most important. It is an adhesion molecule specifically expressed in endothelial cells that has an active role in VM [43]. Guo et al. administered Ginsenoside Rg3 to nude mice xenografts of pancreatic cancer, resulting in the downregulation of VE-cadherin and significantly reduced VM formation [44]. Mourad-Zeidan et al. demonstrated that highly metastatic melanoma cells could form vasculogenic-like networks on three-dimensional (3D) type I collagen gel, and this effect could be inhibited by the galectin-3 silencing technique, suggesting that galectin-3 contributed to the aggressive phenotype of melanoma partially by mediating tumor VM [45]. In a similar manner, another study showed that the ability of melanoma cells to form VM was significantly suppressed when exposed to high concentrations of genistein, both on 3D type I collagen gels in vitro and in an ectopic mice model of melanoma in vivo. The authors also demonstrated that genistein inhibited the formation of VM by downregulating VE-cadherin [46]. Because VM can be inhibited by different agents, the clinical utility of these agents may be of potential value for further development of effective anti-pancreatic cancer treatments.
Vasculogenesis
Although most tumors form new microvessels by spouting angiogenesis or intussusceptive angiogenesis, evidence has emerged that vasculogenesis also contributes to tumor growth. Vasculogenesis refers to the spontaneous formation of new blood vessels mediated by bone marrow-derived endothelial progenitor cells (EPCs) [47]. In pancreatic cancer, EPCs have been found to be concentrated within cancer tissues, approximately 26-fold higher than that in the normal pancreas [48]. Moreover, EPC counts are closely associated with increased risk of poor prognoses in pancreatic cancer patients, because patients with high EPC counts have significantly shorter survival compared with those who have normal EPC counts [48].
The mobilization, migration, and differentiation of EPCs are complex events involving different molecular pathways. Pro-angiogenic factors released by pancreatic cancer cells, such as VEGF, can attract circulating EPCs to the tumor site, and direct their differentiation into endothelial cells, which are key components of the newly formed vessels, thereby supporting tumor growth and distant metastasis [49, 50]. Sonic Hedgehog (Shh) derived from pancreatic cancer cells also augments migration and the pro-angiogenic function of EPCs by increasing the expression of angiopoietin-1 (Ang-1), stromal cell-derived factor-1 (SDF-1), and insulin-like growth factor-1 (IGF-1) [51, 52]. In addition, CXC chemokine receptor 2 (CXCR2) signaling is important in promoting EPC-mediated vasculogenesis and subsequent tumor growth in pancreatic cancer, as a study showed that vasculogenesis was significantly reduced in a pancreatic tumor-bearing CXCR2 knockout mouse model [53].
The above studies collectively demonstrated that under the stimulation of different pro-angiogenic signals, EPCs home to the tumor area and contribute to tumor development via vasculogenesis. The homing specificity for angiogenic tumor sites of EPCs makes them potential anti-tumor therapeutic targets for inhibiting intratumoral vasculogenesis.
Characteristics of the vasculature in pancreatic cancer
Heterogeneous distribution
Measurement of MVD is an established method for quantitating tumor angiogenesis [54]. Regarding pancreatic cancer, high levels of tumor MVD are associated with larger tumor sizes, higher frequencies of lymph node and distant metastasis, poorer tumor differentiation, and more R0 resection failure [55,56,57].
Analysis of MVD reveals that microvessels are heterogeneously distributed in pancreatic cancer due to two causes. First, MVD in different subtypes of pancreatic cancer are heterogeneous. van der Zee et al. examined two types of pancreatic cancer, pancreatic head and periampullary cancer, and observed a higher MVD in periampullary cancer compared with pancreatic head cancer [58]. The authors attributed this difference to different stem cell origins of the two tumors. This reflected the extent to which the two subtypes of pancreatic cancers rely on angiogenesis to grow. This is not surprising as diffuse types of gastric cancer are less angiogenesis-dependent than intestinal types of gastric cancer [59].
On the other hand, even within a specific type of pancreatic cancer, heterogeneity of vascular distribution exists. Through digital micro-imaging and computerized analyses, Barău et al. showed that MVD in intratumoral areas of pancreatic adenocarcinoma were significantly higher than that in peritumoral areas and normal pancreatic tissue. Furthermore, peritumoral tissues had a higher MVD compared with normal pancreatic tissue [60]. This phenomenon supports the existence of an active angiogenic process in the central tumor, and the tumor may subsequently extend its influence on the surrounding tissues. However, Di Maggio et al. observed that juxta-tumoral stroma (≤ 100 µm from the epithelial cancer component) was hypovascular, and normal pancreas surrounding the tumor was hypervascular compared to the panstromal compartment. They also suggested that stellate cells played a key role in modulating spatial heterogeneity of microvessel distribution in pancreatic cancer [61]. In both aortic ring angiogenesis assays and 3D organotypic cultures, the authors demonstrated a pro-angiogenic feature of activated stellate cells and significant anti-angiogenic influence exerted by pancreatic cancer cells. Moreover, increasing concentrations of collagen could impair the formation of vascular sprouts and compress the microvessels. Therefore, the authors suggested that in the juxta-tumoral area, the anti-angiogenic signaling induced by cancer cells and the deposition of dense extracellular matrix both contributed to its hypovascular feature. However, in the normal pancreas adjacent to the tumor surrounding stroma, activated stellate cells promoted angiogenesis via different molecular mechanisms, which might include the secretion of VEGF and periostin, driving more aggressive cancer behavior.
Poor perfusion
Pancreatic adenocarcinoma, accounting for over 85% of pancreatic cancer, is predominantly characterized by the development of extensive fibrosis termed desmoplasia. Desmoplasia causes abnormally elevated stromal pressure that results in vascular collapse, presented as an almost complete absence of large diameter vessels (> 10 µm) [8]. Compared with normal pancreatic tissue, the blood flow in malignant pancreatic tumors is decreased by approximately 60% [62]. The poor blood perfusion of pancreatic cancer is simultaneously accompanied by impaired drug delivery to the tumor site, which greatly limits the efficacy of conventional chemotherapy [8].
Shh, a soluble ligand expressed by neoplastic cells, signals to fibroblasts in the surrounding stroma and drives the formation of unique desmoplastic microenvironments in pancreatic cancer [63]. Using a genetically engineered mouse model, Olive et al. showed that administration of IPI-926, a Hedgehog signaling inhibitor, produced a dramatic depletion of stromal components paralleled by an increase in intratumoral MVD and intratumoral concentration of gemcitabine, leading to stabilization of the disease [64]. Therefore, inhibiting Hedgehog signaling can serve as a novel tool in the planning of pancreatic cancer treatments targeting the enhancement of effective drug delivery.
Newly identified vascular projections-basal microvilli
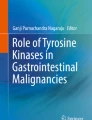
Using thick section immunostaining and 3D construction imaging, Hexige et al. identified a special feature of microvasculature in advanced pancreatic adenocarcinoma. They noticed many “hairy-like” projections on the basal surface of microvessels, which were referred to as “basal microvilli,” measuring approximately 3–41 µm in length and 0.8–1.2 µm in diameter [65] (Fig. 1a). The basal microvilli differed from normal microvessels in three aspects. First, basal microvilli did not express the endothelial cell marker CD31 or the tip cell marker UNC5B, nor did they actively proliferate as they lacked Ki-67 staining. In addition, they had low levels of VEGFR-2 phosphorylation, indicating that they may not depend on the prominent VEGF-A/VEGFR-2 signaling pathway to sustain their growth. Second, basal microvilli contained many glucose transporter-1 (GLUT-1) positive vesicles. Some long projections could transverse the perivascular stroma and connected with tumor epithelium (Fig. 1b). Areas with abundant basal microvilli positively correlated with high glucose uptake as demonstrated by positron emission tomography–computed tomography (PET–CT). The above observations suggested that basal microvilli could enhance glucose trafficking between microvessels and pancreatic tumor cells to help the tumor meet its high glucose needs. Third, basal microvilli only presented in aggressive and metastatic pancreatic tumors, but not in normal pancreas or pancreatic precursor lesions. The emergence of basal microvilli may, therefore, represent a unique phenomenon under pathological, rather than physiological, conditions. From this perspective, basal microvilli add extra diagnostic value and are a promising therapeutic target for pancreatic cancer treatment [65].

Both pictures were quoted from Ref. [65]. a CD34-immunostained 3D image of the basal surface appearance of PDAC microvessels. Basal microvilli are widely distributed across the microvessels, measuring approximately 0.8–1.2 µm in diameter. b Depicts some of the longest basal microvilli that transverse the perivascular stroma and reach the pancreatic neoplastic epithelium. The white arrows points to the basal microvilli, and the white dotted line represents the separation of tumor cells and stroma. Basal microvilli can enhance glucose trafficking between microvessels and pancreatic tumor cells to help the tumor meet its high glucose needs
Impaired microvessel integrity (MVI)
Pericytes serve several important functions for the establishment of normal vasculature. They regulate endothelial cell growth via direct cell–cell contact or paracrine circuits, and contribute to microvessel maturation, stabilization, and remodeling [66, 67]. Therefore, we reviewed the indispensable role of pericytes in maintaining MVI. If MVD represents the quantity of microvessels, then MVI can be deemed a hallmark of the quality of microvessels. Tumor blood vessels in pancreatic cancer typically exhibit low levels of pericyte coverage, namely impaired MVI [68]. Studies indicate that enhancing pancreatic tumor MVI is a key mechanism for normalizing tumor vasculature and inhibiting tumor growth. In a mouse model of pancreatic adenocarcinoma, McCarty et al. showed that overexpression of platelet-derived growth factor BB (PDGF-BB), a key homodimer growth factor involved in stimulating pericyte proliferation and migration, resulted in a significant increase in pericyte coverage of endothelial cells along with decreased tumor volume and improved overall survival (OS) [69]. A recent report by Gilles et al. also revealed that an increase of pericyte coverage was paralleled by enhanced tumor perfusion and reduced hypoxic area in both pancreatic adenocarcinoma and neuroendocrine tumor models. In addition, it also improved the delivery and efficacy of chemotherapeutic drugs [70]. The above studies collectively demonstrate that besides direct targeting of endothelial cell-mediated angiogenesis, focusing on normalization of the tumor vasculature is another potent therapeutic method that may provide clinical benefits for patients.
Wang et al. clarified the relationship between MVI and the prognosis of postoperative patients in hypovascular pancreatic cancer and hypervascular hepatocellular carcinoma. Although perfusion status was distinct, multivariate analyses revealed an identical conclusion that high MVD together with low MVI was predictive of early recurrence, unfavorable metastasis, and short survival after surgical resection in both tumor types [71]. Thus, MVI may provide an important complement to MVD. The quality and quantity of tumor microvessels should be taken into consideration when evaluating the prognoses of patients with pancreatic cancer.
Transcriptional regulation of angiogenesis in pancreatic cancer
Pancreatic cancer angiogenesis is triggered by genetic and epigenetic alterations and a constant evolution of its chaotic microenvironment. The diverse upstream signals seem to converge on limited sets of transcription factors that subsequently transduce those signals to various downstream effector molecules [72]. From this perspective, we may benefit more from targeting a specific transcription factor than solely targeting an upstream or downstream factor. In this section, we focus on the major transcription factors involved in angiogenesis during pancreatic cancer (Fig. 2).

Major transcription factors involved in angiogenesis of pancreatic cancer. Different upstream signals can activate limited sets of transcription factors, which can subsequently bind with DNA and promote the transcription of various pro-angiogenic molecules. NF-κB nuclear factor-κB; Sp specificity protein; STAT3 signal transducer and activator of transcription 3; VEGF vascular endothelial growth factor; VEGFR vascular endothelial growth factor receptor; IL-8 interleukin 8; MMP-2 metalloproteinase 2; COX2 cyclooxygenase 2; CXCL8 chemokine (C-X-C motif) ligand 8; TFs transcription factors; HIF-1α hypoxia-induced factor 1α; COUP-TFII chicken ovalbumin upstream promoter transcription factor type 2; PPARγ peroxisome proliferator-activated receptor γ
Nuclear factor-κB (NF-κB)
NF-κB is a ubiquitous transcription factor that plays critical roles in multiple physiological and pathological processes. Inactive NF-κB resides in the cell cytoplasm and binds with its two inhibitor proteins, IκB-α and IκB-β. Following upstream stimulation, the inhibitor proteins are phosphorylated by IκB kinase and then dissociate from NF-κB, allowing NF-κB to translocate into the nucleus and activate its downstream targets [73]. NF-κB signaling is aberrantly activated in pancreatic cancer and contributes to its malignant phenotype by promoting tumor proliferation, migration, metastasis, anti-apoptotic effects, and epithelial-to-mesenchymal transition (EMT) [74, 75].
In the past decade, accumulating evidence suggests a contributing role for NF-κB in pancreatic tumor angiogenesis. Constitutive activation of NF-κB promotes secretion of pro-angiogenic factors like VEGF-A and chemokine (C-X-C motif) ligand 8 (CXCL8) [76]. Overexpression of G-protein coupled receptor GPR87 is correlated with activation of the NF-κB signaling pathway that enhances pancreatic cancer aggressiveness at least partially by stimulating angiogenesis [77]. Several studies have also shown that blockage of NF-κB signaling, mainly by inhibiting IκB phosphorylation, significantly reduced the expression of angiogenesis-related factors and, therefore, suppressed microvessel formation [78, 79]. Particularly, blocking NF-κB is an effective way to enhance responses to gemcitabine [80]. Thus, inhibition of NF-κB signaling may improve the combining effects of anti-tumor and anti-angiogenic therapies in pancreatic cancer.
Specificity protein (Sp)
Sp belongs to the Sp/Krupel-like factor (KLF) family characterized by the presence of three highly conserved DNA-binding zinc finger domains at the C-terminus and a variable N-terminus with transcriptional regulatory motifs. Sp can be categorized into four subtypes, including Sp1, Sp2, Sp3, and Sp4; all but Sp2 are believed to be essential in tumor angiogenesis [81, 82]. Using RNA interference techniques, Abdelrahim et al. showed that Sp1 and Sp3 were required for transactivation of VEGF-A promoter constructs in pancreatic cancer cells. Moreover, they also demonstrated that Sp4 cooperatively interacted with Sp1 and Sp3 to activate this process [83]. Because VEGF-mediated angiogenesis occurs through binding to specific receptors, two studies showed that Sp could upregulate the expression of VEGFR-1 and VEGFR-2 by binding to GC-rich regions of their promoters [84, 85].
Besides being a direct regulator of angiogenesis-related factors, Sp also regulates the expression of cyclooxygenase 2 (COX2), a key enzyme commonly implicated in chronic inflammation and various malignancies [86]. Inhibition of Sp leads to decreased levels of COX2 that can further suppress angiogenesis via downregulation of VEGF-A, further suggesting an indirect regulatory mechanism between Sp and VEGF-A in pancreatic cancer [86]. The above observations suggest that anti-angiogenic therapy in pancreatic cancer by suppressing the activity of Sp is possible. In fact, some drugs, like celecoxib, tolfenamic acid, and mithramycin, effectively inhibit Sp in different in vitro and in vivo studies [87,88,89].
Signal transducer and activator of transcription 3 (STAT3)
Another major transcription factor that contributes to tumor angiogenesis is STAT3, which is activated through phosphorylation of a conserved tyrosine residue (Y705) by upstream kinases such as JAK2 and c-Src [90, 91]. Once the tyrosine is phosphorylated, two STAT3 monomers form a double-stranded dimer via their Src-homology 2 (SH2) domains, and translocate to the nucleus to regulate transcription of angiogenesis-related target genes [91]. STAT3 activation in pancreatic tumor tissues is significantly higher than that in normal tissues and can promote the expression of VEGF-A, as well as its receptor VEGFR-2 [92, 93]. STAT3 enhances early lymphatic metastasis of pancreatic cancer through VEGF-C [94]. In addition, STAT3 is required for the expression of other angiogenic promoting factors, like interleukin-8 (IL-8) and matrix metalloproteinase 2 (MMP-2) [95, 96]. Administration of FLLL32, a curcumin-derived inhibitor of STAT3 phosphorylation, has been demonstrated to exhibit growth suppressive activity in pancreatic cancer cells by reducing tumor vascularity [97]. Consistent with this, MVD is significantly lower in STAT3-silenced pancreatic tumors compared to that of unsilenced tumors [98].
In recent years, STAT3 was also studied for its potential role in normalizing the vasculature. Studies have demonstrated that endothelial cells treated with STAT3 inhibitors formed abnormal vascular network structures, whereas microvessels in the control group exhibited typical morphologies of normal vasculatures [99]. Other members of the STATs family may also be involved in neovascularization. For example, blockade of STAT5b is accompanied by reduced expression of pro-angiogenic factors in vitro and impaired tumor angiogenesis in vivo [100]. However, their exact roles in pancreatic tumor development including angiogenesis remain to be determined.
Other transcription factors
While the above transcription factors are of utmost importance in angiogenesis of pancreatic cancer, numerous other transcription factors are also important for the regulation of angiogenesis. Sahraei et al. indicated that in pancreatic cancer, Mucin 1 could facilitate nuclear translocation of hypoxia-induced factor 1α (HIF-1α), a well described transcription factor commonly upregulated in hypoxia conditions. This process promoted the expression of platelet-derived growth factor A (PDGF-A), which was one of the many drivers in pancreatic tumor growth, angiogenesis, and metastasis [101]. Polvani et al. demonstrated that silencing of the chicken ovalbumin upstream promoter transcription factor type 2 (COUP-TFII) by shRNA resulted in reduced cell growth and invasiveness of pancreatic tumors, and angiogenesis was strongly inhibited mainly by downregulation of VEGF-C [102]. However, not all transcription factors are pro-angiogenic. For instance, peroxisome proliferator-activated receptor γ (PPARγ) is one of the anti-angiogenic transcription factors that exhibits less impact on the expression of angiogenesis-related molecules once activated by its ligands, such as by pioglitazone [103].
Roles of stromal components in pancreatic tumor angiogenesis
Pancreatic cancer is distinctive from other cancers because of the excessive deposition of stromal matrix. Various stromal components, including non-cellular components and cellular components, are closely associated with the development of pancreatic cancer. In this section, we have reviewed the current studies of different functions of stromal components in pancreatic tumor (Fig. 3), and their impacts on pancreatic tumor angiogenesis (Fig. 4).

Functions of major stromal components in pancreatic cancer. Pancreatic cancer is characterized by an intense stromal desmoplasia reaction surrounding the cancer cells. Both non-cellular and cellular stromal components interact closely with pancreatic tumor cells, providing a specific microenvironment that deeply influences the development of pancreatic cancer. HA hyaluronic acid; EMT epithelial-to-mesenchymal transition; ECM extracellular matrix; MCs mast cells; ECs endothelial cells; PSCs pancreatic stellate cells; TAMs tumor-associated macrophages

Different roles of stromal components in pancreatic cancer angiogenesis. Multiple stromal cells and extracelluar matrix play important roles in stimulating or inhibiting angiogenesis via different pathways in pancreatic cancer. HA hyaluronic acid; IFP interstitial fluid pressure; SS solid stress; ELR− Glu-Leu-Arg−; ELR+ Glu-Leu-Arg+; CXCR2 C-X-C motif chemokine receptor 2; MCs mast cells; TAMs tumor-associated macrophages; MMP-9 metalloproteinase 9; NGAL neutrophil gelatinase associated lipocalin; qPSCs quiescent pancreatic stellate cells; aPSCs activated pancreatic stellate cells; HGF hepatocyte growth factor; Ang-1 angiopoeitin-1; VEGF-A vascular endothelial growth factor A; VEGFR-2 vascular endothelial growth factor receptor 2
Hyaluronic acid (HA)
HA, a non-sulfated glycosaminoglycan composed of repeated N-acetyl glucosamine/glucuronic acid disaccharide units, is highly abundant in the extracellular matrix of pancreatic cancer tissues [104]. Excessive HA deposition has a direct impact on the vascular status of the tumor. In a genetically engineered mouse model of pancreatic cancer, dramatically elevated interstitial fluid pressure (IFP) was detected due to the strong water retention capacity of HA, contributing to compression of tumor blood vessels and impairment of effective drug delivery [8]. Administration of PEGPH20, a PEGylated recombinant hyaluronidase, significantly reduced IFP by ablation of stromal HA, resulting in re-expansion of tumor blood vessels and increased intratumoral concentration of chemotherapeutic agents [8]. This result is in agreement with another study, which apart from confirming the aforementioned observations, also demonstrated that PEGPH20 induced a hyperpermeability phenotype of the pancreatic tumor vasculature by formation of fenestrations and inter-endothelial junctional gaps of tumor vessels [105].
Both studies suggested an effective way of improving pharmacological delivery by means of stromal depletion and, therefore, re-expanded tumor blood vessels. However, whether this innovative strategy can be translated into improved clinical outcomes for pancreatic cancer patients remains to be determined. In a phase Ib clinical trial, combination of PEGPH20 with gemcitabine improved both OS and progression-free survival (PFS) in patients with advanced pancreatic adenocarcinoma, especially those with high HA levels [106]. Other ongoing clinical trials include nab-paclitaxel plus gemcitabine (NCT01839487) or FOLFIRINOX (NCT01959139) with or without PEGPH20 in metastatic pancreatic cancer patients. In addition, some promising HA-targeting agents, such as Minnelide and 4-MU, have already been identified [107, 108]. Of particular note, HA was found to be present at a comparable level in primary and metastatic pancreatic tumor lesions, which strongly indicated that metastatic lesions may also potentially benefit from HA depletion therapy [7].
Collagen
Another important non-cellular component of pancreatic tumor stroma is collagen. Collagen contributes to elevated tissue pressure mainly by increasing solid stress (SS) rather than IFP [109]. The deposition of collagen in the extracellular matrix of pancreatic cancer correlates inversely with patent vessel areas. Enzymatic degradation of collagen has been demonstrated to be an effective way of reducing stromal pressure and increasing drug delivery to tumor cells via decompression of the vasculature [109]. A study showed that collagen deposition level was greatly increased after anti-VEGF therapy, which could promote pancreatic tumor spread and disease progression by collagen-mediated signaling [110]. Berchtold et al. reported that among diverse types of collagen, collagen type V (Col V) was capable of affecting tumor angiogenesis [111]. Ablation of Col V by si-RNA impaired tube formation of endothelial cells and, therefore, resulted in reduced MVD in nude mouse models of pancreatic adenocarcinoma. Liver metastatic burden was also significantly diminished, indicating that Col V accelerated the formation of hepatic metastasis at least partially by promoting angiogenesis [111].
Chemokines
Chemokines are indispensable components in the tumor microenvironment. CXCR2, as well as its corresponding ligands, makes up an important biological axis in regulating microvessel formation of pancreatic cancer. The main ligands for CXCR2 include the ELR+ (Glu-Leu-Arg+) CXC-motif chemokines, among which CXCL8 is the most important [112]. Met signaling is essential in remodeling the tumor vasculature by inducing secretion of pro-angiogenic CXCL8 [113]. CXCL8 also cooperates with CXCL12 to promote angiogenesis and invasiveness in pancreatic cancer [114]. In contrast, ELR− (Glu-Leu-Arg−) CXC-motif chemokines such as CXCL14 usually exhibit anti-angiogenic features [115]. The balance between these two groups of chemokines may help determine the propensity for angiogenesis and the progression of tumor growth.
As for CXCR2, a specific genotype of this G protein-coupled receptor (+ 1208T/T) has been identified as a negative predictor of disease-free survival (DFS) in patients with pancreatic cancer [116]. Pharmacological blockade of CXCR2 is linked with reduced MVD, thereby suppressing tumor hematogenous metastasis [117]. In addition, a recent report showed that high level expression of Duffy antigen receptor for chemokines (DARC), a decoy receptor for CXC-motif chemokines, restrained angiogenesis and tumor progression by inhibiting CXCR2-mediated STAT3 activation [118].
Some non-CXC-motif chemokines also promote tumor angiogenesis. Using the KPC mouse model of pancreatic adenocarcinoma, researchers demonstrated that CCL2 could mediate tumor resistance to radiotherapy by recruiting monocytes to support tumor neovascularization [119]. The combination of radiotherapy and simultaneous CCL2 inhibition may improve treatment efficacy. CCL21-CCR7 chemotactic interaction is critical in pancreatic tumor progression. While CCL21 is significantly associated with the formation of microvessels, its receptor, CCR7, is more relevant to lymphangiogenesis and lymph node metastasis in pancreatic cancer [120].
Fibronectin
Fibronectin is a major constituent of the extracellular matrix that mainly binds to cell surface integrins on multiple cell types. The expression of fibronectin is aberrantly elevated in many solid tumors [121]. Among the large integrin family, α5β1 integrin is required for angiogenesis [122]. Although preclinical studies have supported the effectiveness of inhibiting angiogenesis by disrupting interactions between fibronectin and α5β1 [123, 124], clinical outcomes thus far have been discouraging. The most advanced study to date, a phase III clinical trial of a selective αvβ3 and αvβ5 integrin inhibitor Cilengitide, revealed no treatment benefit [125].
Murphy et al. have suggested a possible explanation for the discrepancy between preclinical and clinical results. Using tissue-specific and inducible genetics to delete the α5 and αv subunits in the endothelium of pancreatic tumors, they observed no decrease in MVD or tumor mass. In addition, deletion of fibronectin could not suppress angiogenesis or deposition of the vascular basement membrane [126]. This result is contrary to the current consensus that impeding fibronectin–integrin interactions is the underlying mechanism by which tumor angiogenesis is inhibited. The authors speculated that multiple other integrin-binding proteins in tumor stroma may compensate and support angiogenesis in the absence of fibronectin. However, this hypothesis remains to be validated.
Mast cells (MCs)
MCs are bone marrow derived cells that play critical roles in adaptive immunities and inflammations [127, 128]. They also interact with other stromal cells to regulate the regional microenvironment and promote tumor growth [129]. Regarding pancreatic cancer, infiltrating mast cell count is positively correlated with tumor MVD, indicating their critical roles in angiogenesis [130, 131]. The distribution of MCs in pancreatic tumor tissues is also zone-specific. A study indicated that MCs tended to accumulate in peritumoral and intratumoral border zones rather than in tumor center zones. Specifically, the greatest number of microvessels was also found in tumor border zones, therefore, suggesting the possibility of involvement of MCs in zone-specific remodeling of tumor blood vessels [132].
In a pancreatic islet tumor model, Soucek et al. first observed that Myc activation triggered rapid accumulation of MCs to the tumor mesenchyme, which could further induce macroscopic tumor expansion by facilitating angiogenesis [133]. However, the underlying mechanism of MC-mediated vascularization has not been well elucidated. A recent study revealed a strong positive correlation between serum mast cell tryptase (MCT) levels and MVD. MCT was found to promote proliferation and tube formation of human umbilical vascular endothelial cells (HUVECs). Notably, expression levels of Ang-1 and its receptor Tie-2, which are both pro-angiogenic factors, were significantly enhanced after treatment with MCT in HUVECs [134]. These results together demonstrate that tryptase secreted by MCs can mediate angiogenesis in pancreatic cancer through activation of the Ang-1/Tie-2 pathway. Several studies have also demonstrated similar pro-angiogenic properties of MCT in other malignancies [135, 136]. Hence, administration of tryptase inhibitors such as gabexate mesilate and nafamostat mesilate may be an effective anti-angiogenic approach in pancreatic cancer therapy.
Pancreatic stellate cells (PSCs)
PSCs are major fibrogenic type cells in the tumor stroma that are closely associated with tumorigenesis, tumor growth and metastasis, and immunosuppression of pancreatic cancer [137,138,139,140,141]. Quiescent PSCs (qPSCs) transform into their activated states under the stimulation of various cytokines and growth factors [142, 143]. Activated PSCs (aPSCs) constitutively produce VEGF-A in an autocrine manner, which in turn, stimulates oriented migration of PSCs in pancreatic tumor tissue [144]. This pro-angiogenic process is upregulated under hypoxia conditions. PSCs also express angiogenesis-regulating molecules including VEGFR-1 and VEGFR-2, Ang-1, and its receptor Tie-2, and vasohibin-1, indicating a close relationship between PSCs and tumor angiogenesis [144]. In addition, PSCs also contribute to the heterogeneity of vascular distribution in pancreatic cancer [61].
Although PSCs are now accepted as dominant promoters of angiogenesis, their overall effect together with pancreatic cancer cells on tumor angiogenesis remains controversial. An in vivo study showed that co-injection of MiaPaCa-2 pancreatic cancer cells and PSCs in the pancreas of mice resulted in increased CD31 staining (a marker of vascular endothelial cells) of primary tumors compared with those injected with cancer cells alone [145]. This observation was further supported by in vitro studies demonstrating that exposure to PSCs significantly enhanced tube formation of vascular endothelial cells. This pro-angiogenic effect could be partially inhibited by VEGF-A neutralizing antibody, suggesting that PSCs mediated tumor angiogenesis, at least in part, through VEGF-A signaling pathway [145]. The study further supports the angiogenesis stimulating property of the pancreatic cancer cell-stellate cell system. However, other studies have different results. For example, Erkan et al. examined the co-culture system of pancreatic cancer cells and PSCs and found it was predominantly anti-angiogenic as indicated by the decreased growth of HUVECs in vitro [146]. In this study, although PSCs induced higher amounts of VEGF-A when treated with cancer cell supernatants, they also increased the production of endostatin (an angiogenesis inhibitor) by cancer cells [146]. Therefore, the overall effect of the system on angiogenesis may be determined by the kinds of molecules that predominate, the pro-angiogenic molecules or anti-angiogenic molecules. The discordance between these studies may reflect the complex interactions between pancreatic cancer cells and PSCs.
Apart from VEGF signaling, the hepatocyte growth factor (HGF)/cMET pathway is another possible candidate pathway in PSCs-mediated angiogenesis. AMG102, an HGF/cMET inhibitor, has been shown to decrease the proliferation and tube formation of endothelial cells upon exposure to secretions of PSCs [147]. Consistent with this, HGF inhibition showed better effects than gemcitabine in reducing tumor angiogenesis and controlling distant metastasis in an orthotopic mouse model of pancreatic cancer [148]. These results are of great clinical importance, providing us with an alternative anti-angiogenic therapeutic strategy that targets the HGF/cMET pathway as a complement to the traditional VEGF inhibitor treatment [149, 150]. Specifically, clinical use of AMG102 has shown encouraging outcomes in treating glioblastoma and gastric cancer, further suggesting the translational utility of this agent in the treatment of pancreatic cancer [151, 152].
Tumor associated macrophages (TAMs)
Macrophages belong to the myeloid cell lineage and are derived from differentiation of circulating monocytes. Under activations by different cytokines, they can be polarized into two opposite states, namely M1 and M2 macrophage phenotypes. The former phenotype mediates resistance against tumors, while the latter phenotype facilitates progression and migration of tumor cells [153]. Macrophages that reside in tumor tissues and interact with cancer cells are usually termed as TAMs. In most solid tumors including pancreatic cancer, the prevalent phenotype of TAMs is M2-like [154, 155].
There is a link between TAMs and VEGF-A/VEGFR-2 signaling. TAMs can express VEGFR-2 and migrate toward VEGF-A with the existence of appropriate cytokines [156]. TAMs can also accelerate the proliferation of endothelial cells and vascular network formation in a VEGF-dependent manner [157]. Of note, TAMs exhibit a pronounced glycolytic signature in response to elevated glycolytic gene transcript levels. Use of glycolysis inhibitors is sufficient to impede TAM-induced angiogenesis, indicating a key role for metabolic reprogramming of TAMs in the development of pancreatic cancer [157]. In addition, some specific subtypes of TAMs have a role in tumor angiogenesis. For example, folate receptor β-expressing (FRβ+) TAMs in pancreatic tumor microenvironments have been shown to express VEGF-A distinctly in perivascular regions of the tumor-invasive fronts, which contributes to the increase of MVD and tumor hematogenous metastasis [158].
To further confirm the role of TAMs in tumor vessel formation, studies have attempted to observe the impact on angiogenesis by suppression of these cells. Two almost simultaneously published studies showed that blockade of specific molecules reduced the recruitment of TAMs to pancreatic tumor tissues and induced an impairment of neovascularization [159, 160]. The pharmacological ablation of TAMs by liposomal clodronate was associated with decreased MVD and markedly reduced circulating VEGF-A levels [161, 162].
The VEGF signaling pathway is an important mechanism in tumor angiogenesis. However, in a pancreatic neuroendocrine tumor model, Harney et al. showed that selective inhibition of Tie-2 receptor resulted in reduced blood vessels and increased vascular maturation, underlining the significance of the Ang-1/Tie-2 pathway in blood vessel formation [163]. The above studies demonstrate that different mechanisms are involved in angiogenesis mediated by TAMs. Anti-angiogenic treatments targeting multiple rather than single signaling pathways may, therefore, produce better clinical outcomes.
TAM-induced angiogenesis is a complex process modulated by various molecules such as HIF-1α, colony stimulating factor 1 (CSF1), and NF-κB [164,165,166]. HIF-1α plays an active role in recruiting TAMs to the tumor sites via CCL2 secretion, which can further accelerate activation of PSCs [164]. Both cell types are strongly pro-angiogenic, thus revealing an extensive interplay between different stromal cells in the tumor microenvironment.
Another important function of TAMs is to promote metastasis by augmenting intravasation into the blood vessels and extravasation out of the blood vessels of pancreatic tumors [157, 158]. This renders cancer cells more mobile, which is the foundation of forming a new metastatic niche. Of interest, ablation of TAMs by inhibiting CCR2 signaling has been demonstrated to block extravasation of tumor cells to the metastatic organs in animal models of breast cancer [167]. Infiltrating TAMs constitutively trigger new vessel formation and enhance the aggressiveness of cancer cells. We, therefore, hypothesize that inhibition of TAMs represents a novel tool for anti-angiogenic and anti-metastatic therapies in pancreatic cancer.
Neutrophils
Compared with PSCs and TAMs, studies that investigate the relationship between neutrophils and angiogenesis in pancreatic cancer are few. Neutrophils have a contradictory role in tumor angiogenesis. Bausch et al. found that neutrophils promoted pancreatic tumor angiogenesis mainly by secreting MMP-9, which is an essential factor during the acquisition of an angiogenic tumor phenotype [168]. In this study, inhibition of MMP-9 alone by doxycycline resulted in a significant decrease in mean MVD and tumor growth, while complete inhibition of angiogenesis required dual inhibition of VEGF-A and MMP-9 [168]. However, neutrophils can also act as suppressors of tumor angiogenesis in pancreatic cancer. Tong et al. demonstrated that neutrophil gelatinase associated lipocalin (NGAL), a 25-kDa acute phase protein first purified from human neutrophils, was highly expressed in well to moderately differentiated PaCa cells, but not in moderately to poorly differentiated PaCa cells. NGAL overexpression was correlated with reduced tumor volume, angiogenesis, and local and distant metastasis [169]. Hence, neutrophils may be a double-edged sword in the process of tumor vessel formation. Further investigations are needed to clarify the roles of this cell type in angiogenesis of pancreatic cancer.
Clinical implications
Since the 2004 approval of bevacizumab, a humanized monoclonal antibody that binds with VEGF-A, it has been used as first-line therapy in colorectal cancer, non-small-cell lung cancer, metastatic breast cancer, and metastatic renal cell carcinoma, and as second-line therapy in glioblastoma multiforme [170]. Other types of anti-angiogenic drugs approved by the FDA are the multi-target tyrosine kinase inhibitors (TKIs), including sunitinib, sorafenib, and pazopanib, all of which target VEGF receptors, particularly VEGFR-2 [171]. For pancreatic cancer treatments, multiple clinical trials of anti-angiogenic agents have been carried out, yet the results are overwhelmingly disappointing [149, 150, 172,173,174,175] (Table 1). Although improved PFS was observed in a few clinical trials [149], none to date has shown significant prolongation of OS for pancreatic cancer patients.
A fundamental challenge is whether angiogenesis status in pancreatic cancer is associated with clinical outcomes. Although high MVD is generally regarded as a predictor of poor prognosis, there were considerable studies that failed to find any correlations between MVD and patient prognosis [57, 58, 60]. For example, van der Zee et al. observed no trend for an association of MVD with recurrence free survival (RFS), cancer specific survival (CSS), and OS in pancreatic cancer patients. They concluded that pancreatic cancer prognosis was angiogenesis independent and MVD provided no additional prognostic information [58]. Indeed, some potential bias exists among the studies, including the use of different criteria for patient enrollment, different methods for angiogenesis quantification, and different markers for identifying endothelial cells. Because MVD is the basis of angiogenesis targeting therapies, it is, therefore, necessary to investigate its value in predicting prognoses for pancreatic cancer patients in more standardized and larger scale studies.
Anti-angiogenic therapy for pancreatic cancer per se is a controversial topic. Anti-angiogenic therapy is based on the theory that tumors are unable to grow without continuous formation of new blood vessels [176]. Blocking vessel formation is, therefore, believed to suppress tumor growth and provide survival benefits for cancer patients. Indeed, this strategy has prolonged the life of many cancer patients [18, 19, 177,178,179,180]. However, a growing number of clinical studies indicates that anti-angiogenic therapy renders tumors with a more invasive phenotype and easily triggers metastasis to distant organs [181,182,183]. In a RIP1-Tag2 model of pancreatic neuroendocrine cancer, Pàez-Ribes et al. showed that administration of DC101, an anti-VEGFR2 antibody, for only 1 week, resulted in reduced tumor vasculature, but induced a more invasive tumor phenotype as determined by histological analyses [181]. Of note, tumor invasiveness was persistently augmented even after the termination of therapy and this invasive tumor phenotype finally translated into distant metastasis [181]. Anti-angiogenic therapy induced invasiveness and metastasis are not confined to pancreatic malignancy, but have also been reported in other types of tumors, including breast cancer and hepatocellular carcinoma [184,185,186].
The reasons for the increased tumor aggressiveness after anti-angiogenesis treatment have not been fully elucidated. One plausible mechanism is tumor hypoxia. Along with angiogenesis inhibition, hypoxia-tolerant tumor cell clones are selected, and those cells more actively escape the hypoxia microenvironment by instigating EMT. As the disseminating cells require stronger resistance to hypoxic conditions, they are more likely to survive in the metastatic lesions [187]. Another explanation for the phenomenon is compensatory upregulation of pro-angiogenic or pro-metastatic cytokines as well as suppression of anti-metastatic mediators [188,189,190]. Some of these factors are capable of recruiting angiogenic bone marrow-derived endothelial and myeloid progenitor cells to create the formation of new metastatic niches [191]. In addition, some anti-angiogenic inhibitors simultaneously impair MVD and MVI, especially broad-spectrum TKIs. The decrease of vascular pericyte coverage destabilizes the vessels, making them more leaky and immature, which subsequently allows for increased intravasation of tumor cells and metastasis [192]. Apart from the aforementioned possible mechanisms, the induction of stromal autophagy, altered endothelial cell adhesion, and increased pro-thrombotic events may all contribute to the malignancy of pancreatic tumor cells [193,194,195].
The enhanced post-therapeutic tumor aggressiveness may, therefore, explain the results of a phase III clinical trial, in which additional use of bevacizumab to gemcitabine plus erlotinib led to 1 month improvement in median PFS, whereas no benefit in OS was observed [149]. We speculate that bevacizumab shows its rapid inhibition of VEGF-A at the initiation of treatment and impairs the growth of primary pancreatic tumors. This is reflected by significant prolongation of PFS. However, rapid emergence of local invasion and distant metastasis following the use of bevacizumab thereupon compromises the initially observed improvement in PFS, and eventually results in no robust benefit in OS. Developing anti-angiogenic strategies that can inhibit the growth of primary tumors, while at the same time suppressing possible invasiveness and metastasis, are critical.
Another paradox is that while anti-angiogenic treatment inhibits blood supply to tumors, it inevitably diminishes drug delivery at the same time [105, 107]. Therefore, an apparent conundrum arises: should tumor vessels be inhibited to induce tumor starvation and shrinkage, or should they be normalized to enhance effective drug concentrations? Studies have focused on vascular normalization in pancreatic cancer. Nagathihalli et al. demonstrated that targeted inhibition of STAT3 combined with gemcitabine was an efficient way to normalize pancreatic tumor vasculature and promote better drug delivery via stromal remodeling without depletion of tumor stromal components. With this method, tumor growth was significantly suppressed and therapeutic response was improved [196]. In a model of pancreatic islet cancer, inhibition of regulator of G-protein signaling 5 (RGS5) resulted in vascular normalization, marked by pericyte maturation, and less leaky and more uniformly distributed microvessels. These changes in vasculature enhanced infiltrations of immune effector cells into pancreatic tumor parenchyma and markedly prolonged the survival of tumor-bearing mice [197]. Because an abnormal tumor vasculature creates an immune-suppressive microenvironment, vascular normalization is now regarded as an emerging strategy to enhance cancer immunotherapy [198, 199]. In addition, it is now becoming increasingly clear that vascular normalization is associated with decreased tumor metastasis [200, 201]. Although some questions still exist, including the proper time to deliver the vascular normalization agents, and when resistance against vessel normalization will occur because vessels are too mature and can no longer remodel [202], vascular normalization is a promising innovative target that could complement conventional anti-angiogenic therapies in the treatment of pancreatic cancer.
As was observed in many clinical trials, the treatment effects varied substantially in different patients. The heterogeneity of therapeutic responses calls for investigations of useful biomarkers to predict which subsets of patients would be likely to benefit the most from treatments. In a phase II clinical trial, Astsaturov et al. evaluated the levels of circulating endothelial cells (CEC) and plasma VEGF-A in the blood of patients with pancreatic cancer receiving bevacizumab. However, they failed to find any relationship between the assumed biomarkers and the patients’ clinical outcomes [203]. Dragovich et al. examined a series of serum angiogenic factors, including VEGF-A, VEGF-C, VEGFR-1, PDGF-BB, Ang-2, osteopontin (OPN), IL-6, and lactate dehydrogenase (LDH), in their clinical trial of the use of vatalanib in pancreatic cancer patients. Among those serum molecules, they confirmed the prognostic value of IL-6 and LDH, as both were demonstrated to correlate with the survival of their patients. None of the factors measured in the study had predictive values for the patient response to vatalanib [204]. Lassau et al. used dynamic contrast-enhanced ultrasonography (DCE-US) to measure mean transit times (MTTs) and found a close correlation with PFS of metastatic pancreatic patients treated with bevacizumab. MTT is, therefore, regarded as an early biomarker to predict clinical outcomes for those who receive anti-angiogenic therapies [205]. To detect additional biomarkers, some studies have identified the angiogenic gene signature in human pancreatic cancers [206].
Taken together, future studies of angiogenesis in pancreatic cancer should consider the following aspects. First, as pancreatic cancer is distinctly characterized by dense deposition of tumor stroma, we should, therefore, pay more attention to their critical roles in angiogenesis. Further exploration of stromal depletion strategies is needed. Second, multiple underlying mechanisms are involved in the angiogenesis of pancreatic cancer. Thus, to block angiogenesis effectively, we need to simultaneously target different molecular signaling pathways. Third, vascular normalization is an emerging therapeutic strategy that has shown great clinical potential for enhancing effective drug delivery, improving local immunosuppressive microenvironment, and reducing distant metastasis. It could, therefore, serve as a supplement to traditional anti-angiogenic therapy and represents a promising future direction of vascular-targeted treatment in pancreatic cancer. Finally, more useful biomarkers are necessary to select appropriate patient populations that respond positively to anti-angiogenic or vascular normalization therapies.
References
Siegel RL, Miller KD, Jemal A (2017) Cancer statistics, 2017. CA Cancer J Clin 67(1):7–30. https://doi.org/10.3322/caac.21387
Siegel RL, Miller KD, Jemal A (2018) Cancer statistics, 2018. CA Cancer J Clin 68(1):7–30. https://doi.org/10.3322/caac.21442
Siegel R, Ma J, Zou Z, Jemal A (2014) Cancer statistics, 2014. CA Cancer J Clin 64(1):9–29. https://doi.org/10.3322/caac.21208
Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM (2014) Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 74(11):2913–2921. https://doi.org/10.1158/0008-5472.can-14-0155
Bosman F, Cameiro F, Hmban R (2010) WHO classification of tumours of the digestive system. IARC Press, Lyon
Kamisawa T, Wood LD, Itoi T, Takaori K (2016) Pancreatic cancer. The Lancet 388(10039):73–85. https://doi.org/10.1016/s0140-6736(16)00141-0
Whatcott CJ, Diep CH, Jiang P, Watanabe A, LoBello J, Sima C, Hostetter G, Shepard HM, Von Hoff DD, Han H (2015) Desmoplasia in primary tumors and metastatic lesions of pancreatic cancer. Clin Cancer Res 21(15):3561–3568. https://doi.org/10.1158/1078-0432.CCR-14-1051
Provenzano PP, Cuevas C, Chang AE, Goel VK, Von Hoff DD, Hingorani SR (2012) Enzymatic targeting of the stroma ablates physical barriers to treatment of pancreatic ductal adenocarcinoma. Cancer Cell 21(3):418–429. https://doi.org/10.1016/j.ccr.2012.01.007
Ehehalt F, Saeger HD, Schmidt CM, Grutzmann R (2009) Neuroendocrine tumors of the pancreas. Oncologist 14(5):456–467. https://doi.org/10.1634/theoncologist.2008-0259
Capozzi M, C VONA, C DED, Ottaiano A, Tatangelo F, Romano GM, Tafuto S (2016) Antiangiogenic therapy in pancreatic neuroendocrine tumors. Anticancer Res 36(10):5025–5030. https://doi.org/10.21873/anticanres.11071
Raymond E, Dahan L, Raoul JL, Bang YJ, Borbath I, Lombard-Bohas C, Valle J, Metrakos P, Smith D, Vinik A, Chen JS, Horsch D, Hammel P, Wiedenmann B, Van Cutsem E, Patyna S, Lu DR, Blanckmeister C, Chao R, Ruszniewski P (2011) Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N Engl J Med 364(6):501–513. https://doi.org/10.1056/NEJMoa1003825
Folkman J (1990) What is the evidence that tumors are angiogenesis dependent? J Natl Cancer Inst 82(1):4–6
Baeriswyl V, Christofori G (2009) The angiogenic switch in carcinogenesis. Semin Cancer Biol 19(5):329–337. https://doi.org/10.1016/j.semcancer.2009.05.003
Ellis LM, Hicklin DJ (2008) VEGF-targeted therapy: mechanisms of anti-tumour activity. Nat Rev Cancer 8(8):579–591. https://doi.org/10.1038/nrc2403
Bry M, Kivela R, Leppanen VM, Alitalo K (2014) Vascular endothelial growth factor-B in physiology and disease. Physiol Rev 94(3):779–794. https://doi.org/10.1152/physrev.00028.2013
Hoff PM, Machado KK (2012) Role of angiogenesis in the pathogenesis of cancer. Cancer Treat Rev 38(7):825–833. https://doi.org/10.1016/j.ctrv.2012.04.006
Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, Heim W, Berlin J, Baron A, Griffing S, Holmgren E, Ferrara N, Fyfe G, Rogers B, Ross R, Kabbinavar F (2004) Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 350(23):2335–2342. https://doi.org/10.1056/NEJMoa032691
Miles DW, Chan A, Dirix LY, Cortes J, Pivot X, Tomczak P, Delozier T, Sohn JH, Provencher L, Puglisi F, Harbeck N, Steger GG, Schneeweiss A, Wardley AM, Chlistalla A, Romieu G (2010) Phase III study of bevacizumab plus docetaxel compared with placebo plus docetaxel for the first-line treatment of human epidermal growth factor receptor 2-negative metastatic breast cancer. J Clin Oncol 28(20):3239–3247. https://doi.org/10.1200/jco.2008.21.6457
Escudier B, Bellmunt J, Negrier S, Bajetta E, Melichar B, Bracarda S, Ravaud A, Golding S, Jethwa S, Sneller V (2010) Phase III trial of bevacizumab plus interferon alfa-2a in patients with metastatic renal cell carcinoma (AVOREN): final analysis of overall survival. J Clin Oncol 28(13):2144–2150. https://doi.org/10.1200/jco.2009.26.7849
Potente M, Gerhardt H, Carmeliet P (2011) Basic and therapeutic aspects of angiogenesis. Cell 146(6):873–887. https://doi.org/10.1016/j.cell.2011.08.039
Jakobsson L, Franco CA, Bentley K, Collins RT, Ponsioen B, Aspalter IM, Rosewell I, Busse M, Thurston G, Medvinsky A, Schulte-Merker S, Gerhardt H (2010) Endothelial cells dynamically compete for the tip cell position during angiogenic sprouting. Nat Cell Biol 12(10):943–953. https://doi.org/10.1038/ncb2103
Galie PA, Nguyen DH, Choi CK, Cohen DM, Janmey PA, Chen CS (2014) Fluid shear stress threshold regulates angiogenic sprouting. Proc Natl Acad Sci USA 111(22):7968–7973. https://doi.org/10.1073/pnas.1310842111
Mentzer SJ, Konerding MA (2014) Intussusceptive angiogenesis: expansion and remodeling of microvascular networks. Angiogenesis 17(3):499–509. https://doi.org/10.1007/s10456-014-9428-3
Paku S, Dezso K, Bugyik E, Tovari J, Timar J, Nagy P, Laszlo V, Klepetko W, Dome B (2011) A new mechanism for pillar formation during tumor-induced intussusceptive angiogenesis: inverse sprouting. Am J Pathol 179(3):1573–1585. https://doi.org/10.1016/j.ajpath.2011.05.033
Hlushchuk R, Makanya AN, Djonov V (2011) Escape mechanisms after antiangiogenic treatment, or why are the tumors growing again? Int J Dev Biol 55(4–5):563–567. https://doi.org/10.1387/ijdb.103231rh
Hlushchuk R, Riesterer O, Baum O, Wood J, Gruber G, Pruschy M, Djonov V (2008) Tumor recovery by angiogenic switch from sprouting to intussusceptive angiogenesis after treatment with PTK787/ZK222584 or ionizing radiation. Am J Pathol 173(4):1173–1185. https://doi.org/10.2353/ajpath.2008.071131
Djonov VG, Kurz H, Burri PH (2002) Optimality in the developing vascular system: branching remodeling by means of intussusception as an efficient adaptation mechanism. Dev Dyn 224(4):391–402. https://doi.org/10.1002/dvdy.10119
Milkiewicz M, Brown MD, Egginton S, Hudlicka O (2001) Association between shear stress, angiogenesis, and VEGF in skeletal muscles in vivo. Microcirculation (New York, NY: 1994) 8(4):229–241. https://doi.org/10.1038/sj/mn/7800074
Egginton S, Zhou AL, Brown MD, Hudlicka O (2001) Unorthodox angiogenesis in skeletal muscle. Cardiovasc Res 49(3):634–646
Gianni-Barrera R, Trani M, Fontanellaz C, Heberer M, Djonov V, Hlushchuk R, Banfi A (2013) VEGF over-expression in skeletal muscle induces angiogenesis by intussusception rather than sprouting. Angiogenesis 16(1):123–136. https://doi.org/10.1007/s10456-012-9304-y
Dill MT, Rothweiler S, Djonov V, Hlushchuk R, Tornillo L, Terracciano L, Meili-Butz S, Radtke F, Heim MH, Semela D (2012) Disruption of Notch1 induces vascular remodeling, intussusceptive angiogenesis, and angiosarcomas in livers of mice. Gastroenterology 142(4):967–977.e962. https://doi.org/10.1053/j.gastro.2011.12.052
Dimova I, Hlushchuk R, Makanya A, Styp-Rekowska B, Ceausu A, Flueckiger S, Lang S, Semela D, Le Noble F, Chatterjee S, Djonov V (2013) Inhibition of Notch signaling induces extensive intussusceptive neo-angiogenesis by recruitment of mononuclear cells. Angiogenesis 16(4):921–937. https://doi.org/10.1007/s10456-013-9366-5
Van den Eynden GG, Bird NC, Majeed AW, Van Laere S, Dirix LY, Vermeulen PB (2012) The histological growth pattern of colorectal cancer liver metastases has prognostic value. Clin Exp Metastasis 29(6):541–549. https://doi.org/10.1007/s10585-012-9469-1
Budde MD, Gold E, Jordan EK, Frank JA (2012) Differential microstructure and physiology of brain and bone metastases in a rat breast cancer model by diffusion and dynamic contrast enhanced MRI. Clin Exp Metastasis 29(1):51–62. https://doi.org/10.1007/s10585-011-9428-2
Franco M, Paez-Ribes M, Cortez E, Casanovas O, Pietras K (2011) Use of a mouse model of pancreatic neuroendocrine tumors to find pericyte biomarkers of resistance to anti-angiogenic therapy. Horm Metab Res 43(12):884–889. https://doi.org/10.1055/s-0031-1284381
Frentzas S, Simoneau E, Bridgeman VL, Vermeulen PB, Foo S, Kostaras E, Nathan M, Wotherspoon A, Gao ZH, Shi Y, Van den Eynden G, Daley F, Peckitt C, Tan X, Salman A, Lazaris A, Gazinska P, Berg TJ, Eltahir Z, Ritsma L, Van Rheenen J, Khashper A, Brown G, Nystrom H, Sund M, Van Laere S, Loyer E, Dirix L, Cunningham D, Metrakos P, Reynolds AR (2016) Vessel co-option mediates resistance to anti-angiogenic therapy in liver metastases. Nat Med 22(11):1294–1302. https://doi.org/10.1038/nm.4197
Bridgeman VL, Vermeulen PB, Foo S, Bilecz A, Daley F, Kostaras E, Nathan MR, Wan E, Frentzas S, Schweiger T, Hegedus B, Hoetzenecker K, Renyi-Vamos F, Kuczynski EA, Vasudev NS, Larkin J, Gore M, Dvorak HF, Paku S, Kerbel RS, Dome B, Reynolds AR (2017) Vessel co-option is common in human lung metastases and mediates resistance to anti-angiogenic therapy in preclinical lung metastasis models. J Pathol 241(3):362–374. https://doi.org/10.1002/path.4845
Folberg R, Hendrix MJ, Maniotis AJ (2000) Vasculogenic mimicry and tumor angiogenesis. Am J Pathol 156(2):361–381. https://doi.org/10.1016/s0002-9440(10)64739-6
Maniotis AJ, Folberg R, Hess A, Seftor EA, Gardner LM, Pe’er J, Trent JM, Meltzer PS, Hendrix MJ (1999) Vascular channel formation by human melanoma cells in vivo and in vitro: vasculogenic mimicry. Am J Pathol 155(3):739–752. https://doi.org/10.1016/s0002-9440(10)65173-5
Liu WB, Xu GL, Jia WD, Li JS, Ma JL, Chen K, Wang ZH, Ge YS, Ren WH, Yu JH, Wang W, Wang XJ (2011) Prognostic significance and mechanisms of patterned matrix vasculogenic mimicry in hepatocellular carcinoma. Medical Oncol (Northwood London England) 28(Suppl 1):S228–S238. https://doi.org/10.1007/s12032-010-9706-x
Tan LY, Mintoff C, Johan MZ, Ebert BW, Fedele C, Zhang YF, Szeto P, Sheppard KE, McArthur GA, Foster-Smith E, Ruszkiewicz A, Brown MP, Bonder CS, Shackleton M, Ebert LM (2016) Desmoglein 2 promotes vasculogenic mimicry in melanoma and is associated with poor clinical outcome. Oncotarget 7(29):46492–46508. https://doi.org/10.18632/oncotarget.10216
Yang J, Zhu DM, Zhou XG, Yin N, Zhang Y, Zhang ZX, Li DC, Zhou J (2017) HIF-2alpha promotes the formation of vasculogenic mimicry in pancreatic cancer by regulating the binding of Twist1 to the VE-cadherin promoter. Oncotarget 8(29):47801–47815. https://doi.org/10.18632/oncotarget.17999
Paulis YW, Soetekouw PM, Verheul HM, Tjan-Heijnen VC, Griffioen AW (2010) Signalling pathways in vasculogenic mimicry. Biochim Biophys Acta 1806(1):18–28. https://doi.org/10.1016/j.bbcan.2010.01.001
Guo JQ, Zheng QH, Chen H, Chen L, Xu JB, Chen MY, Lu D, Wang ZH, Tong HF, Lin S (2014) Ginsenoside Rg3 inhibition of vasculogenic mimicry in pancreatic cancer through downregulation of VEcadherin/EphA2/MMP9/MMP2 expression. Int J Oncol 45(3):1065–1072. https://doi.org/10.3892/ijo.2014.2500
Mourad-Zeidan AA, Melnikova VO, Wang H, Raz A, Bar-Eli M (2008) Expression profiling of Galectin-3-depleted melanoma cells reveals its major role in melanoma cell plasticity and vasculogenic mimicry. Am J Pathol 173(6):1839–1852. https://doi.org/10.2353/ajpath.2008.080380
Cong R, Sun Q, Yang L, Gu H, Zeng Y, Wang B (2009) Effect of Genistein on vasculogenic mimicry formation by human uveal melanoma cells. J Exp Clin Cancer Res 28:124. https://doi.org/10.1186/1756-9966-28-124
Blogowski W, Bodnarczuk T, Starzynska T (2016) Concise review: pancreatic cancer and bone marrow-derived stem cells. Stem Cells Transl Med 5(7):938–945. https://doi.org/10.5966/sctm.2015-0291
Vizio B, Novarino A, Giacobino A, Cristiano C, Prati A, Brondino G, Ciuffreda L, Bellone G (2010) Pilot study to relate clinical outcome in pancreatic carcinoma and angiogenic plasma factors/circulating mature/progenitor endothelial cells: preliminary results. Cancer Sci 101(11):2448–2454. https://doi.org/10.1111/j.1349-7006.2010.01692.x
Vizio B, Biasi F, Scirelli T, Novarino A, Prati A, Ciuffreda L, Montrucchio G, Poli G, Bellone G (2013) Pancreatic-carcinoma-cell-derived pro-angiogenic factors can induce endothelial-cell differentiation of a subset of circulating CD34+ progenitors. J Transl Med 11:314. https://doi.org/10.1186/1479-5876-11-314
Kurtagic E, Rich CB, Buczek-Thomas JA, Nugent MA (2015) Neutrophil elastase-generated fragment of vascular endothelial growth factor-A stimulates macrophage and endothelial progenitor cell migration. PLoS ONE 10(12):e0145115. https://doi.org/10.1371/journal.pone.0145115
Yamazaki M, Nakamura K, Mizukami Y, Ii M, Sasajima J, Sugiyama Y, Nishikawa T, Nakano Y, Yanagawa N, Sato K, Maemoto A, Tanno S, Okumura T, Karasaki H, Kono T, Fujiya M, Ashida T, Chung DC, Kohgo Y (2008) Sonic hedgehog derived from human pancreatic cancer cells augments angiogenic function of endothelial progenitor cells. Cancer Sci 99(6):1131–1138. https://doi.org/10.1111/j.1349-7006.2008.00795.x
Nakamura K, Sasajima J, Mizukami Y, Sugiyama Y, Yamazaki M, Fujii R, Kawamoto T, Koizumi K, Sato K, Fujiya M, Sasaki K, Tanno S, Okumura T, Shimizu N, Kawabe J, Karasaki H, Kono T, Ii M, Bardeesy N, Chung DC, Kohgo Y (2010) Hedgehog promotes neovascularization in pancreatic cancers by regulating Ang-1 and IGF-1 expression in bone-marrow derived pro-angiogenic cells. PLoS ONE 5(1):e8824. https://doi.org/10.1371/journal.pone.0008824
Li A, Cheng XJ, Moro A, Singh RK, Hines OJ, Eibl G (2011) CXCR2-dependent endothelial progenitor cell mobilization in pancreatic cancer growth. Transl Oncol 4(1):20–28
Vermeulen PB, Gasparini G, Fox SB, Colpaert C, Marson LP, Gion M, Belien JA, de Waal RM, Van Marck E, Magnani E, Weidner N, Harris AL, Dirix LY (2002) Second international consensus on the methodology and criteria of evaluation of angiogenesis quantification in solid human tumours. Eur J Cancer (Oxford, England: 1990) 38(12):1564–1579
Hoem D, Straume O, Immervoll H, Akslen LA, Molven A (2013) Vascular proliferation is associated with survival in pancreatic ductal adenocarcinoma. APMIS 121(11):1037–1046. https://doi.org/10.1111/apm.12057
Nishida T, Yoshitomi H, Takano S, Kagawa S, Shimizu H, Ohtsuka M, Kato A, Furukawa K, Miyazaki M (2016) Low stromal area and high stromal microvessel density predict poor prognosis in pancreatic cancer. Pancreas 45(4):593–600. https://doi.org/10.1097/mpa.0000000000000499
Jureidini R, da Cunha JE, Takeda F, Namur GN, Ribeiro TC, Patzina R, Figueira ER, Ribeiro U Jr, Bacchella T, Cecconello I (2016) Evaluation of microvessel density and p53 expression in pancreatic adenocarcinoma. Clinics (Sao Paulo Brazil) 71(6):315–319. https://doi.org/10.6061/clinics/2016(06)05
van der Zee JA, van Eijck CH, Hop WC, van Dekken H, Dicheva BM, Seynhaeve AL, Koning GA, Eggermont AM, ten Hagen TL (2011) Angiogenesis: a prognostic determinant in pancreatic cancer? Eur J Cancer (Oxford England 1990) 47(17):2576–2584. https://doi.org/10.1016/j.ejca.2011.08.016
Takahashi Y, Cleary KR, Mai M, Kitadai Y, Bucana CD, Ellis LM (1996) Significance of vessel count and vascular endothelial growth factor and its receptor (KDR) in intestinal-type gastric cancer. Clin Cancer Res 2(10):1679–1684
Barau A, Ruiz-Sauri A, Valencia G, Gomez-Mateo Mdel C, Sabater L, Ferrandez A, Llombart-Bosch A (2013) High microvessel density in pancreatic ductal adenocarcinoma is associated with high grade. Virchows Archiv 462(5):541–546. https://doi.org/10.1007/s00428-013-1409-1
Di Maggio F, Arumugam P, Delvecchio FR, Batista S, Lechertier T, Hodivala-Dilke K, Kocher HM (2016) Pancreatic stellate cells regulate blood vessel density in the stroma of pancreatic ductal adenocarcinoma. Pancreatology 16(6):995–1004. https://doi.org/10.1016/j.pan.2016.05.393
Komar G, Kauhanen S, Liukko K, Seppanen M, Kajander S, Ovaska J, Nuutila P, Minn H (2009) Decreased blood flow with increased metabolic activity: a novel sign of pancreatic tumor aggressiveness. Clin Cancer Res 15(17):5511–5517. https://doi.org/10.1158/1078-0432.ccr-09-0414
Rhim AD, Oberstein PE, Thomas DH, Mirek ET, Palermo CF, Sastra SA, Dekleva EN, Saunders T, Becerra CP, Tattersall IW, Westphalen CB, Kitajewski J, Fernandez-Barrena MG, Fernandez-Zapico ME, Iacobuzio-Donahue C, Olive KP, Stanger BZ (2014) Stromal elements act to restrain, rather than support, pancreatic ductal adenocarcinoma. Cancer Cell 25(6):735–747. https://doi.org/10.1016/j.ccr.2014.04.021
Olive KP, Jacobetz MA, Davidson CJ, Gopinathan A, McIntyre D, Honess D, Madhu B, Goldgraben MA, Caldwell ME, Allard D, Frese KK, Denicola G, Feig C, Combs C, Winter SP, Ireland-Zecchini H, Reichelt S, Howat WJ, Chang A, Dhara M, Wang L, Ruckert F, Grutzmann R, Pilarsky C, Izeradjene K, Hingorani SR, Huang P, Davies SE, Plunkett W, Egorin M, Hruban RH, Whitebread N, McGovern K, Adams J, Iacobuzio-Donahue C, Griffiths J, Tuveson DA (2009) Inhibition of Hedgehog signaling enhances delivery of chemotherapy in a mouse model of pancreatic cancer. Science 324(5933):1457–1461. https://doi.org/10.1126/science.1171362
Hexige S, Ardito-Abraham CM, Wu Y, Wei Y, Fang Y, Han X, Li J, Zhou P, Yi Q, Maitra A, Liu JO, Tuveson DA, Lou W, Yu L (2015) Identification of novel vascular projections with cellular trafficking abilities on the microvasculature of pancreatic ductal adenocarcinoma. J Pathol 236(2):142–154. https://doi.org/10.1002/path.4506
Armulik A, Abramsson A, Betsholtz C (2005) Endothelial/pericyte interactions. Circ Res 97(6):512–523. https://doi.org/10.1161/01.RES.0000182903.16652.d7
Caporali A, Martello A, Miscianinov V, Maselli D, Vono R, Spinetti G (2017) Contribution of pericyte paracrine regulation of the endothelium to angiogenesis. Pharmacol Ther 171:56–64. https://doi.org/10.1016/j.pharmthera.2016.10.001
Maione F, Molla F, Meda C, Latini R, Zentilin L, Giacca M, Seano G, Serini G, Bussolino F, Giraudo E (2009) Semaphorin 3A is an endogenous angiogenesis inhibitor that blocks tumor growth and normalizes tumor vasculature in transgenic mouse models. J Clin Invest 119(11):3356–3372. https://doi.org/10.1172/jci36308
McCarty MF, Somcio RJ, Stoeltzing O, Wey J, Fan F, Liu W, Bucana C, Ellis LM (2007) Overexpression of PDGF-BB decreases colorectal and pancreatic cancer growth by increasing tumor pericyte content. J Clin Invest 117(8):2114–2122. https://doi.org/10.1172/jci31334
Gilles ME, Maione F, Cossutta M, Carpentier G, Caruana L, Di Maria S, Houppe C, Destouches D, Shchors K, Prochasson C, Mongelard F, Lamba S, Bardelli A, Bouvet P, Couvelard A, Courty J, Giraudo E, Cascone I (2016) Nucleolin targeting impairs the progression of pancreatic cancer and promotes the normalization of tumor vasculature. Cancer Res 76(24):7181–7193. https://doi.org/10.1158/0008-5472.can-16-0300
Wang WQ, Liu L, Xu HX, Luo GP, Chen T, Wu CT, Xu YF, Xu J, Liu C, Zhang B, Long J, Tang ZY, Yu XJ (2013) Intratumoral alpha-SMA enhances the prognostic potency of CD34 associated with maintenance of microvessel integrity in hepatocellular carcinoma and pancreatic cancer. PLoS ONE 8(8):e71189. https://doi.org/10.1371/journal.pone.0071189
Xie K, Wei D, Huang S (2006) Transcriptional anti-angiogenesis therapy of human pancreatic cancer. Cytokine Growth Factor Rev 17(3):147–156. https://doi.org/10.1016/j.cytogfr.2006.01.002
DiDonato JA, Mercurio F, Karin M (2012) NF-kappaB and the link between inflammation and cancer. Immunol Rev 246(1):379–400. https://doi.org/10.1111/j.1600-065X.2012.01099.x
Carbone C, Melisi D (2012) NF-kappaB as a target for pancreatic cancer therapy. Expert Opin Ther Targets 16(Suppl 2):S1–S10. https://doi.org/10.1517/14728222.2011.645806
Maier HJ, Schmidt-Strassburger U, Huber MA, Wiedemann EM, Beug H, Wirth T (2010) NF-kappaB promotes epithelial-mesenchymal transition, migration and invasion of pancreatic carcinoma cells. Cancer Lett 295(2):214–228. https://doi.org/10.1016/j.canlet.2010.03.003
Saito K, Matsuo Y, Imafuji H, Okubo T, Maeda Y, Sato T, Shamoto T, Tsuboi K, Morimoto M, Takahashi H, Ishiguro H, Takiguchi S (2018) Xanthohumol inhibits angiogenesis by suppressing nuclear factor-kappaB activation in pancreatic cancer. Cancer Sci 109(1):132–140. https://doi.org/10.1111/cas.13441
Wang L, Zhou W, Zhong Y, Huo Y, Fan P, Zhan S, Xiao J, Jin X, Gou S, Yin T, Wu H, Liu T (2017) Overexpression of G protein-coupled receptor GPR87 promotes pancreatic cancer aggressiveness and activates NF-kappaB signaling pathway. Mol Cancer 16(1):61. https://doi.org/10.1186/s12943-017-0627-6
Hosoi F, Izumi H, Kawahara A, Murakami Y, Kinoshita H, Kage M, Nishio K, Kohno K, Kuwano M, Ono M (2009) N-myc downstream regulated gene 1/Cap43 suppresses tumor growth and angiogenesis of pancreatic cancer through attenuation of inhibitor of kappaB kinase beta expression. Cancer Res 69(12):4983–4991. https://doi.org/10.1158/0008-5472.can-08-4882
Cai X, Lu W, Yang Y, Yang J, Ye J, Gu Z, Hu C, Wang X, Cao P (2013) Digitoflavone inhibits IkappaBalpha kinase and enhances apoptosis induced by TNFalpha through downregulation of expression of nuclear factor kappaB-regulated gene products in human pancreatic cancer cells. PLoS ONE 8(10):e77126. https://doi.org/10.1371/journal.pone.0077126
Waters JA, Matos J, Yip-Schneider M, Aguilar-Saavedra JR, Crean CD, Beane JD, Dumas RP, Suvannasankha A, Schmidt CM (2015) Targeted nuclear factor-kappaB suppression enhances gemcitabine response in human pancreatic tumor cell line murine xenografts. Surgery 158(4):881–888. https://doi.org/10.1016/j.surg.2015.04.043 discussion 888–889.
Sankpal UT, Maliakal P, Bose D, Kayaleh O, Buchholz D, Basha R (2012) Expression of specificity protein transcription factors in pancreatic cancer and their association in prognosis and therapy. Curr Med Chem 19(22):3779–3786
Huang C, Xie K (2012) Crosstalk of Sp1 and Stat3 signaling in pancreatic cancer pathogenesis. Cytokine Growth Factor Rev 23(1–2):25–35. https://doi.org/10.1016/j.cytogfr.2012.01.003
Abdelrahim M, Smith R 3rd, Burghardt R, Safe S (2004) Role of Sp proteins in regulation of vascular endothelial growth factor expression and proliferation of pancreatic cancer cells. Cancer Res 64(18):6740–6749. https://doi.org/10.1158/0008-5472.can-04-0713
Abdelrahim M, Baker CH, Abbruzzese JL, Sheikh-Hamad D, Liu S, Cho SD, Yoon K, Safe S (2007) Regulation of vascular endothelial growth factor receptor-1 expression by specificity proteins 1, 3, and 4 in pancreatic cancer cells. Cancer Res 67(7):3286–3294. https://doi.org/10.1158/0008-5472.can-06-3831
Higgins KJ, Abdelrahim M, Liu S, Yoon K, Safe S (2006) Regulation of vascular endothelial growth factor receptor-2 expression in pancreatic cancer cells by Sp proteins. Biochem Biophys Res Commun 345(1):292–301. https://doi.org/10.1016/j.bbrc.2006.04.111
Hu H, Han T, Zhuo M, Wu LL, Yuan C, Wu L, Lei W, Jiao F, Wang LW (2017) Elevated COX-2 expression promotes angiogenesis through EGFR/p38-MAPK/Sp1-dependent signalling in pancreatic cancer. Sci Rep 7(1):470. https://doi.org/10.1038/s41598-017-00288-4
Wei D, Wang L, He Y, Xiong HQ, Abbruzzese JL, Xie K (2004) Celecoxib inhibits vascular endothelial growth factor expression in and reduces angiogenesis and metastasis of human pancreatic cancer via suppression of Sp1 transcription factor activity. Cancer Res 64(6):2030–2038
Abdelrahim M, Baker CH, Abbruzzese JL, Safe S (2006) Tolfenamic acid and pancreatic cancer growth, angiogenesis, and Sp protein degradation. J Natl Cancer Inst 98(12):855–868. https://doi.org/10.1093/jnci/djj232
Yuan P, Wang L, Wei D, Zhang J, Jia Z, Li Q, Le X, Wang H, Yao J, Xie K (2007) Therapeutic inhibition of Sp1 expression in growing tumors by mithramycin a correlates directly with potent antiangiogenic effects on human pancreatic cancer. Cancer 110(12):2682–2690. https://doi.org/10.1002/cncr.23092
Zhong Z, Wen Z, Darnell JE, Jr (1994) Stat3: a STAT family member activated by tyrosine phosphorylation in response to epidermal growth factor and interleukin-6. Science 264(5155):95–98
Schindler C, Levy DE, Decker T (2007) JAK-STAT signaling: from interferons to cytokines. J Biol Chem 282(28):20059–20063. https://doi.org/10.1074/jbc.R700016200
Wei D, Le X, Zheng L, Wang L, Frey JA, Gao AC, Peng Z, Huang S, Xiong HQ, Abbruzzese JL, Xie K (2003) Stat3 activation regulates the expression of vascular endothelial growth factor and human pancreatic cancer angiogenesis and metastasis. Oncogene 22(3):319–329. https://doi.org/10.1038/sj.onc.1206122
Boreddy SR, Sahu RP, Srivastava SK (2011) Benzyl isothiocyanate suppresses pancreatic tumor angiogenesis and invasion by inhibiting HIF-alpha/VEGF/Rho-GTPases: pivotal role of STAT-3. PLoS ONE 6(10):e25799. https://doi.org/10.1371/journal.pone.0025799
Huang C, Huang R, Chang W, Jiang T, Huang K, Cao J, Sun X, Qiu Z (2012) The expression and clinical significance of pSTAT3, VEGF and VEGF-C in pancreatic adenocarcinoma. Neoplasma 59(1):52–61. https://doi.org/10.4149/neo_2012_007
Trevino JG, Gray MJ, Nawrocki ST, Summy JM, Lesslie DP, Evans DB, Sawyer TK, Shakespeare WC, Watowich SS, Chiao PJ, McConkey DJ, Gallick GE (2006) Src activation of Stat3 is an independent requirement from NF-kappaB activation for constitutive IL-8 expression in human pancreatic adenocarcinoma cells. Angiogenesis 9(2):101–110. https://doi.org/10.1007/s10456-006-9038-9
Huang C, Jiang T, Zhu L, Liu J, Cao J, Huang KJ, Qiu ZJ (2011) STAT3-targeting RNA interference inhibits pancreatic cancer angiogenesis in vitro and in vivo. Int J Oncol 38(6):1637–1644. https://doi.org/10.3892/ijo.2011.1000
Lin L, Hutzen B, Zuo M, Ball S, Deangelis S, Foust E, Pandit B, Ihnat MA, Shenoy SS, Kulp S, Li PK, Li C, Fuchs J, Lin J (2010) Novel STAT3 phosphorylation inhibitors exhibit potent growth-suppressive activity in pancreatic and breast cancer cells. Cancer Res 70(6):2445–2454. https://doi.org/10.1158/0008-5472.can-09-2468
Li H, Huang C, Huang K, Wu W, Jiang T, Cao J, Feng Z, Qiu Z (2011) STAT3 knockdown reduces pancreatic cancer cell invasiveness and matrix metalloproteinase-7 expression in nude mice. PLoS ONE 6(10):e25941. https://doi.org/10.1371/journal.pone.0025941
Niu F, Li Y, Lai FF, Ni L, Ji M, Jin J, Yang HZ, Wang C, Zhang DM, Chen XG (2015) LB-1 exerts antitumor activity in pancreatic cancer by inhibiting HIF-1alpha and Stat3 signaling. J Cell Physiol 230(9):2212–2223. https://doi.org/10.1002/jcp.24949
Moser C, Ruemmele P, Gehmert S, Schenk H, Kreutz MP, Mycielska ME, Hackl C, Kroemer A, Schnitzbauer AA, Stoeltzing O, Schlitt HJ, Geissler EK, Lang SA (2012) STAT5b as molecular target in pancreatic cancer–inhibition of tumor growth, angiogenesis, and metastases. Neoplasia (New York NY) 14(10):915–925
Sahraei M, Roy LD, Curry JM, Teresa TL, Nath S, Besmer D, Kidiyoor A, Dalia R, Gendler SJ, Mukherjee P (2012) MUC1 regulates PDGFA expression during pancreatic cancer progression. Oncogene 31(47):4935–4945. https://doi.org/10.1038/onc.2011.651
Polvani S, Tarocchi M, Tempesti S, Mello T, Ceni E, Buccoliero F, D’Amico M, Boddi V, Farsi M, Nesi S, Nesi G, Milani S, Galli A (2014) COUP-TFII in pancreatic adenocarcinoma: clinical implication for patient survival and tumor progression. Int J Cancer 134(7):1648–1658. https://doi.org/10.1002/ijc.28502
Ninomiya I, Yamazaki K, Oyama K, Hayashi H, Tajima H, Kitagawa H, Fushida S, Fujimura T, Ohta T (2014) Pioglitazone inhibits the proliferation and metastasis of human pancreatic cancer cells. Oncol Lett 8(6):2709–2714. https://doi.org/10.3892/ol.2014.2553
Toole BP, Slomiany MG (2008) Hyaluronan: a constitutive regulator of chemoresistance and malignancy in cancer cells. Semin Cancer Biol 18(4):244–250. https://doi.org/10.1016/j.semcancer.2008.03.009
Jacobetz MA, Chan DS, Neesse A, Bapiro TE, Cook N, Frese KK, Feig C, Nakagawa T, Caldwell ME, Zecchini HI, Lolkema MP, Jiang P, Kultti A, Thompson CB, Maneval DC, Jodrell DI, Frost GI, Shepard HM, Skepper JN, Tuveson DA (2013) Hyaluronan impairs vascular function and drug delivery in a mouse model of pancreatic cancer. Gut 62(1):112–120. https://doi.org/10.1136/gutjnl-2012-302529
Hingorani SR, Harris WP, Beck JT, Berdov BA, Wagner SA, Pshevlotsky EM, Tjulandin SA, Gladkov OA, Holcombe RF, Korn R, Raghunand N, Dychter S, Jiang P, Shepard HM, Devoe CE (2016) Phase Ib study of PEGylated recombinant human hyaluronidase and gemcitabine in patients with advanced pancreatic cancer. Clin Cancer Res 22(12):2848–2854. https://doi.org/10.1158/1078-0432.ccr-15-2010
Banerjee S, Modi S, McGinn O, Zhao X, Dudeja V, Ramakrishnan S, Saluja AK (2016) Impaired synthesis of stromal components in response to minnelide improves vascular function, drug delivery, and survival in pancreatic cancer. Clin Cancer Res 22(2):415–425. https://doi.org/10.1158/1078-0432.ccr-15-1155
Nagase H, Kudo D, Suto A, Yoshida E, Suto S, Negishi M, Kakizaki I, Hakamada K (2017) 4-Methylumbelliferone suppresses hyaluronan synthesis and tumor progression in SCID mice intra-abdominally inoculated with pancreatic cancer cells. Pancreas 46(2):190–197. https://doi.org/10.1097/mpa.0000000000000741
Nieskoski MD, Marra K, Gunn JR, Hoopes PJ, Doyley MM, Hasan T, Trembly BS, Pogue BW (2017) Collagen complexity spatially defines microregions of total tissue pressure in pancreatic cancer. Sci Rep 7(1):10093. https://doi.org/10.1038/s41598-017-10671-w
Aguilera KY, Rivera LB, Hur H, Carbon JG, Toombs JE, Goldstein CD, Dellinger MT, Castrillon DH, Brekken RA (2014) Collagen signaling enhances tumor progression after anti-VEGF therapy in a murine model of pancreatic ductal adenocarcinoma. Cancer Res 74(4):1032–1044. https://doi.org/10.1158/0008-5472.can-13-2800
Berchtold S, Grunwald B, Kruger A, Reithmeier A, Hahl T, Cheng T, Feuchtinger A, Born D, Erkan M, Kleeff J, Esposito I (2015) Collagen type V promotes the malignant phenotype of pancreatic ductal adenocarcinoma. Cancer Lett 356(2 Pt B):721–732. https://doi.org/10.1016/j.canlet.2014.10.020
Matsuo Y, Raimondo M, Woodward TA, Wallace MB, Gill KR, Tong Z, Burdick MD, Yang Z, Strieter RM, Hoffman RM, Guha S (2009) CXC-chemokine/CXCR2 biological axis promotes angiogenesis in vitro and in vivo in pancreatic cancer. Int J Cancer 125(5):1027–1037. https://doi.org/10.1002/ijc.24383
Hill KS, Gaziova I, Harrigal L, Guerra YA, Qiu S, Sastry SK, Arumugam T, Logsdon CD, Elferink LA (2012) Met receptor tyrosine kinase signaling induces secretion of the angiogenic chemokine interleukin-8/CXCL8 in pancreatic cancer. PLoS ONE 7(7):e40420. https://doi.org/10.1371/journal.pone.0040420
Matsuo Y, Ochi N, Sawai H, Yasuda A, Takahashi H, Funahashi H, Takeyama H, Tong Z, Guha S (2009) CXCL8/IL-8 and CXCL12/SDF-1alpha co-operatively promote invasiveness and angiogenesis in pancreatic cancer. Int J Cancer 124(4):853–861. https://doi.org/10.1002/ijc.24040
Wente MN, Mayer C, Gaida MM, Michalski CW, Giese T, Bergmann F, Giese NA, Buchler MW, Friess H (2008) CXCL14 expression and potential function in pancreatic cancer. Cancer Lett 259(2):209–217. https://doi.org/10.1016/j.canlet.2007.10.021
Uzunoglu FG, Kolbe J, Wikman H, Gungor C, Bohn BA, Nentwich MF, Reeh M, Konig AM, Bockhorn M, Kutup A, Mann O, Izbicki JR, Vashist YK (2013) VEGFR-2, CXCR-2 and PAR-1 germline polymorphisms as predictors of survival in pancreatic carcinoma. Ann Oncol 24(5):1282–1290. https://doi.org/10.1093/annonc/mds634
Ijichi H, Chytil A, Gorska AE, Aakre ME, Bierie B, Tada M, Mohri D, Miyabayashi K, Asaoka Y, Maeda S, Ikenoue T, Tateishi K, Wright CV, Koike K, Omata M, Moses HL (2011) Inhibiting Cxcr2 disrupts tumor-stromal interactions and improves survival in a mouse model of pancreatic ductal adenocarcinoma. J Clin Invest 121(10):4106–4117. https://doi.org/10.1172/jci42754
Maeda S, Kuboki S, Nojima H, Shimizu H, Yoshitomi H, Furukawa K, Miyazaki M, Ohtsuka M (2017) Duffy antigen receptor for chemokines (DARC) expressing in cancer cells inhibits tumor progression by suppressing CXCR2 signaling in human pancreatic ductal adenocarcinoma. Cytokine 95:12–21. https://doi.org/10.1016/j.cyto.2017.02.007
Kalbasi A, Komar C, Tooker GM, Liu M, Lee JW, Gladney WL, Ben-Josef E, Beatty GL (2017) Tumor-derived CCL2 mediates resistance to radiotherapy in pancreatic ductal adenocarcinoma. Clin Cancer Res 23(1):137–148. https://doi.org/10.1158/1078-0432.ccr-16-0870
Zhao B, Cui K, Wang CL, Wang AL, Zhang B, Zhou WY, Zhao WH, Li S (2011) The chemotactic interaction between CCL21 and its receptor, CCR7, facilitates the progression of pancreatic cancer via induction of angiogenesis and lymphangiogenesis. J Hepatobiliary Pancreat Sci 18(6):821–828. https://doi.org/10.1007/s00534-011-0395-4
Ramaswamy S, Ross KN, Lander ES, Golub TR (2003) A molecular signature of metastasis in primary solid tumors. Nat Genet 33(1):49–54. https://doi.org/10.1038/ng1060
Schaffner F, Ray AM, Dontenwill M (2013) Integrin alpha5beta1, the fibronectin receptor, as a pertinent therapeutic target in solid tumors. Cancers 5(1):27–47. https://doi.org/10.3390/cancers5010027
Bhaskar V, Zhang D, Fox M, Seto P, Wong MH, Wales PE, Powers D, Chao DT, Dubridge RB, Ramakrishnan V (2007) A function blocking anti-mouse integrin alpha5beta1 antibody inhibits angiogenesis and impedes tumor growth in vivo. J Transl Med 5:61. https://doi.org/10.1186/1479-5876-5-61
Bhaskar V, Fox M, Breinberg D, Wong MH, Wales PE, Rhodes S, DuBridge RB, Ramakrishnan V (2008) Volociximab, a chimeric integrin alpha5beta1 antibody, inhibits the growth of VX2 tumors in rabbits. Invest New Drugs 26(1):7–12. https://doi.org/10.1007/s10637-007-9078-z
Stupp R, Hegi ME, Gorlia T, Erridge SC, Perry J, Hong YK, Aldape KD, Lhermitte B, Pietsch T, Grujicic D, Steinbach JP, Wick W, Tarnawski R, Nam DH, Hau P, Weyerbrock A, Taphoorn MJ, Shen CC, Rao N, Thurzo L, Herrlinger U, Gupta T, Kortmann RD, Adamska K, McBain C, Brandes AA, Tonn JC, Schnell O, Wiegel T, Kim CY, Nabors LB, Reardon DA, van den Bent MJ, Hicking C, Markivskyy A, Picard M, Weller M (2014) Cilengitide combined with standard treatment for patients with newly diagnosed glioblastoma with methylated MGMT promoter (CENTRIC EORTC 26071—22072 study): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol 15(10):1100–1108. https://doi.org/10.1016/s1470-2045(14)70379-1
Murphy PA, Begum S, Hynes RO (2015) Tumor angiogenesis in the absence of fibronectin or its cognate integrin receptors. PLoS ONE 10(3):e0120872. https://doi.org/10.1371/journal.pone.0120872
St John AL, Chan CY, Staats HF, Leong KW, Abraham SN (2012) Synthetic mast-cell granules as adjuvants to promote and polarize immunity in lymph nodes. Nat Mater 11(3):250–257. https://doi.org/10.1038/nmat3222
The FO, Bennink RJ, Ankum WM, Buist MR, Busch OR, Gouma DJ, van der Heide S, van den Wijngaard RM, de Jonge WJ, Boeckxstaens GE (2008) Intestinal handling-induced mast cell activation and inflammation in human postoperative ileus. Gut 57(1):33–40. https://doi.org/10.1136/gut.2007.120238
Ma Y, Hwang RF, Logsdon CD, Ullrich SE (2013) Dynamic mast cell-stromal cell interactions promote growth of pancreatic cancer. Cancer Res 73(13):3927–3937. https://doi.org/10.1158/0008-5472.can-12-4479
Esposito I, Menicagli M, Funel N, Bergmann F, Boggi U, Mosca F, Bevilacqua G, Campani D (2004) Inflammatory cells contribute to the generation of an angiogenic phenotype in pancreatic ductal adenocarcinoma. J Clin Pathol 57(6):630–636
Ammendola M, Sacco R, Sammarco G, Donato G, Zuccala V, Luposella M, Patruno R, Marech I, Montemurro S, Zizzo N, Gadaleta CD, Ranieri G (2014) Mast cells density positive to tryptase correlates with angiogenesis in pancreatic ductal adenocarcinoma patients having undergone surgery. Gastroenterol Res Pract 2014:951957. https://doi.org/10.1155/2014/951957
Cai SW, Yang SZ, Gao J, Pan K, Chen JY, Wang YL, Wei LX, Dong JH (2011) Prognostic significance of mast cell count following curative resection for pancreatic ductal adenocarcinoma. Surgery 149(4):576–584. https://doi.org/10.1016/j.surg.2010.10.009
Soucek L, Lawlor ER, Soto D, Shchors K, Swigart LB, Evan GI (2007) Mast cells are required for angiogenesis and macroscopic expansion of Myc-induced pancreatic islet tumors. Nat Med 13(10):1211–1218. https://doi.org/10.1038/nm1649
Guo X, Zhai L, Xue R, Shi J, Zeng Q, Gao C (2016) Mast cell tryptase contributes to pancreatic cancer growth through promoting angiogenesis via activation of angiopoietin-1. Int J Mol Sci. https://doi.org/10.3390/ijms17060834
Marech I, Ammendola M, Sacco R, Capriuolo GS, Patruno R, Rubini R, Luposella M, Zuccala V, Savino E, Gadaleta CD, Ribatti D, Ranieri G (2014) Serum tryptase, mast cells positive to tryptase and microvascular density evaluation in early breast cancer patients: possible translational significance. BMC Cancer 14:534. https://doi.org/10.1186/1471-2407-14-534
Ammendola M, Sacco R, Sammarco G, Donato G, Montemurro S, Ruggieri E, Patruno R, Marech I, Cariello M, Vacca A, Gadaleta CD, Ranieri G (2014) Correlation between serum tryptase, mast cells positive to tryptase and microvascular density in colo-rectal cancer patients: possible biological-clinical significance. PLoS ONE 9(6):e99512. https://doi.org/10.1371/journal.pone.0099512
Zambirinis CP, Levie E, Nguy S, Avanzi A, Barilla R, Xu Y, Seifert L, Daley D, Greco SH, Deutsch M, Jonnadula S, Torres-Hernandez A, Tippens D, Pushalkar S, Eisenthal A, Saxena D, Ahn J, Hajdu C, Engle DD, Tuveson D, Miller G (2015) TLR9 ligation in pancreatic stellate cells promotes tumorigenesis. J Exp Med 212(12):2077–2094. https://doi.org/10.1084/jem.20142162
Endo S, Nakata K, Ohuchida K, Takesue S, Nakayama H, Abe T, Koikawa K, Okumura T, Sada M, Horioka K, Zheng B, Mizuuchi Y, Iwamoto C, Murata M, Moriyama T, Miyasaka Y, Ohtsuka T, Mizumoto K, Oda Y, Hashizume M, Nakamura M (2017) Autophagy is required for activation of pancreatic stellate cells, associated with pancreatic cancer progression and promotes growth of pancreatic tumors in mice. Gastroenterology 152(6):1492–1506.e1424. https://doi.org/10.1053/j.gastro.2017.01.010
Qian D, Lu Z, Xu Q, Wu P, Tian L, Zhao L, Cai B, Yin J, Wu Y, Staveley-O’Carroll KF, Jiang K, Miao Y, Li G (2017) Galectin-1-driven upregulation of SDF-1 in pancreatic stellate cells promotes pancreatic cancer metastasis. Cancer Lett 397:43–51. https://doi.org/10.1016/j.canlet.2017.03.024
Ene-Obong A, Clear AJ, Watt J, Wang J, Fatah R, Riches JC, Marshall JF, Chin-Aleong J, Chelala C, Gribben JG, Ramsay AG, Kocher HM (2013) Activated pancreatic stellate cells sequester CD8+ T cells to reduce their infiltration of the juxtatumoral compartment of pancreatic ductal adenocarcinoma. Gastroenterology 145(5):1121–1132. https://doi.org/10.1053/j.gastro.2013.07.025
Mace TA, Bloomston M, Lesinski GB (2013) Pancreatic cancer-associated stellate cells: A viable target for reducing immunosuppression in the tumor microenvironment. Oncoimmunology 2(7):e24891. https://doi.org/10.4161/onci.24891
Erkan M, Adler G, Apte MV, Bachem MG, Buchholz M, Detlefsen S, Esposito I, Friess H, Gress TM, Habisch HJ, Hwang RF, Jaster R, Kleeff J, Kloppel G, Kordes C, Logsdon CD, Masamune A, Michalski CW, Oh J, Phillips PA, Pinzani M, Reiser-Erkan C, Tsukamoto H, Wilson J (2012) StellaTUM: current consensus and discussion on pancreatic stellate cell research. Gut 61(2):172–178. https://doi.org/10.1136/gutjnl-2011-301220
Haqq J, Howells LM, Garcea G, Metcalfe MS, Steward WP, Dennison AR (2014) Pancreatic stellate cells and pancreas cancer: current perspectives and future strategies. Eur J Cancer (Oxford England: 1990) 50(15):2570–2582. https://doi.org/10.1016/j.ejca.2014.06.021
Masamune A, Kikuta K, Watanabe T, Satoh K, Hirota M, Shimosegawa T (2008) Hypoxia stimulates pancreatic stellate cells to induce fibrosis and angiogenesis in pancreatic cancer. Am J Physiol Gastrointest Liver Physiol 295(4):G709–G717. https://doi.org/10.1152/ajpgi.90356.2008
Xu Z, Vonlaufen A, Phillips PA, Fiala-Beer E, Zhang X, Yang L, Biankin AV, Goldstein D, Pirola RC, Wilson JS, Apte MV (2010) Role of pancreatic stellate cells in pancreatic cancer metastasis. Am J Pathol 177(5):2585–2596. https://doi.org/10.2353/ajpath.2010.090899
Erkan M, Reiser-Erkan C, Michalski CW, Deucker S, Sauliunaite D, Streit S, Esposito I, Friess H, Kleeff J (2009) Cancer-stellate cell interactions perpetuate the hypoxia-fibrosis cycle in pancreatic ductal adenocarcinoma. Neoplasia (New York NY) 11(5):497–508
Patel MB, Pothula SP, Xu Z, Lee AK, Goldstein D, Pirola RC, Apte MV, Wilson JS (2014) The role of the hepatocyte growth factor/c-MET pathway in pancreatic stellate cell-endothelial cell interactions: antiangiogenic implications in pancreatic cancer. Carcinogenesis 35(8):1891–1900. https://doi.org/10.1093/carcin/bgu122
Pothula SP, Xu Z, Goldstein D, Biankin AV, Pirola RC, Wilson JS, Apte MV (2016) Hepatocyte growth factor inhibition: a novel therapeutic approach in pancreatic cancer. Br J Cancer 114(3):269–280. https://doi.org/10.1038/bjc.2015.478
Van Cutsem E, Vervenne WL, Bennouna J, Humblet Y, Gill S, Van Laethem JL, Verslype C, Scheithauer W, Shang A, Cosaert J, Moore MJ (2009) Phase III trial of bevacizumab in combination with gemcitabine and erlotinib in patients with metastatic pancreatic cancer. J Clin Oncol 27(13):2231–2237. https://doi.org/10.1200/jco.2008.20.0238
Kindler HL, Niedzwiecki D, Hollis D, Sutherland S, Schrag D, Hurwitz H, Innocenti F, Mulcahy MF, O’Reilly E, Wozniak TF, Picus J, Bhargava P, Mayer RJ, Schilsky RL, Goldberg RM (2010) Gemcitabine plus bevacizumab compared with gemcitabine plus placebo in patients with advanced pancreatic cancer: phase III trial of the Cancer and Leukemia Group B (CALGB 80303). J Clin Oncol 28(22):3617–3622. https://doi.org/10.1200/jco.2010.28.1386
Wen PY, Schiff D, Cloughesy TF, Raizer JJ, Laterra J, Smitt M, Wolf M, Oliner KS, Anderson A, Zhu M, Loh E, Reardon DA (2011) A phase II study evaluating the efficacy and safety of AMG 102 (rilotumumab) in patients with recurrent glioblastoma. Neuro-Oncology 13(4):437–446. https://doi.org/10.1093/neuonc/noq198
Zhu M, Tang R, Doshi S, Oliner KS, Dubey S, Jiang Y, Donehower RC, Iveson T, Loh EY, Zhang Y (2015) Exposure-response analysis of rilotumumab in gastric cancer: the role of tumour MET expression. Br J Cancer 112(3):429–437. https://doi.org/10.1038/bjc.2014.649
Gordon S, Martinez FO (2010) Alternative activation of macrophages: mechanism and functions. Immunity 32(5):593–604. https://doi.org/10.1016/j.immuni.2010.05.007
Kurahara H, Shinchi H, Mataki Y, Maemura K, Noma H, Kubo F, Sakoda M, Ueno S, Natsugoe S, Takao S (2011) Significance of M2-polarized tumor-associated macrophage in pancreatic cancer. J Surg Res 167(2):e211–e219. https://doi.org/10.1016/j.jss.2009.05.026
Yoshikawa K, Mitsunaga S, Kinoshita T, Konishi M, Takahashi S, Gotohda N, Kato Y, Aizawa M, Ochiai A (2012) Impact of tumor-associated macrophages on invasive ductal carcinoma of the pancreas head. Cancer Sci 103(11):2012–2020. https://doi.org/10.1111/j.1349-7006.2012.02411.x
Dineen SP, Lynn KD, Holloway SE, Miller AF, Sullivan JP, Shames DS, Beck AW, Barnett CC, Fleming JB, Brekken RA (2008) Vascular endothelial growth factor receptor 2 mediates macrophage infiltration into orthotopic pancreatic tumors in mice. Cancer Res 68(11):4340–4346. https://doi.org/10.1158/0008-5472.can-07-6705
Penny HL, Sieow JL, Adriani G, Yeap WH, See Chi Ee P, San Luis B, Lee B, Lee T, Mak SY, Ho YS, Lam KP, Ong CK, Huang RY, Ginhoux F, Rotzschke O, Kamm RD, Wong SC (2016) Warburg metabolism in tumor-conditioned macrophages promotes metastasis in human pancreatic ductal adenocarcinoma. Oncoimmunology 5(8):e1191731. https://doi.org/10.1080/2162402x.2016.1191731
Kurahara H, Takao S, Kuwahata T, Nagai T, Ding Q, Maeda K, Shinchi H, Mataki Y, Maemura K, Matsuyama T, Natsugoe S (2012) Clinical significance of folate receptor beta-expressing tumor-associated macrophages in pancreatic cancer. Ann Surg Oncol 19(7):2264–2271. https://doi.org/10.1245/s10434-012-2263-0
Schmid MC, Avraamides CJ, Dippold HC, Franco I, Foubert P, Ellies LG, Acevedo LM, Manglicmot JR, Song X, Wrasidlo W, Blair SL, Ginsberg MH, Cheresh DA, Hirsch E, Field SJ, Varner JA (2011) Receptor tyrosine kinases and TLR/IL1Rs unexpectedly activate myeloid cell PI3kgamma, a single convergent point promoting tumor inflammation and progression. Cancer Cell 19(6):715–727. https://doi.org/10.1016/j.ccr.2011.04.016
Schmid MC, Avraamides CJ, Foubert P, Shaked Y, Kang SW, Kerbel RS, Varner JA (2011) Combined blockade of integrin-alpha4beta1 plus cytokines SDF-1alpha or IL-1beta potently inhibits tumor inflammation and growth. Cancer Res 71(22):6965–6975. https://doi.org/10.1158/0008-5472.can-11-0588
Partecke LI, Gunther C, Hagemann S, Jacobi C, Merkel M, Sendler M, van Rooijen N, Kading A, Trung DN, Lorenz E, Diedrich S, Weiss FU, Heidecke CD, von Bernstorff W (2013) Induction of M2-macrophages by tumour cells and tumour growth promotion by M2-macrophages: a quid pro quo in pancreatic cancer. Pancreatology 13(5):508–516. https://doi.org/10.1016/j.pan.2013.06.010
Griesmann H, Drexel C, Milosevic N, Sipos B, Rosendahl J, Gress TM, Michl P (2017) Pharmacological macrophage inhibition decreases metastasis formation in a genetic model of pancreatic cancer. Gut 66(7):1278–1285. https://doi.org/10.1136/gutjnl-2015-310049
Harney AS, Karagiannis GS, Pignatelli J, Smith BD, Kadioglu E, Wise SC, Hood MM, Kaufman MD, Leary CB, Lu WP, Al-Ani G, Chen X, Entenberg D, Oktay MH, Wang Y, Chun L, De Palma M, Jones JG, Flynn DL, Condeelis JS (2017) The selective Tie2 inhibitor rebastinib blocks recruitment and function of Tie2(Hi) macrophages in breast cancer and pancreatic neuroendocrine tumors. Mol Cancer Ther 16(11):2486–2501. https://doi.org/10.1158/1535-7163.mct-17-0241
Li N, Li Y, Li Z, Huang C, Yang Y, Lang M, Cao J, Jiang W, Xu Y, Dong J, Ren H (2016) Hypoxia inducible factor 1 (HIF-1) recruits macrophage to activate pancreatic stellate cells in pancreatic ductal adenocarcinoma. Int J Mol Sci. https://doi.org/10.3390/ijms17060799
Pyonteck SM, Gadea BB, Wang HW, Gocheva V, Hunter KE, Tang LH, Joyce JA (2012) Deficiency of the macrophage growth factor CSF-1 disrupts pancreatic neuroendocrine tumor development. Oncogene 31(11):1459–1467. https://doi.org/10.1038/onc.2011.337
Casazza A, Laoui D, Wenes M, Rizzolio S, Bassani N, Mambretti M, Deschoemaeker S, Van Ginderachter JA, Tamagnone L, Mazzone M (2013) Impeding macrophage entry into hypoxic tumor areas by Sema3A/Nrp1 signaling blockade inhibits angiogenesis and restores antitumor immunity. Cancer Cell 24(6):695–709. https://doi.org/10.1016/j.ccr.2013.11.007
Qian B, Deng Y, Im JH, Muschel RJ, Zou Y, Li J, Lang RA, Pollard JW (2009) A distinct macrophage population mediates metastatic breast cancer cell extravasation, establishment and growth. PLoS ONE 4(8):e6562. https://doi.org/10.1371/journal.pone.0006562
Bausch D, Pausch T, Krauss T, Hopt UT, Fernandez-del-Castillo C, Warshaw AL, Thayer SP, Keck T (2011) Neutrophil granulocyte derived MMP-9 is a VEGF independent functional component of the angiogenic switch in pancreatic ductal adenocarcinoma. Angiogenesis 14(3):235–243. https://doi.org/10.1007/s10456-011-9207-3
Tong Z, Kunnumakkara AB, Wang H, Matsuo Y, Diagaradjane P, Harikumar KB, Ramachandran V, Sung B, Chakraborty A, Bresalier RS, Logsdon C, Aggarwal BB, Krishnan S, Guha S (2008) Neutrophil gelatinase-associated lipocalin: a novel suppressor of invasion and angiogenesis in pancreatic cancer. Cancer Res 68(15):6100–6108. https://doi.org/10.1158/0008-5472.can-08-0540
Heath VL, Bicknell R (2009) Anticancer strategies involving the vasculature. Nat Rev Clin Oncol 6(7):395–404. https://doi.org/10.1038/nrclinonc.2009.52
Ivy SP, Wick JY, Kaufman BM (2009) An overview of small-molecule inhibitors of VEGFR signaling. Nat Rev Clin Oncol 6(10):569–579. https://doi.org/10.1038/nrclinonc.2009.130
Kindler HL, Ioka T, Richel DJ, Bennouna J, Letourneau R, Okusaka T, Funakoshi A, Furuse J, Park YS, Ohkawa S, Springett GM, Wasan HS, Trask PC, Bycott P, Ricart AD, Kim S, Van Cutsem E (2011) Axitinib plus gemcitabine versus placebo plus gemcitabine in patients with advanced pancreatic adenocarcinoma: a double-blind randomised phase 3 study. Lancet Oncol 12(3):256–262. https://doi.org/10.1016/s1470-2045(11)70004-3
Goncalves A, Gilabert M, Francois E, Dahan L, Perrier H, Lamy R, Re D, Largillier R, Gasmi M, Tchiknavorian X, Esterni B, Genre D, Moureau-Zabotto L, Giovannini M, Seitz JF, Delpero JR, Turrini O, Viens P, Raoul JL (2012) BAYPAN study: a double-blind phase III randomized trial comparing gemcitabine plus sorafenib and gemcitabine plus placebo in patients with advanced pancreatic cancer. Ann Oncol 23(11):2799–2805. https://doi.org/10.1093/annonc/mds135
Rougier P, Riess H, Manges R, Karasek P, Humblet Y, Barone C, Santoro A, Assadourian S, Hatteville L, Philip PA (2013) Randomised, placebo-controlled, double-blind, parallel-group phase III study evaluating aflibercept in patients receiving first-line treatment with gemcitabine for metastatic pancreatic cancer. Eur J Cancer (Oxford England 1990) 49(12):2633–2642. https://doi.org/10.1016/j.ejca.2013.04.002
Yamaue H, Tsunoda T, Tani M, Miyazawa M, Yamao K, Mizuno N, Okusaka T, Ueno H, Boku N, Fukutomi A, Ishii H, Ohkawa S, Furukawa M, Maguchi H, Ikeda M, Togashi Y, Nishio K, Ohashi Y (2015) Randomized phase II/III clinical trial of elpamotide for patients with advanced pancreatic cancer: PEGASUS-PC Study. Cancer Sci 106(7):883–890. https://doi.org/10.1111/cas.12674
Folkman J (1971) Tumor angiogenesis: therapeutic implications. N Engl J Med 285(21):1182–1186. https://doi.org/10.1056/nejm197111182852108
Giantonio BJ, Catalano PJ, Meropol NJ, O’Dwyer PJ, Mitchell EP, Alberts SR, Schwartz MA, Benson AB 3rd (2007) Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: results from the Eastern Cooperative Oncology Group Study E3200. J Clin Oncol 25(12):1539–1544. https://doi.org/10.1200/jco.2006.09.6305
Cohen MH, Shen YL, Keegan P, Pazdur R (2009) FDA drug approval summary: bevacizumab (Avastin) as treatment of recurrent glioblastoma multiforme. Oncologist 14(11):1131–1138. https://doi.org/10.1634/theoncologist.2009-0121
Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A, Schwartz M, Porta C, Zeuzem S, Bolondi L, Greten TF, Galle PR, Seitz JF, Borbath I, Haussinger D, Giannaris T, Shan M, Moscovici M, Voliotis D, Bruix J (2008) Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 359(4):378–390. https://doi.org/10.1056/NEJMoa0708857
Herbst RS, Sun Y, Eberhardt WE, Germonpre P, Saijo N, Zhou C, Wang J, Li L, Kabbinavar F, Ichinose Y, Qin S, Zhang L, Biesma B, Heymach JV, Langmuir P, Kennedy SJ, Tada H, Johnson BE (2010) Vandetanib plus docetaxel versus docetaxel as second-line treatment for patients with advanced non-small-cell lung cancer (ZODIAC): a double-blind, randomised, phase 3 trial. Lancet Oncol 11(7):619–626. https://doi.org/10.1016/s1470-2045(10)70132-7
Paez-Ribes M, Allen E, Hudock J, Takeda T, Okuyama H, Vinals F, Inoue M, Bergers G, Hanahan D, Casanovas O (2009) Antiangiogenic therapy elicits malignant progression of tumors to increased local invasion and distant metastasis. Cancer Cell 15(3):220–231. https://doi.org/10.1016/j.ccr.2009.01.027
Ebos JM, Lee CR, Cruz-Munoz W, Bjarnason GA, Christensen JG, Kerbel RS (2009) Accelerated metastasis after short-term treatment with a potent inhibitor of tumor angiogenesis. Cancer cell 15(3):232–239. https://doi.org/10.1016/j.ccr.2009.01.021
Ribatti D (2011) Antiangiogenic therapy accelerates tumor metastasis. Leuk Res 35(1):24–26. https://doi.org/10.1016/j.leukres.2010.07.038
Shao YY, Lu LC, Cheng AL, Hsu CH (2011) Increasing incidence of brain metastasis in patients with advanced hepatocellular carcinoma in the era of antiangiogenic targeted therapy. Oncologist 16(1):82–86. https://doi.org/10.1634/theoncologist.2010-0272
Zhu XD, Sun HC, Xu HX, Kong LQ, Chai ZT, Lu L, Zhang JB, Gao DM, Wang WQ, Zhang W, Zhuang PY, Wu WZ, Wang L, Tang ZY (2013) Antiangiogenic therapy promoted metastasis of hepatocellular carcinoma by suppressing host-derived interleukin-12b in mouse models. Angiogenesis 16(4):809–820. https://doi.org/10.1007/s10456-013-9357-6
Yin T, He S, Ye T, Shen G, Wan Y, Wang Y (2014) Antiangiogenic therapy using sunitinib combined with rapamycin retards tumor growth but promotes metastasis. Transl Oncol 7(2):221–229. https://doi.org/10.1016/j.tranon.2014.02.007
Rofstad EK, Gaustad JV, Egeland TA, Mathiesen B, Galappathi K (2010) Tumors exposed to acute cyclic hypoxic stress show enhanced angiogenesis, perfusion and metastatic dissemination. Int J Cancer 127(7):1535–1546. https://doi.org/10.1002/ijc.25176
Shojaei F, Wu X, Qu X, Kowanetz M, Yu L, Tan M, Meng YG, Ferrara N (2009) G-CSF-initiated myeloid cell mobilization and angiogenesis mediate tumor refractoriness to anti-VEGF therapy in mouse models. Proc Natl Acad Sci USA 106(16):6742–6747. https://doi.org/10.1073/pnas.0902280106
Joyce JA, Pollard JW (2009) Microenvironmental regulation of metastasis. Nat Rev Cancer 9(4):239–252. https://doi.org/10.1038/nrc2618
Galluzzo M, Pennacchietti S, Rosano S, Comoglio PM, Michieli P (2009) Prevention of hypoxia by myoglobin expression in human tumor cells promotes differentiation and inhibits metastasis. J Clin Invest 119(4):865–875. https://doi.org/10.1172/jci36579
Kaplan RN, Riba RD, Zacharoulis S, Bramley AH, Vincent L, Costa C, MacDonald DD, Jin DK, Shido K, Kerns SA, Zhu Z, Hicklin D, Wu Y, Port JL, Altorki N, Port ER, Ruggero D, Shmelkov SV, Jensen KK, Rafii S, Lyden D (2005) VEGFR1-positive haematopoietic bone marrow progenitors initiate the pre-metastatic niche. Nature 438(7069):820–827. https://doi.org/10.1038/nature04186
Bergers G, Hanahan D (2008) Modes of resistance to anti-angiogenic therapy. Nat Rev Cancer 8(8):592–603. https://doi.org/10.1038/nrc2442
Martinez-Outschoorn UE, Whitaker-Menezes D, Pavlides S, Chiavarina B, Bonuccelli G, Casey T, Tsirigos A, Migneco G, Witkiewicz A, Balliet R, Mercier I, Wang C, Flomenberg N, Howell A, Lin Z, Caro J, Pestell RG, Sotgia F, Lisanti MP (2010) The autophagic tumor stroma model of cancer or “battery-operated tumor growth”: A simple solution to the autophagy paradox. Cell Cycle (Georgetown Tex) 9(21):4297–4306. https://doi.org/10.4161/cc.9.21.13817
Reynolds AR, Hart IR, Watson AR, Welti JC, Silva RG, Robinson SD, Da Violante G, Gourlaouen M, Salih M, Jones MC, Jones DT, Saunders G, Kostourou V, Perron-Sierra F, Norman JC, Tucker GC, Hodivala-Dilke KM (2009) Stimulation of tumor growth and angiogenesis by low concentrations of RGD-mimetic integrin inhibitors. Nat Med 15(4):392–400. https://doi.org/10.1038/nm.1941
Elice F, Rodeghiero F, Falanga A, Rickles FR (2009) Thrombosis associated with angiogenesis inhibitors. Best Pract Res Clin Haematol 22(1):115–128. https://doi.org/10.1016/j.beha.2009.01.001
Nagathihalli NS, Castellanos JA, Shi C, Beesetty Y, Reyzer ML, Caprioli R, Chen X, Walsh AJ, Skala MC, Moses HL, Merchant NB (2015) Signal transducer and activator of transcription 3, mediated remodeling of the tumor microenvironment results in enhanced tumor drug delivery in a mouse model of pancreatic cancer. Gastroenterology 149(7):1932.e1939–1943.e1939. https://doi.org/10.1053/j.gastro.2015.07.058
Hamzah J, Jugold M, Kiessling F, Rigby P, Manzur M, Marti HH, Rabie T, Kaden S, Grone HJ, Hammerling GJ, Arnold B, Ganss R (2008) Vascular normalization in Rgs5-deficient tumours promotes immune destruction. Nature 453(7193):410–414. https://doi.org/10.1038/nature06868
Huang Y, Snuderl M, Jain RK (2011) Polarization of tumor-associated macrophages: a novel strategy for vascular normalization and antitumor immunity. Cancer Cell 19(1):1–2. https://doi.org/10.1016/j.ccr.2011.01.005
Huang Y, Goel S, Duda DG, Fukumura D, Jain RK (2013) Vascular normalization as an emerging strategy to enhance cancer immunotherapy. Cancer Res 73(10):2943–2948. https://doi.org/10.1158/0008-5472.can-12-4354
Wang WQ, Liu L, Sun HC, Fu YL, Xu HX, Chai ZT, Zhang QB, Kong LQ, Zhu XD, Lu L, Ren ZG, Tang ZY (2012) Tanshinone IIA inhibits metastasis after palliative resection of hepatocellular carcinoma and prolongs survival in part via vascular normalization. J Hematol Oncol 5:69. https://doi.org/10.1186/1756-8722-5-69
Zhang H, Ren Y, Tang X, Wang K, Liu Y, Zhang L, Li X, Liu P, Zhao C, He J (2015) Vascular normalization induced by sinomenine hydrochloride results in suppressed mammary tumor growth and metastasis. Sci Rep 5:8888. https://doi.org/10.1038/srep08888
Carmeliet P, Jain RK (2011) Principles and mechanisms of vessel normalization for cancer and other angiogenic diseases. Nat Rev Drug Discov 10(6):417–427. https://doi.org/10.1038/nrd3455
Astsaturov IA, Meropol NJ, Alpaugh RK, Burtness BA, Cheng JD, McLaughlin S, Rogatko A, Xu Z, Watson JC, Weiner LM, Cohen SJ (2011) Phase II and coagulation cascade biomarker study of bevacizumab with or without docetaxel in patients with previously treated metastatic pancreatic adenocarcinoma. Am J Clin Oncol 34(1):70–75. https://doi.org/10.1097/COC.0b013e3181d2734a
Dragovich T, Laheru D, Dayyani F, Bolejack V, Smith L, Seng J, Burris H, Rosen P, Hidalgo M, Ritch P, Baker AF, Raghunand N, Crowley J, Von Hoff DD (2014) Phase II trial of vatalanib in patients with advanced or metastatic pancreatic adenocarcinoma after first-line gemcitabine therapy (PCRT O4-001). Cancer Chemother Pharmacol 74(2):379–387. https://doi.org/10.1007/s00280-014-2499-4
Lassau N, Coiffier B, Kind M, Vilgrain V, Lacroix J, Cuinet M, Taieb S, Aziza R, Sarran A, Labbe-Devilliers C, Gallix B, Lucidarme O, Ptak Y, Rocher L, Caquot LM, Chagnon S, Marion D, Luciani A, Feutray S, Uzan-Augui J, Benatsou B, Bonastre J, Koscielny S (2016) Selection of an early biomarker for vascular normalization using dynamic contrast-enhanced ultrasonography to predict outcomes of metastatic patients treated with bevacizumab. Ann Oncol 27(10):1922–1928. https://doi.org/10.1093/annonc/mdw280
Gore J, Craven KE, Wilson JL, Cote GA, Cheng M, Nguyen HV, Cramer HM, Sherman S, Korc M (2015) TCGA data and patient-derived orthotopic xenografts highlight pancreatic cancer-associated angiogenesis. Oncotarget 6(10):7504–7521. https://doi.org/10.18632/oncotarget.3233
Acknowledgements
This work was supported by grants from the National Science Foundation for Distinguished Young Scholars of China (81625016), the National Natural Science Foundation of China (81472670, 81402397, and 81402398), the National Natural Science Foundation of Shanghai (14ZR1407600), and the “Yang-Fan” Plan for Young Scientists of Shanghai (14YF1401100).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Li, S., Xu, HX., Wu, CT. et al. Angiogenesis in pancreatic cancer: current research status and clinical implications. Angiogenesis 22, 15–36 (2019). https://doi.org/10.1007/s10456-018-9645-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10456-018-9645-2