
Abstract
Aim
This article describes the German recommendations for physical activity promotion. Such recommendations serve as an important stepping stone to increase physical activity prevalences on the population level.
Subjects and methods
The German recommendations for physical activity promotion are based on three separate reviews: (1) a systematic review of reviews to formulate recommendations on the efficacy and effectiveness of interventions for physical activity promotion, which included 213 reviews; (2) a systematic review of reviews to investigate the cost-effectiveness of interventions for the promotion of physical activity, comprising of 18 reviews; (3) a review to identify literature on quality criteria for the conceptualisation, implementation and evaluation of interventions for physical activity promotion, which encompassed 24 studies and documents. Through an expert consensus panel, findings from each review were utilised to formulate specific recommendations for Germany.
Results
Recommendations for physical activity promotion are provided for the following target groups: children and adolescents, adults, older adults, adults with a chronic disease and the general population. For each target group, other than the general population, the recommendations are structured by setting. Alongside recommendations on the efficacy and effectiveness of interventions, recommendations were also formulated for health equity, cost-effectiveness and quality criteria.
Conclusion
From a political perspective, the development of recommendations for physical activity promotion highlights an important milestone for Germany. Not only do the national recommendations describe the amount of physical activity people should engage in, but they also provide organisations with information on how to support people in becoming more active.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
In the field of physical activity (PA), two types of recommendation can be distinguished. According to Leon and Pesce (2017), the first type—physical activity recommendations—can be described as an evidence-based, clinically guided framework that centres on the nature, duration, intensity and volume of PA. Such recommendations focus on health-enhancing levels of PA by providing specific guidance on PA amounts and modalities through different fitness levels and age groups (Leon and Pesce 2017). The World Health Organisation (WHO) has urged nations to develop PA recommendations (WHO 2004), with a number of nations already having done so. For example, out of 37 European nations, 21 currently adopt this form of recommendation (Kahlmeier et al. 2015).
The second type of recommendation concerns physical activity promotion. This type attends to stakeholders such as practitioners, professionals and organisations involved with health prevention and promotion as well as political decision-makers and institutions. Recommendations for PA promotion target evidence-based interventions in specific settings and concentrate on daily living. The intention is not to define PA practice in terms of amount and frequency, but to inform policy on how to promote health-enhancing PA (Leon and Pesce 2017). Nations have been called upon to increase efforts for PA promotion, and guiding documents have been developed on the supranational level (European Commission 2008; Council of the European Union 2013; WHO 2009). On a national level, however, recommendations on how to promote PA are rarely seen. For example, the UK and the USA have published guidance on PA promotion (e.g. CDC 2011; NICE 2008), but PA and PA promotion recommendations have not been integrated into one single document.
From a Public Health perspective, the development of national recommendations for PA promotion can be challenging. This is due to several key points that need to be considered regarding the formulation of recommendations for physical activity promotion. First, it is essential that the efficacy of recommended interventions has been demonstrated. Commonly, intervention efficacy is shown in trials that utilise randomised and/or controlled designs. However, interventions should also prove that they are effective outside of the laboratory setting and can actually be implemented as part of public health practice (Flay 1986). Alongside efficacy and effectiveness, it is important to comprehend the effects that PA interventions have on existing health inequalities. Doing so will admit the formulation of PA recommendations that are potentially able to address and reduce health inequalities. From a governmental perspective, the promotion of PA also needs be cost-effective. In this regard, the costs and benefits of different PA interventions should be compared. Alongside efficacy, effectiveness, cost-effectiveness and impact on health equity, the success of an intervention will also depend on implementation.
In Germany, increases in political effort centred around PA promotion have been seen in recent years through collaboration between the Federal Ministry of Health—responsible for PA promotion in Germany—and the Federal Ministry of Nutrition. This heightened level of engagement can be partially credited for the development of national recommendations on PA and PA promotion. The decision to formulate the recommendations was supported by Germany’s Conference of Health Ministers and Germany’s Conference of Sport Ministers (2015). It was agreed that such recommendations should serve as a scientific guide for stakeholders and organisations within Germany to support the development of future activities in the field.
Regarding PA prevalence, Germany is comparable to other European nations. For example, 1/4 of boys and 1/6 of girls are sufficiently active in their leisure time (Lampert et al. 2007). Furthermore, 1/5 of women and 1/4 of men meet WHO PA recommendations (Finger et al. 2017). Considering PA patterns, a large proportion of the German population is active in sport clubs (27 Million people in 2017) (DOSB 2018). Moreover, Germany shows higher than average rates in reported exercise (European Commission 2014) or cycling (European Commission 2013) compared with other European nations.
This article describes the developmental process that resulted in the formulation of German recommendations for physical activity promotion. It is important to mention that reviews of reviews on interventions for PA promotion have already been conducted. These reviews deal partly with interventions that take place in a specific setting such as schools (e.g. Kriemler et al. 2011) or childcare facilities (e.g. Steenbock et al. 2014). Others deal with PA promotion across different settings, but are limited by focusing solely on efficacy/effectiveness (e.g. Heath et al. 2012; Jepson et al. 2010) or health equity (e.g. Lorenc et al. 2012). Differing from other reviews of reviews, our work encompasses a life course perspective and considers efficacy, effectiveness, health equity, cost-effectiveness and quality criteria of interventions for the promotion of PA. It reports on PA interventions for the target groups of children and adolescents, adults, older people, adults with a chronic disease and the general population. The process and results described could support other nations in the development of their own recommendations for physical activity promotion.
Methods
Three separate reviews were conducted, which were drawn upon for the overall formulation of recommendations for physical activity promotion. A brief description of the methodology employed for each separate review, as well as the process to build an expert consensus that followed to formulate the recommendations, can be found below. A more detailed description can be found elsewhere (Abu-Omar et al. 2017a, b; Messing and Rütten 2017).
Efficacy/effectiveness
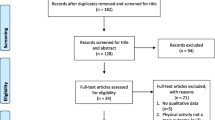
First, a systematic review of reviews was conducted to support the formulation of recommendations that centre on the efficacy and effectiveness of interventions (Abu-Omar et al. 2017a). Six electronic databases (PubMed, Scopus, Sport Discus, PsycInfo, ERIC, IBSS) were searched. In collaboration with a university librarian, the following search terms were agreed upon: “physical activity”, “intervention”, “evidence”, “effect”, “health” and “review”. Alternative terms (e.g. bike, biking, cycling, walking, active transport, human powered transport, sedentary, exercise, sport) were defined and MESH terms were formulated. Two independent reviewers screened the titles and abstracts deriving from the obtained literature and excluded duplicates. The screening process was based on the following criteria: (1) the review contains empirical results from single studies; (2) the review includes interventions focused on the promotion of PA or the reduction of inactivity; (3) the review focuses on the efficacy and/or effectiveness of interventions; (4) reviews are written in English or German.
To ensure the above inclusion criteria were met, the titles and abstracts of the identified records were screened. In a secondary screening process, two reviewers independently screened full texts from 223 reviews. Hand searches were conducted to identify additional reviews. The 213 remaining reviews were then categorised by target group (children and adolescents, adults, older people, adults with a chronic disease, general population). Review quality was assessed by one independent researcher using the AGREE instrument (The AGREE Collaboration 2003), which was also utilised in the formulation of the Canadian Physical Activity Guidelines (Tremblay et al. 2010). For each target group, two researchers independently evaluated the reviews by following the methodology proposed by Smith et al. (2011).
Cost-effectiveness
A second systematic review of reviews was conducted to investigate the cost-effectiveness of interventions for the promotion of PA (Abu-Omar et al. 2017b). Ten electronic databases were searched: PubMed, Scopus, EBSCOhost, PsychInfo, SPORTDiscus, EBSCON-ECON LIT, Pro-Quest, ERIC, IBSS and NH-SEED. Included search terms comprised of “physical activity”, “cost”, “intervention”, “systematic review” and “health outcome”. Alternative terms were included and MESH terms were formulated. From the 762 identified reviews, titles and abstracts were screened and 247 duplicates were removed. In a screening process, two independent reviewers applied the following inclusion criteria: (1) reviews are written in English or German; (2) reviews model or summarise the health economic evaluation of interventions for PA promotion; (3) reviews document their search strategy and state inclusion/exclusion criteria; (4) The objective of interventions is to increase PA and/or improve health; (5) interventions target healthy individuals. Of the 515 remaining reviews, researchers agreed on 8 that met the above inclusion criteria. A hand search was conducted and ten additional reviews were identified. One independent reviewer assessed the quality of the 18 included reviews by following the National Collaborating Centre for Methods and Tools (2008).
Quality criteria
A third review was conducted to identify literature on quality criteria for the conceptualisation, implementation and evaluation of interventions for PA promotion (Messing and Rütten 2017). This review followed the methodology of a state-of-the-art review (Grant and Booth 2009). A systematic search was conducted in the electronic databases PubMed and Scopus. A Google search was also conducted to include English and German publications that (1) have been issued by governmental and non-governmental organisations and (2) have not been published in scientific journals. Included search terms comprised the following: “physical activity promotion”, “sitting”, “health promotion”, “quality criteria” and “good practice”. Fifty-five documents were identified and screened in a process that applied the following inclusion criteria: The document contains quality criteria focused on the conceptualisation, implementation and evaluation of interventions for PA promotion. Thirty-eight documents met the inclusion criteria for analysis in a secondary step. This process led to the exclusion of another 14 documents, which either did not meet the inclusion criteria or were classified as dated. With emphasis on quality criteria, the formulation of the recommendations occurred through the analysis of the 24 final included documents.
Expert consensus
Based on these three literature reviews, National Recommendations for Physical Activity Promotion were formulated by a range of experts. Based on prior expertise, two reviewers were assigned to assess the efficacy/effectiveness of reviews for a specific target group (e.g. children and adolescents). Once assigned to a target group, both reviewers underwent a systematic reviewing process: (1) conduction of an independent review of the identified literature and compilation of a draft summary statement; (2) a meeting comprising both reviewers to discuss statements and agree on a conjointly revised summary statement; (3) presentation and discussion of the summary statement with reviewers assigned to other target groups. Further adjustments were made to each summary statement through necessary feedback. (4) Conduction of a workshop meeting to present each summary statement to the whole project group (including scientists involved in drafting the PA recommendations) as well as an International Scientific Advisory Board. Each summary statement was revised on the basis of expert feedback. (5) Drafting of recommendations for each target group using the finalised summary statements. A template specifying how to draft the recommendations was developed and provided by project leaders. (6) Circulation of the drafted recommendations for review by the whole project group as well as the International Scientific Advisory Board.
Regarding cost-effectiveness and quality criteria, the same reviewers assigned for each target group were provided with analysis results deriving from the respective reviews. Reviewers sorted through results and selected outcomes relevant to their target group and also searched for additional target group-related information. Through this process, recommendations on cost-effectiveness and quality criteria were formulated.
Regarding health equity, the same reviewers assigned for each target group analysed the results of the systematic review of reviews for efficacy/effectiveness. Based on the selected results and the obtainement of additional information from the original reviews, recommendations on health equity were formulated.
Recommendations were made when both reviewers rated the available evidence as strong or medium based on the following criteria: (1) the number of available reviews focusing on a given intervention type is sufficient to formulate recommendations; (2) the reviews show conclusive evidence for efficacy and/or effectiveness. Recommendations were not made when the above criteria were not fulfilled (weak or inconclusive evidence).
Results
General results on cost-effectiveness
The cost-effectiveness of an intervention was analysed by comparing the intervention costs to the expected intervention benefit. The key results of a systematic review of reviews (Abu-Omar et al. 2017b) informed the recommendations regarding cost-effectiveness. In short, the results have been summarised as follows: low-cost interventions (e.g. playground markings on existing schoolyards compared with building new playgrounds) and regulatory measures (e.g. policies for active breaks) were identified as being more cost-effective across different target groups. Interventions that are rather brief and reach a wider population (e.g. point-of-decision prompts) were also defined as cost-effective. Costly interventions might be appropriate for target groups that cannot be reached by simplistic measures or high-risk groups.
General results on quality criteria
The success of an intervention also depends on the quality of implementation. Based on a state-of-the-art review, a list of 18 evidence-based quality criteria was developed for the conceptualisation, implementation and evaluation of interventions for PA promotion. The key results of this study (Messing and Rütten 2017) were integrated into the formulation of the recommendations by defining quality criteria that are most relevant to the respective target group.
General results on health equity
Recommendations were formulated regarding the health equity of different interventions. Due to the small amount of available research, evidence was insufficient to define specific recommendations for each target group. Our analysis indicates three findings: (1) environmental approaches seem to address health inequalities better than behavioural and/or individual approaches (Lorenc et al. 2012); (2) health equity can be promoted by interventions that directly address socially disadvantaged groups (Durand et al. 2014); (3) interventions should enable the target group to actively participate in decisions concerning conceptualisation and implementation (Durand et al. 2014).
Children and adolescents
Based on the number of empirical studies on PA promotion, research pertaining to the target group of children and adolescents is clearly dominant (Rütten et al. 2016). This is due to the extent of school-related research (WHO 2009).
The formulation of recommendations for physical activity promotion among children and adolescents was based on 39 reviews. Of those 39, 3 were reviews of reviews (Heath et al. 2012; Kriemler et al. 2011; Steenbock et al. 2014); 33 were systematic reviews, with 6 having conducted a meta-analysis (Beets et al. 2009; Cushing et al. 2014; Kamath et al. 2008; Lonsdale et al. 2013; van Grieken et al. 2012; Waters et al. 2014). The other three were non-systematic reviews (Public Health England 2015; Trost et al. 2010; Ward et al. 2010). Of the 39 reviews, 28 dealt with PA promotion in schools (Atkin et al. 2011; Barr-Anderson et al. 2011; Beets et al. 2009; Brennan et al. 2014; Broekhuizen et al. 2014; Chillón et al. 2011; Crutzen 2010; De Meester et al. 2009; Dobbins et al. 2009, 2013; Dudley et al. 2011; Escalante et al. 2014; Heath et al. 2012; Kriemler et al. 2011; Langford et al. 2014; Larouche et al. 2014; Lonsdale et al. 2013; Naylor et al. 2015; Parrish et al. 2013; Pate et al. 2011; Public Health England 2015; Quitério 2013; Salmon et al. 2007; van Grieken et al. 2012; Van Lippevelde et al. 2012; van Sluijs et al. 2008; Waters et al. 2014; WHO 2009), 4 reviews were based on childcare (Ling et al. 2015; Mehtälä et al. 2014; Steenbock et al. 2014; Ward et al. 2010), and 3 reviews focused on the family and home setting (Marsh et al. 2014; Mitchell et al. 2012; Xu et al. 2015). The four remaining reviews attended to interventions that address multiple health behaviours (Cushing et al. 2014; Hillier-Brown et al. 2014), obesity prevention (Kamath et al. 2008) and computer-based interventions (Hamel et al. 2011).
Recommendations were drafted for the family and home setting, childcare facilities and schools (see Table 1). In particular, the school setting has proved to be central in the promotion of PA among children and adolescents. Due to the large number of identified reviews, strong evidence exists in this setting for the development of specific recommendations. The recommendations for the family and home setting and childcare facilities are based on a small number of studies that place emphasis on the individual level (medium evidence). Additionally, specific recommendations were formulated based on the cost-effectiveness of interventions and quality criteria for effective implementation. Due to the low number of available studies (weak evidence), recommendations were not made for computer-based interventions and health equity.
Adults
The formulation of recommendations for physical activity promotion among adults was based on 45 reviews. Of those 45, 5 were reviews of reviews (Brand et al. 2014; Heath et al. 2012; Jepson et al. 2010; Kahn et al. 2002; WHO 2009); 25 reviews analysed PA counselling and exercise programmes (Adams and White 2003; Anokye et al. 2012; Barr-Anderson et al. 2011; Bully et al. 2015; CADTH 2014; Campbell et al. 2012; Chau et al. 2010; Conn et al. 2009; Dishman et al. 1998; Engbers et al. 2005; Fry and Neff 2009; Lin et al. 2010; Malik et al. 2014; Marshall 2004; Morgan 2005; Morton et al. 2014; Orrow et al. 2012; Passon et al. 2011; Pronk 2009; Proper et al. 2003; Schroer et al. 2014; Senore et al. 2012; Shrestha et al. 2015; Stensel 2009; Wong et al. 2012), 7 reviews pertained to technology-based interventions (Broekhuizen et al. 2012; Cavill et al. 2012; Eakin et al. 2007; Maher et al. 2014; Neville et al. 2009; van den Berg et al. 2007; Vandelanotte et al. 2007), 3 reviews were pedometer-based interventions (Bravata et al. 2007; Freak-Poli et al. 2013; Kang et al. 2009), and 2 reviews addressed the topic of health equity (Cleland et al. 2013; WHO Europe 2013). The three remaining reviews dealt with different settings or specific intervention types (Matson-Koffman et al. 2005; Mitchell et al. 2013; Webel et al. 2010). It was striking to see that although a many reviews focused on a particular setting (13 workplace, 7 health care), most of them did not analyse the intervention type. For example, one meta-analysis showed that PA interventions at the workplace can be effective without comparing the effects of different intervention types (Conn et al. 2009).
Recommendations were defined for the workplace setting as well as for PA counselling and exercise programmes in different settings (Table 2). These recommendations are based on medium-level evidence. Additionally, specific recommendations were formulated regarding both cost-effectiveness of interventions and quality criteria for effective implementation. Due to the low number of available studies (weak evidence), recommendations were not made for health equity.
Older adults
The formulation of recommendations for physical activity promotion among older adults was based on ten reviews. Of those ten, four reviews dealt with general interventions for PA promotion (Cyarto et al. 2004; Hobbs et al. 2013; Morgan 2005; WHO 2009), with four reviews focusing on interventions in the health care setting (Arbesman and Mosley 2012; Hinrichs and Brach 2012; Neidrick et al. 2012; Stevens et al. 2014). The remaining reviews dealt with specific intervention types (Clark et al. 2012) and quality criteria for interventions based on PA promotion (Marques et al. 2011).
Recommendations were put forward for PA counselling and exercise programmes in different settings (Table 3). These recommendations are based on medium-level evidence. Additionally, specific recommendations were formulated for both the cost-effectiveness of interventions and quality criteria for effective implementation. Due to the low number of available studies (weak evidence), recommendations were not made for health equity.
Adults with a chronic disease
The formulation of recommendations for physical activity promotion among adults with chronic disease was based on 26 reviews. From those 26, 2 reviews focused on general interventions for PA promotion (Conn et al. 2009; Leidy et al. 2014), whereas 9 reviews dealt with interventions that address adults with one specific chronic disease (Aldcroft et al. 2011; Beinart et al. 2013; Cox et al. 2013; Cramp et al. 2013; Iversen et al. 2012; Kavookjian et al. 2007; Morris et al. 2014; Short et al. 2013; ter Hoeve et al. 2015). Nine reviews addressed the primary care setting (Ashenden et al. 1997; Hudon et al. 2008; McGrane et al. 2015; Morgan 2005; Neidrick et al. 2012; Orrow et al. 2012; Pavey et al. 2011; Smith 2004; Sorensen et al. 2006), with the six remaining reviews concentrating on specific intervention types (Bossen et al. 2014; Mansi et al. 2014; Mastellos et al. 2014; Munro et al. 2013; O'Halloran et al. 2014; Sargent et al. 2012).
Recommendations were made for interventions in health care institutions (Table 4). These recommendations are based on medium-level evidence. Additionally, specific recommendations were formulated for both the cost-effectiveness of interventions and quality criteria for effective implementation. Due to the low number of available studies (weak evidence), recommendations were not made for health equity.
General population
Due to the extent of reach, PA-promoting interventions targeting the general population present high public health potential. However, scientifically analysing the efficacy of policy and environmental interventions is very difficult using an experimental design. As a consequence, prioritising experimental studies would lead to the prioritisation of intervention strategies that are least relevant for public health and health promotion. To counter this dilemma, reviews that allowed a broad range of study designs were also taken into account.
The formulation of recommendations for physical activity promotion among the general population was based on 31 reviews. Ten reviews cover a broad range of population-based interventions (Baker et al. 2011, 2015; Heath et al. 2012; Jepson et al. 2010; Lorenc et al. 2012; Mozaffarian et al. 2012; NICE 2008; Reynolds et al. 2014; WHO 2009; Zaza et al. 2005), with the other 21 reviews focusing on one specific intervention type. Of these 21 reviews, 5 deal with the promotion of active transport (de Nazelle et al. 2011; Fraser and Lock 2010; Ogilvie et al. 2007; Pucher et al. 2010; Yang et al. 2011), 2 with infrastructures (Lee and Maheswaran 2010; McCormak and Shiell 2011), 1 with economic instruments (Shemilt et al. 2013), 3 with mass-media campaigns (Abioye et al. 2013; Brown et al. 2012; Leavy et al. 2011), 3 with sport organisations or sport events (Jackson et al. 2005; Murphy and Bauman 2007; Priest et al. 2008), 4 with intersectoral policy (Chircop et al. 2014; Durlak and DuPre 2008; Naylor et al. 2015; Shankardass et al. 2015) and 3 with health equity (Durand et al. 2014; Hillier-Brown et al. 2014; WHO Europe 2013).
Recommendations were made for mass-media campaigns, point-of-decision prompts, community-based multi-component approaches, environmental approaches, policy approaches and PA promotion through sport clubs (Table 5). These recommendations are based on medium-level evidence. Additionally, specific recommendations were formulated for health equity, the cost-effectiveness of interventions and quality criteria for the effective implementation of interventions.
Discussion
The above-described recommendations for physical activity promotion were centred on three reviews. Investigation into existing evidence for PA interventions was undergone regarding efficacy/effectiveness, cost-effectiveness, impacts on health inequalities and quality criteria for implementation. The main purpose of this investigation was to generate a robust evidence base for the comprehensive formulation of PA recommendations. To our knowledge, such a rigorous process to incorporate recommendations for physical activity and physical activity promotion has not been conducted in other nations. The effective process employed to draft the recommendations may thus serve as helpful guidance for nations looking to adopt a similar strategy for the formulation of national PA recommendations.
Conducting this review of reviews helped shed light on a number of research gaps:
-
(1)
A vast majority of identified reviews dealt with issues relating to the efficacy of PA interventions. Considerably less is known about the effectiveness of PA interventions. Reviews that deal with issues focused on the health equity of PA interventions are currently scarce. A number of reviews address the issue of cost-effectiveness, but research is currently limited for certain interventions in the field (e.g. policy and environmental).
-
(2)
By capturing the life course perspective, differences were exposed with respect to the amount of reviews available by target group. Regarding the efficacy of PA interventions, approximately 40 reviews dealt each with children and adolescents or adults. In comparison, only ten reviews were conducted that placed the spotlight on older people. This finding highlights the need to conduct more research concentrating on the effects of PA interventions among older people.
-
(3)
Differences were observed in the amount of available research in particular settings. When reviewing each target group, it was clear to see that interventions in the school setting were researched the most. Interventions in settings such as the workplace, health care and family have been researched, though gaps in the knowledge base remain. Surprisingly, very little research has been conducted on PA interventions in the sport club setting.
-
(4)
When comparing the number of available reviews with the various intervention types, it becomes apparent that many reviews deal much more with individual-level interventions than with policy and environmental-level interventions.
The above-mentioned gaps posed a number of challenges when formulating the recommendations. First, due to the contrasting amount of available evidence, questions were raised regarding the quantity of evidence required to formulate a specific recommendation. While certain schemes have been proposed to classify the available evidence (e.g. Guyatt et al. 2008), such schemes do not consider that the amount of evidence might differ between intervention types. Considering the “inverse evidence law” (Brownson et al. 2009; Petticrew et al. 2004), there is currently much more evidence available for individual-level interventions. However, policy- and environmental-level interventions might be more promising in increasing PA levels that in turn influence public health impact.
Other challenges arose when attempting to weigh the available evidence on the different aspects of efficacy/effectiveness, cost-effectiveness, health equity impact and quality criteria:
-
(1)
The more quality criteria one considers in development, implementation and evaluation, the more costly an intervention will be. Though adhering to quality criteria will increase the likelihood of an intervention’s success, incurring costs may make implementation less likely.
-
(2)
Certain cost-effective interventions seem to result in smaller, rather short-term increases in PA (e.g. point-of-decision prompts). The potential public health impact of these intervention types therefore has to be questioned.
-
(3)
Certain brief and cost-effective interventions might not be able to reach vulnerable and at-risk population groups (e.g. mass-media campaigns) and may thus increase health inequalities when implemented. Interventions better suited to reach these groups are often more intensive and therefore more costly.
The development of recommendations for physical activity promotion highlights an important milestone for Germany. Committed engagement from a large group of scientists was instrumental in the formulation of the recommendations, as was the financial backing from the Federal Ministry of Health. To a certain degree, the process of formulating the recommendations may also reflect the political context of PA promotion in Germany. The Federal Ministry of Health took the political lead; other sectors were integrated into the process of dissemination, but did not play a large role in the formulation of the recommendations. The German Federal structure might cause challenges when taking the implementation of certain recommendations into account (e.g. changing state-level school curricula to allow for more physical education). Other nations that wish to develop recommendations for physical activity promotion will need to consider their own political context in this process.
Research limitations were related to the sheer number of reviews and the diversity of methodologies employed by such reviews. The extraction and summarisation of key findings proved to be a challenge due to the fact that certain reviews dealt with specific target groups, whereas others pertained to a specific setting or intervention type. Although more than 200 reviews were included for analysis, these reviews may only represent part of the existing research on this topic. Furthermore, the current layout of the recommendations comes across as rather broad. To further support implementation into public health practice, the recommendations may benefit from being developed into more specific action plans.
Conclusion
Our research stresses the great importance of integrating recommendations for PA promotion into national physical activity recommendations. Not only do the national recommendations describe the amount of PA people should engage in, they also provide information for organisations on how to support people in becoming more active. Though nations should adjust the process of recommendation development to their own political context, stakeholder engagement may prove valuable.
The research gaps identified in this review of reviews are significant and should thus be addressed in the future. Considering demographic changes and emerging chronic disease patterns, the inadequate depth of research on older people could signal cause for concern.
References
Abioye A, Hajifathalian K, Danaei G (2013) Do mass media campaigns improve physical activity? A systematic review and meta-analysis. Arch Public Health 71:1–10
Abu-Omar K, Rütten A, Burlacu I, Messing S, Pfeifer K, Ungerer-Röhrich U (2017a) Systematischer Review von Übersichtsarbeiten zu Übersichtsarbeiten zu Interventionen der Bewegungsförderung: Methodologie und erste Ergebnisse. Gesundheitswesen 79:S45–S50
Abu-Omar K, Rütten A, Burlacu I, Schätzlein V, Messing S, Suhrcke M (2017b) The cost-effectiveness of physical activity interventions: A systematic review of reviews. Prev Med Rep 8:72–78
Adams J, White M (2003) Are activity promotion interventions based on the transtheoretical model effective? A critical review. Br J Sports Med 37:106–114. https://doi.org/10.1136/bjsm.37.2.106
Aldcroft SA, Taylor NF, Blackstock FC, O'Halloran PD (2011) Psychoeducational rehabilitation for health behavior change in coronary artery disease: a systematic review of controlled trials. J Cardiopulm Rehabil Prev 31:273–281. https://doi.org/10.1097/HCR.0b013e318220a7c9
Anokye N, Jones T, Fox-Rushby J (2012) Intervention guidance physical activity—brief advice for adults in primary care: economic analysis. Review of economic evidence. https://www.nice.org.uk/guidance/ph44/evidence/review-of-economic-evidence-pdf-430313437. Accessed 01 Oct 2018
Arbesman M, Mosley LJ (2012) Systematic review of occupation- and activity-based health management and maintenance interventions for community-dwelling older adults. Am J Occup Ther 66:277–283. https://doi.org/10.5014/ajot.2012.003327
Ashenden R, Silagy C, Weller D (1997) A systematic review of the effectiveness of promoting lifestyle change in general practice. Fam Pract 14:160–175
Atkin A, Gorely T, Biddle S, Cavill N, Foster C (2011) Interventions to promote physical activity in young people conducted in the hours immediately after school: a systematic review. Int J Behav Med 18:176–187
Baker PR, Francis DP, Soares J, Weightman AL, Foster C (2011) Community wide interventions for increasing physical activity. Cochrane Database Syst Rev. https://doi.org/10.1590/S1516-31802011000600013
Baker PR, Francis DP, Soares J, Weightman AL, Foster C (2015) Community wide interventions for increasing physical activity. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD008366.pub3
Barr-Anderson DJ, Auyoung M, Whitt-Glover MC, Glenn BA, Yancey AK (2011) Integration of short bouts of physical activity into organizational routine: a systematic review of the literature. Am J Prev Med 40:76–93. https://doi.org/10.1016/j.amepre.2010.09.033
Beets MW, Beighle A, Erwin HE, Huberty JL (2009) After-school program impact on physical activity and fitness. A meta-analysis. Am J Prev Med 36:527–537. https://doi.org/10.1016/j.amepre.2009.01.033
Beinart NA, Goodchild CE, Weinman JA, Ayis S, Godfrey EL (2013) Individual and intervention-related factors associated with adherence to home exercise in chronic low back pain: a systematic review. Spine J 13:1940–1950. https://doi.org/10.1016/j.spinee.2013.08.027
Bossen D, Veenhof C, Dekker J, De Bakker D (2014) The effectiveness of self-guided web-based physical activity interventions among patients with a chronic disease: a systematic review. J Phys Act Health 11:665–677. https://doi.org/10.1123/jpah.2012-0152
Brand T, Pischke CR, Steenbock B, Schoenbach J, Poettgen S, Samkange-Zeeb F, Zeeb H (2014) What works in community-based interventions promoting physical activity and healthy eating? A review of reviews. Int J Environ Res Public Health 11:5866–5888. https://doi.org/10.3390/ijerph110605866
Bravata DM, Smith-Spangler C, Sundaram V, Gienger AL, Lin N, Lewis R, Stave CD, Olkin I, Sirard JR (2007) Using pedometers to increase physical activity and improve health: a systematic review. J Am Med Assoc 298:2296–2304. https://doi.org/10.1001/jama.298.19.2296
Brennan LK, Brownson RC, Orleans CT (2014) Childhood obesity policy research and practice. Evidence for policy and environmental strategies. Am J Prev Med 46:1–16
Broekhuizen K, Kroeze W, Van Poppel MNM, Oenema A, Brug J (2012) A systematic review of randomized controlled trials on the effectiveness of computer-tailored physical activity and dietary behavior promotion programs: an update. Ann Behav Med 44:259–286. https://doi.org/10.1007/s12160-012-9384-3
Broekhuizen K, Scholten AM, De Vries SI (2014) The value of (pre)school playgrounds for children's physical activity level: a systematic review. Int J Behav Nutr Phys Act 11. https://doi.org/10.1186/1479-5868-11-59
Brown DR, Soares J, Epping JM, Lankford TJ, Wallace JS, Hopkins D, Buchanan LR, Orleans CT, Community Preventive Services Task Force (2012) Stand-alone mass media campaigns to increase physical activity. A community guide updated review. Am J Prev Med 43:551–561
Brownson RC, Fielding JE, Maylahn CM (2009) Evidence-based public health: a fundamental concept for public health practice. Annu Rev Public Health 30:175–201
Bully P, Sánchez A, Zabaleta-del-Olmo E, Pombo H, Grandes G (2015) Evidence from interventions based on theoretical models for lifestyle modification (physical activity, diet, alcohol and tobacco use) in primary care settings: a systematic review. Prev Med. https://doi.org/10.1016/j.ypmed.2014.12.020
CADTH (2014) Lifestyle prescriptions: a review of the clinical evidence. https://www.cadth.ca/sites/default/files/pdf/htis/jun-2014/RC0552_Lifestyle%20Rx_Final.pdf. Accessed 01 Oct 2018
Campbell F, Blank L, Messina J, Day M, Woods HB, Payne N, Goyder E, Armitage C (2012) Physical activity: brief advice for adults in primary care (National Institute for Health and Clinical Excellence Public Health Intervention Guidance). https://www.nice.org.uk/guidance/ph44/evidence/review-of-effectiveness-andbarriers-and-facilitators-pdf-69102685. Accessed 01 Oct 2018
Cavill J-L, Jancey JM, Howat P (2012) Review and recommendations for online physical activity and nutrition programmes targeted at over 40s. Glob Health Promot 19:44–53
CDC (2011) Strategies to prevent obesity and other chronic diseases: the CDC guide to strategies to increase physical activity in the community. US Department of Health and Human Services, Atlanta
Chau JY, der Ploeg HP, van Uffelen JG, Wong J, Riphagen I, Healy GN, Gilson ND, Dunstan DW, Bauman AE, Owen N, Brown WJ (2010) Are workplace interventions to reduce sitting effective? A systematic review. Prev Med 51:352–356. https://doi.org/10.1016/j.ypmed.2010.08.012
Chillón P, Evenson KR, Vaughn A, Ward DS (2011) A systematic review of interventions for promoting active transportation to school. Int J Behav Nutr Phys Act 8:1–17
Chircop A, Basset R, Taylor E (2014) Evidence on how to practice intersectoral collaboration for health equity: a scoping review. Crit Public Health 25:178–191. https://doi.org/10.1080/09581596.2014.887831
Clark IN, Taylor NF, Baker FA (2012) Music interventions and physical activity in older adults: a systematic literature review and meta-analysis. J Rehabil Med 44:710–719
Cleland V, Granados A, Crawford D, Winzenberg T, Ball K (2013) Effectiveness of interventions to promote physical activity among socioeconomically disadvantaged women: a systematic review and meta-analysis. Obes Rev 14:197–212
Conn VS, Hafdahl AR, Cooper PS, Brown LM, Lusk SL (2009) Meta-analysis of workplace physical activity interventions. Am J Prev Med 37:330–339. https://doi.org/10.1016/j.amepre.2009.06.008
Council of the European Union (2013) Council recommendation on promoting health-enhancing physical activity across sectors. Brussels. https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:C:2013:354:0001:0005:EN:PDF. Accessed 01 Oct 2018
Cox NS, Alison JA, Holland AE (2013) Interventions for promoting physical activity in people with cystic fibrosis. Cochrane Database Syst Rev 12. https://doi.org/10.1002/14651858.CD009448.pub2
Cramp F, Berry J, Gardiner M, Smith F, Stephens D (2013) Health behaviour change interventions for the promotion of physical activity in rheumatoid arthritis: a systematic review. Musculoskeletal Care 11:238–247. https://doi.org/10.1002/msc.1049
Crutzen R (2010) Adding effect sizes to a systematic review on interventions for promoting physical activity among European teenagers. Int J Behav Nutr Phys Act 7:29. https://doi.org/10.1186/1479-5868-7-29
Cushing CC, Brannon EE, Suorsa KI, Wilson DK (2014) Systematic review and meta-analysis of health promotion interventions for children and adolescents using an ecological framework. J Pediatr Psychol 39:949–962. https://doi.org/10.1093/jpepsy/jsu042
Cyarto EV, Moorhead GE, Brown WJ (2004) Updating the evidence relating to physical activity intervention studies in older people. J Sci Med Sport 7:30–38
De Meester F, van Lenthe FJ, Spittaels H, Lien N, De Bourdeaudhuij I (2009) Interventions for promoting physical activity among European teenagers: a systematic review. Int J Behav Nutr Phys Act 6. https://doi.org/10.1186/1479-5868-6-82
de Nazelle A, Nieuwenhuijsen MJ, Antó JM, Brauer M, Briggs D, Braun-Fahrlander C, Cavill N, Cooper AR, Desqueyroux H, Fruin S, Hoek G, Panis LI, Janssen N, Jerrett M, Joffe M, Andersen ZJ, van Kempen E, Kingham S, Kubesch N, Leyden KM, Marshall JD, Matamala J, Mellios G, Mendez M, Nassif H, Ogilvie D, Peiró R, Pérez K, Rabl A, Ragettli M, Rodríguez D, Rojas D, Ruiz P, Sallis JF, Terwoert J, Toussaint JF, Tuomisto J, Zuurbier M, Lebret E (2011) Improving health through policies that promote active travel: a review of evidence to support integrated health impact assessment. Environ Int 37:766–777
Dishman RK, Oldenburg B, O'Neal H, Shephard RJ (1998) Worksite physical activity interventions. Am J Prev Med 15:344–361. https://doi.org/10.1016/S0749-3797(98)00077-4
Dobbins M, De Corby K, Robeson P, Husson H, Tirilis D (2009) School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6–18. Cochrane Database Syst Rev 1. https://doi.org/10.1002/14651858.CD007651
Dobbins M, Husson H, DeCorby K, LaRocca RL (2013) School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18 Cochrane Database Syst Rev 2. https://doi.org/10.1002/14651858.CD007651.pub2
DOSB (2018) Bestandserhebung 2017. Aktualisierte Fassung vom 25. Januar 2018. https://cdn.dosb.de/user_upload/www.dosb.de/uber_uns/Bestandserhebung/BEHeft_2017_aktualisierte_Version_25.01.18.pdf. Accessed 01 Oct 2018
Dudley D, Okely A, Pearson P, Cotton W (2011) A systematic review of the effectiveness of physical education and school sport interventions targeting physical activity, movement skills and enjoyment of physical activity. Eur Phys Educ Rev 17:353–378
Durand M-A, Carpenter L, Dolan H, Bravo P, Mann M, Bunn F, Elwyn G (2014) Do interventions designed to support shared decision-making reduce health inequalities? A systematic review and meta-analysis. PLoS One 9(4):1–13. https://doi.org/10.1371/journal.pone.0094670
Durlak JA, DuPre EP (2008) Implementation matters: a review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am J Community Psychol 41:327–350
Eakin EG, Lawler SP, Vandelanotte C, Owen N (2007) Telephone interventions for physical activity and dietary behavior change. A systematic review. Am J Prev Med 32:419–434. https://doi.org/10.1016/j.amepre.2007.01.004
Engbers LH, van Poppel MN, Chin APMJ, van Mechelen W (2005) Worksite health promotion programs with environmental changes: a systematic review. Am J Prev Med 29:61–70. https://doi.org/10.1016/j.amepre.2005.03.001
Escalante Y, García-Hermoso A, Backx K, Saavedra JM (2014) Playground designs to increase physical activity levels during school recess: a systematic review. Health Educ Behav 41:138–144
European Commission (2008) EU physical activity guidelines. Recommended Policy Actions in Support of Health-Enhancing Physical Activity. Brussels. http://ec.europa.eu/assets/eac/sport/library/policy_documents/eu-physical-activity-guidelines-2008_en.pdf. Accessed 01. Oct 2018
European Commission (2013) Special Eurobarometer 406. Attitudes of Europeans towards urban mobility. Brussels. http://ec.europa.eu/commfrontoffice/publicopinion/archives/ebs/ebs_406_en.pdf. Accessed 01. Oct 2018
European Commission (2014) Special Eurobarometer 412. Sport and physical activity. Report. Brussels. http://ec.europa.eu/commfrontoffice/publicopinion/archives/ebs/ebs_412_en.pdf. Accessed 01. Oct 2018
Finger JD, Mensink GBM, Lange C, Manz K (2017) Gesundheitsfördernde körperliche Aktivität in der Freizeit bei Erwachsenen in Deutschland. Journal of Health Monitoring 2:37–44
Flay BR (1986) Efficacy and effectiveness trials (and other phases of research) in the development of health promotion programs. Prev Med 15:451–474
Fraser S, Lock K (2010) Cycling for transport and public health: a systematic review of the effect of the environment on cycling. Eur J Pub Health 21:738–743
Freak-Poli RL, Cumpston M, Peeters A, Clemes SA (2013) Workplace pedometer interventions for increasing physical activity. Cochrane Database Syst Rev 4:1–78. https://doi.org/10.1002/14651858.CD009209.pub2
Fry JP, Neff RA (2009) Periodic prompts and reminders in health promotion and health behavior interventions: systematic review. J Med Internet Res 11. https://doi.org/10.2196/jmir.1138
Germany’s Conference of Health Ministers (2015) 88. Konferenz der Ministerinnen und Minister, Senatorinnen und Senatoren für Gesundheit der Länder am 24. und 25. Juni 2015 In Bad Dürkheim. Ergebnisniederschrift
Grant MJ, Booth A (2009) A typology of reviews: an analysis of 14 review types and associated methodologies. Health Inf Libr J 26:91–108
Guyatt GH, Oxman AD, Kunz R, Falck-Ytter Y, Gunn EV, Liberati A, Schünemann HJ, for the GRADE Working Group (2008) Rating quality of evidence and strength of recommendations: going from evidence to recommendations. BMJ 336:1049–1051
Hamel LM, Robbins LB, Wilbur J (2011) Computer- and web-based interventions to increase preadolescent and adolescent physical activity: a systematic review. J Adv Nurs 67:251–268. https://doi.org/10.1111/j.1365-2648.2010.05493.x
Heath GW, Parra DC, Sarmiento OL, Andersen LB, Owen N, Goenka S, Montes F, Brownson RC, Lancet Physical Activity Series Working Group (2012) Evidence-based intervention in physical activity: lessons from around the world. Lancet 380:272–281. https://doi.org/10.1016/S0140-6736(12)60816-2
Hillier-Brown FC, Bambra CL, Cairns JM, Kasim A, Moore HJ, Summerbell CD (2014) A systematic review of the effectiveness of individual, community and societal level interventions at reducing socioeconomic inequalities in obesity amongst children. BMC Public Health 14. https://doi.org/10.1186/1471-2458-14-834
Hinrichs T, Brach M (2012) The general practitioner's role in promoting physical activity to older adults: a review based on program theory. Curr Aging Sci 5:41–50. https://doi.org/10.2174/1874609811205010041
Hobbs N, Godfrey A, Lara J, Errington L, Meyer TD, Rochester L, White M, Mathers JC, Sniehotta FF (2013) Are behavioral interventions effective in increasing physical activity at 12 to 36 months in adults aged 55 to 70 years? A systematic review and meta-analysis. BMC Med 11. https://doi.org/10.1186/1741-7015-11-75
Hudon C, Fortin M, Soubhi H (2008) Single risk factor interventions to promote physical activity among patients with chronic diseases: systematic review. Can Fam Physician 54:1130–1137
Iversen MD, Brawerman M, Iversen CN (2012) Recommendations and the state of the evidence for physical activity interventions for adults with rheumatoid arthritis: 2007 to present. Int J Clin Rheumatol 7:489–503. https://doi.org/10.2217/ijr.12.53
Jackson NW, Howes FS, Gupta S, Doyle JL, Waters E (2005) Interventions implemented through sporting organisations for increasing participation in sport. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD004812.pub2
Jepson RG, Harris FM, Platt S, Tannahill C (2010) The effectiveness of interventions to change six health behaviours: a review of reviews. BMC Public Health 10. https://doi.org/10.1186/1471-2458-10-538
Kahlmeier S, Wijnhoven TMA, Alpiger P, Schweizer C, Breda J, Martin BW (2015) National physical activity recommendations: systematic overview and analysis of the situation in European countries. BMC Public Health 15(133):1–14. https://doi.org/10.1186/s12889-015-1412-3
Kahn EB, Ramsey LT, Brownson RC, Heath GW, Howze EH, Powell KE, Stone EJ, Rajab MW, Corso P (2002) The effectiveness of interventions to increase physical activity: a systematic review. Am J Prev Med 22:73–107. https://doi.org/10.1016/S0749-3797(02)00434-8
Kamath CC, Vickers KS, Ehrlich A, McGovern L, Johnson J, Singhal V, Paulo R, Hettinger A, Erwin PJ, Montori VM (2008) Behavioral interventions to prevent childhood obesity: a systematic review and metaanalyses of randomized trials. J Clin Endocrinol Metab 93:4606–4615
Kang M, Marshall SJ, Barreira TV, Lee J-O (2009) Effect of pedometer-based physical activity interventions: a meta-analysis. Res Q Exerc Sport 80:648–655
Kavookjian J, Elswick BM, Whetsel T (2007) Interventions for being active among individuals with diabetes: a systematic review of the literature. Diabetes Educ 33:962–988. https://doi.org/10.1177/0145721707308411
Kriemler S, Meyer U, Martin E, van Sluijs EM, Andersen LB, Martin BW (2011) Effect of school-based interventions on physical activity and fitness in children and adolescents: a review of reviews and systematic update. Br J Sports Med 45:923–930. https://doi.org/10.1136/bjsports-2011-090186
Lampert T, Mensink GBM, Romahn N, Woll A (2007) Körperlich-sportliche Aktivität von Kindern und Jugendlichen in Deutschland. Ergebnisse des kinder- und Jugendgesundheitssurveys (KiGGS) Bundesgesundheitsblatt, Gesundheitsforschung. Gesundheitsschutz 5(6):643–642
Langford R, Bonell CP, Jones HE, Pouliou T, Murphy SM, Waters E, Komro KA, Gibbs LF, Magnus D, Campbell R (2014) The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement (review). Cochrane Libr. https://doi.org/10.1002/14651858.CD008958.pub2
Larouche R, Saunders TJ, Faulkner G, Colley R, Tremblay M (2014) Associations between active school transport and physical activity, body composition, and cardiovascular fitness: a systematic review of 68 studies. J Phys Act Health 11:206–227. https://doi.org/10.1123/jpah.2011-0345
Leavy JE, Bull FC, Rosenberg M, Bauman A (2011) Physical activity mass media campaigns and their evaluation: a systematic review of the literature 2003–2010. Health Educ Res 26:1060–1085
Lee ACK, Maheswaran R (2010) The health benefits of urban green spaces: a review of the evidence. J Public Health 33:212–222
Leidy NK, Kimel M, Ajagbe L, Kim K, Hamilton A, Becker K (2014) Designing trials of behavioral interventions to increase physical activity in patients with COPD: insights from the chronic disease literature. Respir Med 108:472–481. https://doi.org/10.1016/j.rmed.2013.11.011
Leon L, Pesce C (2017) From delivery to adoption of physical activity guidelines: realist synthesis. Int J Environ Res Public Health 14(1193). https://doi.org/10.3390/ijerph14101193
Lin JS, O’Connor E, Whitlock EP, Beil TL, Zuber SP, Perdue LA, Plaut D, Lutz K (2010) Behavioral Counseling to Promote Physical Activity and a Healthful Diet to Prevent Cardiovascular Disease in Adults: Update of the Evidence for the US Preventive Services Task Force. https://www.ncbi.nlm.nih.gov/books/NBK51030/pdf/Bookshelf_NBK51030.pdf. Accessed 01 Oct 2018
Ling J, Robbins LB, Wen F, Peng W (2015) Interventions to increase physical activity in children aged 2-5 years: a systematic review. Pediatr Exerc Sci 27:314–333. https://doi.org/10.1123/pes.2014-0148
Lonsdale C, Rosenkranz RR, Peralta LR, Bennie A, Fahey P, Lubans DR (2013) A systematic review and meta-analysis of interventions designed to increase moderate-to-vigorous physical activity in school physical education lessons. Prev Med 56:152–161. https://doi.org/10.1016/j.ypmed.2012.12.004
Lorenc T, Petticrew M, Welch V, Tugwell P (2012) What types of interventions generate inequalities? Evidence from systematic reviews. J Epidemiol Community Health 67(2):190–193
Maher CA, Lewis LK, Ferrar K, Marshall S, De Bourdeaudhuij I, Vandelanotte C (2014) Are health behavior change interventions that use online social networks effective? A systematic review. J Med Internet Res 16(2):e40. https://doi.org/10.2196/jmir.2952
Malik SH, Blake H, Suggs LS (2014) A systematic review of workplace health promotion interventions for increasing physical activity. Br J Health Psychol 19:149–180. https://doi.org/10.1111/bjhp.12052
Mansi S, Milosavljevic S, Baxter GD, Tumilty S, Hendrick P (2014) A systematic review of studies using pedometers as an intervention for musculoskeletal diseases. BMC Musculoskelet Disord 15. https://doi.org/10.1186/1471-2474-15-231
Marques AI, Santos L, Soares P, Santos R, Oliveira-Tavares A, Mota J, Carvalho J (2011) A proposed adaptation of the European Foundation for Quality Management Excellence Model to physical activity programmes for the elderly—development of a quality self-assessment tool using a modified Delphi process. Int J Behav Nutr Phys Act 8:1–9
Marsh S, Foley LS, Wilks DC, Maddison R (2014) Family-based interventions for reducing sedentary time in youth: a systematic review of randomized controlled trials. Obes Rev 15:117–133. https://doi.org/10.1111/obr.12105
Marshall AL (2004) Challenges and opportunities for promoting physical activity in the workplace. J Sci Med Sport 7:60–66
Mastellos N, Gunn LH, Felix LM, Car J, Majeed A (2014) Transtheoretical model stages of change for dietary and physical exercise modification in weight loss management for overweight and obese adults. Cochrane Database Syst Rev 2. https://doi.org/10.1002/14651858.CD008066.pub3.
Matson-Koffman DM, Brownstein JN, Neiner JA, Greaney ML (2005) A site-specific literature review of policy and environmental interventions that promote physical activity and nutrition for cardiovascular health: what works? Am J Health Promot 19:167–193
McCormak GR, Shiell A (2011) In search of causality: a systematic review of the relationship between the built environment and physical activity among adults. Int J Behav Nutr Phys Act 8:1–11
McGrane N, Galvin R, Cusack T, Stokes E (2015) Addition of motivational interventions to exercise and traditional physiotherapy: a review and meta-analysis. Physiotherapy 101:1–12. https://doi.org/10.1016/j.physio.2014.04.009
Mehtälä MAK, Sääkslahti AK, Inkinen ME, Poskiparta MEH (2014) A socio-ecological approach to physical activity interventions in childcare: a systematic review. Int J Behav Nutr Phys Act 11:1–12
Messing S, Rütten A (2017) Qualitätskriterien für die Konzipierung, Implementierung und Evaluation von Interventionen zur Bewegungsförderung: Ergebnisse eines State-of-the-Art Reviews. Das Gesundheitswesen 79:S60–S65
Mitchell J, Skouteris H, McCabe M, Ricciardelli LN, Milgrom J, Baur LA, Fuller-Tyszkiewicz M, Dwyer G (2012) Physical activity in young children: a systematic review of parental influences. Early Child Dev Care 182:1411–1437
Mitchell MS, Goodman JM, Alter DA, John LK, Oh PI, Pakosh MT, Faulkner GE (2013) Financial incentives for exercise adherence in adults: systematic review and meta-analysis. Am J Prev Med 45:658–667. https://doi.org/10.1016/j.amepre.2013.06.017
Morgan O (2005) Approaches to increase physical activity: reviewing the evidence for exercise-referral schemes. Public Health 119:361–370. https://doi.org/10.1016/j.puhe.2004.06.008
Morris JH, Macgillivray S, McFarlane S (2014) Interventions to promote long-term participation in physical activity after stroke: a systematic review of the literature. Arch Phys Med Rehabil 95:956–967. https://doi.org/10.1016/j.apmr.2013.12.016
Morton K, Beauchamp M, Prothero A, Joyce L, Saunders L, Spencer-Bowdage S, Dancy B, Pedlar C (2014) The effectiveness of motivational interviewing for health behaviour change in primary care settings: a systematic review. Health Psychol Rev 9(2):205–223. https://doi.org/10.1080/17437199.2014.882006
Mozaffarian D, Afshin A, Benowitz NL, Bittner V, Daniels SR, Franch HA, Jacobs DR Jr, Kraus WE, Kris-Etherton PM, Krummel DA, Popkin BM, Whitsel LP, Zakai NA, American Heart Association Council on Epidemiology and Prevention, Council on Nutrition, Physical Activity and Metabolism, Council on Clinical Cardiology, Council on Cardiovascular Disease in the Young, Council on the Kidney in Cardiovasc (2012) Population approaches to improve diet, physical activity, and smoking habits: a scientific statement from the American Heart Association. Circulation 126:1514–1563. https://doi.org/10.1161/CIR.0b013e318260a20b
Munro J, Angus N, Leslie SJ (2013) Patient focused internet-based approaches to cardiovascular rehabilitation—a systematic review. J Telemed Telecare 19:347–353. https://doi.org/10.1177/1357633X13501763
Murphy NM, Bauman A (2007) Mass sporting and physical activity events—are they “bread and circuses” or public health interventions to increase population levels of physical activity? J Phys Act Health 4:193–202
National Collaborating Centre for Methods and Tools (2008) Quality assessment tool for quantitative studies. McMaster University, Hamilton
Naylor PJ, Nettlefold L, Race D, Hoy C, Ashe MC, Wharf Higgins J, McKay HA (2015) Implementation of school based physical activity interventions: a systematic review. Prev Med 72:95–115. https://doi.org/10.1016/j.ypmed.2014.12.034
Neidrick TJ, Fick DM, Loeb SJ (2012) Physical activity promotion in primary care targeting the older adult. J Am Acad Nurse Pract 24:405–416. https://doi.org/10.1111/j.1745-7599.2012.00703.x
Neville LM, O'Hara B, Milat A (2009) Computer-tailored physical activity behavior change interventions targeting adults: a systematic review. Int J Behav Nutr Phys Act 6. https://doi.org/10.1186/1479-5868-6-30
NICE (2008) Physical activity and the environment. https://www.nice.org.uk/guidance/ph8. Accessed 01. Oct 2018
Ogilvie D, Foster CE, Rothnie H, Cavill N, Hamilton V, Fitzsimons CF, Mutrie N (2007) Interventions to promote walking: systematic review. Br Med J 334:1204–1207. https://doi.org/10.1136/bmj.39198.722720.BE
O'Halloran PD, Blackstock F, Shields N, Holland A, Iles R, Kingsley M, Bernhardt J, Lannin N, Morris ME, Taylor NF (2014) Motivational interviewing to increase physical activity in people with chronic health conditions: a systematic review and meta-analysis. Clin Rehabil 28:1159–1171. https://doi.org/10.1177/0269215514536210
Orrow G, Kinmonth AL, Sanderson S, Sutton S (2012) Effectiveness of physical activity promotion based in primary care: systematic review and meta-analysis of randomised controlled trials. BMJ (Online) 344:16. https://doi.org/10.1136/bmj.e1389
Park A-L, McDaid D, Weiser P, Von Gottberg C, Becker T, Kilian R for the HELPS Network (2013) Examining the cost effectiveness of interventions to promote the physical health of people with mental health problems: a systematic review. BMC Public Health 13:787
Parrish A-M, Okely A, Stanley R, Ridgers N (2013) The effect of school recess interventions on physical activity. Sports Med 43:287–299
Passon AM, Gerber A, Schröer-Günther MA (2011) Evaluation in prevention and health promotion—workplace physical activity interventions. Zentralbl Arbeitsmed Arbeitssch Ergonomie 61:100-104
Pate RR, Trilk JL, Byun W, Wang J (2011) Policies to increase physical activity in children and youth. J Exerc Sci Fit 9:1–14
Pavey TG, Anokye N, Taylor AH, Trueman P, Moxham T, Fox KR, Hillsdon M, Green C, Campbell JL, Foster C, Mutrie N, Searle J, Taylor RS (2011) The clinical effectiveness and cost-effectiveness of exercise referral schemes: a systematic review and economic evaluation. Health Technol Assess 15. https://doi.org/10.3310/hta15440
Petticrew M, Whitehead M, Macintyre SJ, Graham H, Egan M (2004) Evidence for public health policy on inequalities: 1: the reality according to policymakers. J Epidemiol Community Health 58:811–816
Pinto D, Robertson MC, Hansen P, Abbott JH (2012) Cost-effectiveness of nonpharmacologic, nonsurgical interventions for hip and/or knee osteoarthritis: systematic review. Value Health 15:1–12. https://doi.org/10.1016/j.jval.2011.09.003
Priest N, Armstrong R, Doyle J, Waters E (2008) Interventions implemented through sporting organisations for increasing participation in sport. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD004812.pub3
Pronk NP (2009) Physical activity promotion in business and industry: evidence, context, and recommendations for a national plan. J Phys Act Health 6:220–235
Proper KI, Koning M, Van der Beek AJ, Hildebrandt VH, Bosscher RJ, Van Mechelen W (2003) The effectiveness of worksite physical activity programs on physical activity, physical fitness, and health. Clin J Sport Med 13:106–117. https://doi.org/10.1097/00042752-200303000-00008
Public Health England (2015) What works in schools and colleges to increase physical activity? A briefing for head teachers, college principals, staff working in education settings, directors of public health and wider partners. London
Pucher J, Dill J, Handy S (2010) Infrastructure, programs, and policies to increase bicycling: an international review. Prev Med 50:106–125
Quitério ALD (2013) School physical education: the effectiveness of health-related interventions and recommendations for health-promotion practice. Health Educ J 72:716–732. https://doi.org/10.1177/0017896912460934
Reynolds R, McKenzie S, Allender S, Brown K, Foulkes C (2014) Systematic review of incidental physical activity community interventions. Prev Med 67:46–64. https://doi.org/10.1016/j.ypmed.2014.06.023
Roine E, Roine RP, Rasanen P, Vuori I, Sintonen H, Saarto T (2009) Cost-effectiveness of interventions based on physical exercise in the treatment of various diseases: a systematic literature review. Int J Technol Assess Health Care 25:427–454. https://doi.org/10.1017/s0266462309990353
Rütten A, Schow D, Breda J, Galea G, Kahlmeier S, Oppert JM, van der Ploeg H, van Mechelen W (2016) Three types of scientific evidence to inform physical activity policy: Results from a comparative scoping review. Int J Public Health 61:553–563
Salmon J, Booth ML, Phongsavan P, Murphy N, Timperio A (2007) Promoting physical activity participation among children and adolescents. Epidemiol Rev 29:144–159. https://doi.org/10.1093/epirev/mxm010
Sargent GM, Forrest LE, Parker RM (2012) Nurse delivered lifestyle interventions in primary health care to treat chronic disease risk factors associated with obesity: a systematic review. Obes Rev 13:1148–1171. https://doi.org/10.1111/j.1467-789X.2012.01029.x
Schroer S, Haupt J, Pieper C (2014) Evidence-based lifestyle interventions in the workplace—an overview. Occup Med 64:8–12. https://doi.org/10.1093/occmed/kqt136
Senore C, Giordano L, Bellisario C, Di Stefano F, Segnan N (2012) Population based cancer screening programmes as a teachable moment for primary prevention interventions. A review of the literature. Front Oncol 2. https://doi.org/10.3389/fonc.2012.00045
Shankardass K, Renahy E, Muntaner C, O'Campo P (2015) Strengthening the implementation of Health in All Policies: a methodology for realist explanatory case studies. Health Policy Plan 30:462–473
Shemilt I, Hollands GJ, Marteau TM, Nakamura R, Jebb SA, Kelly MP, Suhrcke M, Oglivie D (2013) Economic instruments for population diet and physical activity behaviour change: a systematic scoping review. PLoS One 8. https://doi.org/10.1371/journal.pone.0075070
Short CE, James EL, Stacey F, Plotnikoff RC (2013) A qualitative synthesis of trials promoting physical activity behaviour change among post-treatment breast cancer survivors. J Cancer Surviv 7:570–581. https://doi.org/10.1007/s11764-013-0296-4
Shrestha N, Ijaz S, Kukkonen-Harjula KT, Kumar S, Nwankwo CP (2015) Workplace interventions for reducing sitting at work. Cochrane Database Syst Rev 1. https://doi.org/10.1002/14651858.CD010912.pub2
Smith BJ (2004) Promotion of physical activity in primary health care: update of the evidence on interventions. J Sci Med Sport 7:67–73
Smith V, Devane D, Begley CM, Clarke M (2011) Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med Res Methodol 11(15). https://doi.org/10.1186/1471-2288-11-15
Sorensen JB, Skovgaard T, Puggaard L (2006) Exercise on prescription in general practice: a systematic review. Scand J Prim Health Care 24:69–74. https://doi.org/10.1080/02813430600700027
Steenbock B, Pischke CR, Schonbach J, Pottgen S, Brand T (2014) Wie wirksam sind ernährungs- und bewegungsbezogene primärpräventive Interventionen im Setting Kita? Ein Review von Reviews. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz 1–11. https://doi.org/10.1007/s00103-014-2100-7
Stensel D (2009) Primary prevention of CVD: physical activity. BMJ Clin Evidence
Stevens Z, Barlow C, Kendrick D, Masud T, Skelton DA, Dinan-Young S, Iliffe S (2014) Effectiveness of general practice-based physical activity promotion for older adults: systematic review. Prim Health Care Res Dev 15:190–201. https://doi.org/10.1017/s1463423613000017
Taylor RS, Sagar VA, Davies EJ, Briscoe S, Coats AJ, Dalal H, Lough F, Rees K, Singh S (2014) Exercise-based rehabilitation for heart failure. Cochrane Database Syst Rev 4. https://doi.org/10.1002/14651858.CD003331.pub4
ter Hoeve N, Huisstede BMA, Stan HJ, van Domburg RT, Sunamura M, van den Berg-Emons RJG (2015) Does cardiac rehabilitation after an acute cardiac syndrome lead to changes in physical activity habits? Systematic review Phys Ther 95:167-179
The AGREE Collaboration (2003) Development and validation of an international appraisal instrument for assessing the quality of clinical practice guidelines: the AGREE project. Qual Saf Health Care 12:18–23
Tremblay MS, Kho ME, Tricco AC, Duggan M (2010) Process description and evaluation of Canadian Physical Activity Guidelines development. Int J Behav Nutr Phys Act 7:42. https://doi.org/10.1186/1479-5868-7-42
Trost SG, Ward DS, Senso M (2010) Effects of child care policy and environment on physical activity. Med Sci Sports Exerc 42:520–525
van den Berg MH, Schoones JW, Vliet Vlieland TP (2007) Internet-based physical activity interventions: a systematic review of the literature J Med Internet Res 9. https://doi.org/10.2196/jmir.9.3.e26
van Grieken A, Ezendam NPM, Paulis WD, van der Wouden JC, Raat H (2012) Primary prevention of overweight in children and adolescents: a meta-analysis of the effectiveness of interventions aiming to decrease sedentary behaviour. Int J Behav Nutr Phys Act 9. https://doi.org/10.1186/1479-5868-9-61
Van Lippevelde W, Verloigne M, De Bourdeaudhuij I, Brug J, Bjelland M, Lien N, Maes L (2012) Does parental involvement make a difference in school-based nutrition and physical activity interventions? A systematic review of randomized controlled trials. Int J Public Health 57:673–678. https://doi.org/10.1007/s00038-012-0335-3
van Sluijs EMF, McMinn AM, Griffin SJ (2008) Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. BMJ (Online) 1-13. https://doi.org/10.1136/bmj.39320.843947.BE
Vandelanotte C, Spathonis KM, Eakin EG, Owen N (2007) Website-delivered physical activity interventions. A review of the literature. Am J Prev Med 33:54–64. https://doi.org/10.1016/j.amepre.2007.02.041
Ward DS, Vaughn A, McWilliams C, Hales D (2010) Interventions for increasing physical activity at child care. Med Sci Sports Exerc 42:526–534
Waters E, de Silva-Sanigorski A, Hall BJ, Brown T, Campbell KJ, Gao Y, Armstrong R, Prosser L, Summerbell CD (2014) Interventions for preventing obesity in children. Sao Paulo Med J 132. https://doi.org/10.1590/1516-3180.20141322T2
Webel AR, Okonsky J, Trompeta J, Holzemer WL (2010) A systematic review of the effectiveness of peer-based interventions on health-related behaviors in adults. Am J Public Health 100:247–253. https://doi.org/10.2105/AJPH.2008.149419
WHO (2004) Global strategy on diet. Physical Activity and Health, Geneva
WHO (2009) Interventions on diet and physical activity: what works: summary report, Geneva
WHO Europe (2013) Physical activity promotion in socially disadvantaged groups: principles for action. Copenhagen. http://www.euro.who.int/en/publications/abstracts/physical-activity-promotion-in-sociallydisadvantaged-groups-principles-for-action.-policy-summary-2013. Accessed 01 Oct 2018
Wong JYL, Gilson ND, van Uffelen JGZ, Brown WJ (2012) The effects of workplace physical activity interventions in men: a systematic review. Am J Mens Health 6:303–313. https://doi.org/10.1177/1557988312436575
Xu H, Wen LM, Rissel C (2015) Associations of parental influences with physical activity and screen time among young children: a systematic review. J Obes 1–23. https://doi.org/10.1155/2015/546925
Yang L, Sahlqvist S, McMinn AM, Griffin SJ, Ogilvie D (2011) Interventions to promote cycling: systematic review. BMJ (Online) 1–10. https://doi.org/10.1136/bmj.c5293
Zaza S, Briss PA, Harris KW (2005) Preventive Services. What works to promote health? Task Force on Community Preventive Services. Oxford University Press, Oxford
Funding
This research was conducted as part of a project funded by the German Federal Ministry of Health (ZMVI 5 2514FSB-200). The ministry was involved in neither writing this manuscript nor in the decision to submit the article for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure of potential conflicts of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Abu-Omar, K., Rütten, A., Messing, S. et al. The German recommendations for physical activity promotion. J Public Health (Berl.) 27, 613–627 (2019). https://doi.org/10.1007/s10389-018-0986-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-018-0986-5