
Abstract
Background
After school is a critical period in the physical activity and sedentary behaviour patterns of young people. Interventions to promote physical activity during these hours should be informed by existing evidence.
Purpose
The present study provides a systematic review of interventions to promote physical activity in young people conducted in the hours immediately after school.
Methods
The review was conducted in accordance with guidelines from the National Institute for Health and Clinical Excellence. Studies were located through searches of electronic databases, including MEDLINE, EMBASE, PsychINFO and ERIC. For included studies, data were extracted and methodological quality assessed using standardised forms.
Results
Ten papers, reporting nine studies, met inclusion criteria. Three studies reported positive changes in physical activity and six indicated no change. Evidence suggests that single-behaviour interventions may be most effective during these hours.
Conclusion
Limitations in study design, lack of statistical power and problems with implementation have likely hindered the effectiveness of interventions in the after-school setting to date. Further work is required to develop interventions during this critical period of the day.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Regular physical activity is associated with decreased risk of cardiovascular disease [1, 2] and improvements in psychological well-being amongst children and adolescents [3]. However, in the UK and other developed countries, a sizeable proportion of young people are largely inactive and lead sedentary lifestyles [4]. Evidence suggests that the global incidence of childhood obesity is rising [5], increasing interest in the understanding of physical activity and sedentary behaviours of young people. These behaviours may be implicated in the aetiology of obesity [6]. The development and evaluation of interventions to promote physical activity in young people is, therefore, a public health priority.
Based on the behavioural setting concept [7], interventions to increase physical activity in young people have been located within the community, family or primary care, with varying degrees of success [8]. The majority of physical activity interventions with young people, however, have been school-based, targeting the curriculum, physical education, the school environment, school policy or combinations of these [9]. Whilst school-level programmes may be effective at increasing activity during physical education, they appear less successful in improving activity outside of school hours [9]. Numerous studies indicate that the majority of young peoples’ physical activity occurs outside of school, reinforcing the need for interventions in other settings [10, 11]. Objective measures of physical activity, such as accelerometry, allow researchers to study patterns of physical activity across the day.
Studying the hours immediately after school may be particularly insightful because during this time young people have discretion as to how they use their time, freed from the constraints of school and parental curfews that may restrict behaviour in the evening. After school, often referred to as ‘critical hours’, is a time when young people engage in a considerable proportion of their daily leisure time activity [12] and is predictive of overall activity patterns [13]. Previous research indicates that the after-school hours should be targeted for physical activity promotion in young people [14]. Interventions based in the after-school setting, whilst seeking to increase total physical activity, may provide valuable information as to what can be achieved during these hours. A previous review of after-school interventions reported mixed findings [15]. However, this study was limited by failure to describe the search strategy employed (i.e. search terms used, inclusion/exclusion criteria). In addition, it included studies that did not report physical activity outcome data or assessed fitness rather than physical activity behaviour or recorded activity only during intervention sessions. Four papers from this previous study were included in the current review [16–19].
The purpose of the present study was to systematically review the effectiveness of interventions to promote physical activity in young people conducted in the hours immediately after school.
Method
The review was conducted in accordance with guidelines developed by the National Institute for Health and Clinical Excellence (NICE; [20]) The search strategy was devised by the Public Health Collaborating Centre for Physical Activity and NICE. Search terms included ‘physical activity‘, ‘exercise‘, ‘play’, ‘child’, ‘adolescent’, ‘youth’, ‘community’ and ‘gym’. Terms were employed in the following order: (1) physical activity terms, (2) child terms, (3) location terms. Electronic searching was conducted independently by the Support Unit for Research Evidence at Cardiff University, using the following databases: Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effectiveness, Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, PsychINFO, CINAHL, HMIC, SPORTDiscus, ASSIA, SIGLE, Current Contents, ERIC, TRANSPORT, Environline, EPPI Centre Databases and NRR. Searches were performed for the period January 1990 to March 2010. Reference lists of all included papers and relevant reviews were scrutinised for articles not identified through electronic searches [9, 10, 21–26].
Inclusion criteria required that studies (1) conducted an intervention to promote physical activity based in the after-school setting, (2) targeted participants less than 18 years of age, (3) reported an outcome measure of physical activity (objective or self-report). Studies aimed at preventing overweight/obesity were included, but obesity treatment studies were excluded. Studies assessing both physical activity and physical fitness were included; however, those with only physical fitness assessment were excluded. Unpublished articles, conference papers and dissertations were also excluded.
For included studies, data were extracted using standardised forms developed by the Public Health Collaborating Centre for Physical Activity and NICE. Studies were assessed for quality independently by two reviewers using design-specific quality assessment tools produced by NICE [20]. The tool for the assessment of randomised trials comprises 10 items relating to internal validity, e.g. study design, sample size and outcome measurement. For each item, a rating of ‘well covered’, ‘adequately addressed’, ‘poorly addressed’, ‘not reported’ or ‘not applicable’ was provided based upon reviewers assessment of the article in question. Studies were categorised ‘++’ (excellent quality), ‘+’ or ‘−’ (poor quality) based on the extent to which potential sources of bias had been minimised. Any discrepancies between reviewers were resolved through discussion.
Results
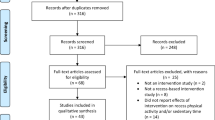
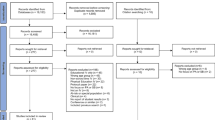
Searching produced 15,581 potentially relevant ‘hits’. One member of the research team conducted initial screening based on title and removal of duplicates, with 355 papers deemed potentially relevant. Secondary screening based on title and abstract identified 209 papers for full retrieval and assessment against inclusion/exclusion criteria. This included 67 studies identified through sources other than electronic searching. The primary reasons for exclusion included interventions not being located in the after-school setting, lack of or inappropriate outcome assessment and studies aimed at the treatment of obesity. To ensure consistency, a third member of the team checked 10% of included and excluded papers, with no discrepancies found. Ten papers, reporting nine studies, were accepted for full data extraction [16–19, 27–32]. Taylor et al. [29, 30] report data from the same sample. The sample is the unit of analysis. The Quality of Reporting of Meta-analyses statement [33] provided the structure for the flow diagram indicating the process of study identification shown in Fig. 1. We were not able to perform a quantitative synthesis due to heterogeneity of studies [34].

Flow diagram of study selection process
Included Studies: Summary
All studies were conducted in the USA, except Cliff et al. [27] and Taylor et al. [29, 30] which took place in Australia and New Zealand, respectively. All studies targeted the after-school period and five included a family component [16–18, 27, 29, 30]. Four studies were designed to prevent weight gain [16, 17, 19, 29, 30], four targeted physical activity and/or its psychosocial determinants [18, 27, 28, 31] and one targeted physical activity and fruit and vegetable intake [32]. Five studies were aimed at the African-American population [16, 17, 28, 31, 32] and one targeted young people from rural communities [17]. For methodological quality, two studies were scored ‘++’ [29–31], four scored ‘+’ [16–19] and three received a ‘−’ rating [27, 28, 32]. Three studies reported positive changes in physical activity [19, 28, 31] and six resulted in no change [16–18, 27, 29, 30, 32]. An overview of included studies is presented below. A detailed description of included studies is provided in Table 1.
Wilson et al. [32] recruited 53 predominantly African-American middle-school pupils aged 11–15 years. The intervention was 12 weeks in duration, conducted 3 days a week as part of an after-school intramural sports programme. Participants were randomised within schools to one of three arms: Social Cognitive Theory (SCT), SCT plus motivational intervention (MI) or an education-only control condition. Physical activity was assessed by accelerometry at baseline and post-intervention. The SCT intervention focussed on education, behavioural skills training, feedback and reinforcement. For the SCT + MI condition, participants received the same SCT-based intervention plus 30 min of strategic self-presentation videotapes. Participants took part in a videotaped interview in which they demonstrated for ‘beginners’ their positive coping strategies for increasing physical activity and fruit and vegetable intake. The interventions did not result in increased physical activity. There were no significant group by time differences, though interpretation of findings is limited because no statistics were reported. The SCT + MI group showed a decrease in moderate physical activity (MPA; −9.4%) and vigorous physical activity (VPA; −29%), whilst the SCT condition increased both MPA (6.1%) and VPA (50%). In the control condition, MPA and VPA decreased over time. The study may have been underpowered, with only 69% of participants remaining in the control group at follow-up and attrition rates of 17% and 30% in the intervention groups.
Story et al. [17] and Robinson et al. [16] report pilot studies from the Girls Health Enrichment Multi-site Studies (GEMS). The multi-site project funded four centres to test interventions designed to prevent weight gain in African-American girls. Story et al. [17] used SCT to develop a 12-week after-school programme entitled “Girlfriends for KEEPS”—‘Keys to Eating, Exercising, Playing and Sharing’. The study recruited 54 predominantly African-American girls in the top 25th percentile for age- and sex-specific body mass index (BMI). The intervention was offered twice a week for 1 h after school. Physical activity was assessed by accelerometer and self-report at baseline and post-intervention. The intervention targeted environmental, personal and behavioural factors, including peer support, self-efficacy and goal setting. Programme meetings consisted of culturally appropriate, interactive and practical activities emphasising skill building and practice of the health behaviour message for that week. Messages included information about the benefits of physical activity, watching less television and enhancing self-esteem. The family component included weekly family packets to take home, family night events and phone calls to parents. Physical activity was consistently greater in the intervention group relative to the controls at post-intervention, though differences were not significant. At post-intervention, mean accelerometer counts per minute and minutes of MVPA per day were 503.7 vs. 446.2 (d = 0.62, p = 0.12) and 119.0 vs. 116.1 (d = 0.08, p = 0.83) for intervention and control groups, respectively. The authors state that the study was underpowered to detect statistically significant differences between groups.
Robinson et al. [16] recruited 61 African-American girls aged 8–10 years with a BMI above the 50th percentile and/or at least one overweight parent or guardian. The 12-week intervention, based on SCT, focussed on increasing physical activity and reducing television viewing. Physical activity was assessed by accelerometer and self-report at baseline and post-intervention. The primary intervention strategy was dance sessions offered 5 days/week from 1530 to 1800 hours at local community centres. Forty-six percent of intervention participants attended at least 2 days/week on average. Sessions comprised a healthy snack, followed by 60 min of homework time and 45–60 min of dance. Sessions ended with a 30-min talk exploring the meaning of dance in the African-American culture and community. The TV viewing strand was delivered through five home visits. Strategies included self-monitoring and provision of an electronic TV time manager. Accelerometer data indicated a non-significant (d = 0.14, p = 0.67) increase (7%) in MVPA for the intervention group at follow-up. The adjusted difference between intervention and control groups of 55.1 counts per minute from noon to 6 pm was not significant (d = 0.21, p = 0.53). Self-reported TV viewing decreased by 23% for girls in the intervention group (d = 0.4, p = 0.14) and intervention families indicated a significant reduction in total household TV viewing (d = 0.73, p = 0.007). Consistent with other studies in the GEMS project, the study was underpowered to detect differences in the primary outcome variable of BMI and other main outcome variables.
Pate et al. [18] conducted a community-based intervention to increase physical activity and modify psychosocial determinants of activity in rural, predominantly African-American children. Children (n = 436) aged 10–11 years took part in the study. The theoretical framework for the intervention was Pender’s Health Promotion Model and SCT. Physical activity was assessed using the validated Previous-Day Physical Activity Recall at baseline, mid-intervention and post-intervention. The predominant intervention component was an after-school and summer camp programme known as ‘Active Kids’ (2 h after school for 5 days/week for 15 weeks). The ‘Active Kids’ intervention comprised three strands (‘Fit for Fun’, ‘Be a Sport’ and ‘Social Rap’) which aimed to increase knowledge and skills relating to physical activity, sport and understanding social influences on behaviour. Three additional components (‘Active Home’, ‘Active School’ and ‘Active Community’) were devised to foster involvement of parents, schools and the local community in facilitating opportunities for children to be active. There were no significant differences in MVPA or VPA between the intervention and control groups for either boys or girls at mid-intervention or post-intervention. In addition, there were no changes in hypothesised psychosocial determinants of physical activity. Process evaluation indicated there were a number of implementation challenges; specifically, the home, school and community strands were not delivered as intended.
Wilson et al. [31] conducted a 4-week student-centred intervention to increase physical activity in underserved youth. Participants were 48 adolescents aged 10–12 years. The study used Self-Determination Theory and SCT to inform intervention design. The intervention took place on 3 days/week, for 2 h after school. Physical activity was measured over five consecutive days using accelerometry. Intervention sessions comprised a 30-min snack/homework component, 60 min of MVPA and a 30-min SCT and motivational component, including self-monitoring and goal setting. Participants took part in a videotaped ‘strategic self-presentation’ exercise, wherein they described positive coping strategies for increasing physical activity. Results showed a significant increase in MPA (adjusted means 99.36 vs. 72.63 min/day, p < 0.02), MVPA (adjusted means 113.94 vs. 78.78 min/day, p < 0.02) and VPA (adjusted means 11.33 vs. 5.31 min/day, p < 0.02) for intervention versus control participants at follow-up.
Taylor et al. [29, 30] conducted a 2-year intervention with 472 children aged 5–12 years. The primary aim of the study was to prevent excess weight gain by increasing opportunities for healthy eating and non-curricular physical activity. Physical activity was assessed by accelerometer and self-report at baseline and at 1- and 2-year follow-up. The primary intervention in both years was the provision of a Community Activity Co-ordinator, employed part time at each intervention school. Their role was to encourage all children to be more physically active by increasing opportunities for activity during breaks, lunch time and after school. During the second year of the intervention, additional elements were introduced to reduce intake of sugary drinks, increase fruit and vegetable consumption and reduce television viewing. At year 1, after adjustment for baseline activity, age and sex, accelerometer counts per minute were 28% (95% CI 11–47%) higher in the intervention group. This was true for physical activity during school hours and at home. However, results at year 2 showed no effect for physical activity behaviour change. Self-report data showed that intervention children were less active than control children at both year 1 and year 2.
Annesi et al. [28] recruited 241 African-American children, aged 9–12 years, for a 12-week intervention. The study compared the effects of the ‘Youth Fit for Life’ intervention protocol, as delivered in the after-school setting or during physical education classes. Intervention content was informed by SCT. A single-item self-report measure assessed the number of days participants had taken part in MVPA in the previous week. The after-school intervention was delivered by school counsellors. Sessions were approximately 45 min in duration, comprising 20 min of non-competitive activities, followed by 20 min of strength training exercises 2 days/week. On the third day, participants reviewed various self-management and self-regulatory skills, consistent with SCT. For the PE condition, the intervention was delivered on 2 days/week by PE specialist teachers in the school gymnasium. The key differences between conditions were leadership (counsellors vs. PE teachers), location (multi-purpose room vs. gymnasium) and timing (after school, 3 days/week vs. during PE, 2 days/week). Results showed a significant increase in the number of days of MVPA for both intervention groups (after-school group 2.20 to 2.91 days/week, p < 0.001; PE group 2.38 to 3.13 days/week, p < 0.001).
Cliff et al. [27] report a small pilot intervention to increase physical activity by improving motor development and perceived competence in overweight and obese children aged 8–12 years. Thirteen participants were recruited and assessed for physical activity by accelerometry at baseline, post-treatment (10 weeks) and follow-up (36 weeks). There was no control group. The intervention comprised weekly 2-h group meetings delivered in a community centre. Sessions were delivered in a manner that provided a learning environment based on mastery goal orientation. Each session focussed upon two or three key skills, structured to include introductory, skill development and skill application activities. Participants were also set ‘Home Challenges’, modified from session activities, in order to encourage practice of key skills and family involvement. Analysis indicated a significant decrease in accelerometer-assessed MVPA from baseline to post-treatment and follow-up (mean (SD) MVPA min: baseline 144.5 (37.5); post-treatment 108.7 (43.5), d = 0.88, p = 0.001; follow-up 85.8 (32.0), d = 1.69, p = 0.001). The authors report that during post-treatment and follow-up, compliance to accelerometer wearing declined, indicating that some activity may not have been recorded.
Weintraub et al. [19] report findings from the Stanford Sports to Prevent Obesity Randomised Trial, a pilot intervention targeting overweight and obese children in school grades 4 and 5. Twenty-one children with a BMI at or above the 85th percentile took part. Physical activity was assessed by accelerometry at baseline and 3 and 6 months. The intervention comprised an after-school football programme offered 3 days/week for 6 months. Towards the end of the programme, sessions were held more frequently (5 days/week) at participants’ request. No theoretical framework was indicated. Sessions were approximately 2.25 h in duration, including a homework period and 75 min of activity. Sessions focussed upon skill building, respect for self and others, inclusion and teamwork. Participants in the control group received a general nutrition and health education programme, also delivered after school. Adjusted intervention versus control group differences in counts per minute (d = 1.22, p = 0.04), MPA (d = 1.22, p = 0.03) and VPA (d = 1.13, p = 0.02) were significant at 3 months, but not at 6 months (counts per minute d = 0.61, p = 0.29, MPA d = 0.48, p = 0.36, VPA d = 0.43, p = 0.35).
Differences Between Effective and Non-effective Interventions
Few clear differences between effective and non-effective studies emerged. Effective studies used randomised and non-randomised controlled trial designs, similar to non-effective studies. There was some indication that targeting physical activity alone was more likely to result in positive findings. Effective studies generally focussed solely upon increasing physical activity, whereas a high proportion of non-effective studies targeted weight gain prevention or diet and activity together. Effective interventions were located in schools, providing some support for this setting in after-school studies. However, a large proportion of non-effective studies were also school-based, often targeted in combination with community or home intervention strands. With regard to intervention duration, a large proportion of non-effective but also two of the effective studies were short term, lasting less than 12 weeks from baseline to post-testing. Only three interventions were conducted over a period in excess of 12 weeks, one of which indicated a smaller decrease in activity amongst intervention versus control participants [19]. There were no clear differences between effective and non-effective studies regarding intervention quality, sampling characteristics, theory utilised, follow-up duration or method of physical activity assessment used.
Discussion
We reviewed the effectiveness of interventions to promote physical activity in young people located in the after-school setting. In addition, we sought to identify key features that could be used to inform interventions designed to increase physical activity during these hours.
Of the nine studies meeting inclusion criteria, three reported an increase or smaller decrease in physical activity amongst intervention participants compared with controls [19, 28, 31]. It is appropriate to note that one of these studies received a ‘−’ rating for quality, primarily due to the use of a weak outcome measure for physical activity [28]. A further two studies, both from the GEMS project, reported trends towards increased activity but were underpowered to detect differences in the primary outcome of BMI and were likely underpowered for physical activity too [16, 17]. Calculation of effect sizes for physical activity variables indicated that effects were generally small. In eight of the nine reviewed studies, physical activity outcomes were assessed at baseline and post-intervention only; thus, where behaviour change was reported, it is not possible to determine whether it was maintained long term. Six of the nine included studies were targeted at the African-American population, often with an emphasis upon low socio-economic groups. Recruitment strategies and intervention materials were tailored specifically to the needs of this population, thus generalising the methods, and findings of reviewed studies to other population groups may be inappropriate. Overall, findings indicate that interventions to promote physical activity delivered in the after-school setting have been ineffective to date. Whilst most reviewed studies failed to increase physical activity, weaknesses in methodology or implementation may have limited their impact, suggesting that further research in this area is needed.
Potential moderators of intervention effectiveness include sample characteristics, study quality or theoretical framework employed. Comparison of effective and non-effective interventions may provide insight into what does and does not work in the after-school setting. However, few clear moderators of effectiveness emerged. This is likely a consequence of the low number of studies reviewed and that only three were successful in increasing activity. Nonetheless, there is some evidence that targeting physical activity alone, rather than in combination with diet or as part of a weight gain prevention programme, may be a more effective strategy. It is possible that single-behaviour interventions, with fewer messages focussed on a single issue, are more suited to the cognitive capacity of children and adolescents.
Setting and duration may also be important in the design of effective interventions after school. Effective studies were located primarily in the school setting, whilst non-effective interventions more likely took place in combinations of school, home or the community. Access may be a key issue here, such that school-based programmes are more readily accessible to participants and do not require additional transport or rely on the presence and co-operation of parents or other family members. Overall, interventions that cut across school, home and community boundaries provide greater opportunities to influence social and environmental determinants of physical activity and reinforce key intervention messages but provide additional challenges of implementation. Intervention design must ensure that participants (and their families where necessary) are provided with the means to attend intervention programmes at home or in the community.
With regard to intervention duration, the majority of reviewed studies were relatively short term: two effective studies and four non-effective studies being less than 12 weeks from baseline to post-intervention assessment. Two studies that were implemented over longer duration failed to increase physical activity [18, 29, 30]. This most likely reflects challenges of implementation and fidelity in long-term intervention delivery. Pate et al. [18] report that the home, school and community strands of the Active Winners intervention were not implemented as planned due to time and resource limitations. Whilst long-term interventions present considerable challenges in delivery, sustained contact over a prolonged period may increase the likelihood of maintaining behaviour change. Of the three studies that reported a positive effect on physical activity, long-term follow-up was not conducted; thus, it is not possible to determine whether changes were maintained beyond intervention termination. Future interventions in this area should ensure follow-up assessment is conducted.
A comment regarding intervention reporting and process evaluation is warranted. Only Pate et al. [18] conducted a rigorous process evaluation to determine the extent to which the programme was implemented as intended. This enabled the authors to provide possible explanations for why the intervention was not successful. In this case, it was problems regarding intervention implementation, rather than failures in design, theory or content, that could account for the lack of impact. Too few studies included process measures, which may have enabled a more complete discussion of why specific interventions did or did not result in increased activity. Allied to this, the use of mediation analysis to identify which intervention components are effective and how they operate will allow for further refinement of intervention methods [35].
A limitation of this review is that only articles published in peer review journals in the English language were included. A key strength was the development of a comprehensive search strategy, implemented by a specialist information science unit. The review was limited to articles published from 1990 onwards, to allow for studies that were most reflective of current knowledge and practice.
Conclusion
We reviewed interventions to increase physical activity in children and adolescents located in the after-school setting. Of the nine studies meeting inclusion criteria, three reported positive effects on physical activity. Limitations in study design, lack of statistical power and problems with implementation most likely account for the lack of effectiveness in after-school interventions to date. There is some evidence to suggest that single-behaviour interventions may be most successful during after-school hours. Further work is required to develop interventions delivered during this time and determine whether changes in behaviour can be maintained over extended periods of follow-up.
References
Boreham C, Riddoch C. The physical activity, fitness and health of children. J Sport Sci. 2001;19(12):915–29.
Strong WB, Malina RM, Blimkie CJ, Daniels SR, Dishman RK, Gutin B, et al. Evidence based physical activity for school-age youth. Pediatr. 2005;146(6):732–7.
Tortelero SR, Wendell CT, Murray NG. Physical activity, physical fitness and social, psychological and emotional health. In: Armstrong N, Van-Mechelen W, editors. Paediatric exercise science and medicine. Oxford: Oxford University Press; 2000. p. 273–95.
Varo JJ, Martinez-Gonzalez MA, de Irala-Estevez J, Kearney J, Gibney M, Martinez JA. Distribution and determinants of sedentary lifestyles in the European Union. Int J Epidemiol. 2003;32(1):138–46.
Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1(1):11–25.
Lobstein T, Baur L, Uauy R. Obesity in children and young people: a crisis in public health. Obes Rev. 2004;5 Suppl 1:4–104.
Sallis JF, Owen N. Ecological models. In: Glanz K, editor. Health behaviour and health education. 2nd ed. San Francisco: Jossey-Bass; 1997. p. 403–24.
Salmon J, Booth ML, Phongsavan P, Murphy N, Timperio A. Promoting physical activity participation among children and adolescents. Epidemiol Rev. 2007;29:144–59.
Cale L, Harris J. Interventions to promote young people's physical activity—issues, implications and recommendations for practice. Health Educ J. 2006;65(4):348–65.
Tudor-Locke C, Lee SM, Morgan CF, Beighle A, Pangrazi RP. Children's pedometer determined physical activity during the segmented school day. Med Sci Sports Exerc. 2006;38(10):1732–8.
Mota J, Santos P, Guerra S, Ribeiro JC, Duarte JA. Patterns of daily physical activity during school days in children and adolescents. Am J Human Biol. 2003;15(4):547–53.
Atkin AJ, Gorely T, Biddle SJH, Marshall SJ, Cameron N. Critical hours: physical activity and sedentary behaviour of adolescents after school. Pediatr Exerc Sci. 2008;20(4):446–56.
O'Connor J, Ball EJ, Steinbeck KS, Davies PSW, Wishart C, Gaskin KJ, et al. Measuring physical activity in children: a comparison of four different methods. Pediatr Exerc Sci. 2003;15(2):202–15.
Battista J, Nigg CR, Chang JA, Yamashita M, Chung R. Elementary after school programs: an opportunity to promote physical activity for children. Californian J Health Promot. 2005;3(4):108–18.
Pate RR, O'Neill JR. After-school interventions to increase physical activity among youth. Brit J Sports Med. 2009;43(1):14–8.
Robinson TN, Killen JD, Kraemer HC, Wilson DM, Matheson DM, Haskell WL, et al. Dance and reducing television viewing to prevent weight gain in African-American girls: the Stanford GEMS pilot study. Ethn Dis. 2003;13(1 Suppl 1):S65–77.
Story M, Sherwood NE, Himes JH, Davis M, Jacobs Jr DR, Cartwright Y, et al. An after-school obesity prevention program for African-American girls: the Minnesota GEMS pilot study. Ethn Dis. 2003;13(1 Suppl 1):S54–64.
Pate RR, Saunders RP, Ward DS, Felton G, Trost SG, Dowda M. Evaluation of a community-based intervention to promote physical activity in youth: lessons from Active Winners. Am J Health Promot. 2003;17(3):171–82.
Weintraub DL, Tirumalai EC, Haydel KF, Fujimoto M, Fulton JE, Robinson TN. Team sports for overweight children: the Stanford Sports to Prevent Obesity Randomized Trial (SPORT). Arch Pediatr Adolesc Med. 2008;162(3):232–7.
National Institute for Health and Clinical Excellence. The guidelines manual. London, http://www.nice.org.uk/aboutnice/howwework/developingniceclinicalguidelines/clinicalguidelinedevelopmentmethods/theguidelinesmanual2006/the_guidelines_manual_2006.jsp2006, 2006.
Jago R, Baranowski T. Non-curricular approaches for increasing physical activity in youth: a review. Prev Med. 2004;39(1):157–63.
Kahn EB, Ramsey LT, Brownson RC, Heath GW, Howze EH, Powell KE, et al. The effectiveness of interventions to increase physical activity. A systematic review. Am J Prev Med. 2002;22(4 Suppl):73–107.
Pate RR, Trost SG, Mullis R, Sallis JF, Wechsler H, Brown DR. Community interventions to promote proper nutrition and physical activity among youth. Prev Med. 2000;31(2):S138–49.
Stone EJ, McKenzie TL, Welk GJ, Booth ML. Effects of physical activity interventions in youth. Review and synthesis. Am J Prev Med. 1998;15(4):298–315.
Timperio A, Salmon J, Ball K. Evidence-based strategies to promote physical activity among children, adolescents and young adults: review and update. J Sci Med Sport. 2004;7(1 Suppl):20–9.
van Sluijs EM, McMinn AM, Griffin SJ. Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. BMJ. 2007;335(7622):703.
Cliff DP, Wilson A, Okely AD, Mickle KJ, Steele JR. Feasibility of SHARK: a physical activity skill-development program for overweight and obese children. J Sci Med Sport. 2007;10(4):263–7.
Annesi JJ, Faigenbaum AD, Westcott WL, Smith AE, Unruh JL, Hamilton FG. Effects of the Youth Fit For Life protocol on physiological, mood, self-appraisal, and voluntary physical activity changes in African American preadolescents: contrasting after-school care and physical education formats. Int J Clin Health Psychol. 2007;7(3):641–59.
Taylor RW, McAuley KA, Barbezat W, Strong A, Williams SM, Mann JI. APPLE Project: 2-y findings of a community-based obesity prevention program in primary school-age children. Am J Clin Nutr. 2007;86(3):735–42.
Taylor RW, Mcauley KA, Williams SM, Barbezat W, Nielsen G, Mann JI. Reducing weight gain in children through enhancing physical activity and nutrition: the APPLE project. Int J Pediatr Obes. 2006;1(3):146–52.
Wilson DK, Evans AE, Williams J, Mixon G, Sirard JR, Pate R. A preliminary test of a student-centered intervention on increasing physical activity in underserved adolescents. Ann Behav Med. 2005;30(2):119–24.
Wilson DK, Friend R, Teasley N, Green S, Reaves IL, Sica DA. Motivational versus social cognitive interventions for promoting fruit and vegetable intake and physical activity in African American adolescents. Ann Behav Med. 2002;24(4):310–9.
Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement. Quality of Reporting of Meta-analyses. Lancet. 1999;354(9193):1896–900.
Higgins JPT, Green S, editors. Cochrane handbook for systematic reviews of interventions, version 5.0.2 (updated September 2009). The Cochrane Collaboration; 2009.
Baranowski T, Anderson C, Carmack C. Mediating variable framework in physical activity interventions. How are we doing? How might we do better? Am J Prev Med. 1998;15(4):266–97.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Atkin, A.J., Gorely, T., Biddle, S.J.H. et al. Interventions to Promote Physical Activity in Young People Conducted in the Hours Immediately After School: A Systematic Review. Int.J. Behav. Med. 18, 176–187 (2011). https://doi.org/10.1007/s12529-010-9111-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-010-9111-z