
Abstract
Background
The benefits of physical activity to maintain optimal health and well-being in children and adolescents are undisputed. The school environment offers opportunities for children to be physically active.
Objective
The aim of this review is to systematically examine the effects of recess-based interventions on the physical activity (PA) levels of school-aged children and adolescents.
Data Sources
A systematic literature search was conducted to identify papers reporting interventions to promote PA during school recess and/or lunchtime periods. The search was conducted in six databases (PubMed, SPORTDiscus™, Web of Science, Proquest, Cochrane and Scopus) for papers published between January 2000 and April 2011.
Study Selection
Articles were included in the review if (i) they reported the findings of an intervention targeting PA levels of children and/or adolescents during school recess and/or lunchtime; (ii) have a measure of PA as an outcome variable; (iii) participants were aged between 5 and 18 years; and (iv) were published in English.
Methods
Two authors independently searched the literature using the same search strategies to identify papers reporting interventions that promote PA during school recess and lunchtime periods. Methodological quality was assessed using an adapted eight item assessment scale. The effects of the interventions were assessed with a rating system used in a recent review of interventions in youth.
Results
The search originally retrieved 2,265 articles. Nine published peer-reviewed journal articles met the inclusion criteria for this review. Eight studies used randomized controlled trials and one was a controlled trial. Three studies demonstrated high methodological quality (33%). None of the studies adequately reported the randomization procedure or used power calculations. Few studies reported potential confounders and three studies had less than a 6 week follow-up. Five studies demonstrated a positive intervention effect on children’s PA levels, with four reporting statistically significant increases and two reporting significant decreases in recess PA. The summary of the levels of evidence for intervention effects found inconclusive results for all intervention types, though promising strategies that require further investigation were identified.
Limitations
Whilst every effort was made to ensure that this review was as encompassing as possible, it may be limited by its search terms especially if there were studies with unclear titles or abstracts. In addition, only manuscripts published in English were considered, eliminating any possible studies published in other languages.
Conclusions
All of the studies used an objective measure to assess PA outcomes, although several criteria were consistently absent from the studies. The levels of evidence were not sufficient to establish conclusive intervention effects on children’s recess PA. This could be due to the small number of published studies. There is a need for higher-quality intervention research to strengthen published findings to inform recess PA interventions. Intervention research is needed in adolescents due to the absence of school recess intervention research in this population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Physical inactivity is a major contributor to the chronic disease burden as it is associated with increased risk of coronary heart disease, diabetes mellitus, osteoporosis, some cancers, mental illness and obesity [1–4]. The benefits of physical activity (PA) in maintaining optimal health and well-being in children and adolescents are undisputed. There is a consensus among developed countries that children and youth should accumulate a minimum of 60 minutes of moderate-to-vigorous physical activity (MVPA) every day [1, 5, 6]. The opportunity for children and adolescents to be active has declined in many countries over time, and is likely due to a combination of factors including school policies, parental rules and environmental factors, such as a reduction in active travel to and from school [7, 8].
The school environment plays a crucial role in providing opportunities for children to be physically active [6, 9–11]. However, schools are often pressured to meet curricular goals that compete with opportunities for PA, including physical education and school recess [12, 13]. As there are inconsistencies with terminology for school recess, a broad definition has been used. Recess is defined as “the non-curricular time allocated by schools between lessons for children to engage in physical activity and leisure activities” [14] (p. 361), and often includes lunchtime (that is also considered a recess period in some countries). School recess offers an ideal opportunity for children to be active on a daily basis in many countries around the world. Moreover, as most children attend school and many schools have facilities to provide PA opportunities during recess, this time of the day has the potential to contribute up to 40% towards PA recommendations [14]. In recent years, there has been increasing interest in the promotion of children’s PA during school recess using a number of different strategies, including playground markings and games equipment [14]. However, the evidence concerning these approaches has not yet been reviewed to identify the effects of recess-based interventions in school environments. Consequently, the aim of this review was to systematically examine the effects of recess interventions on PA levels among school-aged children and adolescents.
2 Methods
2.1 Identification of studies
A systematic literature search was conducted to identify papers reporting interventions to promote PA during school recess and/or lunchtime periods. The search was conducted in six databases (PubMed, SPORTDiscus™, Web of Science, Proquest, Cochrane and Scopus). Two authors (AMP and NDR) independently searched the literature using the same search strategies. The search included the following key words: ‘child’, ‘infant’, ‘youth’, ‘adolescent’, ‘school’, ‘primary’, ‘elementary’, ‘middle school’, ‘high school’, ‘secondary’, ‘breaktime’, ‘break time’, ‘school recess’, ‘recess’, ‘playtime’, ‘lunchtime’ and ‘free play’. Abstracts, expert opinions, commentaries, case studies, conference proceedings and dissertations were excluded from the review. The review only included published peer-reviewed journal articles. Additional papers were sourced from bibliographies of the retrieved papers and the authors’ personal collections. Initially, journal titles and abstracts were searched for relevance. When appropriateness of the article could not be determined, full-text articles were retrieved for consideration.
2.2 Inclusion/Exclusion Criteria
Articles were included in the review if (i) they reported the findings of an intervention targeting PA levels of children and/or adolescents during school recess and/or lunchtime; (ii) they had a measure of PA as an outcome variable; (iii) participants were aged between 5 and 18 years; (iv) they were written in English; and (v) were published between January 2000 and April 2011 [15].
2.3 Assessment of Methodological Quality
Methodological quality was assessed using an adapted eight-item assessment scale described by van Sluijs and colleagues [15] (Table 1). Three items were removed from the scale as two (‘drop out’ and ‘intention to treat’) were only pertinent to studies that focused on individual measures, and the remaining item (blinded assessments) was not possible given the nature of the studies involved in the review. Two reviewers (AMP and ADO) independently assessed each article to determine whether the study rated as ‘positive’ or ‘negative’ for each item. Study items that were ‘insufficiently described’ were given a negative score [15]. The reviewers considered any item where there was disagreement until consensus was reached. The accumulated positive scores for each study were used as a measure of quality. The quality scores were proportionally adapted for the eight-item assessment scale [15]. That is, a study was considered to be high quality if it scored ≥5 for a randomized controlled trial (RCT) and ≥4 for a controlled trial (CT).
2.4 Intervention Studies Compared
To compare studies, the following data were extracted from each research paper: (i) study overview including author/date, country of study, population characteristics, intervention type and length of follow-up, method of assessing PA, PA outcome variables, break period assessed, recess length and a description of the recess; (ii) study design and randomization process; (iii) intervention details; and (iv) intervention effectiveness through examination of the levels of evidence and change observed. A study was considered large if the sample size was more than 250 participants.
2.5 Levels of Evidence
A meta-analysis was considered inappropriate for this review due to the divergent nature of the studies when considering sample size, data collection and randomization methods, PA measures, and the complexities of the school environment. In addition, a meta-analysis requires that the systematic review considers studies of acceptable quality [16]. The limitation of including low-quality studies in a meta-analysis could result in inappropriate findings [16]. With reference to data analysis techniques, some studies used multilevel modelling (MLM) to analyse data, which is an appropriate technique for nested designs but is best avoided when there is no heterogeneity between studies [17]. In the literature to date, studies utilizing MLM have typically reported the intervention effect and adjusted for a number of confounding variables. However, few studies have reported unadjusted mean scores separately for the intervention and control groups, which makes it difficult to calculate effect sizes for use in a meta-analysis [18]. Consequently, a scoring system used in a recent review of child and adolescent PA interventions was adopted [15]. To maintain consistency with this review [15], a rating system that includes five levels (strong, moderate, limited, inconclusive or no evidence) was used to describe the effect of the intervention. Evidence was based on study design, methodological quality and sample size. Strong, moderate or limited levels of evidence were identified for each recess intervention strategy when at least two-thirds of the studies reported significant positive results [15]. Studies were required to have more than 250 participants to be considered large when considering levels of evidence [15]. A detailed explanation of the decision-making process is provided as a supplement by van Sluijs and colleagues [15].
3 Results
3.1 Overview
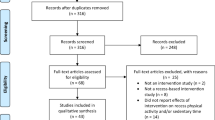
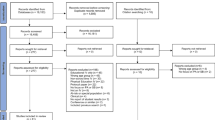
The extraction process for studies included in the final review is outlined in Fig. 1. The database search originally retrieved 2,265 articles. After screening, nine published peer-reviewed journal articles met the inclusion criteria for this review. Sample sizes examining intervention effects ranged from 28 to 470 children, whilst one study assessed PA using direct observation (at 13 schools) where the average enrolment was 667 children at each school [19]. No studies examining recess interventions in adolescent populations met the inclusion criteria. Six studies were conducted in the UK [20–25] and the remaining three studies were conducted in Belgium [26], Cyprus [27] and the US [19], respectively. Five studies targeted schools from lower socioeconomic areas [19, 21–23, 25]. A range of follow-up periods were investigated. Five studies used short-term follow-up periods of 6 weeks or less [20, 21, 23, 24, 27], while 4 studies examined intervention effects over 3–12 months [19, 22, 25, 26]. Five of the studies used a multicomponent approach [19, 22, 23, 25, 27] and the remainder used a single intervention [20, 21, 24, 26]. A range of objective measures were used to measure PA, including heart rate monitors [20, 21], accelerometers [23, 26], pedometers [27] direct observation [19], and a combination of these measures [22, 24, 25]. All studies assessed MVPA and vigorous PA (VPA) except one that used steps to assess PA outcomes [27]. A number of different recess periods were examined in the studies. Four studies reported school recess breaks [20, 21, 23, 25] using morning, lunch and afternoon periods, one study reported before school, morning and lunch periods [19], two studies reported morning and lunch recess periods [22, 26], and two studies reported only one break, a morning recess [27] and lunch recess [24], respectively. Further details of the studies, including recess length and a description of the recess period are summarized in Table 2.

Flowchart of included studies
3.2 Study Design and Randomization Process
Eight studies were RCTs [19–24, 26, 27] and one used a CT design [25]. Four of the RCTs were randomized at the school level and four at the individual level. None of the studies adequately described the randomization process. Details concerning the study designs are provided in Table 3.
3.3 Intervention Details
A summary of the interventions used during school recess are reported in Table 2. A range of intervention strategies were implemented. Five studies used multiple intervention strategies that included a combination of playground markings, physical structures, colour-coded playground areas and zones, non-fixed equipment, court rotation and organized activities [19, 22, 23, 25, 27]. These studies included one small [23] and one large high-quality RCT [22] and one large high-quality CT [25]. The remaining four studies investigated single strategy interventions using playground markings, games equipment and active video games [20, 21, 24, 26]. All studies involved male and female participants and all but one study [24] reported male and female results separately.
3.4 Methodological Quality
There was 96.3 % agreement on the 72 items scored during the quality assessment. Consensus was reached on three items where originally there was disagreement. Three studies demonstrated high methodological quality (33 %) [22, 23, 25], four studies had more than 250 participants [19, 22, 23, 25] and three studies had a follow-up period of ≥6 months [19, 22, 25]. Table 4 provides a summary of the methodological quality analysis.
3.5 Intervention Effectiveness
Five studies demonstrated a positive intervention effect on children’s PA levels during school recess (see Table 3) [20, 21, 25–27]. Four of these studies reported statistically significant findings [21, 25–27]. Playground markings and games equipment significantly increased children’s recess and lunchtime moderate PA, VPA and MVPA compared with controls [21, 25, 27]. Studies that examined combined strategies had mixed findings, with two approaches significantly increasing children’s MVPA, VPA and steps [25, 27] and three reported no significant effects [19, 22, 23]. Studies that found a significant increase in mean MVPA during recess reported increases ranging from 4 to 12.9 % [21, 25–27]. Two studies reported a significant decrease in MVPA. One study used a video gaming intervention that decreased children’s MVPA and steps [24], while the other combined strategies resulted in decreased activity in boys [19]. Table 3 provides a summary of the effectiveness of interventions whilst Table 5 reports the levels of evidence for the intervention effect on promoting school break-time PA. Despite some promising findings regarding playground markings, games equipment and combined strategies, the levels of evidence were not sufficient to establish conclusive intervention effects on children’s recess PA.
4 Discussion
This review investigated the effectiveness of school recess interventions on children’s and adolescent’s PA. Nine studies were identified that had implemented interventions in primary (elementary) school settings, while no intervention studies were found for adolescent populations. Overall, this review found that the levels of evidence concerning the effectiveness of recess interventions in children were inconclusive, though some promising strategies were identified.
4.1 Intervention Components
The majority of studies within this review utilized multiple component interventions during school recess. Research investigating multicomponent interventions has combined a range of different strategies, making it difficult to conclude which approach is most effective. It should be noted, however, that the strategies that combined playground markings, playground coding or court rotation (to rotate playground use) and non-fixed equipment increased recess PA significantly, suggesting that this may be a promising strategy that could benefit PA levels during school recess. More research is needed, however, to identify effective multicomponent recess-based strategies in school-aged children.
Whilst multicomponent approaches highlight that recess is a complex setting in which to intervene, and that multiple strategies may be needed to increase PA levels, future research should also investigate which single-component interventions are effective in increasing recess pa. There is currently a dearth of literature examining single component interventions, yet such information would have the potential to identify strategies that could be used in combination with other strategies or highlight appropriate strategies for different populations of children. Of the single-component strategies used, games equipment [26] and playground markings [20, 21] significantly increased PA during recess, whilst active video games [24] had a negative outcome on children’s lunchtime activity levels. Taken together, these findings suggest that recess intervention strategies should aim to facilitate free play in an outdoor environment.
The review did not find any interventions addressing school recess PA among adolescents. This was not surprising, as few studies have examined adolescents’ PA levels in this context in the literature to date [14, 28]. However, this finding was concerning, given that adolescents’ recess and daily PA levels decrease over time [36]. Indeed, since recess can contribute up to one-quarter of their daily PA levels [29], recess interventions for adolescents have the potential to benefit their daily PA levels. The lack of interventions in this context highlights a missed opportunity to encourage adolescents to be active in an environment that may be relatively free of electronic sedentary distractions. Future research should investigate the most ideal activities to promote adolescent school recess PA, and examine these using appropriate interventions over time.
Eight of the interventions in this review aimed to increase children’s PA using environmental changes to or within the school playground environment. The influence of policy and social variables were not assessed, though changes within the playground are likely to influence social aspects of school recess. It is possible that variables such as the influence of peers, teachers and school policy may influence playground PA levels [30]. For instance, policies can restrict playground activity as a form of punishment, and antisocial behaviour may affect children’s willingness to participate in playground PA [30, 31]. Future intervention studies should examine the effects of interventions on policy and social variables in combination with the effects on recess PA levels.
An important consideration during this review was whether the interventions examined had social validity; that is, the intervention strategies avoided negative consequences such as decreasing PA. Overall, the majority of strategies employed benefited boys’ and girls’ recess PA levels. One study decreased children’s PA levels during lunchtime [24], suggesting that active gaming during lunchtime may not be a suitable approach for increasing PA levels during a time when children engage in spontaneous activities. In addition, one study found that boys in the intervention group were significantly less active in the playground after 12 months compared with their control group peers [19]. This study used a combination of playground markings, a walking club and organized recess activities. It is possible that the types of organized recess activities did not suit boys, or did not promote as much PA as their usual unstructured play activity. Research indicates that boys prefer to play games, including ball, fantasy and rough and tumble games [14, 32, 33]. Boys tend to dominate playground space and play in larger groups [33, 34]. Sarkin and colleagues [35] suggest that structured activities in the school environment may benefit girls PA over boys. It is therefore not surprising in this study that structured interventions did not increase boy’s PA levels. Research is needed to identify interventions that have social validity, and benefit target children’s PA without negatively affecting other children’s activity levels during recess.
Variability between study methods can cause difficulties when evaluating which strategies are effective for promoting recess PA. For example, studies in the review differed in the length of their intervention periods, and there were differences in the combinations of the intervention approaches. Six of the nine studies had inadequate follow-up duration periods. Ideally the duration of an intervention should be a minimum of 6 months [15]. With the majority of recess interventions conducted thus far examining short-term follow-ups, they may have captured novelty effects of the intervention, making decisions concerning the effectiveness of strategies difficult to determine. Some strategies (e.g. playground markings, games equipment) show promise as intervention strategies, but further work in more diverse settings are needed; findings are currently inconclusive at best.
4.2 Methodological Quality
Only three of the nine studies (33 %) were rated as demonstrating high methodological quality. A strength of all the studies was the use of objective measures to assess PA outcomes. However, several criteria were consistently absent from the studies. For example, none of the studies adequately reported the randomization procedure or used power calculations. Few studies reported potential confounders and three studies had less than a 6 week follow-up, falling well short of the recommended 6 month follow-up period [15]. It is essential that intervention studies are reported transparently to ensure external validity, enhance the current literature base and allow the determination of the quality of each study. A lack of detail could mask potential limitations or poor quality research, possibly leading to inappropriate interpretation of results. Furthermore, the summary of the levels of evidence for intervention effects indicates inconclusive results for all intervention types, which could be largely due to the small number of large high-quality studies. The limited number of high-quality studies testing both multi- and single-component interventions indicates an urgent need for higher-quality intervention research to strengthen published findings and to enable practitioners to identify which interventions may be most effective to increase children’s PA levels during school recess.
4.3 Limitations
There are several limitations associated with this review. Whilst every effort was made to ensure that this review was as encompassing as possible, it may be limited by its search terms, especially if there were studies with unclear titles or abstracts. A meta-analysis was not possible due to the divergent nature of the interventions such as sample size, data collection and randomization methods, PA measures and the complexities of the school environment. In addition, only manuscripts published in English were considered, eliminating any possible studies published in other languages.
4.4 Recommendations
The use of methodological checklists as a guide when designing intervention research could assist in improving intervention methodological quality in school recess PA research. Whilst there has been interest in recess interventions in recent years, the overall lack of interventions investigating strategies used to increase children’s PA levels indicates a need for further research in this area. In particular, there is a need to target adolescents due to the absence of adolescent school recess intervention research, despite the contribution that recess can make to an adolescent’s daily PA. Lastly, it is possible that some intervention strategies are more beneficial for males and females or lower and upper primary/elementary school [23]. Further research is needed to identify the most appropriate strategies to increase PA in these population subgroups.
5 Conclusion
There is currently a dearth of intervention studies investigating the effectiveness of school recess strategies to increase PA for children and adolescents. The small number of studies and lack of high-quality research resulted in an absence of conclusive results for any of the four types of intervention methodologies used to date. School environments provide potential opportunities to increase children’s PA levels, although there is a need for more methodologically sound interventions to promote PA during school recess, with a particular focus on adolescents.
References
World Health Organisation. Global strategy on diet, physical activity and health. Geneva: WHO; 2004.
Cancer Council New South Wales. Position statement: physical activity and reducing cancer risk. Kings Cross: Cancer Council, 2009 [online] Available from URL: http://www.cancercouncil.com.au/html/healthprofessionals/nutrition_physical/downloads/position%20statement%20-%20physical%20activity.pdf. [Accessed 2011 Oct 25].
Royal Australian College of General Practitioners. Physical activity: policy endorsed by the 50th RACGP Council. 2008 [online]. Available from URL: http://www.racgp.org.au/policy/Physical_activity.pdf [Accessed 2011 Oct 25].
Strong WB, Malina RM, Blimkie CJR, et al. Evidence based physical activity for school-age youth. J Pediatr. 2005;146(6):732–7.
Australian Government Department of Health and Ageing. Active kids are healthy kids. Australia’s physical activity recommendations for 5–12 year olds. Canberra (ACT): DoHA, 2004 [online]. http://www.health.gov.au/internet/main/publishing.nsf/Content/9D7D393564FA0C42CA256F970014A5D4/$File/kids_phys.pdf [Accessed 25 Oct 2011].
Pate RR, Davis MG, Robinson TN, et al. Promoting physical activity in children and youth. Circulation. 2006;114(11):1214–24.
Dollman J, Norton K, Norton L. Evidence for secular trends in children’s physical activity behaviour. Br J Sports Med. 2005;39(12):892–7.
Meron D, Rissel C, Reinten-Reynolds T, et al. Changes in active travel of school children from 2004 to 2010 in New South Wales, Australia. Prev Med. 2011;53(6):408–10.
Kriemler S, Meyer U, Martin E, et al. Effect of school-based interventions on physical activity and fitness in children and adolescents: a review of reviews and systematic update. Br J Sports Med. 2011;45(11):923–30.
Centre for Disease Control. School health guidelines to promote healthy eating and physical activity. Mortality and Morbidity Weekly Report. 2011;60(5).
Robert Wood Johnson Foundation. Recess rules: why the undervalued playtime may be America’s best investment for healthy kids and healthy schools. Princeton: Robert Wood Johnson Foundation; 2007.
Beurden E, Barnett LM, Zask A, et al. Can we skill and activate children through primary school physical education lessons? “Move it groove it”: a collaborative health promotion intervention. Prev Med. 2003;36(4):493–501.
Evans J. Changes to (primary) school recess and their effect on children’s physical activity: an Australian perspective. J Phys Educ NZ. 2003;36(1):53.
Ridgers ND, Stratton G, Fairclough SJ. Physical activity levels of children during school playtime. Sports Med. 2006;36(4):359–71.
van Sluijs EMF, McMinn AM, Griffin SJ. Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. BMJ. 2007;335(7622):703.
Crombie IK, Davies HT. What is a meta-analysis? Evidence based medicine: what is? series. 2nd ed [online]. Available from URL: http://www.medicine.ox.ac.uk/bandolier/painres/download/whatis/syst-review.pdf [Accessed 1 Jun 2012].
Higgins JPT, Green SE, editors. Cochrane handbook for systematic reveiws. 2011 [online]. Available from URL: http://www.mrc-bsu.cam.ac.uk/cochrane/handbook/ [Accessed 1 of June 2012].
Goldstein H, Yang M, Omar R, et al. Meta-analysis using multilevel models with an application to the study of class size effects. J R Stat Soc Ser C Appl Stat. 2000;49(3):399–412.
Elder JP, McKenzie TL, Arredondo EM, et al. Effects of a multi-pronged intervention on children’s activity levels at recess: the Aventuras para Ninos Study. Adv Nutr. 2011;2:171S–6S.
Stratton G. Promoting children’s physical activity in primary school: an intervention study using playground markings. Ergonomics. 2000;43:1538–46.
Stratton G, Mullan E. The effect of multicolor playground markings on children’s physical activity level during recess. Prev Med. 2005;41(5–6):828–33.
Ridgers ND, Fairclough SJ, Stratton G. Twelve-month effects of a playground intervention on children’s morning and lunchtime recess physical activity levels. J Phys Act Health. 2010;7(2):167–75.
Ridgers ND, Stratton G, Fairclough SJ, et al. Children’s physical activity levels during school recess: a quasi-experimental intervention study. Int J Behav Nutr Phys Act. 2007;4:19.
Duncan M, Staples V. The impact of a school-based active video game play intervention on children’s physical activity during recess. Hum Mov. 2010;11(1):95–9.
Ridgers ND, Stratton G, Fairclough SJ, et al. Long-term effects of a playground markings and physical structures on children’s recess physical activity levels. Prev Med. 2007;44(5):393–7.
Verstraete SJM, Cardon GM, De Clercq DLR, et al. Increasing children’s physical activity levels during recess periods in elementary schools: the effects of providing game equipment. Eur J Public Health. 2006;16(4):415–9.
Loucaides CA, Jago R, Charalambous I. Promoting physical activity during school break times: piloting a simple, low cost intervention. Prev Med. 2009;48(4):332–4.
Ridgers ND, Salmon J, Parrish AM, et al. Review of correlates of children’s and adolescent’s physical activity during school recess periods. Am J Prev Med. 2012;43(3):320–8.
Ridgers ND, Timperio A, Crawford D, et al. Five-year changes in school recess and lunchtime and the contribution to children’s daily physical activity. Br J Sports Med. 2012;46(10):741–6.
Parrish A-M, Yeatman H, Iverson D, et al. Using interviews and peer pairs to better understand how school environments affect young children’s playground physical activity levels: a qualitative study. Health Educ Res. 2012;27(2):269–80.
Parrish AM, Iverson D, Russell K, et al. Psychosocial barriers to playground activity levels. Br J School Nurs. 2012;7(3):20–6.
Pate RR, Baranowski TOM, Dowda M, et al. Tracking of physical activity in young children. Med Sci Sports Exerc. 1996;28(1):92–6.
Blatchford P, Baines E, Pellegrini A. The social context of school playground games: sex and ethnic differences, and changes over time after entry to junior school. Br J Dev Psychol. 2003;21(4):481–505.
Boyle DE, Marshall NL, Robeson WW. Gender at play. Am Behav Sci. 2003;46(10):1326–45.
Sarkin JA. Gender differences in physical activity during fifth-grade physical education and recess periods. J Teach Phys Educ. 1997;17(1):99.
Kjønniksen L, Torsheim T, Wold B. Tracking of leisure-time physical activity during adolescence and young adulthood: a 10-year longitudinal study. Int J Behav Nutr Phys Act. 2009;5:69.
Acknowledgments
Funding: Anthony D. Okely is supported by a National Heart Foundation of Australia Career Development Fellowship (CR11S 6099). Nicola Ridgers is supported by an Australian Research Council Discovery Early Career Researcher Award (DE120101173). The remaining authors received no funding.
Conflict of interest
There are no known conflicts of interest that are directly relevant to this content of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Parrish, AM., Okely, A.D., Stanley, R.M. et al. The Effect of School Recess Interventions on Physical Activity. Sports Med 43, 287–299 (2013). https://doi.org/10.1007/s40279-013-0024-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-013-0024-2