
Abstract
Skull fracture is a common finding following head trauma. It has a prognostic significance and its presence points to severe trauma. Additionally, there is a greater possibility of detecting associated small underlying extra-axial hematomas and subtle injuries to the brain parenchyma. In pediatric patients, the presence of multiple open sutures often makes fracture evaluation challenging. In our experience, 3D volume (3DV)-rendered CT images complement routine axial bone window (RBW) images in detection and characterization of fractures. This is a multi-reader, multi-case, paired retrospective study to compare the sensitivity and specificity of RBW and 3DV images in detection of calvarial fractures in pediatric patients. A total of 60 cases (22 with fractures and 38 without) were analyzed. Two experienced neuroradiologists and a radiology trainee were the readers of the study. For all readers, the sensitivity was not statistically different between the RBW and the 3DV interpretations. For each reader, there was a statistically significant difference in the interpretation times between the RBW and the 3DV viewing formats. A greater number of sutural diastasis was identified on 3DV. We propose that 3DV images should be part of routine head trauma imaging, especially in the pediatric age group. It requires minimal post-processing time and no additional radiation. Furthermore, 3DV images help in reducing the interpretation time and also enhance the ability of the radiologist to characterize the calvarial fractures.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Skull fracture is a common finding following head trauma. It has a prognostic significance and its presence points to severe trauma. Additionally, there is greater possibility of detecting associated small underlying extra-axial hematomas and subtle injuries to the brain parenchyma. In specific circumstances like non-accidental trauma, detection of fractures is of paramount importance for diagnosis. For the evaluation of skull fracture, non-contrast head CT (NECT) is considered the gold standard. In pediatric patients, the presence of multiple open sutures often makes fracture evaluation challenging [1]. In our experience, 3D volume (3DV)-rendered CT images complement routine axial bone window (RBW) images in detection and characterization of fractures. While multiple studies have demonstrated the value of 3DV in pre-surgical planning and management in maxillofacial trauma [2, 3] studies investigating the use of 3DV in evaluation of calvarial fractures are very few. Hence, this retrospective study was conducted to compare the sensitivity and specificity of RBW and 3DV images in detection of skull fractures in pediatric patients.
Materials and methods
This is a multi-reader, multi-case, paired retrospective study. The HIPAA-compliant study protocol was approved by our institutional review board (IRB), with a waiver of informed consent. Images used in this study had been exclusively generated for clinical purposes; no additional images were acquired or generated for this study.
Case selection
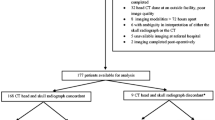
We searched our radiology report database from January 2011 through November 2012 for CT head reports with the keyword “fracture” and selected only the patients who met all the following criteria: pediatric age group (less than 17 years old); presented to the emergency room with history of trauma and had head CT at the emergency room, and had a repeat head CT within 5 days. Consecutive cases of positive calvarial fractures were identified in this dataset by reviewing the reports. There were no restrictions with respect to gender. The patients with skull base or facial fracture, but without calvarial fractures were excluded. Images from the initial CT study at the emergency room were selected for the study. By selecting only patients with a repeat scan in a short interval, we intended to select cases with significant head trauma and exclude less severe injuries. Age-matched pediatric head CTs without fractures (half of them with scalp swelling and the other half without) were selected from the ER radiology database as controls. A total of 60 cases were included in the reader study.
CT technique
All the examinations were performed with a commercially available 64-detector row scanner (Brilliance 64, Philips Healthcare, Best, The Netherlands) without intravenous contrast administration. The CT was performed in helical mode in patients less than 7 years old (120 KV, 225 mAs, 16 × 0.625 collimation, 0.75-s rotation time, 1.058 pitch). Axial mode was used in patients who were older than 7 years (120 KV, 250 mAs, 16 × 0.625 collimation, 1-s rotation time). Five-millimeter axial images using soft tissue and bone filter kernels, 0.625-mm-thick axial images, 3-mm-thick coronal and sagittal reformats, and 3D volume-rendered images were generated on the scanner and sent to picture archiving and communication system (PACS). The RBW images used in this study included 5 mm (standard) and 0.6 mm (thin section) axial bone series. Volume rendered images rotated about the z-axis that were generated at the time of original study were used for study analysis.
Readers of the study
The study readers included two radiologists, who are board certified in neuroradiology with 8 and 15 years of subspecialty experience, and a third year radiology resident. The readers interpreted the images on diagnostic workstation blinded to the diagnosis, patient metrics, history, and other information. Each reader provided 120 interpretations, 60 each for RBW and 3DV formats. In each session and for each reader, either the RBW images (both axial 5 mm as well as 0.6-mm-thin axial slices) or the 3DV images were provided. For each reader and for each case, there was at least a 2-week gap between the RBW and 3DV interpretation sessions to minimize memorization bias. During interpretation, each reader was instructed to record the presence or absence of fractures and, if a fracture was present, to describe the extent of fractures with the bones involved. The time taken for interpretation by each reader and for each case was recorded with a stopwatch.
Reference standard
Six weeks after completion of all reader sessions, the two experienced neuroradiologists, who were participants in the reader study, performed a consensus read, which was considered the reference standard (truth). This consensus read was obtained by referring to entire imaging (RBW and 3DV) including follow-up CT scans, and all available patient information.
Statistical methods
The sensitivity and specificity for RBW and 3DV interpretations were analyzed with and without consideration as to whether the location of the fracture was correctly identified. For the location-independent analysis, the reader interpretation for the presence or absence of fracture was binary coded (presence = 1; absence = 0). McNemar’s test (two-tailed) for correlated proportions was used to determine if the sensitivity and specificity differed between RBW and 3DV interpretations for each reader, for both radiologists (pooled) and for all readers (pooled). Additionally, to understand the effect of combined interpretation of RBW and 3DV images on sensitivity and specificity, if at least one of the two interpretations (either RBW or 3DV) was positive for the presence of fracture, then it was treated as positive for the combined interpretation. For the location-dependent analysis, if either the suture or at least two of the adjoining bones were correctly identified, then the interpretation was considered positive and correctly localized for the analysis. If the interpretation indicated the presence of the fracture without correct identification of either the suture or the adjoining bones, then the interpretation was considered negative for the analysis. The sensitivity and specificity were computed and analyzed in a similar manner as the location-independent analysis. Depending on whether the interpretation times for each viewing format (RBW and 3DV) satisfied the normality assumption (Shapiro-Wilk’s test), and either the paired t test or the Wilcoxon signed rank test was used to identify if the interpretation time varied between the viewing formats. Additionally, the data was analyzed to determine if the difference in interpretation times between RBW and 3DV was statistically different among the readers. Statistical analysis was performed using SAS (Version 9.3, SAS Inc., Cary, NC). Effects associated with p values less than 0.05 were considered statistically significant.
Results
The reference standard from consensus interpretation by two experienced radiologists indicated that there were 22 cases with skull fracture and the remainder (38 cases) did not have skull fracture. For all interpretations, when the fracture was detected, the location of the fracture was correctly identified by either the suture or the adjoining bones. Hence, the results from the location-dependent analysis are identical to the location-independent analysis.
For all readers (pooled), for the two experienced radiologists (pooled) and for each individual reader, the sensitivity was not statistically different between the RBW and the 3DV interpretations (p > 0.317, McNemar’s test). Also, the combined interpretation did not differ with either the RBW (p > 0.157) or the 3DV (p > 0.083) interpretations. Similar analysis for the specificity showed that for each reader, for the two experienced radiologists (pooled), and for all readers (pooled), the specificity did not statistically differ between the RBW and the 3DV interpretations (p > 0.317), and between the 3DV and the combined interpretations (p > 0.317). There were no discordant pairs between the RBW and the combined interpretations. Tables 1 and 2 summarize the sensitivity and specificity, respectively, for RBW and 3DV interpretations.
Sutural diastasis was present in five cases (one involving the squamosal suture, three in coronal suture, one in sagittal suture). The one case with squamosal sutural diastasis was missed in RBW by all the readers. Three of the other four were missed by the resident reader on RBW.
For each reader, the interpretation times for both viewing formats (RBW and 3DV) did not satisfy the normality assumption (p < 0.021, Shapiro-Wilk’s test). Hence, Wilcoxon signed ranks test was used to determine if the interpretation times differed between the RBW and the 3DV viewing formats. For each reader, there was a statistically significant difference in the interpretation times between the RBW and the 3DV viewing formats (p < 0.001). Figure 1 provides the box plots of the interpretation times for RBW, 3DV, and the difference in interpretation time between RBW and 3DV formats (difference = RBW − 3DV) for each reader. The difference in interpretation time between RBW and 3DV formats varied among the three readers (p < 0.001, Kruskal-Wallis test). For the two experienced radiologists, the difference in interpretation time between RBW and 3DV formats was also statistically significant (p = 0.0013, Wilcoxon-Mann-Whitney test). Also, the differences in interpretation time between RBW and 3DV formats between the resident and each experienced radiologist was also statistically significant (p < 0.001). Table 3 summarizes the interpretation time for all readers (pooled), for both experienced radiologists (pooled), and for each reader.

Box plots of the interpretation times for routing bone windows (RBW), 3D volume rendering (3DV), and the difference in interpretation time between RBW and 3DV formats (difference = RBW − 3DV) for each reader. For each reader, there was a statistically significant difference in interpretation time between RBW and 3DV (p < 0.001), with shorter duration for 3DV interpretation
Discussion
The diagnosis of the fracture itself is not clinically more important than intracranial hemorrhage, contusion, or ischemia. However, there are other events that accompany skull fractures such as hemorrhage, cerebrospinal fluid leakage, neurovascular injury, meningitis, cranial nerve palsy, carotid artery dissection, and carotid-cavernous fistula that can change patient management as well as prognosis and there are legal issues [4, 5]. Subtle non-displaced fractures can be missed on thick axial sections of the CT (Fig. 2). It is important to reduce the incidence of missing such fractures to minimize the potential adverse consequences. Thin sections and 3DV are likely of benefit (Fig. 2). In cases of non-accidental trauma, missing fractures may result in improper diagnosis and may have a dire consequence.

Non-displaced fracture in the right parietal bone. Not appreciated in thick axial slices (a); subtle on 0.6-mm axial slice (arrow in b); easily identifiable in 3DV (arrow in c). Time taken for interpretation was over 2 min for axial slices and less than half a minute for 3DV
Although detection of fractures is straight forward in a majority of CT scans, there are potential pitfalls. Cranial sutures (more so in variant anatomy like accessory sutures) and neurovascular markings resemble the appearance of fractures. The parietal and occipital bones, in particular, are common regions for accessory sutures because of their multiple ossification centers [6]. Non-displaced skull fractures show sharp lucencies with non-sclerotic edges, as opposed to sclerotic and wavy margins of the sutures. When fractures extend into a major suture, there could be widening of the fracture line as it approaches the suture or there could be associated diastasis of the adjacent synchondrosis or suture (Fig. 3) [6]. An accessory suture will usually not produce this appearance. High-impact fractures can cross suture lines or extend from one major suture to another, whereas accessory sutures join and merge with the major suture. Accessory sutures are often bilateral and fairly symmetric. Sutural diastasis can be less apparent in RBW. In one of our cases, although the adjacent fracture was identified, the squamosal sutural diastasis was missed on RBW by all the three readers (Fig. 4). 3DV simplifies the imaging evaluation of sutures. It facilitates differentiation of sutures and fractures and improves visualization of sutural diastasis.

Left parietal lucency (black arrow) with sharp margins and widening as it approaches the lambdoid suture, indicating a fracture and not an accessory intraparietal suture. Accessory occipital suture (white arrow) showing the expected imaging features of a suture

Squamosal sutural diastasis (arrow in a) missed on RBW by all three readers. Normal suture on the contralateral side (arrow in b) for comparison
Skull fractures, when they occur parallel to the acquisition plane, may be wholly invisible on axial images [7]. Additionally, non-displaced morphology of the fractures and volume averaging from adjacent high attenuation bone may make fracture visualization difficult on axial images [8]. 3DV can act as problem solver in these cases [9]. In our study, the sensitivity of RBW and 3DV was equivalent. This is mainly due to the inclusion of 0.6-mm axial slices for interpretation, which is a part of routine head CT at our institution. Based on our clinical experience, if only 5-mm axial slices were to be used for interpretation, then the sensitivity of the RBW could have been lower.
With the current multidetector CTs, in addition to the traditional 5-mm axial slices, we have thinner axial slices, multi-planar reformats, and 3DV to aid in the diagnosis. Although these additional images could increase the accuracy [9, 7], they can result in increased time for interpretation; this can be an issue with the need for expedient interpretation in emergency radiology, particularly for high-volume settings. Efficient use of resources has become a necessity. A more time-efficient way of visualizing fractures is extremely advantageous to the radiologist, and ultimately provides better patient care. Our study shows 3DV is equally sensitive and specific for detection of calvarial fractures and is more time-efficient. For experienced readers, the time efficiency increases, as demonstrated in our study.
3DV of the skull yield important clinical information regarding the etiology of the fractures (e.g., a blow vs. a fall) and/or the type of weapon used as well as the dynamics of the event [10] (Fig. 5). 3DV is also superior to simple x-ray in the assessment of the pediatric skull fracture due to incomplete skull ossification [11]. They are helpful in the better understanding of spatial relations of the fractures and for surgical planning [12].

Comminuted depressed skull fracture secondary to fall on a rock. Corroboration with mechanism of injury is obvious on EDV
Limitations to the study include the following: coronal and sagittal reformats were not used when evaluating for fractures in this study. We limited this as coronal and sagittal reformats may not be routine in other institutions. 3DV were limited to rotation about the z-axis. While free control over 3D rotation would be ideal, we only analyzed preprocessed images that were present on the PACS. We did not specifically evaluate the other commonly used 3D reconstruction method, i.e., the surface-shaded display. Prior studies have shown the superiority of volume rendering technique over the surface rendering [13]. The size of the study with 22 positive fracture cases out of 60 cases was small but was sufficient to demonstrate a statistically significant time difference in fracture evaluation between RBW and 3DV images.
We propose that 3DV images should be part of routine head trauma imaging, especially in the pediatric age group. It requires minimal post-processing time and no additional radiation. Furthermore, 3DV images help in reducing the interpretation time and also enhance the ability of the radiologist to characterize the calvarial fractures.
References
Pekcevik Y, Hasbay E, Pekcevik R (2013) Three-dimensional CT imaging in pediatric calvarial pathologies. Diagn Interv Radiol. doi:10.5152/dir.2013.13140
Kapil Saigal RSW (2005) Use of three-dimensional computerized tomography reconstruction in complex facial trauma. Facial Plast Surg FPS 21(3):214–220. doi:10.1055/s-2005-922862
Fox LA, Vannier MW, West OC, Wilson AJ, Baran GA, Pilgram TK (1995) Diagnostic performance of CT, MPR and 3DCT imaging in maxillofacial trauma. Comput Med Imaging Graph Off J Comput Med Imaging Soc 19(5):385–395
Samii M, Tatagiba M (2002) Skull base trauma: diagnosis and management. Neurol Res 24(2):147–156. doi:10.1179/016164102101199693
Ringl H, Schernthaner RE, Schueller G et al (2010) The skull unfolded: a cranial CT visualization algorithm for fast and easy detection of skull fractures. Radiology 255(2):553–562. doi:10.1148/radiol.10091096
Sanchez T, Stewart D, Walvick M, Swischuk L (2010) Skull fracture vs. accessory sutures: how can we tell the difference? Emerg Radiol 17(5):413–418. doi:10.1007/s10140-010-0877-8
Wei SC, Ulmer S, Lev MH, Pomerantz SR, González RG, Henson JW (2010) Value of coronal reformations in the CT evaluation of acute head trauma. AJNR Am J Neuroradiol 31(2):334–339. doi:10.3174/ajnr.A1824
Sodickson A, Okanobo H, Ledbetter S (2011) Spiral head CT in the evaluation of acute intracranial pathology: a pictorial essay. Emerg Radiol 18(1):81–91. doi:10.1007/s10140-010-0914-7
Prabhu SP, Newton AW, Perez-Rossello JM, Kleinman PK (2013) Three-dimensional skull models as a problem-solving tool in suspected child abuse. Pediatr Radiol 43(5):575–581. doi:10.1007/s00247-012-2546-4
Viel G, Cecchetto G, Manara R, Cecchetto A, Montisci M (2011) Role of preoperative 3-dimensional computed tomography reconstruction in depressed skull fractures treated with craniectomy: a case report of forensic interest. j forensic med 32(2):172–175. doi:10.1097/PAF.0b013e318219c88c
Kim Y-I, Cheong J-W, Yoon SH (2012) Clinical comparison of the predictive value of the simple skull x-ray and 3 dimensional computed tomography for skull fractures of children. J Korean Neurosurg Soc 52(6):528–533. doi:10.3340/jkns.2012.52.6.528
Demant AW, Bangard C, Bovenschulte H, Skouras E, Anderson SE, Lackner KJ (2010) MDCT evaluation of injuries after tram accidents in pedestrians. Emerg Radiol 17(2):103–108. doi:10.1007/s10140-009-0844-4
Kuszyk BS, Heath DG, Bliss DF, Fishman EK (1996) Skeletal 3-D CT: advantages of volume rendering over surface rendering. Skelet Radiol 25(3):207–214
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dundamadappa, S.K., Thangasamy, S., Resteghini, N. et al. Skull fractures in pediatric patients on computerized tomogram: comparison between routing bone window images and 3D volume-rendered images. Emerg Radiol 22, 367–372 (2015). https://doi.org/10.1007/s10140-015-1300-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-015-1300-2