
Abstract
Background
The value of 3-D skull models in evaluation of young children with suspected child abuse is not known.
Objective
The purpose of this study was to assess the value of 3-D skull models as a problem-solving tool in children younger than 2 years.
Materials and methods
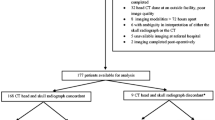
We performed a retrospective study on 73 children (ages 0–24 months) seen by a child protection team (CPT) who were undergoing head CT between August 2007 and July 2009.
Results
Of the 73 children, volume-rendered 3-D models were obtained in 26 (35.6%). Three-dimensional models changed initial CT interpretation in nine instances (34.6%). Findings thought to be fractures were confirmed as normal variants in four children. Depressed fractures were correctly shown to be ping-pong fractures in two cases. In one case, an uncertain finding was confirmed as a fracture, and an additional contralateral fracture was identified in one child. A fracture seen on skull radiographs but not seen on axial CT images was identified on the 3-D model in one case. Changes in interpretation led to modification in management in five children.
Conclusion
Use of 3-D skull models can be a problem-solving tool when there is discordance among the CT reading, subsequent radiographic investigations and clinical evaluation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
A head CT is the most common imaging study performed in an infant or young child following head trauma [1]. Depending on the initial interpretation, a referral to a multidisciplinary child protection team (CPT) might be made to assess the possibility of child abuse [2]. Problems can arise when there is a discrepancy between the initial CT head findings and subsequent skull radiographs obtained as part of the skeletal survey or the clinical assessment performed by a CPT [3]. With the widespread availability of multidetector CT, 3-D cranial models can be generated to supplement axial acquisitions. A smattering of reports describe examples of 3-D renderings of skull fractures and developmental variants in children following head trauma [4]. Recently, a study in pediatric cadaver skulls found that high-resolution CT scans with 3-D projections and conventional CT provide the most accurate fracture diagnosis, followed by radiographs [5]. Another recent study has documented the value of 3-D CT in evaluating the occipital suture and its variations [6]. There is however, little evidence in the literature regarding the clinical utility of 3-D models in the interpretation of CT scans performed in infants and toddlers following head trauma. This study assesses the value of 3-D models as a problem-solving tool in cases where there is discordance among the initial CT interpretation and subsequent radiographic and clinical assessments.
Materials and methods
Patients
This retrospective study was approved by the Institutional Review Board. A search of our institutional CPT database was carried out for all children ages 0–24 months who underwent axial head CT and were also seen by the CPT between August 2007 and July 2009. During this period, 3-D models were not part of the standard CT protocol and were constructed only at the request of the radiologist. We identified those cases where volume-rendered 3-D models were constructed, and evaluated the clinical history, initial reports of the CT (either a preliminary trainee report provided to the clinician or an attending neuroradiologist report before review by the mandated reporter) and a skull series performed as part of the skeletal survey. Subsequently, we documented those cases where there was a change from the initial to the final interpretation of the CT based on the 3-D images. The impact of this change of interpretation on the work-up by the CPT was analyzed. This included either immediate termination of the CPT investigation, a decision to take the investigation further or a decision to recall the child following discharge from the emergency department.
CT scanning technique and reformats
All children in our study population underwent a non-contrast CT in the contiguous axial mode with a gantry rotation time of 1–2 s, with gantry tilt parallel to the nasion and occipital condyle on a multidetector CT scanner. Scanners used were a 16-slice or 32-slice (GE Healthcare, Waukesha, WI) or a 64-slice (Siemens Healthcare, Erlangen, Germany). The exposure parameters were kVp 120 and mA 215, with 5-mm thick axial scans generated initially in all cases. Following this, submillimeter (0.625 mm on the 16-slice GE and 0.63 mm on the 64-slice Siemens) axial images were generated retrospectively from the axial data in a bone algorithm, and using this dataset, 3-mm thick coronal and sagittal reformats were performed and sent to a PACS workstation for review.
Three-dimensional models were generated at a Vitrea workstation (Vital Images version 4.2, Plymouth, MN) by the CT technologist and reviewed on the diagnostic PACS workstation. Images generated were displayed as orthographic views with 19 images rotating through 360° in the longitudinal and horizontal axes. Tissue classification and color assignment were based on the standard CT bone algorithm on the software used and were further tailored to minimize over-smoothing in the very young infant. In two cases, the volume-rendered 3-D model was generated on a workstation running Voxar 3D (Version 6.1; Toshiba Medical Visualization Systems, Edinburgh, UK) by the reporting neuroradiologist and viewed on the workstation in real time before saving the images to PACS.
The 3-D models were constructed when this was expressly requested by an interpreting radiologist at the time of initial report of the CT or subsequently during work-up of the case by the CPT/mandated reporter to clarify or resolve a discrepancy between skull radiography, head CT, clinical history or clinical findings.
For the purposes of this study, we considered the report by the interpreting attending neuroradiologist as the initial report. The final report pertains to the subsequent report generated at the time of review of the case by the mandated reporter along with the skeletal survey.
Skull radiographic technique
Frontal and lateral skull radiographs were obtained as part of the skeletal survey performed according to the departmental protocol based on American College of Radiology guidelines [7, 8]. Since the question of head injury was raised, the standard AP and single lateral view assessment was supplemented with the opposite lateral and a Townes projection. The peak voltage employed was 55–65 kVp and the tube current was adjusted accordingly for high-detail imaging. Images were acquired on a high-detail dual-side read computed radiography system (50 μm resolution) and reviewed on a PACS workstation.
Clinical information
The presenting histories as given by the child’s caregiver, physical examination findings and a report of the consultation by the child protection team clinician were recorded. The child protection team used accepted criteria to reach the diagnosis of non-accidental head trauma versus accidental injury. These included: (1) detailed history including confession of adult caretaker of intentional injury, (2) inconsistent or inadequate histories given by caretakers (the history did not explain nature and severity of the injuries) and (3) presence of unexplained injuries including fractures or intra-abdominal injuries. Specific note was made of cases where the initial assessment by the CPT was either changed or strengthened based on the reports of the radiographic studies (CT and/or the skeletal survey).
Results
A total of 73 children ages 0–24 months were referred to the CPT and seen by medical consultants at our institution between August 2007 and July 2009. Ages ranged from 13 days to 23 months, with a mean of 10.5 months (43 boys and 30 girls).
CT findings
Of the 73 children who underwent CT and were seen by the medical consultants of the CPT, volume-rendered 3-D images were performed in 26 (35.6%) cases. The initial CT interpretation was changed in 9 cases (34.6%) out of the 26 children in whom a 3-D model was generated. These cases are summarized in Table 1 and are illustrated in the accompanying figures.
Findings thought to be fractures on the axial CT images were confirmed as normal variants on the 3-D model in four children (cases 1–4; Figs. 1, 2 and 3). The 3-D model characterized depressed skull fractures as ping-pong fractures in two cases (cases 5 and 6; Fig. 4). In one case, the 3-D model helped confirm that a subtle finding reported as “suspicious for a fracture” on axial images was a definite fracture (case 7) and an additional contralateral fracture was detected on the 3-D model in one child (case 8). A fracture seen on skull radiographs but not seen on the axial CT images was identified clearly on the 3-D model in one child (case 9; Fig. 5).

Representative of case 1. CT head and skull radiograph in a young infant with scalp swelling over the left vertex. a Axial 0.75-mm CT image was interpreted as a calvarial fracture (arrow) with associated sutural diastasis. b Magnified view of the frontal skull radiograph demonstrates a well-defined curvilinear lucency (arrow) in the left high frontal region, thought to be a normal variant. c Three-dimensional model of the head CT confirms that the well-defined lucency (arrow) seen on the skull radiograph is a normal parasagittal fissure

Representative of case 2. a Axial CT and coronal reformat (b) raised suspicion for a fracture of the left parietal bone (arrows). c Three-dimensional model demonstrates the Wormian bone

Representative of case 3. a Axial CT in a 7-month-old boy shows a linear lucency (arrow) in the right frontal bone suspicious for a fracture but without overlying soft-tissue swelling. b A linear well-defined lucency on the skull radiograph at this site was more consistent with a prominent vascular marking (arrows). c Three-dimensional model shows a branching well-defined groove (arrows) in the left frontal bone, consistent with a prominent vascular marking

Representative of case 5. A 6-month-old infant presented after a fall from a bed. The child protection team consulted because the axial CT (a) reportedly demonstrated complex left parietal depressed skull fracture without overlying swelling (white arrow), possibly representing an old injury. b Three-dimensional model shows a ping-pong fracture, compatible with the history of a fall from a bed (black arrow)

Representative of case 9, an 8-month-old who fell backward from a sitting position and struck head on corner of furniture. a Initial report of the 5-mm axial CT commented on a right-side subgaleal hematoma (white arrow) but no underlying fracture was identified. No reformats were obtained at this time. b Skull radiograph obtained as part of a skeletal survey demonstrates a right parietal fracture (black arrow). c Coronal reformats and the 3-D model (d) obtained from the axial data following the skull radiograph clearly demonstrate the right parietal fracture (arrows)
Changes in interpretation of the CT based on the 3-D model led to modification in the work-up by the child protection team in 5/9 children (55.6%) as shown in the final column of Table 1.
Discussion
Volume-rendered 3-D models can be a useful supplement to axial imaging in young children with head trauma, especially in cases where there is a discrepancy between the initial CT report and subsequent clinical and radiographic investigations. The problem-solving capability of the 3-D model is most apparent in cases where axial CT images cannot differentiate between a subtle fracture and a normal variant and in cases where a fracture is not clearly visualized because it is oriented in the axial plane [9, 10]. Although sagittal or coronal reformats might provide this information, the findings are particularly well shown with a 3-D rendering. Bilateral skull fractures might be regarded as resulting from two separate sites of trauma and therefore inconsistent with a reported single contact injury. Demonstration of contiguity of biparietal fractures across the midline on a 3-D model can help determine whether the two fractures resulted from a single site of impact [11, 12].
The unique subset of ping-pong fractures in young infants, where the skull is deformed with a shallow depression, is more readily identified on the 3-D model, as found in two of the children in our series. These fractures have been attributed to short distance falls when the head of a young infant strikes a blunt object [13]. Differentiating this injury from other types of depressed fractures can optimize the clinical assessment by a multidisciplinary CPT. Many institutions rely on axial CT images for interpretation in these children, although the use of multiplanar (coronal and sagittal) reformats is becoming more readily accepted [14].
Another important benefit of 3-D models is that less experienced radiologists can identify anatomical variants better on the 3-D models compared to axial images or multiplanar coronal and sagittal 2-D reformats. Making this distinction between a fracture and a normal variant can change the management in some cases, as illustrated in cases 1, 2 and 3.
One of the facets of the study that merits elaboration is our routine use of the direct axial mode of scanning as opposed to helical acquisition in this population of infants [15]. The advantages of the helical mode of acquisition are increased scan speed, decreased need for sedation and fewer patient motion-related artifacts along with the retention of the ability to reconstruct in multiple planes with the creation of 3-D models from overlapping slices [16]. A key drawback of helical scanning is the need to repeat the entire scan if there is patient motion, doubling the radiation dose [17]. On the other hand, the longer scan times of axial scans increase the possibility of patient motion, but fewer scans need repeating in this instance. Also, as our scanners allowed initiation of individual images during axial acquisition, we did not find motion to be a significant problem in this retrospective study.
Furthermore, the helical images are not as sensitive as those obtained axially at detecting subtle differences in gray and white matter differentiation in brain parenchyma [18, 19]. This is most relevant in the young infant with non-myelinated white matter where the inherent difference between the normal gray and white matter is less than 10 HU (Hounsfield units). To balance image quality and patient dose, our policy has been to perform scans axially in children with possible traumatic head injury.
It is important to carefully consider the difference in radiation dose between axial and helical CT. Prior studies focused on dose comparisons between axial CT and helical CT have indicated that for a short scan length, the relative contribution of over-ranging is much larger and can result in higher doses in pediatric patients [20]. This is especially important in scanners not designed to spare non-imaged tissues at the end of the scan volume during helical scanning. This problem is less of an issue with the advent of newer helical systems with adaptive beam collimation [21]. We have therefore preferred axial scanning for children younger than 2 years of age.
Also, we would like to emphasize the need to scan using the smallest detector elements provided by the scanner in the z direction for both axial and helical scans. This allows reformatting of images in the coronal and sagittal planes and creation of 3-D models [22].
The results from our study suggest that the 3-D models generated from the axial data can be of diagnostic value while enabling reduction in radiation dose and maintaining sensitivity.
Limitations of the study include the relatively small study population, which precludes estimation of sensitivity and specificity of the 3-D models in detection of abnormalities following head trauma in infants. As we instituted the policy of creating 3-D models in all children younger than 2 years after obtaining the results from this retrospective review, we could not add to the patient population that we had already studied as our design could only include cases where the 3-D model was generated as a specific problem-solving tool at the time of initial case management. This study design prevented us from examining whether management would have changed in those cases where 3-D models were not performed at the time of the original case work-up. We did not compare the sensitivity and specificity of 2-D coronal and sagittal reformats with volume-rendered 3-D models. Studies in adults with head trauma have shown that multiplanar reformats can aid in interpretation of head CTs. This has been our experience as well and we have routinely included coronal and sagittal reformats in bone and soft-tissue windows as part of post-trauma head CT in young children. Also, we did not specifically evaluate the differences between the two main algorithms commonly used for 3-D reconstructions—namely, surface-shaded display and volume-rendering techniques [23, 24]. However, studies have shown that volume-rendering techniques are superior to surface-rendering techniques in evaluating skeletal injuries [25].
We cannot exclude entirely the presence of abuse in cases that were considered to be low risk. Finally, our retrospective method does not ensure that the CPT assessment was performed in a standardized fashion. However, use of stringent criteria by the CPT including presence of subdural hematoma, retinal hemorrhages and fractures (excluding classic metaphyseal lesions) for diagnosis minimized the possibility that abuse was present in cases considered to be low risk.
Conclusion
Our study provides evidence that 3-D models of axially acquired head CT data can be useful in problem-solving in young children with suspected non-accidental head injury.
Use of this technique can result in modification of the initial CT interpretation and this is of particular importance when the CT read it is not in accordance with subsequent skull radiographs or clinical evaluation. This approach should be considered especially in young infants to be routine practice as it could have a significant impact on assessments by institutional CPTs in the appropriate clinical setting.
References
Tung GA, Kumar M, Richardson RC et al (2006) Comparison of accidental and nonaccidental traumatic head injury in children on noncontrast computed tomography. Pediatrics 118:626–633
Foerster BR, Petrou M, Lin D et al (2009) Neuroimaging evaluation of non-accidental head trauma with correlation to clinical outcomes: a review of 57 cases. J Pediatr 154:573–577
Kemp AM, Butler A, Morris S et al (2006) Which radiological investigations should be performed to identify fractures in suspected child abuse? Clin Radiol 61:723–736
Medina LS (2000) Three-dimensional CT maximum intensity projections of the calvaria: a new approach for diagnosis of craniosynostosis and fractures. Am J Neuroradiol 21:1951–1954
Mulroy MH, Loyd AM, Frush DP et al (2012) Evaluation of pediatric skull fracture imaging techniques. Forensic Sci Int 214:167–172
Choudhary AK, Jha B, Boal DK et al (2010) Occipital sutures and its variations: the value of 3D-CT and how to differentiate it from fractures using 3D-CT? Surg Radiol Anat 32:807–816
Section of Radiology, American Academy of Pediatrics (2009) Diagnostic imaging of child abuse. Pediatrics 123:1430–1435
Perez-Rossello JM, Connolly SA, Newton AW et al (2010) Whole-body MRI in suspected infant abuse. Am J Roentgenol 195:744–750
Wei SC, Ulmer S, Lev MH et al (2010) Value of coronal reformations in the CT evaluation of acute head trauma. Am J Neuroradiol 31:334–339
Zacharia TT, Nguyen DT (2010) Subtle pathology detection with multidetector row coronal and sagittal CT reformations in acute head trauma. Emerg Radiol 17:97–102
Arnholz D, Hymel KP, Hay TC et al (1998) Bilateral pediatric skull fractures: accident or abuse? J Trauma 45:172–174
Kleinman PK, Barnes PD (1998) Diagnostic imaging of child abuse, 2nd edn. Mosby, St. Louis
Zia Z, Morris AM, Paw R (2007) Ping-pong fracture. Emerg Med J 24:731
Prabhu SP, Young-Poussaint T (2010) Pediatric central nervous system emergencies. Neuroimaging Clin N Am 20:663–683
White KS (1996) Invited article: helical/spiral CT scanning: a pediatric radiology perspective. Pediatr Radiol 26:5–14
Hu H (1999) Multi-slice helical CT: scan and reconstruction. Med Phys 26:5–18
Tzedakis A, Perisinakis K, Raissaki M et al (2006) The effect of z overscanning on radiation burden of pediatric patients undergoing head CT with multidetector scanners: a Monte Carlo study. Med Phys 33:2472–2478
Halpin SF (2004) Brain imaging using multislice CT: a personal perspective. Br J Radiol 77:S20–S26
Abdeen N, Chakraborty S, Nguyen T et al (2010) Comparison of image quality and lens dose in helical and sequentially acquired head CT. Clin Radiol 65:868–873
Schilham A, van der Molen AJ, Prokop M et al (2010) Overranging at multisection CT: an underestimated source of excess radiation exposure. Radiographics 30:1057–1067
Bushberg JT (2012) The essential physics of medical imaging, 3rd edn. Wolters Kluwer Health/Lippincott Williams & Wilkins, Philadelphia
Strauss KJ, Goske MJ, Kaste SC et al (2010) Image gently: ten steps you can take to optimize image quality and lower CT dose for pediatric patients. Am J Roentgenol 194:868–873
Philipp MO, Kubin K, Mang T et al (2003) Three-dimensional volume rendering of multidetector-row CT data: applicable for emergency radiology. Eur J Radiol 48:33–38
Fishman EK, Ney DR (1993) Advanced computer applications in radiology: clinical applications. Radiographics 13:463–475
Kuszyk BS, Heath DG, Bliss DF et al (1996) Skeletal 3-D CT: advantages of volume rendering over surface rendering. Skeletal Radiol 25:207–214
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Prabhu, S.P., Newton, A.W., Perez-Rossello, J.M. et al. Three-dimensional skull models as a problem-solving tool in suspected child abuse. Pediatr Radiol 43, 575–581 (2013). https://doi.org/10.1007/s00247-012-2546-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-012-2546-4