
Abstract
The aim of the present study was to determine clinical parameters for the use of Er,Cr:YSGG laser in the treatment of dentine hypersensitivity. Two antagonist areas were determined as control and experimental areas for irradiation in 90 premolar roots. Each surface was conditioned with 24% EDTA (sub-group 1) and 35% phosphoric acid (sub-group 2) and irradiated with the following settings: 1) Er:YAG, 60 mJ, 2 Hz, defocused; groups 2 to 9: irradiation with Er,Cr:YSGG laser, 20 Hz, Z6 tip, 0% of air and water: 2) Er,Cr:YSGG 0.25 W; 3) 0.5 W; 4) 0.75 W; 5) 1.0 W; 6) 1.25 W, 7) 1.50 W, 8) 2 W; 9) 2 W. After irradiation, samples were immersed in methylene blue solution and included in epoxy resin to obtain longitudinal cuts. The images were digitalized and analyzed by computer software. Although the samples irradiated with Er:YAG laser showed less microleakage, sub-group 1 showed differences between the groups, differing statistically from groups 3, 6, and 9. The results of sub-group 2 showed that the mean values of Er:YAG samples showed a negative trend, however, no differences were detected between the groups. For scanning electron microscopy analysis, dentine squares were obtained and prepared to evaluate the superficial morphology. Partial closure of dentinal tubules was observed after irradiation with Er:YAG and Er,Cr:YSGG laser in the 0.25 and 0.50 W protocols. As the energy densities rose, open dentinal tubules, carbonization and cracks were observed. It can be concluded that none of the parameters were capable of eliminating microleakage, however, clinical studies with Er:YAG and Er,Cr:YSGG lasers should be conducted with the lowest protocols in order to determine the most satisfactory setting for dentine hypersensitivity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Dentine hypersensitivity (DH) is a common complaint in adults and it is one of the most painful and chronic problems reported in dental offices. It is defined as a short and sharp pain arising from exposed dentine, in response to chemical, thermal, tactile, or osmotic stimuli, which cannot be explained as arising from other forms of old dental defects or pathologies [1–3].
Microscopically, the features that determine the different degrees of DH include the number, patency, and size of the open dentinal tubules. In sensitive teeth, the number of tubules per unit area is about eight times greater than the number found in non-sensitive teeth. In addition, tubular diameter is two times greater in sensitive teeth [4–6].
Considering that sensitive dentine is permeable, any decrease in dentinal permeability would reduce the movement of the fluid inside the tubules and consequently reduce the pain from dentine sensitivity. Consequently, various agents have been recommended to partially or completely occlude dentinal tubules. However, most of the treatments are either ineffective or last for a short period of time [7].
Since the development of the first ruby laser system, a variety of lasers have been used and research has focused on possible detrimental effects on pulp after irradiation. The use of a laser in DH has been investigated and the results have shown promising effects [8]. The Er:YAG laser in DH treatment is hypothesized as being highly effective in reducing the diameter of dentinal tubules under some specific conditions, with partial obliteration of dentinal tubules [8, 9].
However, few published data are available concerning the desensitizing effects of erbium lasers [10]. In vitro studies have shown that dentine permeability is decreased after Er:YAG laser irradiation and clinical trials have described the equipment as effective in decreasing pain [11–13]. With the advent of the Er,Cr:YSGG lasers, new possibilities of treatment for DH have been proposed.
As the most important factor in laser therapy is to have the correct parameter, the aim of this study was to analyze dentine permeability and the morphology of exposed dentine surfaces irradiated with Er:YAG and Er,Cr:YSGG lasers using different parameters.
Materials and methods
Sample preparation
After the research project was approved by the Research Ethics Committee of the University of São Paulo (Protocol 204/03), 144 premolars were selected and cleaned. Crowns were sectioned at the enamel–cement junction, using double-faced diamond discs (KG Sorensen Ind. e Com. Ltda), with water cooling at low speed.
A flow-type composite resin (Tetric Flow, Ivoclar/Vivadent, Shaan, Liechtenstein) was used to seal the root canal to prevent the dye solution from penetrating into it.
Manual root scaling was performed to remove the cementum layer and expose the dentine surface.
Two cervical windows with an area of 9 mm2 were made in each sample in opposite positions (mesial and distal surfaces). In one of the windows, a mark was made corresponding to the control group window (without irradiation). Due to the variation in dentinal tubule morphology from tooth to tooth, the choice was to use the same sample as experimental and control unit.
The specimens were impermeabilized with ethyl cyanoacrylate (Super Bonder®, Loctite) and two coats of colored cosmetic nail varnish, so that the entire area was covered, except for the experimental windows.
After this, to simulate a hypersensitive dentine surface, the windows received an application of 35% phosphoric acid (3M ESPE, St Louis, MN, USA) (sub-group A) and EDTA solution (Formula e Ação, São Paulo, SP, Brazil) (sub-group B), respectively.
Laser irradiation
Laser irradiation was performed in accordance with the safety protocol of the international standards. Two wavelengths, Er:YAG (2.94 μm) and Er,Cr:YSGG (2.78 μm) lasers, were used in this study.
For group 1, the Er:YAG laser (KaVo Key Laser 1243, Ulm, Germany) was used perpendicularly in scanning movements, defocused, 6 mm from the surface, with a repetition rate of 2 Hz, 60 mJ energy setting in the display, and a real energy output of 32.4 mJ (handpiece 2055, fiber 50/10 with transmission factor of 54%), and an energy density of 5.9 J/cm2. Four irradiations of 20 s each were performed, with a 1-min interval between them, with air cooling.
For groups 2 to 9, the Er,Cr:YSGG laser (Waterlase, Biolase Technology, Irvine, CA, USA) used has a fixed repetition rate of 20 Hz, pulse width of 140 to 200 μs. Irradiation was made perpendicular, 1 mm from the surface with the Z6 tip (600 μm diameter). Power settings varied from 0.25 to 2 W as shown in Table 1.
After irradiation, samples were immersed in 2% methylene blue dye solution (Fórmula e Ação, São Paulo, SP, Brazil) for 4 h. After the immersion period, samples were washed with tap water for 15 min and embedded in epoxy resin to perform the longitudinal cuts (Buehler ISOMET 100™, Buehler Ltd., IL, USA), sectioning the two opposite windows.
Specimens were analyzed with a Stereoscopic Lupe (Stemi SV11, Zeiss, NY, USA) to define which of the halves presented more leakage. Samples were then analyzed by an image program (Leica Qwin Colour). The percentage of dyed dentine surface in relation to the total dentine surface was found. The difference in percentage of dyed dentine surface between the control and the irradiated surfaces showed the decrease in dentine permeability in each sample.
Data were submitted to statistical analysis using a parametric test, due to normal distribution of samples. Analysis of variance with a significance level of 1% was performed and Tukey and Kruskal–Wallis test were used to observe differences between the groups.
Morphological analysis
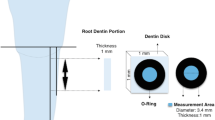
For the scanning electron microscopy analysis, 40 recently extracted human pre-molars were selected and cleaned. From each tooth, dentine samples measuring 3 × 3 mm were removed in the cervical region, using double-faced diamond discs (KG Sorensen, Barueri, SP, Brazil). Samples were randomly divided (n = 2) into the groups described for the dentine permeability analysis, and irradiation was performed according to the description given previously.
After this, samples were immersed in a 2.5% glutaraldehyde solution for 24 h to preserve biological tissues and were then chemically dehydrated in ascending grades of ethanol. To avoid specimen shrinkage during air drying, samples were immersed in 100% HMDS (Hexamethyldisilazane) for 30 min and left under a fume hood equipped with an exhaust system until it had completely evaporated.
Samples were mounted on aluminum stubs and gold sputtered (Baltec Sputtercoater, SCD 050, Germany). Analyses were performed by scanning electron microscopy (LEO 430i, Cambridge, England).
Results
As there was an internal control group in each specimen, the difference in percentage of dyed dentine surface between the control and irradiated surfaces was used. In sub-group 1, in which samples were conditioned with EDTA, it was observed that the Er:YAG laser (group 1) was the only group that showed a trend toward negative values. From groups 2 to 9, a trend toward increase in leakage could be noted (diagram 1).
From the analysis of variance, it was possible to observe differences between the groups. To verify the differences, Tukey’s test was used, and showed that group 1 (Er:YAG) differed statistically from groups 3, 6, and 9, which were irradiated with Er,Cr:YSGG laser.
In sub-group 2, in which samples were conditioned with 35% phosphoric acid, fewer negative values were observed but the mean of group 1 was close to zero. From group 6 to group 9, a higher mean could be noted and group 3 presented great variability. From the Kruskal–Wallis test, no statistical differences could be observed among the studied groups (p = 0.064) (diagram 2).
Figure 1 shows representative illustrations of dentine irradiated with all the different settings. Irradiation with the Er:YAG laser parameter and the lower parameters of Er,Cr:YSGG laser showed no visible alterations. The Er,Cr:YSGG laser protocols using over 0.75 W did show some degree of carbonization.

Representative illustrations of dentin irradiated with all settings. 1 Er:YAG, 60 mJ, 2 Hz, defocused mode; 2–9 irradiation with Er,Cr:YSGG laser, 20 Hz, Z6 tip, 0% of air and water: 2 Er,Cr:YSGG 0.25 W; 3 0.5 W; 4 0.75 W; 5 1.0 W; 6 1.25 W, 7 1.50 W, 8 2 W; 9 2 W
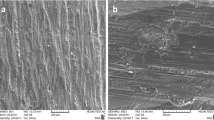
Morphological differences could be seen between the EDTA and phosphoric acid-etched surfaces. It could be noted that the 1-min application of EDTA was not enough to open the dentinal tubules to the extent that phosphoric acid did (Fig. 2).

Electron scanning micrographs of dentin treated with EDTA 24% and phosphoric acid 35% (12 kV, 500x)
Regarding the lasers, micrographs showed melted dentine when the Er:YAG laser was used, with dentinal tubules partially obliterated (Fig. 3). Er,Cr:YSGG laser irradiation with power settings of 0.25 and 0.5 W showed a partially obliterated dentine surface without the presence of cracks and carbonization. This pattern differs from that observed in surfaces with power settings of over 0.75 W. Open dentinal tubules, rupture of solidified tissue, carbonization, and crack formation can be observed (Figs. 4 and 5).

Representative micrographs of dentin irradiated with Er:YAG. EDTA samples (a 12 kV, 500x) and acid phosphoric (b 12 kV, 3,500x)

Representative micrographs of dentin conditioned with EDTA 24% and irradiated with Er,Cr:YSGG: a 0.25 W (500x), b 0.50 W (500x), c 0.75 W (500x), d 1 W (500x), e 1.25 W (500x), f 1.50 W (50x), g 1.75 W (50x), h 2 W (50x)

Representative micrographs of dentin conditioned with phosphoric acid 35% and irradiated with Er,Cr:YSGG: a 0.25 W, b 0.50 W, c 0.75 W, d 1 W, e 1.25 W, f 1.50 W, g 1.75 W, h 2 W (500x)
Discussion
Since hypersensitive teeth exhibit significantly wider dentine tubule diameters than those of non-sensitive teeth, it would appear that treatment focused on decreasing the radius of dentinal tubules is a prerequisite for effective desensitization [3, 14]. Most of the desensitizing procedures or agents attempt to inhibit painful stimuli either by sealing the dentinal tubules with coating mechanisms or by altering tubule contents through coagulation, protein precipitation, or the creation of insoluble calcium complexes. However, the desired long-lasting effect does not occur.
In the present study, to open the dentinal tubules widely, in order to simulate dentine hypersensitivity, EDTA solution was used. According to Fig. 2, the micrographs obtained by scanning electron microscopy showed that the 1-min application was not enough to completely open the dentinal tubules on the dentine surface. This affirmation is in agreement with the literature [15]. Therefore, the use of 35% phosphoric acid in another sub-group was proposed, and micrographs showed the hypersensitivity pattern with wide-open dentinal tubules, similar to the substrate observed in dentine hypersensitivity. Both solutions were considered in the study, as EDTA can represent a moderate category of DH, and the acid a severe form of it.
Since dentinal tubule blockage to decrease hydraulic conductance has been considered in the treatment of DH, investigators have logically proposed the use of treatments that would seal the dentinal tubules [14]. However, due to the lack of success in routine treatments, in the mid-1980s, the use of a laser to decrease the level of DH was proposed. In most of the cases, lasers such as Nd:YAG, CO2, and Er:YAG were used and a relative success was described [16–21].
Although the effects of Nd:YAG laser on DH is known, and have been described as the melting and re-crystallization of dentine, few data are available on the effects of erbium lasers on dentinal tubules and dentinal fluid flow.
The Er:YAG laser irradiation parameters used in the present study caused a reduction in permeability in the protocol used. Samples that were irradiated with Er:YAG laser showed lower levels of microleakage when conditioned with EDTA. The mean values of samples conditioned with phosphoric acid showed values close to zero. As the difference between the irradiation and control area was evaluated, this means that the irradiation window showed less leakage than the control area. The results are in agreement with the results in the literature. In a previous study, Aranha et al. [11] showed a reduction in permeability in 85% of the samples irradiated by Er:YAG laser.
The high absorption of erbium lasers by water and hydroxyapatite can cause ablation of the dentine surface and would open the dentinal tubules, as opposed to sealing the dentinal tubules [22, 23]. This is an ambiguous discussion about the mechanism of erbium lasers in DH. According to Schwarz et al. [13] and Birang et al. [24], it is supposed that lower power settings would result in an evaporation of the dentinal fluid and the smear layer, causing the decrease in dentine permeability, and consequently, a decrease in dentinal pain.
It should be considered that in the present study, the Er:YAG laser was used without cooling, but the energy settings used were lower than the ablation threshold of dental hard tissues. The results can be described as satisfactory when related to dentine permeability for both conditioning methods. However, an effective method to completely seal the dentinal tubules was also observed.
In the scanning electron microscopy analysis, some portions can be described as the melting process, however, with the lower settings used in this study, and when compared with the micrographs usually presented by the Nd:YAG laser in which the melting process is easily recognized, the alteration in the morphology after Er:YAG and Er,Cr:YSGG laser irradiation showed portions of recrystallization and portions of open dentinal tubules. Gholami et al. [25] showed that the Er,Cr:YSGG laser was able to melt peritubular dentine, occlude dentinal tubules partially or totally, and therefore reduce patients' hypersensitivity symptoms. In addition, Badran et al. [9] affirmed that Er:YAG irradiation seemed to be promising therapy for the clinical management of DH.
To evaluate the effects of Er:YAG and Nd:YAG lasers on radicular dentine permeability when using different substances as irrigating solutions, Brugnera et al. [12] used a protocol with higher energy density for Er:YAG laser and concluded that greater dentine permeability was observed with the Er:YAG laser. In the present study, protocols with higher power settings define the pattern of dentine surfaces with wide-open dentinal tubules.
The Er,Cr:YSGG laser used has a fixed repetition rate of 20 Hz, which is quite a concern in the treatment of DH. Similar to the Er:YAG laser, the power settings used were lower, however, the Er:YAG laser promoted less permeability and in some cases, the values were negative, meaning that the dye solution penetrated more into the irradiated window than into the control window, as previously explained. In Fig. 3 it can be clearly noted that with settings of above 0.75 W, spots of carbonization can be recognized and these are not desirable protocols for use in the treatment of DH.
Studies comparing the two types of equipment and parameters have not yet been conducted. Although the literature shows that dentine surfaces prepared by Er:YAG and Er,Cr:YSGG lasers are similar in micromorphology [26], speculation on the different forms of action of the two lasers are still discussed. The greater absorption of the OH− ions from hydroxyapatite by Er,Cr:YSGG laser could promote a different interaction between the laser and the dentine surface. Moreover, the higher and fixed repetition rate of 20 Hz could involve more leakage into the irradiated windows.
Once the parameters are well established, the potential for developing lasers for the treatment of dentine hypersensitivity can be fully explored and performed. Clinical studies following the protocols suggested by in vitro studies would be of great interest with regard to analysis of the relationship between dentinal tubule closure and reduction in permeability, observing whether there is correlation between the analgesic effect and the reduction in dentine permeability.
Conclusions
Within the limitations of an in vitro study, it can be concluded that:
-
1.
A decrease in dentine permeability could be observed; however, none of the parameters completely eliminated microleakage and reduced dentine permeability. The Er:YAG laser showed superior results to those of Er,Cr:YSGG laser in sealing the tubules.
-
2.
Morphologically, none of the types of equipment and parameters used were capable of sealing dentinal tubules completely.
References
Holland GR, Narhi MN, Addy M, Gangarosa I, Orchardson R (1997) Guidelines for the design and conduct of clinical trials on dentine hypersensitivity. J Clin Periodontol 24(11):808–813
West NX (2008) Dentine hypersensitivity: preventive and therapeutic approaches to treatment. Periodontol 2000(48):31–41
Addy M, Smith SR (2010) Dentine hypersensitivity: an overview on which to base tubule occlusion as a management concept. J Clin Dent 21(2):25–30
Rimondini L, Baroni C, Carrassi A (1995) Ultrastructure of hypersensitive and non-sensitive dentine. A study on replica models. J Clin Periodontol 22(12):899–902
Absi EG, Addy M, Adams D (1987) Dentine hypersensitivity. A study of the patency of dentineal tubules in sensitive and non-sensitive cervical dentine. J Clin Periodont 14(5):280–284
Yoshiyama M, Masada J, Ishida H (1989) Scanning electron microscopic characterization of sensitive vs. insensitive human radicular dentine. J Dent Res 68(11):1498–1502
Walters PA (2005) Dentineal hypersensitivity: a review. J Contemp Dent Pract 6(2):107–117
Kimura Y, Wilder-Smith P, Yonaga K, Matsumoto K (2000) Treatment of dentine hypersensitivity by lasers; a review. J Clin Periodontol 27(10):715–721
Badran Z, Boutigny H, Struillou X, Baroth S, Laboux O, Soueidan A (2011) Tooth desensitization with an Er:YAG laser: in vitro microscopical observation and a case report. Lasers Med Sci 26(1):139–142
de Paula EC, de Freitas PM, Esteves-Oliveira M, Aranha AC, Ramalho KM, Simões A, Bello-Silva MS, Tunér J (2010) Laser phototherapy in the treatment of periodontal disease. A review. Lasers Med Sci 25(6):781–792
Aranha AC, Domingues FB, Franco VO, Gutknecht N, Eduardo CP (2005) Effects of Er:YAG and Nd:YAG lasers on dentine permeability in root surfaces: a preliminary in vitro study. Photomed Laser Surg 23(5):504–508
Brugnera A Jr, Zanin F, Barbin EL, Spanó JC, Santana R, Pécora JD (2003) Effects of Er:YAG and Nd:YAG laser irradiation on radicular dentine permeability using different irrigating solutions. Lasers Surg Med 33(4):256–259
Schwarz F, Arweiler N, Georg T, Reich E (2002) Desensitizing effects of an Er:YAG laser on hypersensitive dentine. J Clin Periodontol 29(3):211–215
Gillam DG (1995) Mechanisms of stimulus transmission across dentine—a review. J West Soc Periodontol Period 43(2):53–65
Scelza MF, Pierro V, Scelza P, Pereira M (2004) Effect of three different time periods of irrigation with EDTA-T, EDTA, and citric acid on smear layer removal. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 98(4):499–503
Naylor F, Aranha AC, Eduardo Cde P, Arana-Chavez VE, Sobral MA (2006) Micromorphological analysis of dentineal structure after irradiation with Nd:YAG laser and immersion in acidic beverages. Photomed Laser Surg 24(6):745–752
Lan WH, Lee BS, Liu HC, Lin CP (2004) Morphologic study of Nd:YAG laser usage in treatment of dentineal hypersensitivity. J Endod 30(3):131–134
de Magalhães MF, Matson E, de Rossi W, Alves JB (2004) A morphological in vitro study of the effects of Nd:YAG laser on irradiated cervical dentine. Photomed Laser Surg 22(6):527–532
Ciaramicoli MT, Carvalho RC, Eduardo CP (2003) Treatment of cervical dentine hypersensitivity using neodymium: yttrium-aluminum-garnet laser. Clinical evaluation. Lasers Surg Med 33(5):358–362
Moritz A, Schoop U, Goharkhay K, Aoid M, Reichenbach P, Lothaller MA, Wernisch J, Sperr W (1998) Long-term effects of CO2 laser irradiation on treatment of hypersensitive dental necks: results of in vivo study. J Clin Laser Med Surg 16(4):211–215
Romano AC, Aranha AC, Lopes da Silveira B, Baldochi SL, Eduardo CD (2011) Evaluation of carbon dioxide laser irradiation associated with calcium hydroxide in the treatment of dentineal hypersensitivity. A preliminary study. Lasers Med Sci 26(1):35–42
Hibst R, Stock K, Gall R, Keller U (1996) Controlled tooth surface heating and sterilization by Er:YAG laser irradiation. SPIE 2922:119–127
Wigdor HA, Walsh JT, Featherstone JDB, Visuri SR, Fried D, Waldvogel JL (1995) Lasers in dentistry. Lasers Surg Med 16(2):103–133
Birang R, Poursamimi J, Gutknecht N, Lampert F, Mir M (2007) Comparative evaluation of the effects of Nd:YAG and Er:YAG laser in dentine hypersensitivity treatment. Lasers Med Sci 22(1):21–24
Gholami GA, Fekrazad R, Esmaiel-Nejad A, Kalhori KA (2011) An evaluation of the occluding effects of Er;Cr:YSGG, Nd:YAG, CO2 and diode lasers on dentineal tubules: a scanning electron microscope in vitro study. Photomed Laser Surg 29(2):115–121
Harashima T, Kinoshita J, Kimura Y, Brugnera A, Zanin F, Pecora JD, Matsumoto K (2005) Morphological comparative study on ablation of dental hard tissues at cavity preparation by Er:YAG and Er, Cr:YSGG lasers. Photomed Laser Surg 23(1):52–55
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Aranha, A.C.C., de Paula Eduardo, C. In vitro effects of Er,Cr:YSGG laser on dentine hypersensitivity. Dentine permeability and scanning electron microscopy analysis. Lasers Med Sci 27, 827–834 (2012). https://doi.org/10.1007/s10103-011-0986-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-011-0986-y