
Abstract
Attempts have been made to treat dentinal hypersensitivity by sealing exposed dentinal tubules, and the carbon dioxide (CO2) laser has been shown to have a sealing effect on dentinal surfaces. The purpose of this study was to analyze the morphological ultra-structure and temperature change after CO2 laser irradiation of dentin. Fourteen human third molars were selected and cleaned. An area was delimited, and the samples were randomly divided into seven groups: Group 1 (G1): control; G2, calcium hydroxide paste (CA) + CO2 laser (L) (0.5 W/63,69 W/cm2); G3, CA + L (1 W/125,38 W/cm2); G4, CA + L (1.5 W/191,08 W/cm2); G5, L (0.5 W); G6, L (1 W); G7, L (1.5 W). All irradiation was performed in unfocused mode. The electron micrographs were analyzed by three observers. For temperature analysis, a thermocouple was used. Data were subjected to statistical analysis. The Kruskal–Wallis non-parametric test showed statistical differences between the groups (P < 0.05). For the two by two comparisons, all groups treated with calcium hydroxide paste presented significantly higher mean scores. In the groups treated by CO2 laser only, fusion, re-crystallization, cracks and carbonization were observed. A change of 1 ± 5°C was noted in the temperature. Under the limitation of an in vitro study, and with the protocols used, we concluded that CO2 laser is safe to use for the establishment of partial fusion and re-solidification of the dentinal surface.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Dentinal hypersensitivity (DH) is a condition frequently encountered in dental clinics and is a relatively common problem in periodontal practice. In this condition, dentin is exposed to the oral environment due to the loss or removal of enamel or cement [1, 2]. It is known that the layer of cement in the cervical third is extremely thin and that the enamel is easily removed by the action of abrasive pastes, toothbrushes, periodontal curettes and even by the ingestion of certain types of food.
Exposure of dentinal tubules causes short and acute pain, characteristic of DH. The reported discomfort persists only while the stimulus is being applied [3–6].
There are several therapies available for DH, ranging from treatment at home to treatment in the consulting room. Unfortunately, treatment strategies for this problem are not so successful and have no long-term effects.
In an attempt to find new alternatives for treating patients with DH, several authors have studied the possibility of using laser, aimed at the obstruction of dentinal tubules by melting and re-crystallization of the dentin, and reducing the painful symptoms [7, 8].
The mechanism by which laser acts on DH is related to the type of laser used. Wakabayashi et al. [9] concluded that low intensity lasers might act directly on the pulp nerve terminals, causing analgesia by depressing the transmission of the nerve stimulation. On the other hand, high intensity lasers, such as neodymium:yttrium–aluminum–garnet (Nd:YAG), erbium:yttrium–aluminum–garnet (Er:YAG) and carbon dioxide (CO2), cause the occlusion of the dentinal tubules, contributing towards the elimination of dentinal pain [10]. However, the protocols must assure the safety of the procedure with regard to temperature increase and morphological alteration of the dentinal surfaces.
Based on these considerations, the objective of this study was to analyze the effects of CO2 laser with or without calcium hydroxide paste through a morphological and temperature evaluation of dentin surfaces after root scaling.
Materials and methods
Fourteen human third molars were selected. All teeth had been recently extracted due to orthodontic indications, with the patients’ consent, after approval by the Ethics Committee on Research of the local institution (report no. 89/03).
After extraction, the teeth were cleaned, washed well under running water, and then kept in distilled water to maintain the level of hydration.
Sample preparation
The vestibular face of each root was scraped to remove the layer of root cement and expose the dentin surface, using specific Gracey number 7/8 periodontal curettes in an apical–coronary direction.
After scraping, the crown was sectioned at the enamel–cement limit, with double-faced 911H steel disks under water cooling at low speed.
To determine the region used for irradiation, we delimited an area of 12 mm2 at the cervical portion of the root, with the aid of a millimeter periodontal probe.
Samples were randomly divided into seven groups and were subjected to different treatments (n = 2) (Table 1). The samples in group 1 did not receive any treatment and were considered as the control group. For groups 2, 3 and 4 a layer of calcium hydroxide paste (Fórmula e Ação, São Paulo, Brazil) was applied to the delimited area, diluted in a physiologic serum solution, with a carpule-type syringe and a long 27G needle.
Laser equipment
The equipment used was a continuous emission CO2 laser (Union Medical Engineering Co., CO2 laser system, UM L-30), wavelength 10.6 µm, emitting a guide light by a diode laser of 5 mW (emitting in red), at a distance of 30 mm from the dentinal surface in unfocused mode. The beam diameter was calculated in 0.5 mm.
During irradiation, the necessary safety regulations were followed, with the emphasis on the use of safety eye glasses for the operator and other persons directly involved in the irradiation. In addition to gauging the outlet power of the laser beam applied to the samples, we used a power meter device (Coherent, Newport, CA, USA).
Irradiation
After the surface had been covered with the prepared paste, the surface was irradiated with CO2 laser at a distance of 30 mm from the dentinal surface, in unfocused mode, with a sweeping movement in the mesio-distal and disto-mesial directions. For irradiation, the specimen was fixed in a utility wax plate and the hand piece containing the fiber was moved by the operator, simulating the procedure. The specimens were irradiated six times in 5 s bursts, with intervals of 10 s between them for cooling. Irradiation was performed with a continuous laser beam perpendicular to the dentin surface. Group 2 was irradiated with 0.5 W of power and power density of 63.69 W/cm2; group 2 was irradiated with CO2 laser at 1.0 W and power density (PD) of 125.38 W/cm2, and, in group 4, the specimens were irradiated with 1.5 W power and energy density of 191.08 W/cm2.
In groups 5, 6 and 7 the specimens were not treated with calcium hydroxide paste. The delimited surface received irradiation with CO2 laser at 0.5 W power (PD = 63.69 W/cm2), 1 W (PD = 125.38 W/cm2) and 1.5 W (PD = 191.08 W/cm2), respectively. Irradiation was performed in the same mode as in groups 2, 3 and 4.
Temperature measurement
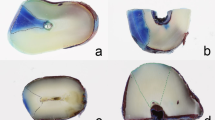
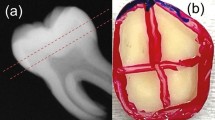
For the evaluation of temperature variation during irradiation, measurements were taken under the following conditions. A type K (copper–constantan) thermocouple with a diameter of 130 μm (Omega Engineering Inc., Stanford, CA, USA) was introduced into the root canal and adapted to the layer subjacent to the irradiated area, in two configurations: (a) by perforation of the pulp layer through the occlusal face and (b) by an opening in the cervical third of the dentinal crown, close to the irradiated area (Fig. 1).

Diagram of the configurations used for temperature measurement. a In configuration (a) the thermocouple is positioned near the opening in the cervical third of the dentinal crown. b In configuration (b) the thermocouple is positioned near the opening in the pulp layer, through the occlusal face
In both configurations a thermal paste was used to assure good heat contact between the tip of the thermocouple element and the internal wall of the sample (opposite the irradiated area). The samples were fixed in an acrylic support and immersed in a thermal bath, with the root portion immersed in water and kept at a temperature of 37 ± 1°C to simulate body conditions in the most adequate way.
To record the temperature we used a system composed of a lock-in amplifier (5RS10, Stanford Research System, USA) coupled to a computer. The system software allowed the thermocouple reading to be read and recorded. Afterwards, the data obtained were statistically analyzed with the MicroCalTM OriginTM, version 5.0 software.
Morphologic analysis
After irradiation and temperature analysis, the same samples that were used initially were put into an ultrasonic bath for 15 min to remove the impurities from the root dentin surface. Next, they were dehydrated in increasing alcohol concentrations of 50%, 70%, 80%, 90%, and 100%, for 30 min each. Then, the samples were covered with a layer of gold and once again kept in a desiccator until they were required for evaluation.
They were examined with a scanning electron microscope (Philips LX 300) at magnifications of ×500 and ×1,000, for data uniformity.
Assessment of micrographs
The most representative micrographs were analyzed by three observers, making use of a standard questionnaire that graded the images from 0 to 6 and contained the scores listed below:
-
Score 0. Completely open tubules without material deposition
-
Score 1. Closed tubules with fusion in less than 50% of the area without material deposition
-
Score 2. Closed tubules with fusion in over 50% of the area without material deposition
-
Score 3. Closed tubules with fusion in less than 50% of the area with material deposition
-
Score 4. Closed tubules in over 50% of the area with material deposition
-
Score 5. Completely closed tubules with material deposition
-
Score 6. Presence of a smear layer.
The results were grouped and subjected to statistical analysis.
Results
All data from the experimental groups were statistically analyzed.
We first used descriptive analysis, by means of tables and graphics, to find out if there were any differences between the groups treated by CO2 laser and calcium hydroxide and those treated by CO2 laser only. After that, we ran a test to find out whether the differences observed were significant or not (Table 2).
To analyze whether the differences between the six groups were significant, we used the Kruskal–Wallis non-parametric test and obtained a descriptive level of 0.003, from which it was concluded that the groups were different.
After concluding that there were differences between the groups, we did a second Kruskal–Wallis test, in which the groups were compared between each other, grouped two by two, to check where the differences occurred.
Differences in the three groups that used paste + laser, irrespective of power variation, were not significant. The same was true for the groups in which only laser was used. For the two by two comparisons between the groups treated with paste + laser and those treated by laser alone, there was a statistically significant difference. According to the mean score data, the paste + laser group presented more satisfactory results, as the mean score was 4, which represented closed tubules in over 50% of the area with mineral deposition. All the groups treated with paste presented significantly higher mean scores than all of the groups without paste.
Scanning electronic microscopy
An image of the controlled dentinal root surface without irradiation (group 1) can be seen in Fig. 2. Open dentinal tubules can be observed, without the presence of a smear layer, characteristic of scraped and planed root dentin. Only one specimen presented a smear layer, this material being identified by all the examiners.

Representative micrograph of the control group (×1,000). Note the opened dentinal tubules
In Fig. 3 the dentinal surface treated with CO2 laser (0.5 W) and calcium hydroxide paste (group 2) can be observed. Dispersed mineral deposits of irregular pattern on a heterogeneous surface without uniformity were noted.

Dentinal surfaces treated with CO2 laser (0.5 W of power) and calcium hydroxide. Note the presence of mineral deposits (×1,000)
Figure 4 shows the surfaces irradiated with CO2 laser associated with calcium hydroxide paste, with an irradiation parameter of 1.0 W (group 3). Sealing of the dentinal tubules, with deposition of material granules, can be seen. These granules appear to be aggregated on the substrate, presenting an irregular surface with a more homogeneous pattern, suggesting better laser–dentin interaction.

Dentinal surface treated with CO2 laser (1 W of power) and calcium hydroxide. Complete fusion of dentinal surfaces and deposits of granules can be seen (×1,000)
Figure 5 is an electron micrograph representative of group 4. Sealing of the dentinal tubules, with deposition of calcium hydroxide granules, can be observed. They are shown to be aggregated on the substrate, with an irregular surface and homogeneous pattern.

Electron micrograph representative of group 4, after CO2 laser irradiation with 1.5 W power in association with calcium hydroxide. Deposition of calcium hydroxide granules on the surface can be seen (×1,000)
In general, for the groups that were treated with calcium hydroxide and laser (groups 2, 3, 4), the observations of the evaluators were similar, even when the power used varied. In the evaluation of the groups treated with CO2 laser without the paste (groups 5, 6, 7), fusion, re-crystallization with the formation of fusion pores, cracks and carbonization were noted in all specimens.
The representative micrograph of group 5 can be seen in Fig. 6. Partial fusion with sealing of the dentinal tubules could be noted in over 50% of the irradiated area. The presence of fusion pores is also noted. For group 6 (Fig. 7), partial fusion and re-solidification, with the presence of fusion pores, may be noted, as there was thermal interaction between the CO2 laser and the dentinal surface.

Electron micrograph representative of group 5 after CO2 laser irradiation with 0.5 W power. Fusion and re-crystallization can be observed, and 50% of the dentinal tubules are blocked (×1,000)

Electron micrograph representative of group 6 after CO2 laser irradiation alone, with a power of 1 W. Fusion and re-solidification of dentin can be noted (×1,000)
The electron micrographs of the dentinal surfaces treated with CO2 laser at a power of 1.5 W (Fig. 8) shows partial fusion of the dentin and re-solidification of the structure; the presence of pores formed after fusion as well as cracks characteristic of treatment at high temperatures may also be noted

Electron micrograph of the dentinal surfaces treated with CO2 laser irradiation alone, with a power of 1.5 W. Carbonization and cracks can be observed (×1,000)
Temperature analysis
A change on the order of 5°C was noted for the measurement in configuration (a) and of 1°C for configuration (b) (Fig. 9). This effect was due to the thermal characteristics of the system being measured and the measuring process. The heat resulting from dentinal surface irradiation tends to dissipate into the medium, which, in this case, may be considered as being composed of the surface under irradiation and the water or air around it. Thus, the position of the thermocouple, its contact with the surface, and the medium that surrounded them were determining factors in the measured temperature curve.

Discussion
Dentinal hypersensitivity is one of the most frequent complaints in the daily clinic. The exposure of the dentinal tubules present throughout the full extent of the dentin is the main cause [1–3]. Although the literature presents numerous studies on the treatment of DH, the reports still show that there is difficulty in controlling this painful condition.
The desensitizing agents are classified according to their mechanism of action [11]. Calcium hydroxide acts as a tubular occlusion agent, whereas high intensity lasers act directly on the pulp nerve terminals, causing analgesia by depressing the transmission of the nerve stimulus, and also altering the dentinal surface, by tubular obliteration [7, 8, 10, 12].
Owing to the biological properties of calcium hydroxide, its use in clinical practice has its anti-microbial action as a reference, associated with the ability to favor the tissue repair process [13]. The interaction between the calcium hydroxide paste and the dentin, associated with the morphologic changes resulting from the thermal effect of laser on dentin, were hypothesized as a promise for the treatment of dentinal hypersensitivity.
The results of our study showed that fusion and re-solidification were observed to obliterate the dentinal tubules. The calcium hydroxide [Ca(OH)2] paste impregnated the dentinal structure, covering the entire area in which there were open dentinal tubules. This double blockage, by preventing the movement of the intratubular fluid and preventing the transmission of the nerve stimulus, may result in a reduction of the painful symptoms.
These results are in agreement with others that found morphologic changes in dentin after laser irradiation and reduction in dentinal sensitivity [8, 12, 14–16]. Thus, considering the favorable characteristics of the two techniques and emphasizing the problem of obtaining satisfactory clinical results, the association of techniques can be an advantage.
CO2 laser is easily absorbed by tissues with large water content, presenting superficial penetration. The wavelength of 10.6 μm also coincides with the absorption curve of hydroxyapatite, thus presenting satisfactory interaction. Also, enamel can be modified by pulsed CO2 laser to form a more acid-resistant substrate [17].
According to the results obtained in this study, CO2 laser interaction with root dentin may be noted, as well as the laser interaction with calcium hydroxide paste and root dentin. Morphologic changes were found on the dentinal surface, such as fusion and re-solidification, formation of pores after fusion, cracks, carbonization and also the presence of material granules on the dentinal surface. These observations are corroborated in related studies in the literature [7, 12, 14, 15, 18]. However, with regard to irradiation by CO2 laser and its association with calcium hydroxide paste, there is a lack of published studies.
It should be emphasized that this result was dependent on the power applied, as power densities of over 125.38 W/cm2 result in carbonization of the irradiated surface that has a blackened appearance, which is esthetically unfavorable and causes damage to the irradiated surface. The proposed treatment requires morphologic change but must not cause injuries to the tooth. Morphologically, parameters above 1.0 W power with continuous CO2 laser led to carbonization and cracks (Fig. 8), a characteristic result of high temperatures, making it unfeasible for clinical procedures. Similar results were related by Sasaki et al. in 2002 [18], who found carbonized cement and dentin on the surfaces irradiated with CO2 laser, and significantly deleterious alterations in the chemical composition of these structures were related.
Owing to the problem of temperature increase, and according to the requirements for an ideal treatment, we observed the temperature variation to check the safety with regard to the heat generated by the irradiation of the dentin in relation to the pulp chamber.
According to a study by Zach and Cohen [19], pulp tissue will bear a rise of up to 5°C without histological damage. Temperature increase in the pulp chamber is directly proportional to the amount of energy applied, associated with exposure time, which is of fundamental importance. In fact, a temperature increase proportional to the irradiation time and power applied in the two configurations that we used here could be noted. The use of 0.5 W power for 5 s assures that CO2 laser may safely be used, because, with heat generated in surrounding regions, temperature increases of fewer than 5°C were always observed. However, there was a difference in the temperature variation curve for different positionings of the thermocouple, shown for the maximum power used (1.5 W).
In the first case, a change on the order of 5°C was obtained, and, in the second case, one on the order of 1°C was found. These results show the need for the careful evaluation or comparison of the temperature measurements reported in various studies in the literature; that is, for identical irradiation parameters, diverse results may be obtained.
The temperature variation in the case of the top thermocouple was higher, since the wall between the thermocouple tip and the laser irradiation tip was certainly smaller. Also, the temperature variation detected by the thermocouple was more intense. This effect was due to the thermal characteristics of the system being measured and the measuring process. Heat resulting from the irradiation of the dentinal surface tends to dissipate into the medium, which, in this case, may be considered as being composed of the surface under irradiation and the water or air around it. Thus, the position of the thermocouple, its contact with the surface, and the medium that surrounds them, are determining factors in the measured temperature curve.
Also, the images suggested that laser irradiation could prolong the retention of the calcium hydroxide inside the dentinal tubules, by increasing the adhesion of the paste to the subjacent surface. Thus, it would be possible to maintain the desensitization effect for longer, allowing the calcium hydroxide to develop the property of inducing the formation of tertiary dentin [13]. Pashley [4] observed that, when Ca (OH)2 was used on dentin, there was an increase in the concentration of calcium ions, which came from the calcium hydroxide inside the tubules, and that this physical blockage promoted the reduction in dentinal permeability.
Based on these observations, the use of medications capable of obliterating tubules, together with laser therapy, go towards meeting the desire to fulfill the shortcomings in the techniques used up to now. However, the long-lasting nature and the stability of calcium hydroxide trapped in the dentin are much contested, due to the solubility of this material. In our study calcium hydroxide was shown to enhance tooth structure, but further studies should be carried out to test the efficacy and permanence of the trapped calcium hydroxide over time.
References
Yoshiyama M, Niori Y, Ozaki K, Uchida A, Ishikawa Y (1990) Transmission electron microscopic characterization of hypersensitive human dentin. J Dent Res 69:1293–1297
Yoshiyama M, Suge T, Kawasaki A, Ebisu S (1996) Morphological characterization of tubule-like structure in hypersensitive human radicular dentin. J Dent 24:57–63
Orchardson R, Gillam DG (2006) Managing dentin hypersensitivity. J Am Dent Assoc 137:990–998
Pashley DH (1986) Sensitivity of dentin to chemical stimuli. Endodont Dent Traumatol 2:130–137
Jacobsen PL, Bruce G (2001) Clinical dentin hypersensitivity: understanding the causes and prescribing a treatment. J Contemp Dent Pract 2:1–8
Bartold PM (2006) Dentinal hypersensitivity: a review. Aust Dent J 51:212–218
Tanji EY, Matsumoto K (1994) The comparative study of the morphological changes of dentin surface after Nd:YAG, CO2 and argon lasers irradiation. J Jpn Endod Assoc 15:14–20
Yonaga K, Kimura Y, Matsumoto K (1999) Treatment of cervical dentin hypersensitivity by various methods using pulsed Nd: YAG laser. J Clin Laser Med Surg 17:205–210
Wakabayashi H, Hamba M, Matsumoto K, Tachibana H (1993) Effect of irradiation by semiconductor laser on responses evoked in trigeminal caudal neurons by tooth pulp stimulation. Lasers Surg Med 13:605–619
Birang R, Poursamimi J, Gutknecht N, Lampert F, Mir M (2007) Comparative evaluation of the effects of Nd:YAG and Er:YAG laser in dentin hypersensitivity treatment. Lasers Med Sci 22:21–24
Ling TYY, Gillam DG (1996) The effectiveness of desensitizing agents for the treatment of cervical dentin sensitivity. A review. J West Soc Periodontol Periodontal Abstr 44:5–12
Zhang C, Matsumoto K, Kimura Y, Harashima T, Takeda F, Zhou H (1998) Effects of CO2 laser in treatment of cervical dentin hypersensitivity. J Endod 24:595–597
Olsson H, Petersson K, Rohlin M (2006) Formation of a hard tissue barrier after pulp cappings in humans. A systematic review. Int Endod J 39:429–442
Moritz A, Gutknecht N, Schoop U, Goharkhay K, Ebrahim D, Wernisch J, Sperr W (1996) The advantage of CO2-treated dental necks, in comparison with a standard method: results of an in vivo study. J Clin Laser Med Surg 14:27–32
Moritz A, Schoop U, Goharkhay K, Aoid M, Reichenbach P, Lothaller MA, Wernisch J, Sperr W (1998) Long-term effects of CO2 laser irradiation on treatment of hypersensitive dental necks: results of an in vivo study. J Clin Laser Med Surg 16:211–215
Misra V, Mehrotra J, Dixit J, Maitra SC (1999) Effects of a carbon dioxide laser on periodontally involved root surface. J Periodontol 70:1046–1052
Steiner-Oliveira C, Rodrigues LK, Soares LE, Martin AA, Zezell DM, Nobre-dos-Santos M (2006) Chemical, morphological and thermal effects of 10.6-microm CO2 laser on the inhibition of enamel demineralization. Dent Mater J 25:455–462
Sasaki KM, Aoki A, Masuno H, Ichinose S, Yamada S, Ishikawa I (2002) Compositional analysis of root cementum and dentin after Er:YAG laser irradiation compared with CO2 laser and intact roots using Fourier transformed infrared spectroscopy. J Periodont Res 5:50–59
Zach I, Cohen G (1965) Pulp response to externally applied heat. Oral Surg Oral Med Oral Pathol 19:515–530
Grossman LI (1935) A systematic method for the treatment of hypersensitive dentin. J Am Dent Assoc 22:592–602
Pashley E, Horner H, Liu M, Kim S, Pashley D (1992) The effects of CO2 laser energy on dentin permeability. J Dent Res 71:162
Luomanen M, Hemmerlé J, Voege CJ, Rauhamaa R, Meurman JH (1998) Transformation of hydroxyapatite to fluorapatite with CO2 laser irradiation. Proceedings of the 6th International Congress on Lasers in Dentistry. International Society for Lasers In Dentistry, Maui, Hawaii, pp 72–73
Lan WH, Chen KW, Jeng JH, Lin CP, Lin SK (2000) A comparison of the morphological changes after Nd:YAG and CO2 laser irradiation of dentin surfaces. J Endod 26:450
Acknowledgements
The authors wish to express their gratitude to the Special Laboratory of Lasers in Dentistry (LELO) at the University of São Paulo, Brazil. They thank the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) for financial support, the Mestrado Profissionalizante de Lasers em Odontologia (MPLO; Professional Master’s Course in Lasers in Dentistry) and Fundação para o Desenvolvimento Científico e Tecnológico da Odontologia (FUNDECTO; Foundation for the Scientific and Technological Development of Dentistry) for the use of the CO2 laser.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Romano, A.C.C.C., Aranha, A.C.C., Lopes da Silveira, B. et al. Evaluation of carbon dioxide laser irradiation associated with calcium hydroxide in the treatment of dentinal hypersensitivity. A preliminary study. Lasers Med Sci 26, 35–42 (2011). https://doi.org/10.1007/s10103-009-0746-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-009-0746-4