
Abstract
Hereditary spastic paraplegias (HSPs) are a group of neurodegenerative disorders which involve the corticospinal tracts and present with distinct spasticity and weakness of the lower extremities. The estimated prevalence of HSP is around 1.8/100,000 cases for both autosomal dominant and autosomal recessive types. Classification of HSP is based on inheritance pattern, clinical phenotype, and molecular pathophysiological mechanisms. The most common neuropathological sign is the axonal degeneration involving the lateral corticospinal tracts in both the cervical and thoracic spinal cord. The target of this review article is to provide a comprehensive overview of the HSP classification, neuropathology, and differential diagnosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hereditary spastic paraplegias (HSPs) are a group of neurodegenerative disorders which involve the corticospinal tracts and present with distinct spasticity and weakness of the lower extremities [1, 2]. HSPs are inherited in an autosomal dominant (AD), autosomal recessive (AR), X-linked recessive (XLR), and mitochondrial inheritance manner with > 80 published loci or genes [2, 3].
Clinically HSPs are classified into a pure form and a complex form. Pure forms present with slowly progressive lower extremity weakness and spasticity, corticospinal tract signs, disturbance in vibration sense and proprioception, and a variable hypertonic urinary disturbance. Complex HSP form has leg spasticity and other complications like ataxia, a thin corpus callosum, extrapyramidal signs, chorioretinal dystrophy, peripheral neuropathy, and mental retardation. Complex forms of HSP most often present with AR inheritance rather than AD form [1, 2].
Historical perspective
Neurologist Ernst Adolf von Strumpell, in 1880, published the first case report of patients with HSP [4]. In 1886, Strumpell also described the pathological characteristics of HSP [5]. Maurice Lorrain in 1888 published the comprehensive clinical and anatomical study of the HSPs. HSP is also known as Strumpell-Lorrain disease [6].
Schwarz in 1952 published a detailed review on pathological characteristics of HSP and also established the fact that initially lesions are restricted to the spinal cord particularly affecting the corticospinal and posterior tracts, which differentiates the HSP from other diseases like cerebellar ataxias and motor neuron disorders [7].
Anita Harding in 1981 published the investigational study of pure HSP families; it was also reported from this study that the pure subtypes of HSPs are most commonly inherited through AD way [8]. Harding also confirmed that spasticity is the main cause of disability and not weakness, which also differentiates the HSP from other myelopathies. In 1983, Harding introduced the classification of HSP into pure and complicated forms. Along with spastic paraparesis, other neurological symptoms like vibration and proprioception deficits, sphincter dysfunction, and a slight distal amyotrophy are also reported in the pure form of HSP [6].
Schady et al., in 1991, reported the neurophysiological findings through transcranial magnetic stimulation by central motor conduction studies in HSP patients [8]. Jouet et al., in 1994, described that the three disorders X-linked paraplegia, X-linked hydrocephalus, and MASA syndrome (mental retardation, aphasia, shuffling gait, and adducted thumbs) are the allelic conditions which occurred due to the mutations in the gene for L1CAM (neuronal cell adhesion molecule) or SPG1 (spastic paraplegia gene) [9]. Casari et al., in 1998, discovered the first gene for autosomal recessive HSP, while cloning the HSP-SPG7 gene. SPG7 gene encodes paraplegin protein which is found in mitochondria and ragged red muscle fibers [10]. Hazan et al., in 1999, cloned the SPG4 gene, which responds to 60% of cases with AD inherited HSP [11].
In 2006, the German network for HSP developed a spastic paraplegia rating scale to quantify the clinical disease progression [10]. In 2014, Novarino discovered up to 18 new HSP-related genes. Currently, > 80 different loci along with > 50 genes related to HSP are discovered. Historical timeline of HSP clinical research over the last century is shown below in Table 1 [6, 10].
Epidemiology
There are limited studies of HSP and its prevalence rate varies based on the geographic location, patient’s inclusion criteria, classification, and diagnosis. Worldwide, the estimated prevalence of HSP is around 1.8/100,000 cases for both AD and AR types. Few other studies suggested that the prevalence could range from 4.3 to 9.8/100,000 [12].
In Europe, there is an estimate of 3–10 HSP patients for 100,000 individuals. In Japan, it is estimated that there are 0.2 cases for 100,000 individuals [2]. Prevalence of AD-HSP is about 0.5 to 5.5/100,000 and for AR-HSP, it ranges from 0.0 to 5.3/100,000 population, with pooled average of 1.8/100,000 [13].
Classification
Classification of HSP is based on inheritance pattern, clinical phenotype, and other pathophysiological molecular mechanism. Classifications of HSP and its main subtypes are shown below in Table 2 [12].
Pure form of HSP presents with pyramidal signs like quadriparesis or paraparesis, brisk tendon reflexes, extensor plantar response, and spasticity along with deep sensory loss and sphincter disturbances [14, 15].
Complex or complicated form of HSP is characterized with both neurological and non-neurological signs. Neurological signs include the following [14, 16]:
-
Cerebellar dysfunctions like tremor, ataxia, and nystagmus
-
Cognitive impairment which includes dementia, intellectual disability, and mental retardation
-
Epilepsy
-
Axonal or demyelinating peripheral neuropathy involving dysautonomia and significant sensory disturbances
-
Myopathic characteristics include ptosis and opthalmoparesis (chronic progressive external ophthalmoplegia-like phenotype)
-
Psychiatric disturbances
-
Extrapyramidal features like chorea, parkinsonism, and dystonia
-
Brain and spine MRI abnormalities of distinct genetic subtypes are hypomyelination, leukodystrophy, thin corpus callosum, hydrocephalus, mild white matter changes, brain iron accumulation, cerebellar atrophy, and spinal cord atrophy
Non-neurological symptoms of complicated HSP include the following [15, 17]:
-
Ophthalmological abnormalities like optic atrophy, cataracts, optic neuropathy, macular degeneration, and retinitis pigmentosa
-
Dysmorphic features like macrocephaly, microcephaly, short stature, facial dysmorphisms, and other complex deformative syndromes
-
Orthopedic anomalies include scoliosis, hip dislocation, and various foot deformities
Based on inheritance pattern, HSP is inherited through AD, AR, XLR, and maternal pattern trait disorders. AD forms of HSP are less common than the AR forms; pure phenotypic forms are significantly seen in AD-HSP form. AR inheritance is the most frequently seen HSP form and is commonly seen in consanguineous families. XLR inheritance is seen in isolated cases and has five genetic subtypes known so far. Mitochondrial maternal inheritance is so sporadic with almost all the cases having a complex HSP phenotype; numerous signs and symptoms are usually seen which point towards a mitochondrial disorder [12, 17].
Although various pathophysiological mechanisms are involved in the development of HSP, it is classified based on the intracellular mechanisms involved in the pathophysiology. Molecular mechanisms which are commonly involved are mitochondrial dysfunction, axonal transport, membrane trafficking and organelle shaping, myelination abnormalities, and lipid metabolism disturbances [12, 15].
Neuropathology
Postmortem studies in HSP patients most commonly showed degeneration of axons involving the lateral corticospinal tracts with maximum severity in the thoracic portion of the spinal cord distal ends and relatively with little severity in the cervical portion of the spinal cord [14, 18]. Axonal degeneration in fasciculus gracilis fibers are typically found and are most significant in the cervical portion of the spinal cord; demyelination of these fibers is correlated with the degree of axon degeneration instead of suggesting a disease of primary demyelinative cause [14].
Axonal degeneration in the spinal cord causes mild to distinct atrophy in both cervical and thoracic segments [19]. In few cases, corticospinal tract degeneration stretches rostrally into the internal capsule, cerebral peduncles, pons, and medulla; reduced amount of pyramidal neurons (“Betz cells”) was also found in some specimens [14, 20].
HSP showed distinct susceptibility towards the long, sensory and motor axons of the CNS and depicts primary axonopathy. HSP expands beyond the CNS and causes peripheral neuropathy as a common symptom in many subtypes of HSP [14, 21]. HSP also involves not so long neurons, particularly seen in the neurons of the cerebellum, basal ganglia, anterior horn cells, and Clarke’s column (SPG4 subtype) [22].
Myelin abnormalities are frequently seen in HSP, specifically because of the genetic mutations in the neurons. Postmortem of a SPG2 HSP showed moderate cerebral atrophy, diffuse pallor of CNS myelin (corticospinal tract), and severe axonal degeneration of the corticospinal tract [23].
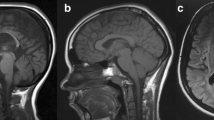
Few HSP abnormalities might be developmental instead of degenerative causes. Diameter of the spinal cord was relatively smaller in HSP subjects, which might be due to developmental disturbance in the spinal canal because of mutated induction in the development of the spinal cord [24]. Thin corpus callosum was believed to be an abnormality in development; however, Franca et al. have shown progressive thinning of the corpus callosum on serial brain MRI scans [25].
Genetics
HSP is inherited through AD, AR, XLR, and maternal pattern trait disorders [12]. HSP subtypes, inheritance mode, their gene encoded protein functions, and distinct clinical features are shown below in Table 3 [12, 26].

SPG4
SPG4 is inherited in an AD pattern and comprises 45% of pure HSP form. Mutations in the SPAST gene, which encode spastin, which is an ATPase-microtubule-severing protein family member engaged in intracellular motility, proteolysis, membrane trafficking, organelle biogenesis, endosomal tabulation, and fission and protein folding. Common presentation includes spastic paraparesis, sphincter disturbances, mild spastic dysarthria, and pes cavus; atypical symptoms include head tremor, nystagmus, depression, mental retardation, behavioral disturbances, psychosis, and cognitive decline with executive dysfunction; isolated symptoms are bulbar dysfunction, lower motor neuron syndrome, and restless leg syndrome [12, 14, 27].
SPG11
SPG11 is inherited in an AR pattern, which constitutes about 40% of AR-HSP form. Mutations in SPG11 gene encode spatacsin protein which causes intracellular trafficking, neuronal axonal growth, and function. Typical presentation is of slowly progressive spastic paraparesis, sphincter disturbances, cerebellar ataxia, parkinsonism, cognitive decline, mental retardation with learning disability, pes cavus, neuropathy, dysphagia, and pigmented macular degeneration leading to loss of visual acuity. Typical “ears-of-the-lynx” sign is seen on neuroimaging due to thin corpus callosum, symmetric periventricular white matter changes, cortical atrophy, and mild ventricular dilatation [17, 28].
Clinical features
Main clinical feature of HSP is slowly, progressive spastic paraparesis which develops as a gait disturbance. Delayed motor milestones are seen in patients with early-onset HSP (childhood). Brisk jaw jerk and asymptomatic upper limb hyperreflexia without spasticity are commonly seen. Other neurological symptoms commonly seen in more than 50% of the cases are ataxia, cognitive impairment, neuropathy, seizures, and dysarthria [3, 29].
Vibration sensation impairment is usually seen in a few cases due to dorsal column degeneration and other sensory systems are seldom involved [3]. Urinary symptoms due to detrusor sphincter dyssynergia or instability are commonly seen in the late stages of the disease [30]. HSP subtypes and their typical clinical features are shown in Table 3 [12, 26].
Diagnosis
HSP molecular diagnosis depends mainly on distinguishing the pathogenic mutations in the SPG genes [31]. Clinical diagnosis of HSP depends on the existence of spastic paraparesis along with other neurological and systemic presentations with or without family history [12]. A detailed family and developmental history of the patient plays a key role in the diagnosis and an acute or subacute presentation points towards an acquired form of HSP [31].

Patients usually present with slowly, progressive leg stiffness, abnormal gait, or gait instability, but maintain muscle power in spite of high tone in the lower limbs. Age of presentation varies from the first year of age with slowed motor milestones to delayed onset of pure HSP [17].
Neuroimaging including magnetic resonance imaging (MRI) of the brain and spinal cord can help in differentiating the SPG types. MRI of the spinal cord can be normal or might show thinning in a large number of SPG types [31, 32]. The “ears of the lynx” sign shows the distinct pattern of hyperintensities at the anterior forceps of the corpus callosum, which is commonly seen in SPG11 and SPG15 [33].
Neurophysiological studies include central motor conduction times (CMCTs), somatosensory-evoked potentials (SSEPs), electromyography (EMG), and nerve conduction studies (NCS). Although abnormal neurophysiological tests are common in HSP, they are not specific to the subtypes of HSP. Mononeuropathy like carpel tunnel syndrome and multifocal compression neuropathy is also seen in some isolated cases of HSP [31].
Genetic testing with next-generation sequencing-based gene panels is being extensively used in the diagnosis of HSP. These panels screen the exons of a vast variety of genes causing HSP; however, they do not detect triplet repeat disorders, mutations in deep intronic or promoter regions, and copy number variants like large duplications or deletions and exon deletions. One should be vigilant while diagnosing HSP, as monogenic diseases which present with lower limb spasticity without abnormalities on spinal cord MRIs are not defined in the SPG classification [31, 34].
Differential diagnosis
The differential diagnosis of HSP is expansive and multiple complementary test panels should be performed to rule out various inherited and acquired etiologies. The main differential diagnoses of HSP are shown below in Table 4 [12].
Various diagnostic tests which are used in differentiating HSP from other diseases are neuroimaging studies of the brain, cervical and thoracic spinal cord MRI, lumbar puncture with CSF analysis, neurophysiological tests, complete ophthalmologic examination, and full metabolic screening for inherited neurometabolic disorders [12, 14, 35]. In some unique isolated cases, further investigations are required to establish the diagnosis of HSP, which include very long chain fatty acid (VLCFA) analysis in plasma, serum vitamin E and cobalamin, plasma lipoprotein and amino acid profiles, serum copper, ceruloplasmin analysis, human immunodeficiency virus (HIV), human T cell leukemia virus type I (HTLV-I), and serological tests for Treponema pallidum [12, 14, 20].
As HSP is a heterogeneous disease, genetic testing became a main component in the clinical assessment and diagnosis. Genetic testing panels along with newer techniques in genetic sequencing (whole-exome) are having a considerable effect in both pure and complicated forms of HSP [12].
Treatment
Current treatment
Oral antispasmodics comprising of baclofen and tizanidine have demonstrated benefit in HSP patients [31]. In cases of severe spasticity, intrathecal baclofen is effective in decreasing the tone, pain, and disability; in its usage in the earlier stages of wheelchair-requiring patients, it showed an improvement in gait [36]. Dalfampridine (4-aminopyridine) showed some advantage in a small group of HSP and large studies are needed to establish its role [37].
Botulinum toxin (Botox) injections are efficacious in selective problematic muscle groups alongside the hip, knee, and ankle. Both stretching exercises and injections into calf decrease muscle tone, and enhance gait velocity while preserving balance and strength [38]. Oxybutynin helps in decreasing urinary urgency after ruling out urinary infection and establishing there is no marked increase in post-micturition residual volume of urine [31].
Physical therapy along with an exercise program by neurophysiotherapists is recommended to build up and maintain the lower extremity strength, to improve the range of motion, and to enhance cardiovascular conditioning. Both ankle foot orthotics and peroneal nerve stimulation transcutaneously reduce the toe dragging [14].
Genetic testing and counseling help the patients and families in understanding the disease and risk of transmission to the next generations. Clinicians must be vigilant while providing counseling and prognosis as most of the HSP genetic types of complete phenotypic spectrum and genetic penetrance are unfamiliar. Caution is necessary while counseling about SPG7, as in a minority of cases it can cause an AD form of HSP, in addition to the more frequent recessive form [14].
Gene therapy and future directions
Although genotype-targeted therapy has made marked advances in neurological diseases like spinal muscular atrophy and Huntington’s disease, HSP has not seen much progress because of genetic heterogeneity, rare form of genetic subtypes, mechanistic diversity, and a slow clinical disease progression [31].
In HSP-SPG4, microtubule severing causes partial loss of function, which might be corrected with gene therapy. Recent study showed that the human-induced plutipotent stem cells from a patient with spastin nonsense mutation with M1 or M87 isoform expressions redevelop the neurite numbers, length, branching, and reducing of the neuronal swelling [39].
SPG5 HSP is autosomal recessive and caused by the mutation in CYP7B1 gene encoding oxysterol-7α-hydroxylase which causes cholesterol degradation to primary bile acids and thus accumulating neurotoxic oxysterols. Management usually involves cholesterol-lowering drugs like atorvastatin which are used in reducing the levels of 27-hydroxycholesterol and chenodeoxycholic acid decreases the abnormal bile acid levels in SPG5 patients. More research studies are needed to establish the benefits of the combination therapies [31].
Paraplegin plays a key role in fine tuning the fast opening of the mitochondrial permeability transition pore, which can be pharmacologically modulated [31]. Study conducted by Pirozzi et al. showed that paraplegin delivery through the intramuscular route stops the neuropathology progression and also saves the peripheral nerve mitochondrial morphology [40].
Development of gene therapy for common recessive forms like SPG11, SPG15, and SPG7 offers vast possibilities for targeted gene editing or replacement. There is a need for all the international research groups to come together and get benefitted from the large clinical trials to achieve progress in gene therapy and other therapeutic areas [31].
References
Chrestian N, Dupré N, Gan-Or Z, Szuto A, Chen S, Venkitachalam A et al (2017) Clinical and genetic study of hereditary spastic paraplegia in Canada. 3(1):e122
Koh K, Ishiura H, Tsuji S, Takiyama Y (2018) JASPAC: Japan Spastic Paraplegia Research Consortium. Brain Sci 8(8):153
Schüle R, Wiethoff S, Martus P, Karle KN, Otto S, Klebe S et al (2016) Hereditary spastic paraplegia: clinicogenetic lessons from 608 patients. 79(4):646–658
Strümpell A (1880) Beiträge zur Pathologie des Rückenmarks. Archiv für Psychiatrie und Nervenkrankheiten 10(3):676–717
Strümpell A (1886) Ueber eine bestimmte Form der primären combinirten Systemerkrankung des Rückenmarks. Archiv für Psychiatrie und Nervenkrankheiten 17(1):217–238
Faber I, Pereira ER, Martinez AR, França M Jr, Teive HAG (2017) Hereditary spastic paraplegia from 1880 to 2017: an historical review. Arq Neuropsiquiatr 75(11):813–818
Schwarz GA (1952) Hereditary (familial) spastic paraplegia. JAAoN, Psychiatry 68(5):655–82
Schady W, Dick J, Sheard A, Crampton S (1991) Central motor conduction studies in hereditary spastic paraplegia. J Neurol Neurosurg Psychiatry 54(9):775–779
Jouet M, Rosenthal A, Armstrong G, MacFarlane J, Stevenson R, Paterson J et al (1994) X–linked spastic paraplegia (SPG1), MASA syndrome and X–linked hydrocephalus result from mutations in the L1 gene. 7(3):402–407
Casari G, De Fusco M, Ciarmatori S, Zeviani M, Mora M, Fernandez P et al (1998) Spastic paraplegia and OXPHOS impairment caused by mutations in paraplegin, a nuclear-encoded mitochondrial metalloprotease. 93(6):973–983
Hazan J, Fonknechten N, Mavel D, Paternotte C, Samson D, Artiguenave F et al (1999) Spastin, a new AAA protein, is altered in the most frequent form of autosomal dominant spastic paraplegia. 23(3):296–303
de Souza PVS, de Rezende Pinto WBV, de Rezende Batistella GN, Bortholin T, Oliveira ASB (2017) Hereditary spastic paraplegia: clinical and genetic hallmarks. Cerebellum 16(2):525–551
Ruano L, Melo C, Silva MC, Coutinho P (2014) The global epidemiology of hereditary ataxia and spastic paraplegia: a systematic review of prevalence studies. Neuroepidemiology. 42(3):174–183
Fink JK (2013) Hereditary spastic paraplegia: clinico-pathologic features and emerging molecular mechanisms. Acta Neuropathol 126(3):307–328
Giudice TL, Lombardi F, Santorelli FM, Kawarai T, Orlacchio A (2014) Hereditary spastic paraplegia: clinical-genetic characteristics and evolving molecular mechanisms. Exp Neurol 261:518–539
Novarino G, Fenstermaker AG, Zaki MS, Hofree M, Silhavy JL, Heiberg AD et al (2014) Exome sequencing links corticospinal motor neuron disease to common neurodegenerative disorders. 343(6170):506–511
Klebe S, Stevanin G, Depienne C (2015) Clinical and genetic heterogeneity in hereditary spastic paraplegias: from SPG1 to SPG72 and still counting. Rev Neurol (Paris) 171(6–7):505–530
Buge A, Escourolle R, Rancurel G, Gray F, Pertuiset BJRn (1979) Strümpell Lorrain’s familial spasmodic paraplegia. An anatomical and clinical review and report on a new case (author’s transl) 135(4):329–37
Hedera P, Eldevik O, Maly P, Rainier S, Fink J (2005) Spinal cord magnetic resonance imaging in autosomal dominant hereditary spastic paraplegia. Neuroradiology 47(10):730–734
Salinas S, Proukakis C, Crosby A, Warner TT (2008) Hereditary spastic paraplegia: clinical features and pathogenetic mechanisms. Lancet Neurol 7(12):1127–1138
Ivanova N, Claeys KG, Deconinck T, Litvinenko I, Jordanova A, Auer-Grumbach M et al (2007) Hereditary spastic paraplegia 3A associated with axonal neuropathy. 64(5):706–713
White K, Ince P, Lusher M, Lindsey J, Cookson M, Bashir R et al (2000) Clinical and pathologic findings in hereditary spastic paraparesis with spastin mutation. 55(1):89–94
Suzuki SO, Iwaki T, Arakawa K, Furuya H, Fujii N, Iwaki A (2011) An autopsy case of adult-onset hereditary spastic paraplegia type 2 with a novel mutation in exon 7 of the proteolipid protein 1 gene. Acta Neuropathol 122(6):775–781
Vassilopoulos D, Spengos M, Zoumbou V, Scarpalezos S (1981) The spinal canal in familial spastic paraplegia. Eur Neurol 20(2):110–114
França MC Jr, D’Abreu A, Maurer-Morelli CV, Seccolin R, Appenzeller S, Alessio A et al (2007) Prospective neuroimaging study in hereditary spastic paraplegia with thin corpus callosum. 22(11):1556–1562
Tesson C, Koht J, Stevanin G (2015) Delving into the complexity of hereditary spastic paraplegias: how unexpected phenotypes and inheritance modes are revolutionizing their nosology. Hum Genet 134(6):511–538
Solowska JM, Baas PW (2015) Hereditary spastic paraplegia SPG4: what is known and not known about the disease. Brain 138(9):2471–2484
Pérez-Brangulí F, Mishra HK, Prots I, Havlicek S, Kohl Z, Saul D et al (2014) Dysfunction of spatacsin leads to axonal pathology in SPG11-linked hereditary spastic paraplegia. 23(18):4859–4874
Loureiro JL, Brandão E, Ruano L, Brandao AF, Lopes AM, Thieleke-Matos C et al (2013) Autosomal dominant spastic paraplegias: a review of 89 families resulting from a portuguese survey. 70(4):481–487
Fourtassi M, Jacquin-Courtois S, Scheiber-Nogueira M, Hajjioui A, Luaute J, Charvier K et al (2012) Bladder dysfunction in hereditary spastic paraplegia: a clinical and urodynamic evaluation. 50(7):558–562
Shribman S, Reid E, Crosby AH, Houlden H, Warner TTJTLN (2019) Hereditary spastic paraplegia: from diagnosis to emerging therapeutic approaches
Hobson GM, Garbern JY (eds) (2012) Pelizaeus-Merzbacher disease, Pelizaeus-Merzbacher-like disease 1, and related hypomyelinating disorders. Seminars in neurology. Thieme Medical Publishers
Pascual B, De Bot S, Daniels M, França M, Toro C, Riverol M et al (2019) “Ears of the lynx” MRI sign is associated with SPG11 and SPG15 hereditary spastic paraplegia. 40(1):199–203
Hensiek A, Kirker S, Reid E (2015) Diagnosis, investigation and management of hereditary spastic paraplegias in the era of next-generation sequencing. J Neurol 262(7):1601–1612
Sedel F, Fontaine B, Saudubray J, Lyon-Caen O (2007) Hereditary spastic paraparesis in adults associated with inborn errors of metabolism: a diagnostic approach. J Inherit Metab Dis 30(6):855–864
Margetis K, Korfias S, Boutos N, Gatzonis S, Themistocleous M, Siatouni A et al (2014) Intrathecal baclofen therapy for the symptomatic treatment of hereditary spastic paraplegia. 123:142–145
Béreau M, Anheim M, Chanson J-B, Tio G, Echaniz-Laguna A, Depienne C et al (2015) Dalfampridine in hereditary spastic paraplegia: a prospective, open study. 262(5):1285–1288
de Niet M, de Bot ST, van de Warrenburg BP, Weerdesteyn V, Geurts AC (2015) Functional effects of botulinum toxin type-A treatment and subsequent stretching of spastic calf muscles: a study in patients with hereditary spastic paraplegia. J Rehabil Med 47(2):147–153
Havlicek S, Kohl Z, Mishra HK, Prots I, Eberhardt E, Denguir N et al (2014) Gene dosage-dependent rescue of HSP neurite defects in SPG4 patients’ neurons. 23(10):2527–2541
Pirozzi M, Quattrini A, Andolfi G, Dina G, Malaguti MC, Auricchio A et al (2006) Intramuscular viral delivery of paraplegin rescues peripheral axonopathy in a model of hereditary spastic paraplegia. 116(1):202–208
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
None
Additional information
We confirm that we have read the journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Murala, S., Nagarajan, E. & Bollu, P.C. Hereditary spastic paraplegia. Neurol Sci 42, 883–894 (2021). https://doi.org/10.1007/s10072-020-04981-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-020-04981-7