
Abstract
To investigate the clinical characteristics of infection in SLE patients and analyze the risk factors of infection. A retrospective analysis method was used and the data were collected from 173 case times of 142 hospitalized patients. We found the incidence rate of infections in SLE was 50.7%. The most common infection sites were lungs, followed by upper respiratory tracts and urinary tracts. The most common pathogens were bacteria, followed by fungi. The infection-associated risk factors were duration of hospitalization, lupus activity state, the use of high-dose corticosteroids and immunosuppressive agents, the low serum level of complements 3 and 4 (C3 and C4), fever, the high level of erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), the abnormality of white blood cell (< 4 × 109/L or > 10 × 109/L), and the low level of albumin (P < 0.05 or P < 0.001). The independent risk factors for SLE patients with infection consist of the abnormality of white blood cells, the high level of CRP, the low serum level of C4, and longtime hospitalization. Attention should be paid to the risk factors of infection, and treatment to enhance immunity should be carried out to reduce the chance of infection.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease with multiple organs and system involvement. Immune system disorder, T cell and B cell dysfunction, and the use of corticosteroids and immunosuppressive agents result in low immunity and prone to infection in SLE patients. At the same time, infection can also aggravate the activity of SLE, and infection is a common problem and has become one of leading causes of mortality in SLE patients [1, 2].
According to one study, almost 79% of SLE patients had serious infections even though they took glucocorticoids and other immunosuppressive agents sparingly. Infections documented in this study were usually associated with disease exacerbations [3]. In a population-based study, a significant increase in bacterial infections was observed in SLE patients as compared to an age- and gender-matched cohort of normal controls [4]. Many immune abnormalities in SLE, including complement deficiency [5,6,7], defects in chemotaxis [8], and phagocytic activity [9, 10], may account for the susceptibility of infection.
However, clinical characteristics and risk factors of infection in SLE patients vary significantly among different countries. There were few data about the clinical characteristics of infection in SLE patients in China. In this retrospective study, we focused on the clinical characteristics and risk factors of infections in patients with SLE, in order to find the types of infection, to discover the spectrum of infectious agents and predisposing risk factors, and finally to help SLE patients reduce the risks of infection.
Patients and methods
Patients
We conducted a retrospective analysis about the clinical characteristics of 142 SLE patients (173 cases times) hospitalized in 3rd Hospital of Sun Yat-sen University, from January 2015 to December 2016. There were 87 cases of infections which happened to 72 SLE patients (male:female was 1:8).
Inclusion and exclusion criteria were as follows: (1) All patients met the 2012 American College of Rheumatology SLE diagnostic criteria [3]; (2) all patients had complete clinical data and laboratory test results; by pathogen examination, (3) biochemical tests or imaging results of clinical empiric treatment effective methods were used to judge whether SLE patients had infection; (4) exclude the patients who were younger than 16 years; (5) the selected patients had no other disturbing other diseases, such as cancer.
We used body fluid (blood, urine, cerebrospinal fluid, sputum, pleural effusion, and skin secretions, etc.) examination and culture, combined with clinical symptoms, laboratory tests, imaging findings, and empirical anti-infective therapy to analyze pathogens comprehensively.
Methods
Clinical indicators
SLE disease duration: the time from patients firstly diagnosed as SLE to this time they were hospitalized. Fever: axillary temperature exceeds 37.5 °C. The use of high-dose corticosteroids: intravenous methylprednisolone ≥ 60 mg per day.
Specific research methods
Analyze the 173 cases of SLE patients’ treatment of data and summarize the site of infection and the type of infection pathogens of the 87 cases of SLE patients with infection. The 173 cases of hospitalization were divided into infection group and non-infection group; univariate logistic regression analyses were used to analyze gender, age, hospital time, hospital seasons, systemic lupus erythematosus disease activity index (SLEDAI), SLE disease duration, high-dose corticosteroids (≥ 60 mg), the number of white blood cells (WBC) (4–10 × 109/L), complement C3 (0.08–1.6 g/L), C4 (0.1–0.4 g/L), the use of immunosuppressive agents, erythrocyte sedimentation rate (ESR) (0–20 mm/h), C-reactive protein (CRP) (0–6 mg/L), albumin (36–51 g/L), and whether fever or not is the risk factors of infection, and then get out of the risk factors; then, multivariate logistic regression analyses were used to find out the independent risk factors for infection in SLE patients.
Statistical analysis
The software of SPSS version 17.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Count data were denoted by percentage or ratio. Continuous variables were expressed as mean ± standard deviation (‾x ± s). Chi-square test was used for qualitative data analysis. Risk factors were analyzed by two classification logistic regression analysis (first by univariate logistic regression analysis to identify variables, there are significant differences, then these variables into a multivariate logistic regression analysis) and calculated the odds ratio (OR) and 95% confidence interval (95%CI). Differences were considered statistically significant when P was less than 0.05 (P < 0.05).
Results
Characteristics of patients
A total of 142 SLE patients (173 case times) were recruited in this study. The demographic and clinical characteristics, including gender, age, and SLE duration, did not differ between the SLE patients with and without infection. All information about the variables compared between the two groups of patients were shown in Table 1.
Infection rate and distribution site
Seventy-two patients experienced 87 cases of infections (2 cases of infection in 7 patients, 3 cases of infection in 2 patients, 5 cases of infection in 1 patient) among the 142 SLE patients (a total of 173 cases of hospitalization times). Infection rate was 50.7%; the proportion of the total number of infection cases was 50.3%. In addition, 35.63% of infections occurred in the patients whose disease duration was less than half year; secondly, the disease duration was 6 months to 1 year. The main infection sites were located in the lungs, upper respiratory tracts, urinary tracts, skins, intestines, lungs combined with urinary tracts, and lungs combined with skins (Table 2). Ten cases of infection belonging to hospital acquired infection; the hospital infection occurrence rate was 5.78%.
Classifications of pathogens
We analyzed the classifications of pathogens in 87 cases with infection. As a result, we found the most common pathogen was bacteria (74.71%), followed by fungi (11.49%), bacteria combined with fungi (6.9%), bacteria with virus (4.60%), and virus (2.30%). More than half of pathogen culture results in patients with a bacterial infection were negative, and the most common fungal infection was Candida albicans (Table 3).
Schemes, time, and endings of anti-infection treatment
Our study found that 59.8% of the SLE patients with infection used one kind of antibiotics (cephalosporins or quinolones) for anti-infection treatment, followed by 16.1% of patients with a variety of antibiotics in combination with anti-fungal treatment, then 9.1% of patients with two or more antibiotics. Three patients did not use any anti-infective drugs during hospitalization because of the mild condition; others are that single-use anti-fungal, anti-viral, anti-TB treatment (Table 4). Most patients used anti-infection drugs for 1–2 weeks, followed by 1 week, few patients for more than 3 weeks. The infections in most patients (92.0%) were controlled after anti-infection treatment. For other patients, group with uncontrolled infection, two patients died, two patients diagnosed with tuberculosis and return to chest hospital for treatment, three patients lost consciousness, and their families gave up treatment.
Analysis of risk factors for infection
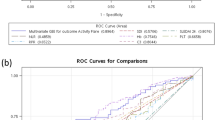
By univariate logistic regression analysis, we found that longtime hospitalization, high SLEDAI score, the use of high-dose corticosteroids (methylprednisolone > 60 mg), the use of immunosuppressive agents, the low serum level of complements 3 and 4 (C3 and C4), fever, the high level of ESR and CRP, the abnormality of WBC (< 4 × 109/L or > 10 × 109/L, including leukopenia and leukocytosis), and the low level of albumin were all risk factors for infection (as seen in Table 5). All the above differences were statistically significant (P < 0.05 or P < 0.001). In addition, gender, age, hospitalization season, and SLE disease duration were not correlated with infection. We then analyzed these above risk factors by multivariate logistic regression analysis. As a result, we found the abnormality of WBC, the high level of CRP, the low serum level of C4, and longtime hospitalization were independent risk factors for SLE patients with infection (as seen in Table 6). When the hospitalization time exceed for more than 14 days, the risk rate of SLE patients with infection was 5.052 times more than that of patients with the hospitalization time within 14 days, then followed by the abnormality of WBC, the high level of CRP, and the low serum level of C4 (shown in Table 6). Finally, we analyzed the correlation between the use of different kinds of immunosuppressive agents and infection, and we found there were significant differences between different kinds of immunosuppressive agents in SLE patients with infection (P = 0.012, shown in Table 7). Then, we made comparison between groups, and we found using mycophenolic acid (MMF) and cyclophosphamide (CTX) was significantly correlated with infection (P = 0.005). What’s more, patients with CTX were more likely to develop infection than those with MMF (shown in Table 8). We tried to perform ROC curve analysis, using CRP, WBC, C4 levels, and hospitalization time to predict whether or not there is infection. As shown in Fig. 1, we found CRP (AUC = 0.675) and hospitalization time (AUC = 0.786) may predict whether or not there is infection (P < 0.000); however, WBC and C4 levels could not predict whether or not there is infection (P > 0.05).

ROC curve analysis. CRP (AUC = 0.675) and hospitalization time (AUC = 0.786) may predict whether or not there is infection (P < 0.000); however, WBC and C4 levels could not predict whether or not there is infection (P > 0.05)
Discussion
Systemic lupus erythematosus (SLE) is a chronic auto-immune disease with varied organ involvement. Infection remains an important cause of mortality and morbidity in patients with SLE. In the Euro Lupus cohort, 36% of patients presented infections during follow-up, and almost 30% of deaths were related to infections in the first 5 years of follow-up [10]. Infections were also one of the leading causes of hospitalization in SLE patients [11, 12].
In this study, we observed the clinical characteristics of infection in SLE patients and analyzed the risk factors of infection. We found almost one half of patients with SLE developed infection before or during their hospitalization. The prevalence observed in our study was higher than that in Korea, Canada, and Britain [13,14,15]. The increased prevalence of infection in our SLE patients might reflect the poor living and public health conditions as well as abuse of antibiotics in developing countries.
Several clinical characteristics in SLE patients with infection were noted in this study. Firstly, infection occurred early, and 60.92% of the infections occurred in the course of less than 1 year. Secondly, infection site distributions in SLE patients were wide, and the most common infection sites were the lungs, followed by upper respiratory tracts and urinary tracts, which was consistent with the discoveries of other researchers [15,16,17,18,19]. Thirdly, the most common pathogens were bacteria, followed by fungi, which was similar to other studies [16, 19, 20]. However, most bacterial culture results were negative, and empirical anti-infective therapy was usually effective. Therefore, for SLE patients with infection, empirical antibiotic therapy should be decided as soon as possible, even should be used before the pathogen test results came out, which may avoid further aggravation of infection. Fourthly, the infection rate of mycobacterium tuberculosis (TB) was 2.3%, which was lower than the 12% reported from South Africa [1], the 14% reported from Spain [21], the 8.3% reported in Korea [15], and the 3.5% reported in Mexico [22]. Fifthly, our study found that more than one half of the SLE patients with infection used one kind of antibiotics (cephalosporins or quinolones) for anti-infection treatment. In additional, most patients used anti-infection drugs for 1–2 weeks, and the infection in most patients (92.0%) were controlled after anti-infection treatment.
By univariate logistic regression analysis, we found that longtime hospitalization, high SLEDAI score, the use of high-dose corticosteroids (methylprednisolone > 60 mg), the use of immunosuppressive agents, the low serum level of complements 3 and 4 (C3 and C4), fever, the high level of ESR and CRP, the abnormality of WBC, and the low level of albumin were all risk factors for infection. Longtime hospitalization not only means relatively difficult to control the disease, but also prefers to increase the probability of infection, especially the probability of nosocomial infection. High SLEDAI score, the low serum level of complements, leukopenia and albumin, the use of high-dose corticosteroids, and immunosuppressive agents will weaken the immune system of patients and reduce the patient’s immunity and increase the chances of infection. However, the patient’s gender, age, hospitalization season, and SLE disease duration were not associated with infection. All the above results were similar to the previous reports [2, 3, 16, 19]. By multivariate logistic regression analysis, we found the abnormality of WBC, the high level of CRP, the low serum level of C4, and longtime hospitalization were independent risk factors for SLE patients with infection. When the above factors happen, they also remind us attentions should be paid to the presence of infection. Moreover, we found that use of MMF and CTX was significantly correlated. What’s more, patients with CTX were more likely to occur infection than those with MMF, which was consistent with the previous discoveries of other researchers [20, 23]. Therefore, the patients who use CTX for treatment should be focused on whether they have infection occurred.
Conclusions
In conclusion, we investigated the clinical characteristics of infection in SLE patients and analyzed the risk factors of infection. There are some notable features of infection in Chinese patients with SLE, including more infections occurred to SLE patients whose disease duration ≤ 1 year, higher proportion of respiratory tract involvement, and bacteria as the most common pathogen, and 1–2 weeks’ empirical anti-infection was effective. The independent risk factors for SLE patients with infection consist of the abnormality of WBC (< 4 × 109/L or > 10 × 109/L, including leukopenia and leukocytosis), the high level of CRP, the low serum level of C4, and longtime hospitalization. Therefore, attention should be paid to the risk factors of infection, and treatment to enhance immunity should be carried out to reduce the chance of infection.
Abbreviations
- SLE:
-
Systemic lupus erythematosus
- ESR:
-
Erythrocyte sedimentation rate
- CRP:
-
C-reactive protein
- C3:
-
Complement 3
- C4:
-
Complement 4
- WBC:
-
White blood cells
- MMF:
-
Mycophenolic acid
- CTX:
-
Cyclophosphamide
- SLEDAI:
-
Systemic lupus erythematosus disease activity index
References
Dubula T, Mody GM (2015) Spectrum of infections and outcome among hospitalized South Africans with systemic lupus erythematosus. Clin Rheumatol 34(3):479–488
Wu L, Wang X, Chen F, Lv X, Sun W, Guo Y, Hou H, Ji H, Wei W, Gong L (2017) T cell subsets and immunoglobulin G levels are associated with the infection status of systemic lupus erythematosus patients. Braz J Med Biol Res 51(2):e4547
Jung JY, Suh CH (2017) Infection in systemic lupus erythematosus, similarities, and differences with lupus flare. Korean J Intern Med 32(3):429–438
Wang KC, Liu PH, Yu KH, Weng YM, Ng CJ, Chiu TF, Chen SY (2017) Is initial C-reactive protein level associated with corticosteroid use in lupus erythematosus patients during a bacterial infection episode? Immunol Lett 185:84–89
Lin H, Wei JC, Tan CY, Liu YY, Li YH, Li FX (2012) Survival analysis of late-onset systemic lupus erythematosus: a cohort study in China. Clin Rheumatol 31:1683–1689
Chen CH, Tai SB, Chen HC, Yang DH, Peng MY, Lin YF (2015) Analysis of erythrocyte C4d to complement receptor 1 ratio: use in distinguishing between infection and flare-up in febrile patients with systemic lupus erythematosus. Biomed Res Int 2015:939783
Hahn BH, Mcmahon MA, Wilkinson A (2012) American College of Rheumatology guidelines for guidelines for screening, treatment, and management of lupus nephritis [J]. Arthritis Care Res 64(6):797–808
Badr G, Sayed A, Abdel-Maksoud MA, Mohamed AO, El-Amir A, Abdel-Ghaffar FA, Al-Quraishy S, Mahmoud MH (2015) Infection of female BWF1 lupus mice with malaria parasite attenuates B cell autoreactivity by modulating the CXCL12/CXCR4 Axis and its downstream signals PI3K/AKT, NFκB and ERK. PLoS One 10(4):e0125340
Wu SA, Yeh KW, Lee WI, Yao TC, Kuo ML, Huang B, Huang JL (2013) Impaired phagocytosis and susceptibility to infection in pediatric-onset systemic lupus erythematosus. Lupus 22(3):279–288
Cervera R, Khamashta MA, Font J (2003) Morbidity and mortality in systemic lupus erythematosus during a 10-year period: a comparison of early and late manifestations in a cohort of 1000 patients. Medicine (Baltimore) 82:299–308
Yurkovich M, Vostretsova K, Chen W, Avina-Zubieta JA (2014) Overall and cause-specific mortality in patients with systemic lupus erythematosus: a meta-analysis of observational studies. Arthritis Care Res 66:608–616
Tektonidou MG, Wang Z, Dasgupta A, Ward MM (2015) Burden of serious infections in adults with systemic lupus erythematosus: a National Population-Based Study, 1996–2011. Arthritis Care Res 67(8):1078–1085
Han BK, Bhatia R, Traisak P (2013) Clinical presentations and outcomes of systemic lupus erythematosus patients with infection admitted to the intensive care unit. Lupus 22(7):690–696
Ekwom PE (2013) Systemic lupus erythematosus (SLE) at the Kenyatta National Hospital. Clin Rheumatol 32(8):1215–1217
Jeong SJ, Choi H, Lee HS, Han SH, Chin BS, Baek JH, Kim CO, Choi JY, Song YG, Kim JM (2009) Incidence and risk factors of infection in a single cohort of 110 adults with systemic lupus erythematosus. Scand J Infect Dis 41(4):268–274
Chen D, Xie J, Chen H, Yang Y, Zhan Z, Liang L, Yang X (2016) Infection in southern Chinese patients with systemic lupus erythematosus: spectrum, drug resistance, outcomes, and risk factors. J Rheumatol 43(9):1650–1656
Goldblatt F, Chambers S, Rahman A, Isenberg DA (2009) Serious infections in British patients with systemic lupus erythematosus: hospitalisations and mortality. Lupus 18:682–689
Bosch X, Guilabert A, Pallarés L, Cervera R, Ramos-Casals M, Bové A, Ingelmo M, Font J (2006) Infections in systemic lupus erythematosus: a prospective and controlled study of 110 patients. Lupus 15:584–589
Danza A, Ruiz-Irastorza G (2013) Infection risk in systemic lupus erythematosus patients: susceptibility factors and preventive strategies. Lupus 22:1286–1294
Tse KC, Tang CS, Lam MF, Yap DY, Chan TM (2009) Cost comparison between mycophenolate mofetil and cyclophosphamide-azathioprine in the treatment of lupus nephritis. J Rheumatol 36(1):76–81
Ruiz-Irastorza G, Olivares N, Ruiz-Arruza I, Martinez-Berriotxoa A, Egurbide MV, Aguirre C (2009) Predictors of major infections in systemic lupus erythematosus. Arthritis Res Ther 11(4):R109
Navarro-Zarza J, Alvarez-Hernandez E, Casasola-Vargas J et al (2010) Prevalence of community-acquired and nosocomial infections in hospitalized patients with systemic lupus erythematosus. Lupus 19(1):43–48
Tse KC, Tang CS, Lio WI, Lam MF, Chan TM (2006) Quality of life comparison between corticosteroid-and-mycofenolate mofetil and corticosteroid and oral cyclophosphamide in the treatment of severe lupus nephritis. Lupus 15(6):371–379
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Rights and permissions
About this article

Cite this article
Hou, C., Jin, O. & Zhang, X. Clinical characteristics and risk factors of infections in patients with systemic lupus erythematosus. Clin Rheumatol 37, 2699–2705 (2018). https://doi.org/10.1007/s10067-018-4198-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-018-4198-8