
Abstract
Objectives
To evaluate light transmittance as a function of wavelength for eight composite materials and compare the transmittance for blue light produced from two curing units with different emission spectra.
Materials and methods
Light transmittance through 2- and 4-mm-thick composite specimens was recorded in real time during 30 s of curing using a broad-spectrum (peaks at 405 and 450 nm) and a narrow-spectrum (peak at 441 nm) LED-curing unit. The spectral resolution of 0.25 nm and temporal resolution of 0.05 s resulted in a large amount of light transmittance data, which was averaged over particular spectral ranges, for the whole measurement period. Statistical analysis was performed using Welch ANOVA with Games-Howell post hoc test, t test, and Pearson correlation analysis. The level of significance was 0.05 and n = 5 specimens per experimental group were prepared.
Results
Light transmittance varied as a function of wavelength and time, revealing significantly different patterns among the tested materials. Light transmittance for different parts of curing unit spectra increased in the following order of emission peaks (nm): 405 < 441 < 450. Of particular interest was the difference in transmittance between 441 and 450 nm, as these peaks are relevant for the photoactivation of camphorquinone-containing composites. A high variability in light transmittance among materials was identified, ranging from statistically similar values for both peaks up to a fourfold higher transmittance for the peak at 450 nm.
Conclusion
Each material showed a unique pattern of wavelength-dependent light transmittance, leading to highly material-dependent differences in blue light transmittance between two curing units.
Clinical relevance
Minor differences in blue light emission of contemporary narrow-peak curing units may have a significant effect on the amount of light which reaches the composite layer bottom.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Multiple variables interact to affect the quality of light curing, thereby determining the final performance of composite restorations [1]. Contemporary high-output light-emitting diode (LED)–curing units allow adequate curing at clinically acceptable times but several important drawbacks are still present, such as the narrow emission spectrum of single-peak LED-curing units which may produce inferior cure in composites containing “alternative” (other than camphorquinone) photoinitiators [2]. Other drawbacks include the spatial inhomogeneity of the radiant exitance, as well as the spectral differences across the curing unit tip [3], the potential for pulpal damage due to the heating effect [4], and issues related with handling and maintenance of curing units in a clinical setting [5]. These issues have been extensively addressed in the recent literature in order to raise awareness among clinicians regarding the importance of appropriate light curing for the overall success of restorative treatments [1, 6,7,8].
The capability of a resin composite material to transmit curing light is a major factor determining the quality of polymerization as a function of depth, thus dictating the clinically applicable layer thickness, which is material-dependent and ranges between 1.5 and 6 mm [7, 9]. Light transmittance through a composite material is determined by light absorption and scattering [10], the latter being a complex function of particle size distribution and the mismatch in the refractive indices between filler particles and the resinous matrix [11]. Light transmittance commonly increases throughout the light curing due to the reduction of refractive index mismatch [12], although it is possible to formulate composites whose refractive index mismatch increases as the light curing progresses [13].
Light transmittance of composite materials declines as the wavelength of incident light shortens, this being the reason why composites containing violet light–absorbing photoinitiators have a severely limited depth of cure [14]. The decline in light transmittance in going from blue towards the violet part of the spectrum is a known issue; however, the importance of small differences in the blue part of the spectrum which exist among curing units has not been evaluated. The blue emission of contemporary curing units usually features a narrow band with peak values in the range of 444–477 nm [1, 15]. The clinical significance of these variations on the curing light penetration has not been sufficiently acknowledged in the literature, as it seems to be overshadowed by the more pronounced difference between the blue and violet light [2, 8, 14]. It was thus of interest to focus on light transmittance differences in the blue part of the spectrum since this part is crucial for the initiation of the majority of contemporary composites which are rendered photosensitive by camphorquinone with absorption in the range of 425–495 nm and maximum at 468 nm [16]. Composites using violet light–absorbing photoinitiators often also contain the camphorquinone/amine system in various amounts [8, 17].
The aim of this study was to evaluate light transmittance as a function of wavelength for eight composite materials and compare the transmittance for blue light produced from two curing units with different emission spectra. In the first part of the study, light transmittance was recorded in real time during light curing using a broad-spectrum LED-curing unit, in order to describe light transmittance as a function of wavelength. In the second part, the clinical relevance of wavelength-dependent light transmittance was demonstrated by comparing the blue light transmittance between two LED-curing units.
The null hypotheses were that (I) light transmittance would not depend on wavelength throughout the light-curing period and (II) that light transmittance for the blue part of the spectrum would not differ between two curing units.
Materials and methods
Eight high-viscosity (sculptable) resin composites were investigated (Table 1) in order to include materials featuring different resin and filler compositions, different filler loadings, and different techniques for clinical use (layering or bulk-fill). Composite specimens of two thicknesses (2 and 4 mm) and a diameter of 8 mm were prepared using cylindrical Teflon molds with black-colored surfaces. The uncured composite was cast into the mold and covered from both sides with polyethylene terephthalate (PET) films. The curing unit tip was centered immediately (0 mm) above the mold opening, perpendicular to the composite surface. Two curing units were used: a single-peak “monowave” unit—Bluephase Style M8 (MW)—and a dual-peak “polywave” unit—Bluephase Style (PW). Both curing units were manufactured by Ivoclar Vivadent, Schaan, Liechtenstein. Radiant exitance values declared by the manufacturer were 800 and 1100 mW/cm2, for MW and PW respectively. Curing units were activated for 30 s and the light transmitted through composite specimens was collected with a lens positioned below the opposite mold opening and directed into a charge-coupled device array fiber spectrometer HR4000 (Ocean Optics, Dunedin, FL, USA). The lens was adjusted as to allow that all of the light which passed through the specimen (d = 8 mm) was captured by the fiber (d = 4 mm). The curing time of 30 s was chosen because it was the longest continuous curing setting available for the curing units investigated and it enabled delivering clinically relevant radiant exposures. The spectra were collected at a rate of 20 per second, using a custom-made computer program prepared in LabView 2011 (National Instruments, Austin, TX, USA). Light transmittance was calculated by dividing the irradiance which passed through the composite specimen by the irradiance which was measured passing through the empty mold covered from both sides with PET films [18]. In this way, the analysis was limited to the light that passed through the 8-mm aperture of the empty mold in order to address inhomogeneities of the curing unit tip. The measurements were performed at room temperature of 22 ± 1 °C. For each combination of composite material, curing unit, and layer thickness, n = 5 specimens were prepared, giving a total number of 160 specimens. For each specimen, 600 spectra were recorded (20 spectra/s × 30 s curing time) in the range of 350–540 nm, with a resolution of 0.25 nm. Logging the light transmittance in real time throughout the light-curing period resulted in a 2-dimensional array, relating each transmittance value to the individual wavelength and time.
Due to the large amount of light transmittance data (600 spectra × 760 wavelengths = 456,000 individual values for each specimen), these were summarized in a parameter denoted as “average transmittance” which was calculated by averaging the transmittance values throughout the whole 30-s curing period. This parameter can be regarded as “effective” transmittance since it can be multiplied by the radiant exposure received at the specimen surface to calculate the radiant exposure which reached the bottom. Thus, defined average transmittance was calculated across different spectral ranges, as follows:
- 1.
For MW: the whole measured range (350–540 nm), denoted as “MW (overall)”
- 2.
For PW: the whole measured range (350–540 nm), denoted as “PW (overall)”
- 3.
For PW: the violet part of the spectrum (360–422 nm), denoted as “PW (violet)”
- 4.
For PW: the blue part of the spectrum (422–525 nm), denoted as “PW (blue)”
All of the investigated composites use the camphorquinone/amine photoinitiator system, while four of them contain additional photoinitiators: TEC A2 and A3 contain Lucirin TPO [8, 19], while TECBF IVA and IVB contain a germanium-based photoinitiator known as Ivocerin [20]. The analysis of the violet light transmittance was performed for all composites for comprehensiveness, despite the fact that some of them lack violet-absorbing photoinitiators. Also, all materials were evaluated at 2 and 4 mm, although the latter is not recommended for conventional composites.
Since the light transmittance data did not significantly deviate from normality (Shapiro-Wilk’s test) but showed heterogeneous variances among experimental groups (Levene’s test), the statistical analysis was performed using a Welch ANOVA followed by Games-Howell post hoc test. Pairwise comparisons between two shades for materials TEC and TECBF were performed using a t test for independent observations and homogeneous or heterogeneous variances, as determined individually for each pair by Levene’s test. Pearson correlation analysis was used to explore the relationship between composite filler load (vol%) and the transmittance ratios of PW (blue)/MW (overall), as well as PW (blue)/PW (violet). Statistical analysis was performed in SPSS 20 (IBM, Armonk, NY, USA) with α = 0.05.
Results
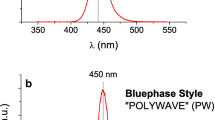
An exemplary plot of light transmittance as a function of wavelength and time is shown in Fig. 1. Light transmittance is presented in the range of 400–500 nm, which allowed a good signal to noise ratio. Below 400 nm, signal quality deteriorated due to the very low irradiance which reached the detector. To put the emission spectra of MW and PW in the context of the investigated wavelength range, these are overlapped on the light transmittance plot. The emission spectra of MW and PW presented in Fig. 1 also indicate which part of light transmittance curves is clinically relevant for light curing of resin composites using these particular curing units.

Example of light transmittance curves recorded during light curing for 30 s, overlapped with the emission spectra of the wide-spectrum curing unit (PW) and the narrow-spectrum unit (MW). The emission spectra of curing units are plotted on an arbitrary scale. Time points on the z-axis (s): 0.2, 0.25, 0.3, 0.35, 0.4, 1, 2, 3, and 30
Light transmittance curves for each material at layer thicknesses of 2 and 4 mm are shown in Figs. 2 and 3, respectively. Note a different scaling on the z-axis—a longer period between time points was chosen in Fig. 3 because of a slower transmittance rise in 4-mm layers. Generally, light transmittance increased with the increase in wavelength and time. The shapes of transmittance curves in Fig. 2 differed among materials, from steeper ones (e.g., GDP, TECBF) to comparatively flat ones (e.g., FBF, XF). The shapes of the curves in Fig. 3 are more difficult to distinguish due to the y-axis scale which was for comparability retained the same as in Fig. 2. However, the material-characteristic behaviors are observable: FBF and XF maintained a more even transmittance across the presented wavelength range, while in the remaining composites the transmittance at low-end wavelengths was very low or immeasurable.

Light transmittance as a function of wavelength and time for the thickness of 2 mm. Time points on the z-axis (s): 0.2, 0.25, 0.3, 0.35, 0.4, 1, 2, 3, and 30

Light transmittance as a function of wavelength and time for the thickness of 4 mm. Time points on the z-axis (s): 0.2, 0.25, 0.3, 0.35, 0.4, 5, 10, 15, and 30
Figure 4 shows the average transmittance calculated for different wavelength ranges. Besides the differences among materials, especially between the groups of conventional and bulk-fill composites, spectral differences also significantly affected light transmittance. For most of the materials, light transmittance increased in the order: PW (violet) < MW (overall) < PW (blue), which reflects the increase in wavelength of these particular parts of the spectrum (Figs. 2 and 3). Exceptions were identified in some materials, for example in FBF and XF, in case of which the light transmittance at 2 mm was higher for PW (violet) than for MW (overall). Also, statistically similar light transmittance values were found in some materials despite wavelength differences, for example in TEC A2 and A3 at 4 mm transmittance for MW (overall) was similar to that for PW (blue).

Light transmittance averaged throughout the 30-s curing period for the selected wavelength ranges: MW (overall)—whole emission spectrum of MW with the peak at 441 nm; PW (blue)—blue part of the PW emission spectrum with the peak at 450 nm; PW (violet)—violet part of the PW emission spectrum with the peak at 405 nm; PW (overall)—whole emission spectrum of PW. Same lowercase letters denote statistically homogeneous groups within a material. Statistically significant differences between two different shades of TEC (A2 vs. A3) and TECBF (IVA vs. IVB) are marked with square brackets. Error bars denote one standard deviation
Figure 5 shows the ratio of PW (blue)/MW (overall). This parameter indicates how many times the blue light transmittance was higher for PW compared with MW. Statistically similar blue light transmittance between PW and MW was identified only at 4 mm in TEC A2 and A3. For all other combinations of material and layer thickness, PW had significantly higher blue light transmittance, reaching up to a fourfold difference. The effect of layer thickness on the ratio of blue light transmittance was minor in comparison to the pronounced differences between materials.

The ratio of blue light transmittance, calculated as PW (blue)/MW (overall). Asterisks (*) denote statistical similarity of blue light transmittance between PW and MW (transmittance ratio close to unity)
Figure 6 shows that a marginally significant, moderate linear correlation was identified between the composite filler load and the ratio of PW (blue)/MW (overall). On the other hand, no significant correlation was identified between the filler load and the ratio of PW (blue)/PW (violet), with p values of 0.9 and 0.6 for 2 mm and 4 mm, respectively.

The ratio of PW (blue)/MW (overall) plotted as a function of filler load. Results of the Pearson correlation analysis are shown
Discussion
This study investigated the wavelength-dependent light transmittance which was found to vary widely among eight composite materials tested. Light transmittance data for particular parts of the curing unit spectra were summarized in a parameter termed average transmittance. It was used to demonstrate that small spectral differences between two curing units can result in a considerable and strikingly material-dependent difference in the amount of blue light that reaches the bottom of a 2- or 4-mm-thick layer. Both null hypotheses were thus rejected. The term “blue light” for MW corresponds to its whole emission spectrum, while for PW it corresponds to wavelengths above 422 nm (Fig. 1). The value of 422 nm was chosen as the boundary between “violet” and “blue” light [14] because the minimum between two peaks in the emission spectrum of PW occurred at this wavelength. This approach for separating “violet” and “blue” light was used for its simplicity and for giving results similar to a more complex approach which would involve deconvolution (variations below 1%).
Light transmittance as a function of wavelength
Although bulk-fill composites as a group were more translucent than conventional composites (Figs. 2 and 3), no patterns of wavelength-dependence which would be characteristic for a particular material group were identified. The shapes of light transmittance curves were unique for each composite, with no influence of belonging to a particular material group. The reason may be that variations in light transmittance as a function of wavelength were due to the geometry of filler particles which varied among different material compositions regardless of their classification as conventional or bulk-fill composites [21].
Generally, light scattering on filler particles reaches maximum intensity for the particle size of approximately half the wavelength of incident light [22], and increasing or decreasing the particle size reduces light scattering, thereby improving transmittance. While the relationship between particle size and light transmittance in dental composites is easy to demonstrate in model composites with known particle sizes [23], commercial composites feature complex and never fully disclosed particle size distributions, making it difficult to relate light transmittance to particle geometry [7]. The particle size data presented in Table 1 is thus insufficient for a detailed explanation of its effect on light transmittance, especially in cases in which only the average particle size (GDP) or the range of particle size distribution (TEC) is disclosed. However, some results can be discussed considering the particle size. Firstly, the “flat” light transmittance profiles of FBF and XF (Figs. 2 and 3) may be caused by particles much smaller (FBF) or much larger (XF) than required for the scattering maximum to occur in the wavelength range investigated. Secondly, a steep transmittance decline towards the violet part of the spectrum in TECBF may be related to two peaks in particle size distribution (160 and 200 nm) which contributed to intense scattering of violet light. A detailed discussion regarding the influence of the refractive index mismatch between the resin and fillers was not possible since the precise material composition was not disclosed by the manufacturers.
Besides the obvious observation that light transmittance at 4 mm was considerably lower than that at 2 mm, it should be noted that for most of the composites, violet light transmittance was severely impaired in a 4-mm-thick layer (Figs. 2 and 3). While this is not an issue for composites without violet-absorbing photoinitiators or conventional composites, it is relevant for TECBF which combines camphorquinone/amine and a proprietary photoinitiator Ivocerin with the absorption maximum at 410 nm [20]. Violet light transmittance in TECBF at 4 mm thickness was significantly impaired from the start of the curing period (no light detectable in the range of 400–430 nm), but improved slightly as the polymerization advanced (Fig. 3). However, until the end of the curing period, no light was detectable for wavelengths below 410 nm. These findings suggest the limited effectiveness of the additional photoinitiator Ivocerin in thick layers of TECBF, which appears to be compensated by the camphorquinone/amine system since TECBF has been reported to attain sufficient cure at 4-mm-thick layers [24, 25]. Also, Ivocerin differs from other violet light–absorbing photoinitiators by its absorption range (370–460 nm) extending into the blue part of the spectrum. It can thus be activated by the blue light of lower wavelengths, albeit the efficiency of activation declines as the wavelength increases from the absorption maximum at 410 nm.
In addition to light scattering, absorption by photoinitiator also contributes to light attenuation [26]. This effect is visible as a modest depression in transmittance curves around the camphorquinone absorption maximum (468 nm) at early times, which gradually disappears towards later times as camphorquinone is consumed. This is best observed by comparing the first curve (0.2 s) and the last curve (30 s) for 2-mm-thick specimens (Fig. 2). A similar effect was identified in TECBF around the absorption maximum of Ivocerin (410 nm), while the effect of Lucirin TPO in TEC was not observed because its absorption maximum (around 350 nm) was outside of the measured range. The barely detectable effect of the photoinitiator absorption was rather small compared with the much more pronounced effect of other factors, namely material composition, wavelength, and time.
In the discussion on the low light transmittance within the violet wavelength range, an important difference between camphorquinone and violet light–absorbing photoinitiators should be mentioned. Unlike camphorquinone which upon excitation undergoes complexation with a co-initiator and produces one amino alkyl radical able to start the polymerization (Norrish type II reaction), the violet light–absorbing photoinitiators produce multiple radicals via a photoactivated cleavage (Norrish type I reaction). In conjunction with higher molar extinction coefficients of violet light–absorbing photoinitiators, this mechanism results in higher quantum yields compared with those of the camphorquinone/amine system [27]. For example, the quantum yield of Lucirin TPO is about five times higher than that of camphorquinone [28], making it more efficient than camphorquinone at low irradiances. This effect can partially compensate for high attenuation of violet light at 2-mm-thick layers (Fig. 2). However, it becomes ineffective at excessively thick layers which for most of the materials transmitted practically no violet light (Fig. 3).
Differences in blue light transmittance between two curing units
Light transmittance in dental composites is known to vary as a function of wavelength [14, 29, 30], and the present study intended to show that a small shift (9 nm) in the blue emission between MW and PW is capable of producing a considerable effect on the capability of a material to transmit curing light (Fig. 4). To compare the sensitivity of the materials to the spectral difference between MW and PW, the ratio of blue light transmittance was calculated (Fig. 5). This parameter varied widely among the materials—from TEC which showed no significant difference between the curing units to the most extreme case of GRA which transmitted four times more blue light from PW compared with MW. It should additionally be mentioned that the emission spectrum of MW is less aligned with the absorption spectrum of camphorquinone than the blue part of PW emission spectrum. That means that photons emitted from MW will, on average, have a lower probability of being absorbed [31]. This phenomenon acts together with the lower light transmittance to render MW less effective than PW for curing of the camphorquinone-initiated composites. Given that curing units available on the market feature narrow blue emission peaks in the range of 444–477 nm [1, 15], even higher differences in blue light transmittance between curing units than reported in the present study can be expected.
The magnitude of differences in blue light transmittance between the curing units was not intuitively predictable by simply observing the shapes of transmittance curves in Figs. 2 and 3 due to the irregularity of the curves and the fact that their shape changed over time. For example, although the curves for FBF at 2 mm appear rather flat, a twofold higher blue light transmittance was measured for PW compared with MW (Fig. 5). A difference of similar magnitude was identified in TECBF, despite the fact that its transmittance curves appear steeper than those of FBF. Furthermore, the slope of transmittance curves can be misjudged due to different y-axis scaling, as exemplified by the comparison of the curves for GRA in Figs. 1 and 2. These considerations suggest that calculating the average transmittance over specific wavelength ranges throughout the whole curing period helped to reveal important differences in curing unit performance, which were not apparent from observing raw transmittance data.
Manufacturers often provide incomplete curing unit specifications (e.g., by reporting only overall radiant exitance values, thus ignoring spectral differences) [1] and overrate the curing unit output [32]. The consequences of these inaccuracies can be illustrated by the following calculation. According to manufacturer specifications, MW and PW deliver 24 and 33 J/cm2 during 30 s of curing, respectively. As reported in a previous study [12], the actual output of MW and PW was lower than specified, amounting to 658 and 938 mW/cm2, thus the incident radiant exposure for 30 s would be 19.7 and 28.1 J/cm2, respectively. For a 2-mm-thick layer of the material which showed the most pronounced difference in light transmittance between the curing units (GRA), radiant exposure for the blue light reaching the bottom of the layer would be 0.68 and 3.59 J/cm2, for MW and PW respectively. Thus, for MW to reach the same radiant exposure of blue light as PW, 5.3 times longer curing time would be required, which is not obvious from scarcely documented manufacturer specifications of the two look-alike curing units with rather similar nominal values of radiant exitance (800 and 1100 mW/cm2). By applying the same calculation, it can be estimated for other composites that curing time for MW should be 2.0 to 3.2 times longer to attain the same radiant exposure for blue light as PW at the bottom of a 2-mm-thick layer. Considering only nominal radiant exitance while disregarding spectral differences and the fact that curing units output is usually lower than specified by manufacturers, one would assume that this factor would be much lower, namely 1100/800 = 1.4.
Light transmittance data of commercial composites are occasionally put forward by manufacturers for marketing purposes. However, these data make little sense unless the spectral range at which transmittance was measured is precisely described. Knowing the light transmittance in one part of the spectra cannot be used to predict transmittance values in other spectral ranges [30], except in the unlikely scenario in which a clinician has detailed data on wavelength-dependent light transmittance, such as those presented in Figs. 2 and 3. Additionally, different shapes of transmittance vs. wavelength curves identified among materials suggest that no generalized approximation, which would be valid for all materials, can be employed.
Small amounts of intensely absorbing pigment compounds used to adjust the composite shade are known to affect light transmittance [7], and this effect is not always straightforward in the sense that darker shades correspond to lower transmittance [30]. A statistically significant difference between the two shades of TECBF was identified for MW at 2 mm (Fig. 4). The differences between shades were more pronounced at 4 mm—statistical significance was identified for both curing units in the case of TEC and for PW in the case of TECBF. However, the magnitude of these differences was minor compared with considerably greater, and thus more clinically relevant, differences due to different material compositions and wavelength ranges.
Since the composite with the highest filler load (GRA) also showed the highest blue light transmittance ratio, a possible correlation between these two parameters was explored. Moderate correlations were found for both layer thicknesses (Fig. 6), suggesting that more highly filled composites tend to be more sensitive to differences in blue emission spectra. This is probably related to the total surface area of filler particles as an important factor affecting the intensity of light scattering [22], but a more profound discussion of this phenomenon is not possible due to the lack of detailed data on filler particle size. Additionally, no correlation was identified between the filler load and the ratio of PW (blue)/PW (violet), suggesting limited relevance of the aforementioned relationship between filler load and light transmittance ratios calculated for different wavelengths.
Conclusions
Plotting light transmittance as a function of curing light wavelength revealed different material-dependent patterns. This dependence of light transmittance on wavelength is clinically relevant because minor differences in the blue light emission of contemporary narrow-peak curing units may have a significant effect on the amount of light which reaches the composite layer bottom. The sensitivity to this effect varied greatly among the tested composites, reaching up to a fourfold difference in blue light transmittance between two curing units whose blue emission peaks differed by 9 nm.
References
Price RB, Ferracane JL, Shortall AC (2015) Light-curing units: a review of what we need to know. J Dent Res 94(9):1179–1186. https://doi.org/10.1177/0022034515594786
Santini A, Miletic V, Swift MD, Bradley M (2012) Degree of conversion and microhardness of TPO-containing resin-based composites cured by polywave and monowave LED units. J Dent 40(7):577–584. https://doi.org/10.1016/j.jdent.2012.03.007
Price RB, Labrie D, Rueggeberg FA, Sullivan B, Kostylev I, Fahey J (2014) Correlation between the beam profile from a curing light and the microhardness of four resins. Dent Mater 30(12):1345–1357. https://doi.org/10.1016/j.dental.2014.10.001
Park SH, Roulet JF, Heintze SD (2010) Parameters influencing increase in pulp chamber temperature with light-curing devices: curing lights and pulpal flow rates. Oper Dent 35(3):353–361. https://doi.org/10.2341/09-234-L
Ernst CP, Price RB, Callaway A, Masek A, Schwarm H, Rullmann I, Willershausen B, Ehlers V (2018) Visible light curing devices - irradiance and use in 302 German dental offices. J Adhes Dent 20(1):41–55. https://doi.org/10.3290/j.jad.a39881
Price RB, Shortall AC, Palin WM (2014) Contemporary issues in light curing. Oper Dent 39(1):4–14. https://doi.org/10.2341/13-067-LIT
Palin WM, Leprince JG, Hadis MA (2018) Shining a light on high volume photocurable materials. Dent Mater 34(5):695–710. https://doi.org/10.1016/j.dental.2018.02.009
Shimokawa C, Sullivan B, Turbino ML, Soares CJ, Price RB (2017) Influence of emission spectrum and irradiance on light curing of resin-based composites. Oper Dent 42(5):537–547. https://doi.org/10.2341/16-349-L
Miletic V, Pongprueksa P, De Munck J, Brooks NR, Van Meerbeek B (2017) Curing characteristics of flowable and sculptable bulk-fill composites. Clin Oral Investig 21(4):1201–1212. https://doi.org/10.1007/s00784-016-1894-0
Emami N, Sjodahl M, Soderholm KJ (2005) How filler properties, filler fraction, sample thickness and light source affect light attenuation in particulate filled resin composites. Dent Mater 21(8):721–730. https://doi.org/10.1016/j.dental.2005.01.002
Musanje L, Darvell BW (2006) Curing-light attenuation in filled-resin restorative materials. Dent Mater 22(9):804–817. https://doi.org/10.1016/j.dental.2005.11.009
Par M, Repusic I, Skenderovic H, Sever EK, Marovic D, Tarle Z (2018) Real-time light transmittance monitoring for determining polymerization completeness of conventional and bulk fill dental composites. Oper Dent 43(1):E19–E31. https://doi.org/10.2341/17-041-L
Ilie N (2017) Impact of light transmittance mode on polymerisation kinetics in bulk-fill resin-based composites. J Dent 63:51–59. https://doi.org/10.1016/j.jdent.2017.05.017
Harlow JE, Rueggeberg FA, Labrie D, Sullivan B, Price RB (2016) Transmission of violet and blue light through conventional (layered) and bulk cured resin-based composites. J Dent 53:44–50. https://doi.org/10.1016/j.jdent.2016.06.007
Harlow JE, Sullivan B, Shortall AC, Labrie D, Price RB (2016) Characterizing the output settings of dental curing lights. J Dent 44:20–26. https://doi.org/10.1016/j.jdent.2015.10.019
Rueggeberg FA, Giannini M, Arrais CAG, Price RBT (2017) Light curing in dentistry and clinical implications: a literature review. Braz Oral Res 31(suppl 1):e61. https://doi.org/10.1590/1807-3107BOR-2017.vol31.0061
Sim JS, Seol HJ, Park JK, Garcia-Godoy F, Kim HI, Kwon YH (2012) Interaction of LED light with coinitiator-containing composite resins: effect of dual peaks. J Dent 40(10):836–842. https://doi.org/10.1016/j.jdent.2012.06.008
Par M, Marovic D, Skenderovic H, Gamulin O, Klaric E, Tarle Z (2017) Light transmittance and polymerization kinetics of amorphous calcium phosphate composites. Clin Oral Investig 21(4):1173–1182. https://doi.org/10.1007/s00784-016-1880-6
Palin WM, Senyilmaz DP, Marquis PM, Shortall AC (2008) Cure width potential for MOD resin composite molar restorations. Dent Mater 24(8):1083–1094. https://doi.org/10.1016/j.dental.2008.01.001
Moszner N, Fischer UK, Ganster B, Liska R, Rheinberger V (2008) Benzoyl germanium derivatives as novel visible light photoinitiators for dental materials. Dent Mater 24(7):901–907. https://doi.org/10.1016/j.dental.2007.11.004
Ilie N, Bucuta S, Draenert M (2013) Bulk-fill resin-based composites: an in vitro assessment of their mechanical performance. Oper Dent 38(6):618–625. https://doi.org/10.2341/12-395-L
Clewell DH (1941) Scattering of light by pigment particles. J Opt Soc Am 31(8):521–527
Campbell PM, Johnston WM, O’Brien WJ (1986) Light scattering and gloss of an experimental quartz-filled composite. J Dent Res 65(6):892–894
Par M, Gamulin O, Marovic D, Klaric E, Tarle Z (2015) Raman spectroscopic assessment of degree of conversion of bulk-fill resin composites--changes at 24 hours post cure. Oper Dent 40(3):E92–E101. https://doi.org/10.2341/14-091-L
Alshali RZ, Salim NA, Satterthwaite JD, Silikas N (2015) Post-irradiation hardness development, chemical softening, and thermal stability of bulk-fill and conventional resin-composites. J Dent 43(2):209–218. https://doi.org/10.1016/j.jdent.2014.12.004
Jakubiak J, Allonas X, Fouassier JP, Sionkowska A, Andrzejewska E, Linden LÅ, Rabek JF (2003) Camphorquinone–amines photoinitating systems for the initiation of free radical polymerization. Polymer 44(18):5219–5226. https://doi.org/10.1016/s0032-3861(03)00568-8
Leprince JG, Palin WM, Hadis MA, Devaux J, Leloup G (2013) Progress in dimethacrylate-based dental composite technology and curing efficiency. Dent Mater 29(2):139–156. https://doi.org/10.1016/j.dental.2012.11.005
Neumann MG, Schmitt CC, Ferreira GC, Corrêa IC (2006) The initiating radical yields and the efficiency of polymerization for various dental photoinitiators excited by different light curing units. Dent Mater 22(6):576–584
Price RB, Felix CA (2009) Effect of delivering light in specific narrow bandwidths from 394 to 515nm on the micro-hardness of resin composites. Dent Mater 25(7):899–908. https://doi.org/10.1016/j.dental.2009.01.098
Arikawa H, Fujii K, Kanie T, Inoue K (1998) Light transmittance characteristics of light-cured composite resins. Dent Mater 14(6):405–411
Neumann MG, Miranda WG Jr, Schmitt CC, Rueggeberg FA, Correa IC (2005) Molar extinction coefficients and the photon absorption efficiency of dental photoinitiators and light curing units. J Dent 33(6):525–532. https://doi.org/10.1016/j.jdent.2004.11.013
Gomes M, DeVito-Moraes A, Francci C, Moraes R, Pereira T, Froes-Salgado N, Yamazaki L, Silva L, Zezell D (2013) Temperature increase at the light guide tip of 15 contemporary LED units and thermal variation at the pulpal floor of cavities: an infrared thermographic analysis. Oper Dent 38(3):324–333. https://doi.org/10.2341/12-060-L
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Par, M., Repusic, I., Skenderovic, H. et al. Wavelength-dependent light transmittance in resin composites: practical implications for curing units with different emission spectra. Clin Oral Invest 23, 4399–4409 (2019). https://doi.org/10.1007/s00784-019-02896-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-019-02896-y