
Abstract
Low persistence with osteoporosis medication is associated with higher fracture risk. Previous studies estimated that 1-year persistence with osteoporosis medication is low. Our aim was to study persistence with osteoporosis medication among patients with long-term follow-up (to 5 years). The InterAction Database (IADB) was used to analyze persistence of 8610 Dutch patients initiating osteoporosis drugs between 2003 and 2011. Drugs under study were alendronate, risedronate, ibandronate, etidronate, raloxifene and strontium ranelate. Cumulative persistence rates were calculated after different time frames (3 months–5 years) using survival analysis. Multivariate Cox proportional hazard analyses were used to identify determinants of non-persistence. Furthermore, switching rates of persistent patients who initiated bisphosphonate therapy were analyzed. Persistence with osteoporosis therapy was 70.7 % (95 % CI, 69.7–71.7), 58.5 % (95 % CI, 57.4–59.6 %), 25.3 % (95 % CI, 24.1–26.5) after 6 months, 1 and 5 years, respectively. Determinants associated with higher risk to non-persistence within the first year were daily dosing regimen [HR, 1.76 (95 % CI, 1.46–2.14)], age <60 years [HR, 1.26 (95 % CI, 1.19–1.34)] and use of glucocorticoids [HR, 1.16 (95 % CI, 1.07–1.26)]. Monthly dosing schedule and use of generic brands of alendronate did not show a significant association with non-persistence. Approximately 4.0 % of patients initiating therapy with weekly alendronate or weekly risedronate switched therapy. Persistence with osteoporosis medication is low. Because low persistence is strongly associated with higher fracture risk, interventions to improve persistence are recommended. This study identified several patient groups in whom such interventions may be most relevant.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a chronic progressive disease characterized by low bone mass and deterioration of the microarchitecture of bone tissue [1]. Bone loss leads to an increased susceptibility to fractures, in particular those of the hip, spine and wrist [1]. The Dutch population contains approximately 800000 osteoporotic patients [2], predominantly postmenopausal women, resulting in over 80000 osteoporotic fractures per year [3]. Osteoporotic fractures are associated with significant morbidity, mortality and reduced quality of life, resulting in a significant burden to society [4]. Osteoporosis medication, such as bisphosphonates, strontium ranelate and raloxifene, have been approved for prevention and treatment of osteoporosis as they have shown to reduce the risk of osteoporotic fractures by 20–50 % in clinical trials [5]. However, to achieve this desired efficacy in a real-world setting, patients must continue taking their medications (persistence) in accordance with their prescribed dosing regimen (compliance). A meta-analysis demonstrated that non-persistence and non-compliance are associated with an increase of fracture risk by 30–40 % [6], which consequently results in significant higher clinical burden and healthcare costs [7]. Determinants influencing persistence have been described including age, dosing frequency, drug type and adverse events [8, 9].
Previous studies had shown that persistence of patients using osteoporosis medications in the Netherlands is poor. It has been estimated that only 22–68 % of the Dutch patients initiating osteoporosis medications still persists with therapy after 1 year [8–11]. These studies focused on only one or more specific bisphosphonate or used a fixed follow-up period of 12 months. Long-term studies on persistence with osteoporosis therapy, however, are absent.
The primary goal of this study was to analyze persistence with oral osteoporosis medication among osteoporotic patients over several years using a Dutch prescription database. A second aim was to identify determinants of non-persistence, including dosing schedule and drug-type. A third aim was to analyze the switching patterns of persistent users in time.
Materials and methods
Data source
Data were obtained from the IADB.nl database, which holds pharmacy-dispensing data from approximately 500000 individuals in The Netherlands (http://www.IADB.nl/). Each prescription record contains basic patient characteristics and information on drug name, ATC-code (Anatomical Therapeutical Chemical), prescription date, dosage and amount of drug units delivered. The use of over-the-counter drugs and in-patient prescriptions are not included. In the Netherlands, patients generally remain loyal to the same pharmacy [12], which allowed us to retrieve complete medication histories of patients. The IADB database has been validated for drug-utilization studies [13, 14] and has previously been used in persistence studies [15]. Data between January 2003 and December 2011 were used for the analyses.
Study population
We selected all patients aged 18 years or older with a first recording of osteoporosis medication between January 2003 and December 2011. Included osteoporosis medications were: alendronic acid, risedronic acid, ibandronic acid, etidronic acid, raloxifene and strontium ranelate. To select new users, patients were required to be known in the database starting from one year before their first prescription of osteoporosis medication (i.e., initial prescription) and at least six months after initial prescription to ensure that the persistence of the patient could be estimated [16]. Patients were excluded if they had prescriptions of anti-neoplastic medication (except methotrexate), pamidronic acid, or clonidronic acid before or on the day of their initial prescription because they may have been already prescribed osteoporosis medication for the treatment of bone-metastasis or multiple myeloma (Kahler’s disease). In addition, patients with prescriptions of calcitonin, tiludronic acid, or risedronic acid 30 mg daily were excluded since these patients are likely to have been prescribed osteoporosis medication for Paget’s disease.
Persistence
Persistence was defined as the duration of time from initiation to discontinuation of therapy [17]. A patient was considered to be persistent until a permissible gap between two consecutive prescriptions was exceeded [17]. The permissible gap was set at 30 days, the same time-interval as has been frequently used in previous studies [18]. Permissible gaps of 60 days, 90 days and a permissible gap according to the method of Catalan (gap = half of duration of last prescription) were explored in a sensitivity analysis [19]. The Catalan method was used in three previous Dutch studies assessing the persistence of osteoporosis medication [8, 10, 11], thus applying this method allows us to compare our results with those studies. To account for stockpiling, patients were able to cover future gaps with accumulated medication from earlier overlapping prescriptions. Avoiding underestimation of true persistence, switching between the included medications was allowed when establishing persistence status for all treatments combined [20]. Since high-dosed oral glucocorticoid therapy is a well-known secondary cause of osteoporosis, non-persistent patients were censored if they simultaneously discontinued the use of glucocorticoid medication. Patients were also censored when they started receiving medication in prepackaged bags or medication boxes because these patients were not supposed to be able to discontinue without intervention of a physician.
Determinants of non-persistence
Dosing regimen and type of osteoporotic medication were the main determinants in this study. Differences in persistence were analyzed compared to a reference regimen or drug and results were adjusted for age, gender, year of therapy initiation, use of gastroprotective medication during 6 months after therapy initiation and glucocorticoid exposure 1 year prior to therapy initiation.
Switching
Treatment switching was defined as initiation of therapy with another of the included osteoporosis medications within the permissible gap [20]. Switching patterns of weekly alendronate and weekly risedronate were analyzed as well as the probability of switching in time. We limited this analysis to these drugs only because they are the first choice drugs according to the Dutch treatment guidelines [3].
Statistical analysis
Persistence estimates were derived using life-tables with discontinuation considered as an event. Patients without an event were censored at the last day known in the database. Cumulative proportions of persistent patients and their confidence intervals were estimated after time-frames varying from 3 months till 5 years. Differences in persistence were displayed using Kaplan–Meier plots and tested using the Log-rank test and Cox Proportional Hazard analysis. All statistical analyses were performed using PASW Statistics (SPSS), version 18.0.3 (Chicago, IL, USA).
Results
Baseline characteristics
We identified 9551 incident users of the included osteoporosis medications. Of these, 308 patients (3.2 %) were excluded because of an anti-neoplastic prescription in history and 131 patients (1.4 %) from a prescription of Paget’s disease medication. Another 527 patients (5.5 %) were excluded because their dosing schedule did not meet the regular treatment schedule of osteoporosis. Therefore, the final cohort contained 8610 patients, who had an average age of 67.5 ± 13.5 years and of whom 75.6 % were female (Table 1). Patients predominantly started osteoporosis therapy with bisphosphonates on weekly regimen (94.3 %). At the start of the study period in 2003, 86 % of the patients started with weekly bisphosphonates and this rate increased to 96 % in 2011 (Fig. 1). Consequently, initial prescriptions of daily bisphosphonates decreased in time from 12.9 % in 2003 to 0.7 % in 2011. Regarding drug type, most prescribed drugs were alendronate weekly (57.6 %) and risedronate weekly (36.7 %). Since generic forms of alendronate became available on the market in 2005, more patients started with this drug, up to 62 % in 2011. Less initial prescribed anti-osteoporotic drugs were raloxifene (0.3 %) and strontium ranelate (0.7 %) (Table 1). In most cases, a general practitioner (GP) was the initial prescriber (52.7 %). Regarding concomitant medication, approximately 62.1 % of the patients used calcium besides osteoporosis medication and 47.9 % vitamin D. Consider that over-the-counter was not included in the database, resulting in a possible underestimation of the actual use of vitamin D. Use of gastric protection increased from 29.7 % of patients before therapy initiation to 45.2 % of patients after initiation.

Distribution of initial osteoporosis drug prescriptions for the full study population distributed by calendar year
Persistence
Cumulative persistence rates for the total population and gender-specific rates are presented in Table 2. For the full cohort, persistence was 70.7 % (95 % CI, 69.7–71.7 %) after 6 months and decreased to 58.5 % (95 % CI, 57.4–59.6 %), 37.8 % (95 % CI, 36.7–39.0 %), 25.3 % (95 % CI, 24.1–26.5 %) after 1, 3 and 5 years, respectively. Median time on treatment (time at which cumulative persistence rate is equal to 50 %) was 597 days. A crude analysis of the gender-specific data showed a difference between women and men (log-rank test, p < 0.001).
Determinants of non-persistence are shown in Table 3. A multivariate analysis showed that users on a daily regimen are more likely to be non-persistent than those who initiated bisphosphonates on a weekly regimen [HR, 1.76 (95 % CI, 1.46–2.14)]. No significant difference was found between a weekly and a monthly dosing schedule of bisphosphonates [HR, 0.96 (95 % CI, 0.71–1.30)]. Regarding specific drugs, the branded form of weekly risedronate showed the highest persistence rate after 1 year (58.5 %) and strontium ranelate showed the lowest (27.3 %). No difference was found when the generic form of weekly alendronate was compared to the branded form of weekly alendronate [Hazard ratio (HR), 1.00 (95 % CI, 0.89–1.12)] or weekly risedronate branded [HR, 0.92 (95 % CI, 0.84–1.01)]. Younger patients were more likely to be non-persistent [<40 years: HR, 2.30 (95 % CI, 1.95–2.66); 41–50 years: HR, 1.65 (95 % CI, 1.43–1.90); 51–60 years: HR, 1.15 (95 % CI, 1.03–1.28)].
Overall, patients below 60 years of age were 1.26 (95 % CI 1.19–1.34) times more likely to be non-persistent.
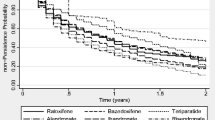
Kaplan–Meier plots of various drug-types and regimens are shown in Fig. 2. The crude analysis of long-term persistence among bisphosphonate users showed a significant difference between daily and weekly regimen (log-rank test, p < 0.001), but no difference between a weekly and a monthly regimen (log-rank test, p = 0.661).

Persistence over time by dosing regimen (a) and by drugtype (b)
In scenario analysis, varying the length of gap to 60 days, 90 days and gap according to Catalan’s method did not highly alter results. After 1 year, the persistence rate was 5.7 % higher using a gap of 60 days as compared with 30 days [64.2 % (95 % CI, 63.1–65.2 %) vs. 58.5 % (95 % CI, 57.4–59.6 %)] and 8.7 % higher using a 90 day-gap [67.2 % (95 % CI, 66.1–68.2 vs. 58.5 % (95 % CI, 57.4–59.6 %)]. A permissible gap according to Catalan’s method showed no significantly different persistence rates as compared with a 30 days gap [56.6 % (95 % CI, 55.5–57.6) vs. 58.5 % (95 % CI, 57.4–59.6 %)].
Switching
Switching behavior was defined as continuing osteoporosis therapy with another drug within the permissible gap. From the 4961 initial users of alendronate weekly, a total of 196 patients (4.0 %) switched therapy, in most cases to risedronate (65 %) and ibandronate (21 %) (Table 4).
A number of 133 of the 3156 initial weekly risedronate users (4.2 %) switched osteoporosis therapy, predominantly towards alendronate (68 %) and ibandronate (19 %). Approximately 60 % of switches took place in the first half year after initiation of either alendronate or risedronate therapy.
Discussion
Treatment persistence
In this study we analyzed persistence with osteoporosis medication among newly-treated osteoporotic patients in a retrospective database. We found that persistence with osteoporosis therapy is low, having 58.5 % of patients still on therapy after 1 year. Previous Dutch studies also showed low persistence rates after 1 year varying between 36.5 and 43.6 % [8–10]. A difference between our study and those studies is that we focused explicitly on osteoporosis patients instead of all new users of osteoporosis medication. We excluded patients who might have been prescribed osteoporosis therapy for Kahler’s disease or bone metastasis. Moreover, we censored patients who discontinued osteoporosis medication simultaneously with glucocorticoid use (which is a valid reason for discontinuing osteoporosis medication), patients switching towards parenteral given osteoporosis medications and patients receiving medications automatically in prepackaged bags. Hereby, non-persistent patients discontinuing with a valid reason were not marked as an event resulting in a more realistic reflection of real-life persistence as compared to previous studies. This may explain why the persistence rates of our study were approximately 15–20 % higher than previous Dutch studies. We chose to investigate persistence in a real-life setting to make our results more applicable to cost-effectiveness studies estimating the clinical effects and costs of non-persistence among osteoporosis patients.
One previous Dutch study, which was performed in multiple Dutch pharmacies, also corrected for simultaneously discontinuation with glucocorticoids [11]. They found a slightly higher 1-year persistence rate than we did (68.3 vs. 58.5 %). This study was conducted in a smaller group of patients (n = 408) from a selected group of pharmacies.
The decreasing trend of persistence with osteoporosis therapy continues after 1 year. Previous Dutch studies had follow-up periods of mostly 1 year with a maximum of 2 years. Our results showed a gradually decrease of persistence up to the maximum follow-up period of 5 years. Studies performed outside The Netherlands studying long-term persistence with osteoporosis therapy showed similar decreasing trends and our study confirmed this trend for the Dutch situation [16, 20].
Persistence rates were fairly insensitive to the length of permissible gap, because increasing the gap from 30 to 90 days changed the persistence rate with only 9 percentage units after 1 year follow up. Moreover, a study of Netelenbos et al. [9] showed that compliance of Dutch patients with osteoporosis therapy is high, because 91 % of patients had a medication possession ratio (MPR) >80 %. This means that patients in the Netherlands generally have small gaps between filled prescriptions.
Determinants of persistence
In line with previous Dutch studies, persistence with bisphosphonates on a weekly regimen was higher as compared with a daily regimen [8, 9]. However, we found no difference between a weekly and monthly regimen. Concerning the comparison of persistence between weekly and monthly bisphosphonates, results in literature vary. Some studies suggested that persistence of monthly ibandronate was higher than weekly alendronate and risedronate [16, 21–23], whereas another study found similar persistent rates between those drugs [9]. Our study confirmed the results of the latter study [9]. This suggests that a further reduction of dosing frequency from weekly to monthly does not necessarily lead to a further improvement of persistence.
This is the first Dutch study that made a distinction between branded and generic forms of weekly alendronate. Previous studies related generic forms of alendronate with lower persistence rates as compared with branded alendronate [24–26]. Our results did not support this relation as we found no different persistence rate for branded and generic alendronate. In the Netherlands, a preference policy is used in which health insurance companies only reimburse the cheap generic form of drugs. Our results demonstrate that this policy does not increase the risk of non-persistence for alendronate. Strontium ranelate showed the lowest persistence rates, which may be mainly caused by its daily dosing regimen. Another possible explanation attributing to its low persistence is the warning by European Medicines Agency (EMEA) on the Drug Reaction (or Rash) with Eosinophilia and Systemic Symptoms (DRESS) syndrome in 2007 associated with two lethal events, which had some media attention [27].
As expected and reported by others, younger patients (age <60) and patients using glucocorticoids previous to therapy initiation have lower persistence rates [8, 9]. Use of gastric protection after therapy initiation did not alter persistence, although experiencing side-effects is a commonly cited reason for discontinuation [11, 28]. However, on the other hand, the gastric protection might treat gastrointestinal side-effects successfully.
Switching patterns
Switching behavior was assessed only for weekly alendronate and weekly risedronate because these drugs are the first choice for naïve osteoporosis patients according to Dutch guidelines of osteoporosis treatment [3]. About 4 % of total starters switched to another anti-osteoporotic drug. This is in the same order as Landfeldt et al. [29] who studied switching behavior in Sweden using similar methodology finding switching rates of 1.69 and 5.66 % for alendronate and risedronate, respectively. As expected, patients predominantly switched in the first six months, generally when they experience side-effects for the first time. Of switching patients, most patients switched between alendronate and risedronate because these drugs are stated as the first choice in the Dutch guidelines of osteoporosis treatment. No notable switch from risedronate to alendronate was noticed, although generic variants became available within the time-period of this study.
Limitations
Our study has several limitations. First of all, our database contained no information on drug indication. Therefore, we had to use proxies to exclude patients who might have used osteoporosis medications for the treatment of Paget’s disease, Kahler’s disease or bone-metastasis. These diseases often require medications only administered in a hospital, but the database we used did not contain in-hospital prescriptions. Therefore, it cannot be ruled out that our study cohort contained patients who received osteoporosis medication with a different indication than osteoporosis. Lack of information about in-hospital prescriptions can also lead to a gap in patient’s medication history when admitted to hospital. However, nowadays patients with fractures are usually not hospitalized for longer than two weeks which is shorter than the permissible gap used in this study [30]. Still, patients may be hospitalized for comorbid conditions and remain in hospital for longer periods. Second, prescription data do not necessarily reflect the actual drug use, although validation studies showed good correlation between prescription claims and actual drug use [31, 32]. Third, no information about the reason for discontinuing was available. Therefore, the study population might contain non-persistent patients who discontinued drug therapy in line with their physicians advice. Fourth, our database doesn’t contain information about Bone Mineral Density (BMD) scores, previous fractures, comorbidities and urbanization density around pharmacies. These factors were previously reported as possible determinants of persistence [8, 21, 28]. Also an association between persistence and the use of calcium and/or vitamin D was reported [9]. However, our database contains no information on over the counter medication or drugs obtained outside the pharmacy. Therefore, we decided to neglect use of calcium and vitamin D as possible determinanst. As we identified age, gender and use of glucocorticoids prior to osteoporosis therapy as confounders in our study, we corrected our results for these parameters only.
Lastly, caution is required for the interpretation of persistence rates of osteoporosis medication other than weekly bisphosphonates as the number of patients using this type of drugs is relatively low.
Clinical implications and recommendations
Osteoporosis is a chronic disease, which needs a long-term treatment. However, therapy only succeeds if patients continue taking their medication because non-persistence is associated with a higher risk of osteoporotic fractures [10]. In the Netherlands, the recommended duration of treatment of osteoporosis with bisphosphonates is 5 years, but can also be continued under certain circumstances [3]. Multiple studies, including our study, demonstrate that persistence with osteoporosis medications in the Netherlands is low and a substantial proportion of patients discontinue within the first year. Furthermore, our study demonstrates that this decreasing trend remains over a long-term follow up, indicating the need for interventions to improve persistence. Healthcare professionals already have developed and evaluated several interventions, primarily based on the provision of extra information, dosing frequency, on a more individual approach of patients, including reminder letters or phone calls and patient support by healthcare professionals [11, 33]. Preferably, national implementation of these interventions should focus on those which are not only effective but also cost-effective [34].
Conclusion
Persistence to treatment of osteoporosis therapy is poor among naïve-treated patients because approximately 60 % are still on therapy after 1 year and 25 % after the recommended treatment duration of 5 years. Interventions are needed to improve persistence as low persistence is associated with higher fracture risk.
References
Anonymous (1993) Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosis. Am J Med 94:646–650
Picavet HSJ (2004) Osteoporose en osteoporotische fracturen: omvang en gevolgen. [in Dutch]
Kwaliteitsinstituut voor de gezondheidszorg CBO (2011) Richtlijn Osteoporose en fractuurpreventie derde herziening. Utrecht [in Dutch]
Lips P, van Schoor NM (2005) Quality of life in patients with osteoporosis. Osteoporos Int 16:447–455
National Institute for Health and Clinical Excellence (NICE) (2010) Systematic reviews of clinical effectiveness prepared for the guideline ‘Osteoporosis: assessment of fracture risk and the prevention of osteoporotic fractures in individuals at high risk’. 2008
Ross S, Samuels E, Gairy K, Iqbal S, Badamgarav E, Siris E (2011) A meta-analysis of osteoporotic fracture risk with medication nonadherence. Value Health 14:571–581
Hiligsmann M, Rabenda V, Bruyère O, Reginster J (2010) The clinical and economic burden of non-adherence with oral bisphosphonates in osteoporotic patients. Health Policy 96:170–177
Penning-van Beest FJA, Goettsch WG, Erkens JA, Herings RMC (2006) Determinants of persistence with bisphosphonates: a study in women with postmenopausal osteoporosis. Clin Ther 28:236–242
Netelenbos JC, Geusens PP, Ypma G, Buijs SJE (2011) Adherence and profile of non-persistence in patients treated for osteoporosis–a large-scale, long-term retrospective study in The Netherlands. Osteoporos Int 22:1537–1546
van den Boogaard CHA, Breekveldt-Postma N, Borggreve SE, Goettsch WG, Herings RMC (2006) Persistent bisphosphonate use and the risk of osteoporotic fractures in clinical practice: a database analysis study. Curr Med Res Opin 22:1757–1764
Stuurman A, Hiddink E (2010) Pharmaceutical care interventions, initiated by computerized drug prescription monitoring, improve drug compliance [article in Dutch]. PW Wetenschappelijk Platform 4:128–135
Leufkens HG, Urquhart J (2006, 2007) Automated Pharmacy Record Linkage in The Netherlands. In: Anonymous (eds) Pharmacoepidemiology. Wiley, New York, pp 311–322
Tobi H, van den Berg P, de Jong-van den Berg L (2000) The InterAction Database: synergy of science and practice in pharmacy. In: Brause R, Hanisch E (eds) Medical data analysis. Springer, Berlin, pp 93–108
Schirm E, Monster TB, de Vries R, van den Berg PB, de Jong-van den Berg LT, Tobi H (2004) How to estimate the population that is covered by community pharmacies? An evaluation of two methods using drug utilisation information. Pharmacoepidemiol Drug Saf 13:173–179
Vegter S, Nguyen NH, Visser ST, de Jong-van den Berg LT, Postma MJ, Boersma C (2011) Compliance, persistence, and switching patterns for ACE inhibitors and ARBs. Am J Manag Care 17:609–616
Li L, Roddam A, Gitlin M, Taylor A, Shepherd S, Shearer A, Jick S (2012) Persistence with osteoporosis medications among postmenopausal women in the UK General Practice Research Database. Menopause 19:33–40
Cramer JA, Roy A, Burrell A, Fairchild CJ, Fuldeore MJ, Ollendorf DA, Wong PK (2008) Medication compliance and persistence: terminology and definitions. Value Health 11:44–47
Rabenda V, Hiligsmann M, Reginster JY (2009) Poor adherence to oral bisphosphonate treatment and its consequences: a review of the evidence. Expert Opin Pharmacother 10:2303–2315
Catalan VS, LeLorier J (2000) Predictors of long-term persistence on statins in a subsidized clinical population. Value Health 3:417–426
Landfeldt E, Strom O, Robbins S, Borgstrom F (2012) Adherence to treatment of primary osteoporosis and its association to fractures–the Swedish Adherence Register Analysis (SARA). Osteoporos Int 23:433–443
Cotte FE, Fardellone P, Mercier F, Gaudin AF, Roux C (2010) Adherence to monthly and weekly oral bisphosphonates in women with osteoporosis. Osteoporos Int 21:145–155
Cooper A, Drake J, Brankin E, PERSIST Investigators (2006) Treatment persistence with once-monthly ibandronate and patient support vs. once-weekly alendronate: results from the PERSIST study. Int J Clin Pract 60:896–905
Weiss TW, Henderson SC, McHorney CA, Cramer JA (2007) Persistence across weekly and monthly bisphosphonates: analysis of US retail pharmacy prescription refills. Curr Med Res Opin 23:2193–2203
Sheehy O, Kindundu CM, Barbeau M, LeLorier J (2009) Differences in persistence among different weekly oral bisphosphonate medications. Osteoporos Int 20:1369–1376
Ringe JD, Moller G (2009) Differences in persistence, safety and efficacy of generic and original branded once weekly bisphosphonates in patients with postmenopausal osteoporosis: 1-year results of a retrospective patient chart review analysis. Rheumatol Int 30:213–221
Strom O, Landfeldt E (2012) The association between automatic generic substitution and treatment persistence with oral bisphosphonates. Osteoporos Int 23:2201–2209
EMEA (2007) EMEA recommends changes in the product information for Protelos/Osseor due to the risk of severe hypersensitivity reactions
Rossini M, Bianchi G, Di Munno O, Giannini S, Minisola S, Sinigaglia L, Adami S, Treatment of Osteoporosis in clinical Practice (TOP) Study Group (2006) Determinants of adherence to osteoporosis treatment in clinical practice. Osteoporos Int 17:914–921
Landfeldt E, Lang A, Robbins S, Strom O (2011) Gastrointestinal tolerability and patterns of switching in patients treated for primary osteoporosis: the Swedish Adherence Register Analysis (SARA). Calcif Tissue Int 89:234–245
(2012) Volksgezondheid Toekomst Verkenning, Nationaal Kompas Volksgezondheid. RIVM, Bilthoven
Enlund H (1982) Measuring patient compliance in antihypertensive therapy–some methodological aspects. J Clin Hosp Pharm 7:43–51
Grymonpre R, Cheang M, Fraser M, Metge C, Sitar DS (2006) Validity of a prescription claims database to estimate medication adherence in older persons. Med Care 44:471–477
Gleeson T, Iversen MD, Avorn J, Brookhart AM, Katz JN, Losina E, May F, Patrick AR, Shrank WH, Solomon DH (2009) Interventions to improve adherence and persistence with osteoporosis medications: a systematic literature review. Osteoporos Int 20:2127–2134
Van Boven JFM, Hiddink EG, Stuurman-Bieze AGG, Postma MJ, Vegter S (2011) Structured medication surveillance for improving adherence to bisphosphonate therapy offers perspectives for cost-effective pharmaceutical care [article in Dutch]. PW Wetenschappelijk Platform 5:160–166
Acknowledgments
This study was funded by a research grant from GlaxoSmithKline.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
van Boven, J.F.M., de Boer, P.T., Postma, M.J. et al. Persistence with osteoporosis medication among newly-treated osteoporotic patients. J Bone Miner Metab 31, 562–570 (2013). https://doi.org/10.1007/s00774-013-0440-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00774-013-0440-2