
Abstract
Horse-racing jockeys are a group of weight-restricted athletes, who have been suggested as undertaking rapid and extreme weight cycling practices in order to comply with stipulated body-mass standards. The aim of this study was to examine bone mass, turnover and endocrine function in jockeys and to compare this group with age, gender and body mass index matched controls. Twenty male professional jockeys and 20 healthy male controls participated. Dual energy X-ray absorptiometry scans and early morning fasting blood and urine samples were used to measure bone mass, turnover and a hormonal profile. Total body bone mineral density (BMD) was significantly lower in jockeys (1.143 ± 0.05 vs. 1.27 ± 0.06 g cm−3, p < 0.01). Bone resorptive activity was elevated in the jockey group as indicated by significantly higher urinary NTx/creatinine (76.94 ± 29.52 vs. 55.9 ± 13.9 nmol mmol−1, p < 0.01), resulting in a significantly negative uncoupling index between bone resorption and formation. Sex hormone binding globulin (SHBG) levels were significantly higher in jockeys (41.21 ± 9.77 vs. 28.24 ± 9.98 nmol L−1, p < 0.01) with a lower percentage of bioavailable testosterone (48.89 ± 7.38 vs. 59.18 ± 6.74 %, p < 0.01). SHBG and insulin-like growth factor-1 were independent predictors of total body and femoral neck BMD, respectively (p < 0.05). In conclusion, it appears that professional jockeys have an elevated rate of bone loss and reduced bone mass that appears to be associated with disrupted hormonal activity. It is likely that this may have occurred in response to the chronic weight cycling habitually experienced by this group.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Professional jockeys are a group of weight-category athletes who engage in a lifestyle of extreme and chronic weight cycling, partaking in acute and severe weight-loss strategies on a regular basis [1–3]. Instead of competing in a specific weight category they must align their body mass with that assigned to the horse they ride in each race. Therefore, these athletes must be prepared to vary their body mass between 52.7 and 64 kg for flat jockeys and between 62 and 76 kg for national hunt jockeys. Flat jockeys compete in races of 5–20 furlongs (1 furlong = 0.201 km) and consist of a run with no obstacles. National hunt races are at least 3.2 km long, throughout which the horse must jump a number of obstacles. Jockeys may compete in as many as 5–7 races per day, over a protracted season lasting 10–12 months, thus having little respite from the physiological strain of “making weight” for competition. Research has suggested that aspects of both physiological and osteogenic function may be affected by the life of chronic weight cycling habitually experienced by these athletes [1, 4].
Previous research suggests that jockeys have reduced bone mass, a finding which was based on DXA derived T scores [3, 4]. Recent data showed markedly lower bone mass in a group of jockeys when compared to an age, gender and body mass index (BMI) matched control group [5]. Lean mass was the primary predictor of bone mass in this study, supporting the suggestion of an allometric relationship between these compartments of body composition [6]. Bone mass was, however, disproportionately low in comparison to lean mass in the flat jockey group, suggesting that additional metabolic or systemic influences may be present which affected bone mass in this jockey group [7]. It is thought that hormonal systems involved in growth and reproduction may be disrupted in times of low energy availability, in an attempt to conserve energy for more immediate and essential processes [8–11]. Hormones such as testosterone, IGF-1, cortisol and vitamin D may all be down-regulated in times of energy deficiency. All of these agents are known to exert varying degrees of control on bone metabolism, both directly via receptor-ligand binding and indirectly through an associated impact on muscular forces and loads [12]. It was hypothesized that a downregulation of hormonal systems such as these, in response to chronically low energy availability [1] may have a role to play in the low bone mass reported in jockeys. Limited information is available, however, regarding endocrine function in jockeys, particularly as it pertains to bone health and development. Accordingly, the aim of the current study was to measure bone mass, turnover and endocrine function in a group of professional jockeys to confirm previous suggestions of abnormally low bone mass and to identify potential endocrine causal mechanisms of this phenomenon.
Materials and methods
Research design overview
Twenty jockeys and 20 age, gender and BMI matched physically active controls participated in this study. All participants were recruited on a volunteer basis following a screening procedure. All participants provided written informed consent prior to participation in this study. Ethical approval for this study was granted by the Dublin City University Research Ethics Committee. Exclusion criteria for this study included any participant with a medical condition or on any medication known to affect either bone health or metabolic function, or anyone who reported having fractured a bone within the previous 12 months. Selection was restricted to male jockeys currently holding a full-time racing license. Selection of control subjects was restricted to healthy males who were recreationally active but did not engage in regular physical training for any particular sport.
Blood and urine sampling and analysis
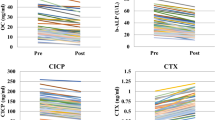
Early morning fasted blood samples were acquired via single venous puncture. Serum was separated and stored at −80 °C until analysis. Urine samples were taken from the second morning void. Albumin, calcium, alkaline phosphatase, creatinine, inorganic phosphorous and magnesium were analysed on the Beckman AU5400 analyser (Beckman Coulter, Ireland). Serum 25(OH) D levels were measured using a commercially available competitive radioimmunoassay kit (Diasorin, Stillwater, USA). Reagents used in conjunction with the ion-selective electrode module of Beckman AU5400 analysers were used for the quantitative determination of the electrolytes: sodium (Na+), potassium (K+) and chloride (Cl−) (Beckman Coulter, Ireland). Cortisol, free thyroxine (free T4), follicle stimulating hormone (FSH), luteinising hormone (LH) and thyroid stimulating hormone (TSH) were analysed using a paramagnetic particle chemiluminescent immunoassay on the Beckman DxI immunoassay system (Beckman Coulter, Ireland). Serum total procollagen type 1 amino terminal propeptide (P-1NP) was analysed by immunoassay on an ELECSYS 2010 analyser (Roche Diagnostics, Ireland). Testosterone was measured by solid phase radioimmunoassay (Spectria, Orion Diagnostica, Finland). Sex hormone binding globulin (SHBG) was measured by solid phase two site chemiluminescent immunometric assay (Immulite 2000, Siemens, USA). Insulin-like growth factor-1 (IGF-1) was measured using a commercially available ELISA kit (R&D Systems Inc, Abingdon, UK). Cross linked N-telopeptides of type 1 collagen (NTx) was measured in the urine using an Osteomark EIA kit on an Etimax analyser (Claymon Biomnis Laboratories, Dublin, Ireland). Assay values were corrected for urinary dilution by urinary creatinine analysis. Creatinine concentration was measured by a kinetic Jaffe method. Urinary NTx/creatinine was expressed in nanomoles of bone collagen equivalents/liter per millimole creatine/liter. An “uncoupling index” between the two markers of bone turnover (serum P1NP and urinary NTx for bone formation and resorption, respectively) was calculated using the formula suggested by Proteau et al. [13]. The Z score for resorption was subtracted from that of formation in order to establish the overall state of bone turnover. A negative score was taken to indicate a bone resorptive state, while a positive score suggests an overall state of bone formation [13]. Free (FT) and bioavailable testosterone (BAT) were calculated according to previously described equations [14].
Bone mass and body composition
Bone mass of the total body, lumbar spine (L2–4) and femoral neck were determined in all participants by dual energy X-ray absorptiometry (DXA) scanning using the GE Lunar Prodigy Advance Scanner (GE Medical Systems, UK). Bone mineral density (BMD) was reported as grams of absolute bone mineral content (BMC) per cm2 of projected bone area (BA). Bone mineral apparent density (BMAD) was calculated to provide an estimation of volumetric bone density (g cm−3), using previously described equations [15, 16]. In addition, BMC was calculated in accordance with differences in height and lean mass as previously described [17, 18]. This was done in order to examine the proportionality of the allometric relationships which exist between these variables and to provide additional information as to the causes of the differing amounts of bone mass. The relative contributions of fat and lean mass were extrapolated from the results of the total body scan. Height and body mass were measured in a standing position wearing minimal clothing following standardized procedures. BMI, fat mass index (FMI) and lean mass index (LMI) were calculated as weight in kilograms (kg) divided by height in meters squared (kg m−2).
Statistical analysis
All data were analysed using SPSS for Windows, version 17. Normality of data distribution was determined using the Shapiro–Wilk test. Differences between the groups were identified using an independent samples t test or Mann–Whitney U test depending on data distribution. Variables were then entered into a bivariate correlation analysis so to determine whether any significant relationships existed between the variables. Pearson’s product moment was used to determine the strength of the relationship between variables. General linear modelling using a univariate analysis of covariance (ANCOVA) was then used to identify significant covariates to each of the bone mass variables (i.e. BMD, BMC and BA of the total body, lumbar spine and femoral neck). Covariates identified by this analysis were taken to be those variables which had a significant influence on the dependent variable in question. Group was included as a fixed factor in this analysis and any variable previously identified as having a significant association with each of the bone mass variables was included as a potential covariate. Variables identified as being significant covariates to each of the bone mass variables were then entered stepwise into a linear regression model. This model was used to identify the relationship between the significant covariates which best explained or predicted the behaviour of the dependent variables (i.e. the bone mass variables). Regression equations and R2 values were generated from the results of this model. All variables were entered into the correlational and predictive analyses in their log transformed state.
Results
Descriptive data
All descriptive data and anthropometric characteristics are presented in Table 1. Differences between the groups reached significance for height, body mass, fat and lean mass. Groups had comparable levels of body mass and lean mass when assessed relative to height (BMI and LMI).
Bone mass and turnover
All indices of bone mass are presented in Table 2. Compared to the controls, jockeys had significantly lower BMD, bone mineral concentration and bone area at all measured sites. Calculation of BMAD showed that the jockey group had significantly lower lumbar spine (L2–4) but not femoral neck BMAD. Bone mass results were then calculated in accordance with differences in height and lean mass, in order to identify underlying causal mechanisms for the low bone mass results reported in the jockeys group. Significant differences between the groups were removed when BMC was adjusted for height (g cm−3), showing that a degree of the variation in bone mass may be accounted for by differences in height between the groups. Significant differences were, however, shown between the groups in relation to total body and lumbar spine BMC expressed relative to lean mass (g kg−1), suggesting additional underlying systemic or metabolic causes of low bone mass in the jockey group.
Control participants showed a greater absolute bone area in terms of cm2. Calculation of bone area relative to height, however, showed that the jockey group had a greater bone area per m2 of height than did the control participants, showing that the jockeys had wider bones relative to height than their control counterparts.
Markers of bone turnover, along with micronutrient and electrolyte information are presented in Table 3. Bone resorption was shown to be elevated in the jockey group as evidenced by significantly increased urinary NTx and NTx/creatinine. In addition calculation of an uncoupling index (UI) between markers of bone formation and resorption showed that the value of the UI was significantly greater in the control group. The negative value of the UI in the jockey group indicated a bone metabolic balance in favour of a bone resorptive state, while the reverse appeared to be true of the control group. No differences were shown in serum concentrations for any of the analysed micronutrients or electrolytes. It has been suggested that individuals should be identified as vitamin D deficient at a 25 (OH) D level of 50 nmol L−1 [19]. Mean serum 25(OH) D levels were below this recommended threshold in the jockey group, however, this finding was not shown to be statistically significant and subsequent analysis revealed 25 (OH) D levels to be unrelated to bone mass at any site.
Endocrine information
Hormonal data are presented in Table 4. SHBG was significantly elevated in the jockey group (p < 0.01), a finding which caused a subsequent reduction in the percentage of total testosterone available in its biologically active free or bioavailable form (p < 0.01). Correlational and predictive analyses identified SHBG as one of the primary independent predictors of total body and lumbar spine BMD available (Tables 5, 6). Lower IGF-1 levels were identified in the jockey group (p = 0.07) and IGF-1 was shown to be independently predictive of femoral neck BMD and BMC (Table 6). A positive correlation was identified between SHBG and the bone resorption marker urinary NTx (r = 0.341, p = 0.036) and between IGF-1 and the bone formation marker serum P1NP (r = 0.347, p = 0.030). Luteinising hormone (LH), although not significantly different between the groups, showed a significantly negative association (p < 0.05) with L2–4 BMD, L2–4 BMC and femoral neck BMC, with r values of −0.488, −0.380 and −0.326, respectively. Table 5 shows all partial correlations of measured indices with the bone mass variables and significant covariates of each as assessed through general linear modelling. Predictive equations generated using the results of the stepwise linear regression model and associated R 2 values are presented in Table 6.
Discussion
Results from this study confirm that jockeys exhibit reduced bone mass [3–5] and an altered hormonal profile when compared to age, gender and BMI matched controls. While lean mass and height were the primary determinants of bone mass, a number of hormonal systems were shown to be disrupted in the jockey group, with SHBG and IGF-1 appearing to be the primary endocrine determinants of bone mass in this study. These abnormalities appeared to be associated with an increased rate of bone turnover and lower bone mass in the jockey group. Down-regulation of anabolic hormonal systems and an associated reduction in bone accrual and mass is likely to be related to the life of chronic weight restriction and energy imbalance previously reported in these athletes [1].
Differences in bone mass were shown to be present between the groups for all absolute variables and the majority of calculated indices (see Table 2). Reduced bone mass is known to increase fracture susceptibility, and this finding may be of particular concern to the horse-racing industry given the high-risk nature of the sport [20]. Adjustments were made to take into account differences in body size and composition, and showed that height and lean mass were the primary anthropometrical determinants of bone mass in this group. Lean mass in particular was shown to be the most influential predictor of bone mass. This finding was expected given the allometric relationship which exists between these body composition compartments and the theory that lean mass and the associated muscular forces which this measure represents may characterize the extent of mechanical loading by which bone is regulated [6, 21]. There was, however, a disproportionate relationship between bone and lean mass in the jockey group (see Table 2), a finding which suggests underlying metabolic or systemic influences on bone mass in this group [7]. This theory was confirmed through examination of the hormonal profile of the jockey group.
An interesting anthropometrical finding in this study was that the jockey group appeared to have a greater cross-sectional bone area than the control participants once the influence of height was accounted for, showing wider bones relative to height in the jockey group. This finding is in agreement with previous research in jockeys [5]. Periosteal dimensions have been shown to be increased in athletes who participate in high intensity sports [22] and it is possible that extended participation in sport may have caused an increase in periosteal apposition in the jockey group. Mineral accrual appeared to lag behind periosteal apposition, however, resulting in the low BMD values reported within the current study. This finding suggests that nutritional, rather than biomechanical factors may have caused the low bone mass findings reported in these athletes, a suggestion which is supported by the accompanying endocrine information reported in this study.
Calculation of an uncoupling index between the bone formation marker serum P1NP and a marker of resorption (urinary NTx) suggest that jockeys have an elevated rate of bone loss with the balance of bone turnover skewed toward excess resorption, causing an associated increase in fracture risk [23]. Low bone mass, accompanied by an elevated rate of bone loss in this group of young athletes may increase susceptibility to osteoporosis in later life, as development of this condition is primarily determined by the level of peak bone mass achieved [24] and the subsequent rate of bone loss [25]. Waldron-Lynch et al. [26] previously reported an elevation of both bone resorption and formation in jockeys [26], but this study did not appear to have calculated an uncoupling index and so the overall balance of bone turnover is unknown. In addition, only those 11 jockeys who had the lowest reported BMD from a larger sample of 27 were evaluated, suggesting a marked selection bias toward those with the lowest initial BMD [26]. The sample of jockeys therefore in our study is likely to reflect more accurately the bone health of the Irish professional jockey.
Results from the examination of a number of key micronutrients and electrolytes were unremarkable (see Table 3). Mean jockey 25(OH) D levels were below the threshold of 50 nmol L−1, a level at which deficiency is diagnosed [19] (43.9 ± 15.5 nmol L−1). 25 (OH) D levels were taken to provide an indication of vitamin D nutritional status. An apparent deficiency in vitamin D status as suggested by these results may impact on calcium resorption, bone mass and bone turnover [27]. 25(OH) D levels were not, however, shown to be significantly different between the groups, nor did subsequent analysis show it to be a predictor of any of the bone mass variables and so it is unlikely that this finding is a significant contributory factor to the differences in bone mass reported in the current study.
Endocrine hormones and factors related to nutrition, metabolism and bone are known to be affected during times of reduced energy availability [9, 10, 28]. In this study we noted that levels of SHBG, a plasma glycoprotein which binds to and decreases the bioavailability of testosterone and estrogen [29] was significantly elevated in the jockey group. Elevated SHBG has previously been reported to play a role in age-associated muscle and bone loss [30], likely through a reduction in the amount of free and BAT present. Elevated SHBG levels in the current study were accompanied by a significant reduction in the percentage of free and BAT present. Further statistical analysis revealed SHBG as one of the primary determinants of total body and lumbar spine BMD, suggesting that depressed activity of free testosterone on bone may have a mechanistic role in the development of low BMD in jockeys. Serum estrogen levels are also known to exert an influence on bone mass in males as well as females [30]. Total and bioavailable estrogen levels were not examined within the current study; however, it is possible that SHBG may have exerted an influence through regulating the action of both of these sex steroids. Further research may be required so to examine this issue. IGF-1 is a pleiotropic growth factor involved in the processes which link nutrition and growth [31] and appears to exert an anabolic influence on virtually all body tissues [32]. It has been suggested as being a relevant indicator of integrated growth hormone secretion and function [33, 34]. In addition, IGF-1 is known to be involved in the regulation of bone mass [31, 35] and it is thought to be involved in the mediation of the complex coupling process of bone remodelling [36, 37]. Statistical analysis in the current study showed IGF-1 to be a primary predictor of femoral neck BMD and concentration (see Table 6). Although differences in serum IGF-1 levels between the groups did not reach statistical significance, a trend toward lower IGF-1 was identified in the jockey group (p = 0.07). Given its presence as a significant predictor of femoral neck BMD and BMC, and previous research which reports that IGF-1 levels may be reduced in times of low energy availability [10, 11], it is thought that this finding may be of clinical relevance in this group. This finding is partially supported by the work of Garnero et al. [23], who identified significant relationships between serum IGF-1 and BMD of the total body and hip but not of the lumbar spine [38]. The apparent site-specific impact of IGF-1 on bone may be related to the cortical content of the bone area in question. It has been suggested that liver derived IGF-1 may exert a systemic influence on cortical periosteal bone growth but not on maintenance of trabecular bone in mice [39].Further research is required in order to more fully evaluate the impact of IGF-1 on bone in this group. A number of statistically significant, albeit weaker correlations were also shown which support the primary findings of this study. The pituitary gonadotropins LH and FSH are thought to act primarily as regulatory agents in a number of anabolic and reproductive processes, potentially through a mediatory effect on SHBG levels [39]. LH showed a significant and negative association (p < 0.05) with lumbar spine BMD (r = −0.488), lumbar spine BMC (r = −0.380) and femoral neck BMC (r = −0.326). In addition further evidence of the apparent catabolic role of SHBG and anabolic role of IGF-1 were provided by the significantly positive association shown between SHBG and the bone resorption marker urinary NTx (r = 0.341, p = 0.036) and between IGF-1 and the bone formation marker P1NP (r = 0.347, p = 0.030). These findings support the suggestion that alterations to metabolic and gonadal hormones and factors within the jockey group may have affected bone mass regulation.
The “female athlete triad” refers to an inter-relationship between energy availability, menstrual function and BMD, which has severe clinical manifestations including eating disorders, functional hypothalamic amenorrhea and osteoporosis [40]. Although more commonly associated with female athletes, results from previous studies showing low energy availability in jockeys [1], along with evidence from the current study of alterations to gonadal and reproductive hormone function, and low bone mass, indicate that male athletes may also be susceptible to this condition.
There are a number of limitations associated with our study which may have affected interpretation of the results. Results are based on single serum samples and so cannot provide information on the pulsatile effect of hormonal activity. Frequent blood sampling so to allow examination of the pulsatile release of studied hormones may provide a more in depth analysis of possible adjustments to endocrine function in jockeys. In addition, examination of a broader range of associated factors, such as adipose derived hormones, e.g. adiponectin and leptin, may allow a more complete analysis to be made. Inferences have been made within this study as to the nutritional habits of the jockey group which are based on previous data [1–3]. Measurement of endocrine and bone data with a concurrent nutritional and physical activity analysis may lend support to assumptions made. A body mass and stature matched control group may have aided in the isolation and identification of hormonal factors specifically related to bone mass in jockeys. The practical limitations of recruiting a non-athletic control group of this mass and stature rendered this difficult, however, and recruitment of a BMI matched control group was deemed as the only reasonable alternative.
In conclusion, the jockey group in this study showed low bone mass along with an apparent bone turnover state in favour of resorption. Adaptations to a number of reproductive and anabolic endocrine agents, in particular SHBG and IGF-1 seem to be related to the low bone mass reported in this group and may be a contributory factor in this finding. It is thought that disturbances to reproductive and anabolic processes may occur in an attempt to conserve energy within this group for more immediately essential metabolic processes. In order to identify more precise mechanistic explanation for the trends identified in the current study further research may be required so to more fully elucidate the potential impact of a severe and chronically weight restricted lifestyle on homeostatic and osteogenic function in this group.
References
Dolan E, O’Connor H, O’Loughlin G, McGoldrick A, Warrington G (2011) Nutritional, lifestyle and weight-control practices of professional jockeys. J Sports Sci 29:791–799
Moore JM, Timperio AF, Crawford DA, Cameron-Smith D (2002) Weight management and weight loss strategies of professional jockeys. Int J Sport Nutr Exerc Metab 12:1–13
Leydon MA, Wall C (2002) New Zealand jockeys’ dietary habits and their potential impact on health. Int J Sport Nutr Exerc 12:220–237
Warrington GD, Dolan E, McGoldrick A, McEvoy J, MacManus C, Griffin M, Lyons D (2009) Chronic weight control impacts on physiological function and bone health in elite jockeys. J Sports Sci 27:543–550
Dolan E, Crabtree N, McGoldrick A, Ashley DT, McCaffrey N, Warrington GD (2011) Weight regulation and bone mass: a comparison between professional jockeys, elite amateur boxers and age. gender and bmi matched controls. J Bone Miner Metab. doi:10.1007/s00774-001-0297-1
Frost HM (2003) Bone’s Mechanostat: A 2003 Update. Anat Rec Part A 275:1081–1101
Cure–Cure C, Capozza RF, Cointry GR, Meta M, Cure-Ramirez P, Ferretti JL (2005) Reference chart for the relationships between dual energy X-ray absorptiometry assessed bone mineral content and lean mass in 3,063 healthy men and premenopausal and postmenopausal women. Osteoporos Int 16:2095–2106
De Souza MJ, Williams NI (2004) Physiological aspects and clinical sequelae of energy deficiency and hypoestrogenism in exercising women. Human Reprod Update 10:433–448
Loucks AB, Thuma JR (2003) Luteinizing hormone pulsatility is disrupted at a threshold of energy availability in regularly menstruating women. J Clin Endocrinol Metab 88:297–311
Haspolat K, Ece A, Gurkan F, Atamer Y, Tutanc M, Yolbas I (2007) Relationship between leptin, insulin, IGF-1 and IGFBP3 in children with energy malnutrition. Clin Biochem 40:201–205
Misra M, Miller KK, Bjornsen J, Hackman A, Aggarwal A, Chung J, Ott M, Herzog DB, Johnson ML, Klibanski A (2003) Alterations in growth hormone secretory dynamics in adolescent girls with anorexia nervosa and effects on bone metabolism. J Clin Endocrinol 88:5615–5623
Solomon AM, Bouloux PMG (2006) Modifying muscle mass: the endocrine perspective. J Endocrinol 191:349–360
Proteau S, Pelle A, Collomp K, Benhamou L, Courteix D (2006) Bone density in elite judoists and effects of weight cycling on bone metabolic balance. Med Sci Sports Exerc 38:694–700
Vermeulen A, Verdonck L, Kaufman JM (1999) A critical evaluation of simple methods for the estimation of free testosterone in serum. J Clin Endocrinol Metab 84:3666–3672
Boot AM, de Ridder MAJ, van der Sluis IM, van Slobbe I, Krenning EP, de Muinick Keizer-Schrama SMBF (2009) Peak bone mineral density, lean body mass and fractures. Bone 46:336–341
Kroger H, Kotaniemi A, Vainio P, Alhava E (1992) Bone densitometry of the spine and femur in children by dual energy X-ray absorptiometry. Bone Miner Bone Mineral 17:75–85
Molgaard C, Thomsen BL, Prentice A, Cole TJ, Michaelsen KF (1997) Whole body bone mineral density in healthy children and adolescents. Arch Dis 76:9–15
Prentice A, Parsons TJ, Cole TJ (1994) Uncritical use of bone mineral density in absorptiometry may lead to size-related artifacts in the identification of bone mineral determinants. Am J Clin Nutr 60:837–842
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, Murad MH, Weaver CM, Endocrine Society (2011) Evaluation, treatment and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 96:1911–1930
Waller AE, Daniels JL, Weaver NL, Robinson P (2000) Jockey injuries in the United States. J Am Med Assoc 283:1326–1328
Bass SL, Eser P, Daly R (2005) The effect of exercise and nutrition on the mechanostat. J Musculoskelet Neuronal Interact 5:239–254
Ferry B, Duclos M, Burt L, Therre P, LeGall F, Jaffre C, Courteix C (2011) Bone geometry and strength adaptations to physical constraints inherent in different sports: comparison between elite female soccer players and swimmers. J Bone Miner Metab 29:342–351
Garnero P, Sornay-Rendu E, Claustrat B, Delmas PD (2000) Biochemical markers of bone turnover, endogenous hormones and the risk of fractures in postmenopausal women: the OFELY study. J Bone Miner Res 15:1526–1536
Mora S, Gilsanz V (2003) Establishment of peak bone mass. Endocrinol Metab Clin North Am 32:39–63
Hansen MA, Overgaard K, Riis BJ, Christiansen C (1991) Role of peak bone mass and bone loss in postmenopausal osteoporosis: 12 year study. BMJ 303:961–964
Waldron-Lynch F, Murray BF, Brady JJ, McKenna MJ, McGoldrick A, Warrington G, O’Loughlin G, Barragry JM (2009) High bone turnover in irish professional jockeys. Osteoporos Int 21:521–525
Iuliano Burns S, Wang XF, Ayton J, Jones G (2009) Skeletal and hormonal responses to sunlight deprivation in Antarctic expeditioners. Osteoporos Int 20:1523–1528
Ihle R, Loucks AB (2004) Dose response relationships between energy availability and bone turnover in young exercising women. J Bone Miner Res 19:1231–1240
Kahn SM, Hryb DJ, Nakhla AM, Romas NA (2002) Sex hormone binding globulin is synthesized in target cells. J Endocrinol 175:113–120
Khosla S, Melton LJ, Atkinson EJ, O’Fallon WM, Klee GG, Riggs BL (1998) Relationship of serum sex steroid levels and bone turnover markers with bone mineral density in men and women: a key role for bioavailable estrogen. J Clin Endocrinol Metab 83:2266–2274
Frystyk J, Delhanty PJD, Skjerbek C, Baxter RC (1999) Changes in the circulating IGF system during short term fasting and refeeding. Am J Physiol Endocrinol Metab 40:245–252
Rajaram S, Baylink DJ, Mohan S (1997) Insulin like growth factor binding proteins in serum and other biological fluids: regulation and functions. Endocr Rev 18:801–831
Aimaretti G, Corneli G, Di Somma C, Baldilli R, Gasco V, Rovere S, Migliaretti G, Colao A, Tamburrano G, Lombardi G, Chigo E, Camami F (2005) Different degrees of gh deficiency evidenced by GHRH + arginine test and IGF-1 levels in adults with pituitary disease. J Endocrinolol Invest 28:247–252
Holt RIG, Webb E, Pentecost C, Sonksen PH (2001) Aging and physical fitness are more important than obesity in determining exercise-induced generation of GH. J Clin Endocrinol Metab 86:5715–5720
Nindl BC, Pierce JR, Durkot MJ, Tuckow AP, Kennett MJ, Nieves JW, Cosman F, Alemany JA, Hymer WC (2008) Relationship between growth hormone in vivo bioactivity, the insulin like growth factor 1 system and bone mineral density in young, physically fit men and women. Growth Horm IGF Res 18:439–445
Rubin J, Ackert-Bicknell CL, Zhu L, Fan X, Murphy TC, Nanes MS, Marcus R, Holloway L, Beamer WG, Rosen CJ (2002) IGF-1 regulates osteoprotegerin (OPG) and receptor activator of nuclear factor-kB ligand in vitro and OPG in vivo. J Clin Endocrinol Metab 87:4273–4279
Ueland T (2004) Bone metabolism in relation to alterations in systemic growth hormone. Growth Horm IGF Res 14:404–417
Garnero P, Sornay E, Rendu E, Delmas PD (2000) Low serum IGF-1 and recurrence of osteoporotic fractures in postmenopausal women. Lancet 355:898–899
Sjogren KS, Sheng M, Moverare S, Liu JL, Wallenius K, Tornell J, Isaksson O, Jansson J, Mohan S, Ohlsson C (2002) Effects of liver derived insulin-like growth factor 1 on bone metabolism in mice. J Bone Miner Res 17:342–351
Nattiv A, Loucks AB, Manore MM, Sunborn CF, Sundgot-Borgen J, Warren MP (2007) The female athlete triad: ACSM position stand. Med Sci Sports Exerc 39:1867–1882
Acknowledgments
This research was supported by an unrestricted grant from the Irish Turf Club.
Conflict of interest
The authors have nothing to declare regarding any potential conflicts of interest which may be perceived as prejudicing the impartiality of the research reported.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Dolan, E., McGoldrick, A., Davenport, C. et al. An altered hormonal profile and elevated rate of bone loss are associated with low bone mass in professional horse-racing jockeys. J Bone Miner Metab 30, 534–542 (2012). https://doi.org/10.1007/s00774-012-0354-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00774-012-0354-4