
Abstract
Schizophrenia is currently believed to result from variations in multiple genes, each contributing a subtle effect, which combines with each other and with environmental stimuli to impact both early and late brain development. At present, schizophrenia clinical heterogeneity as well as the difficulties in relating cognitive, emotional and behavioral functions to brain substrates hinders the identification of a disease-specific anatomical, physiological, molecular or genetic abnormality. Mitochondria play a pivotal role in many essential processes, such as energy production, intracellular calcium buffering, transmission of neurotransmitters, apoptosis and ROS production, all either leading to cell death or playing a role in synaptic plasticity. These processes have been well established as underlying altered neuronal activity and thereby abnormal neuronal circuitry and plasticity, ultimately affecting behavioral outcomes. The present article reviews evidence supporting a dysfunction of mitochondria in schizophrenia, including mitochondrial hypoplasia, impairments in the oxidative phosphorylation system (OXPHOS) as well as altered mitochondrial-related gene expression. Abnormalities in mitochondrial complex I, which plays a major role in controlling OXPHOS activity, are discussed. Among them are schizophrenia specific as well as disease-state-specific alterations in complex I activity in the peripheral tissue, which can be modulated by DA. In addition, CNS and peripheral abnormalities in the expression of three of complex I subunits, associated with parallel alterations in their transcription factor, specificity protein 1 (Sp1) are reviewed. Finally, this review discusses the question of disease specificity of mitochondrial pathologies and suggests that mitochondria dysfunction could cause or arise from anomalities in processes involved in brain connectivity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Schizophrenia is a debilitating, chronic neurocognitive disorder affecting mostly young adults with life prevalence of about 1% worldwide. The disorder is characterized by various abnormal cognitive, affective and motor behavioral features. Its main symptoms involve multiple psychological processes, such as perception (hallucinations), ideation, reality testing (delusions), thought processes (loose associations), feeling (flatness, inappropriate affect), behavior (catatonia, disorganization), attention, concentration, motivation (avolition, impaired intention and planning) and judgment. These psychological and behavioral characteristics are associated with a variety of impairments in occupational and social functioning. No single symptom is pathognomonic of schizophrenia; consequently, the disorder is noted for great heterogeneity across individuals and for its variability within individuals over time (Dingman and McGlashan 1986; McGlashan 1988; McGlashan and Fenton 1992). Despite the tremendous advances in science and medicine, schizophrenia clinical heterogeneity as well as difficulties relating brain’s emergent properties to its physiological substrates hinders the identification of disease-specific anatomical, physiological, molecular or genetic abnormalities.
To date, the prevailing hypothesis for the etiology of schizophrenia is that variations in multiple risk genes, each contributing a subtle effect, interact with each other and with environmental stimuli to impact both early and late brain development. This hypothesis integrates data from postmortem, imaging, epidemiological, physiological and biological studies. Among them are associations between schizophrenia and obstetric complications (Cannon et al. 2002), individual experience of internal or external stressors (Phillips et al. 2007; van Winkel et al. 2008; Zubin and Spring 1977), brain morphological and histological abnormalities (Harrison 1999; Jakob and Beckmann 1989; Wright et al. 2000) and altered expression of genes involved in differentiation, migration, myelination, synaptogenesis and cellular energy metabolism (Harrison and Weinberger 2005; Karry et al. 2004; Muir et al. 2008; Prabakaran et al. 2004; Stefansson et al. 2003). Abnormal gene–environmental interaction during development and later in life can be explained by pathobiological mechanisms, which come “on top of the genetic basis” referred to as epigenetic mechanisms (Feinberg 2007). Genes whose activity may be necessary for normal brain function may be silenced by epigenetic changes and vice versa, and this could impact individual’s risk for adverse health outcomes later in life (Tsankova et al. 2007); such a complex pathological interactions can eventually contribute to one of the main features of schizophrenia, the abnormal activity of brain circuits observed by imaging studies. A conceivable mechanism affecting brain circuitry is abnormal intrinsic- or extrinsic-dependent modulation of neuronal activity.
Neuronal activity or neuronal firing rate impinges on the transmission of neurotransmitter, the neuronal net communication and on the consequent intracellular processes and vise versa. It is the core process by which the nervous system adapts to changes in the environment. Neuronal firing governs the interaction between synaptic strength and efficacy, gene expression and protein activity, which leads to changes in neurogenesis, cell migration as well as a slow spatiotemporal dynamic morphogenesis and neuronal plasticity. These processes are associated with learning and memory, as well as with adaptive changes in emotional, cognitive and sensorimotor function, all abnormal in schizophrenia. Mitochondria are the energy source for driving the biochemical processes involved in various cell functions and take part in intracellular Ca2+ homeostasis and in the maintenance of the intracellular ions concentration against the concentration gradient, both fundamental for neuronal activity.
The present article presents evidence for the role of mitochondrial dysfunction in the pathophysiology of schizophrenia. The accumulating data for abnormal brain activity and energy metabolism, dysfunction of mitochondria and specifically the aberrations in the first complex (complex I) of its oxidative phosphorylation system (OXPHOS) in schizophrenia will be reviewed. In addition, evidence for dopamine interaction with mitochondrial respiration via its interaction with complex I as well as for the role of the ubiquitous transcription factor Sp1 in the regulating the expression of complex I subunits, will be presented. Finally, as dysregulation of mitochondrial function has been reported in various neuropsychiatric disorders, the question as to whether mitochondrial impairment displays disease-specific characteristics or is rather a general non-distinguishing secondary pathology will be discussed.
Brain energy metabolism in schizophrenia
Alteration in brain energy metabolism strongly suggests the involvement of mitochondria, the key players in cellular energy production. Indeed, brain imaging studies largely reveal decreased metabolism in the prefrontal cortex, a major anatomical substrate of schizophrenia (Buchsbaum 1990; Buchsbaum and Hazlett 1998; Carter et al. 1998; Hazlett et al. 2000; Manoach et al. 1999; Shenton et al. 2001). Additional brain regions such as temporal and parietal cortices, thalamus, basal ganglia and cerebellum have also demonstrated alterations in brain metabolic rates, although less consistent (Gur et al. 1987; Hazlett et al. 1999; Tamminga et al. 1992). More direct evidence for mitochondrial dysfunction in schizophrenia is provided by imaging studies using phosphorous or hydrogen magnetic resonance spectroscopy (31P-MRS, and 1H-MRS, respectively). Thus, reduced mitochondrial originated high-energy phosphates, such as ATP and phosphocreatine (PCr), was detected in the frontal lobe, the caudate nucleus and the left temporal lobe of schizophrenic patients (Fujimoto et al. 1992; Jayakumar et al. 2006; Jensen et al. 2006; Volz et al. 2000). Regional deficits have been described in additional cellular factors whose metabolism is strongly suggested to be linked to mitochondrial ATP production including, phospholipids, phosphomonoesters (PMEs), inorganic phosphate (Pi) (Fukuzako et al. 1999; Reddy and Keshavan 2003) and N-acetylaspartate (NAA) (Deicken et al. 2000; Harrison and Weinberger 2005; Madhavarao et al. 2003), in neuroleptic-naive, first episode and chronic schizophrenia subjects.
Alterations in brain metabolism in schizophrenia vary with disease state and the predominance of either negative or positive symptoms both during rest or cognitive task performance (Ben-Shachar et al. 2007; Lahti et al. 2001; Potkin et al. 2002; Wolkin et al. 1985). Antipsychotic medication has been shown to partially contribute to altered brain metabolism particularly in the basal ganglia, but less so in other brain regions. Thus, it has been shown that drug-naive schizophrenic patients, both at first episode and when chronically ill, demonstrated reduced blood flow in the prefrontal, associative frontal, parietal and temporal gyri and increased perfusion in the thalamus, cingulate cortex and cerebellum, suggesting that these abnormalities were neither progressive nor a consequence of medication (Andreasen et al. 1997; Gur et al. 1987; Kim et al. 2000; Kishimoto et al. 1998).
Mitochondria and neuronal activity
Mitochondria role in neuronal activity and thereby long-term structural and functional changes, which modulate synaptic connectivity associated with adaptive changes in emotional and cognitive function, are inferred from histochemical evidence demonstrating mitochondria recruitment to location of high-active zones during neurotransmitter release in response to an increase in synaptic activity (Brodin et al. 1999). In addition, it has been shown that mitochondria play a key role in the establishment of neuronal polarity by concentrating at the site of axogenesis (Mattson 1999). This may be relevant to neurite sprouting, elongation and growth cone motility of axons as well as dendrites. More recent studies have shown that the loss of mitochondria from axon terminal in Drosophila results in defective synaptic transmission (Guo et al. 2005; Stowers et al. 2002; Verstreken et al. 2005). Moreover, a role for axonal mitochondria (pre-synaptic) in short-term facilitation (Kang et al. 2008) as well as for dendritic mitochondria (post-synaptic) in morphogenesis and plasticity of spines and synapses (Li et al. 2004) was demonstrated in mice hippocampal slice cultures. Substantial evidence for mitochondrial role in neuronal activity and plasticity is depicted in studies of the visual system in cat and rats, which serves as a paradigm for neuronal plasticity, in as much as anatomical and physiological development can be altered by visual experience (Sherman and Spear 1982). Thus, in rats exposed to complex environments, synaptogenesis and an increase in the volume of the visual cortex are associated with infiltration of new mitochondria and capillaries (Black et al. 1991). In addition, it has been reported that in the visual system several genes encoding mitochondrial OXPHOS complexes (several subunits of cytochrome oxidase, NADH dehydrogenase, ATPase and of cytochrome b) are regulated by neuronal activity, and their expression is correlated with the extent of plasticity in the visual cortex (Hevner and Wong-Riley 1991; Kaminska et al. 1997; Yang et al. 2001). Further support for the role of mitochondria in mediating synaptic activity is ensued from the findings that the inhibition of succinate dehydrogenase, the second complex of the OXPHOS, induces a long-term potentiation of the NMDA-mediated synaptic excitation, which depends on the activation of dopamine D2 receptors (Calabresi et al. 2001). Finally, mitochondrial permeability transition pores and their constituents the porin proteins which have a significant role in diverse cellular processes, including regulation of mitochondrial ATP and calcium efflux, have been found to have a dynamic functional role in amending neuronal activity, learning and synaptic plasticity (Albensi et al. 2000; Weeber et al. 2002). In all, these studies render a growing body of evidence for the important contribution of mitochondria to neuronal activity and thereby both to short-term modulation and to long-term phenomena in brain.
Mitochondria in schizophrenia
Mitochondrial morphometry
Mitochondrial morphological abnormalities in schizophrenia have been demonstrated by microscopic analysis of autopsy specimens. Electron microscopic analyses of postmortem specimens from the anterior limbic cortex and the caudate putamen nucleus showed mitochondrial deformation and reduced density throughout the neuropil in schizophrenic patients (Kung and Roberts 1999; Uranova and Aganova 1989). Mitochondrial size in both dendrites and axon terminals was smaller than normal in drug-off patients and antipsychotic treatment appeared to partially normalize mitochondrial density and volume. A hypoplasia of mitochondria was observed in the substantia nigra pars compacta, but not in the reticulata, in the presynaptic terminals of tyrosine hydroxylase immunoreactive neurons. This was associated with deformed terminals and altered connectivity (Kolomeet and Uranova 1999). In oligodendrocytes, the most affected glial cells in schizophrenia and bipolar disorder, a significant reduction of approximately 33% in both number and volume of their mitochondria was observed in the caudate nucleus and the prefrontal cortex in patients with schizophrenia (Uranova et al. 2001). In astrocytes, a progressive disturbance due to deficits in mitochondria was recently suggested (Kolomeets and Uranova 2009). Despite the small number of patients and the use of postmortem tissue, which may suffer from inherent artifacts due to the process of tissue collection, these structural findings hold potential importance for the involvement of mitochondria in schizophrenia, and are strengthened by the convergence of additional lines of evidence discussed throughout this review article.
Mitochondrial oxidative phosphorylation system
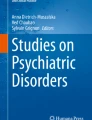
Mitochondria are intracellular organelles that are composed of four functionally specific compartments including the relatively non-selective outer membrane, the intermembrane space, the highly selective inner membrane and its cristae and the matrix. Mitochondria are the “powerhouse” of the cell as they provide ATP, used as a source of chemical energy. In addition to supplying cellular energy, mitochondria are involved in many other cellular processes, such as signaling, cellular differentiation, cell death, as well as the control of the cell cycle and cell growth. In excitatory cells, such as neurons and muscles they are essential for cell activity, firing and contraction, respectively. In addition, the mitochondria have their own DNA (mtDNA), contributing to the mitochondrial proteome, mostly encoded by the nuclear DNA (nDNA). Cellular energy is primarily generated by mitochondrial OXPHOS, a process requiring a coordinated action of four respiratory enzyme complexes arranged in a specific orientation in the inner mitochondrial membrane, termed also the mitochondrial respiratory chain (Fig. 1). Electrons generated from reduced electron carriers NADH and FADH2, produced from oxidation of nutrients, such as glucose, are ultimately transferred through the respiratory chain to molecular oxygen. This process is coupled to proton translocation across the inner membrane forming an electrochemical gradient, which stores energy that is then used for ATP synthesis by the fifth complex, ATP synthase. Each complex of the OXPHOS system consists of multiple components or subunits. Apart from complex II subunits, which are exclusively encoded by the nuclear genome, the subunits of the other four complexes are encoded either by the nDNA, approximately 70 genes, which are randomly distributed over the chromosomes with no obvious clustering, or by the mtDNA which encodes 13 genes.

Schematic representation of the mitochondrial respiratory chain. Electrons, generated from reduced electron carriers NADH and FADH2, produced from oxidation of nutrients such as glucose, are ultimately transferred through the respiratory chain to molecular oxygen. This process is coupled to proton translocation across the inner membrane forming an electrochemical gradient, which stores energy that is then used for ATP synthesis by the fifth complex, ATP synthase. Complex I NADH-ubiquinone oxidoreductase, CoQ coenzyme Q, complex II succinate ubiquinone oxidoreductase, complex III ubiquinonferricytochrome c oxidoreductase, Cyt c cytochrome c, complex IV cytochrome c oxidase, complex V ATP synthase or ATPase
Several groups have studied the enzymatic activity of different complexes of the OXPHOS in schizophrenia postmortem brain specimens. However, functional measurements in postmortem brain specimens have to be taken with reservations, as enzymatic activity is particularly sensitive to postmortem delay (Mizino et al. 1990; Prince et al. 1998), and its detection is less sensitive in whole tissue than in isolated mitochondria. Nevertheless, depending on the brain area studied several groups reported an increase or a decrease as well as no change in cytochrome c oxidase (complex IV) activity (Cavelier et al. 1995; Maurer et al. 2001; Prince et al. 1999), the enzyme which was suggested as an endogenous metabolic marker for neuronal activity (Wong-Riley 1989). Interestingly, another study demonstrated a strong negative correlation between complex IV activity and emotional and intellectual impairments in schizophrenia, but not motor impairment, solely in the putamen (Prince et al. 2000). There are controversial findings regarding the activity of complex I activity in the brains of schizophrenics. A significant reduction in NADH-cytochrome c reductase (complexes I–III) activity was observed in one study in the frontal cortex and in two others in the temporal cortex and in the basal ganglia (Maurer et al. 2001; Prince et al. 1999; Whatley et al. 1996).
Genetic studies also implicate mitochondria abnormalities in schizophrenia. For example, missense variants in mitochondrial DNA (mtDNA), one of which encodes for the ND4 subunit of mitochondrial complex I, are present in schizophrenic patients while absent in healthy controls (Martorell et al. 2006) and an increase in the prevalence of the mtDNA HV lineage cluster in schizophrenia was observed (Amar et al. 2007). Increased number of synonymous base substitution in mtDNA in the prefrontal cortex of schizophrenic patients was recently reported (Rollins et al. 2009). In addition, association studies revealed a significant association of a haplotype, consisting of two SNPs in NDUFV2, a nuclear encoded subunit of complex I, with schizophrenia (Kato et al. 2001; Washizuka et al. 2006). Taken together, these genetic studies suggest complex I as a risk factor in this disorder.
Accumulating molecular data point to abnormalities in mitochondrial mRNA and protein expression, in schizophrenia (Altar et al. 2005; Ben-Shachar 2002; Ben-Shachar et al. 1999; Dror et al. 2002; Karry et al. 2004; Maurer et al. 2001; Middleton et al. 2002; Prabakaran et al. 2004). Studies using transcriptomic, proteomic and metabolomic approaches on human brain tissue, mostly the prefrontal cortex and one study in the hippocampus have demonstrated a specific robust change in gene and protein expression associated with mitochondrial function in schizophrenia (Middleton et al. 2002; Mulcrone et al. 1995; Prabakaran et al. 2004; Shao et al. 2008). The evidence for the alterations in nuclear-encoded mitochondrial gene expression obtained by microarrays is not unequivocal as some studies demonstrated that sample pH as well as statistical complications including multiple comparisons may have a strong effect on the results (Shao et al. 2008; Vawter et al. 2006).
Complex I (NADH: ubiquinone oxidoreductase) in schizophrenia
Among the enzyme complexes that compose the OXPHOS, complex I has the most complex structure (45 subunits) and the least understood mechanism of electron transfer and proton translocation (Hatefi 1985). Complex I plays a major role in controlling oxidative phosphorylation in mitochondria and its abnormal activity can lead to mitochondrial dysfunction (Davey et al. 1998). It is, therefore, not surprising that many human mitochondrial diseases result from complex I deficiencies, including Leber’s hereditary optic neuropathy, severe and fetal lactic acidosis and various neuromuscular myopathies.
Peripheral abnormalities in mitochondrial complex I activity
It was previously suggested that complex I activity is reduced in platelets and lymphocytes of a small sample of schizophrenic patients chronically treated with antipsychotics (Burkhardt et al. 1993; Whatley et al. 1998). We have further substantiated the implication of complex I in schizophrenia in several more recent studies. In 113 schizophrenic patients, we showed disease-state-dependent alterations in complex I activity, with no change in complex IV activity. Thus, platelet complex I activity was significantly reduced (53% of controls) in patients with residual schizophrenia, while significantly increased (190% of controls) both in patients in an acute psychotic episode and those in a chronic active state, as compared to 37 healthy control subjects (Dror et al. 2002). Moreover, in 27 patients with affective disorders, either major depression or bipolar disorder (the depressed type), complex I activity did not differ from that of the control group (Ben-Shachar et al. 1999), suggesting that the alterations in complex I activity may also be disease specific. Further support for the relationship between the clinical state and complex I activity in schizophrenia can be inferred from the highly significant positive correlation (r = 0.7, p < 0.0001) of complex I activity, with the severity of patients’ positive symptom scores, as well as a tendency towards a negative correlation with the negative symptom scores, as assessed by the positive and negative symptom scale (PANSS) (Dror et al. 2002). Interestingly, in the acute active state, increased complex I activity was observed in both 25 medicated and 25 unmedicated patients (Ben-Shachar et al. 1999) suggesting that at least at this state of the disease medication did not affect complex I activity. Interpretation of the observed effects of medication on complex I are far from straightforward given findings that complex I activity can be inhibited by antipsychotic medications in vitro (Balijepalli et al. 1999; Burkhardt et al. 1993). The latter may explain the reduction in complex I activity in the residual state, while the increase in complex I observed in patients with positive symptomology can more likely be an inherent feature of schizophrenia or psychosis. The increase in complex I activity in the active group of patients could imply the presence of a temporary (in acute state) or a long-lasting state (in chronic active patients) of partial ‘non-responsiveness’ to antipsychotic treatment. Alongside antipsychotic drugs, other endogenous factors, that are altered in association with disease state or treatment, may exist that can modulate complex I activity. One such candidate is dopamine whose neuronal release was reported to decrease by partial inhibition of complex I activity (Bao et al. 2005).
Dopamine and complex I activity
Alterations in the dopaminergic system are strongly implicated in schizophrenia (Carlsson 1988). This is primarily based on the high correlation between the therapeutic efficacy of antipsychotic drugs and their potency as dopamine receptors blockers (Seeman 1987), and the ability of dopamine agonists to induce acute psychotic symptoms, with marked resemblance to schizophrenia. Based on PET studies examining blood flow to the brain during a cognitive task, it has been suggested that acute psychotic episodes (positive symptoms) are associated with a hyperdopaminergic state in the mesolimbic regions, while negative symptoms are associated with a hypodopaminergic state in the mesocortical projections to the frontal cortex (Davis et al. 1991). A more direct approach such as PET studies of dopamine synthesis, receptor density and amphetamine challenged release in schizophrenic brains, which were conducted in either first episode, drug-free patients or patients in an acute exacerbation, implicated a dysfunction in dopamine metabolism, storage, release or uptake mechanisms in the mesolimbic systems in schizophrenia (Breier et al. 1997; Laruelle et al. 1999). Further support for the modulation of dopamine activity in this disorder can be inferred from the findings implicating catechol-o-methyl transferase (COMT), the postsynaptic enzyme that methylates released dopamine to its final metabolite the homovanillic acid, as a risk factor in schizophrenia (Shifman et al. 2002; Weinberger et al. 2001).
A wide range of experimental data suggests that DA can inhibit the mitochondrial respiratory system. Thus, elevated rat brain DA concentrations following chronic administration of l-DOPA or d-methamphetamine resulted in a reduction in the activity of complex I and ATP levels in the striatum (Chan et al. 1994; Przedborski et al. 1993). In isolated intact rat, brain mitochondria DA inhibited ATP coupled state III respiration (Berman and Hatings 1999) and suppressed pyruvate- and succinate-dependent electron transport (Cohen et al. 1997). We have shown that in a neuronal cell line DA induced a reduction in cellular ATP levels without affecting cell viability (Ben-Shachar et al. 2004), and in disrupted mitochondria, from both rat brain and human platelets, DA reversibly inhibited complex I activity but not that of complexes II, IV or V of the respiratory system (Ben-Shachar et al. 1995; Khan et al. 2005). This inhibition had functional consequences as mitochondrial membrane potential (ΔΨm) and complex I driven respiration measured in intact neuronal cell line was impaired by intracellular increase in DA concentrations (Brenner-Lavie et al. 2008, 2009). One may argue that DA has to cross the highly selective inner membrane of the mitochondria to be able to inhibit complex I. Indeed, we have recently shown that DA is taken up by synaptosomal-free, intact, coupled and respiring mitochondria, in a saturable, ATP and Na+-dependent manner.
The relevance of DA–complex I interaction to schizophrenia is inferred by the findings that DA was twice as much potent in inhibiting complex I activity in mitochondria isolated from schizophrenic patients than in those of healthy subjects (Brenner-Lavie et al. 2008). Interestingly, DA inhibition of complex I activity in patients with affective disorders, both with major depression and bipolar disorder (the depressed type) was similar to the control. Furthermore, in intact EBV-transformed lymphocytes derived from schizophrenic patients, DA-induced inhibition of mitochondrial respiration was also two times more potent than in those derived from healthy controls (unpublished data).
Complex I subunit’s expression in schizophrenia
Complex I abnormal activity in schizophrenia can stem from impaired expression of its subunits. In our studies, we have focused on three nuclear encoded subunits, the 51-kDa- (NDUFV1) and the 24-kDa (NDUFV2) subunits, both iron–sulfur flavoproteins having catalytic properties, including the site for transhydrogenation from NADH to NAD+, and the 75 kDa (NDUFS1), the largest iron–sulfur transmembranous structural protein (Hatefi 1985). All three subunits form one functional subunit of the complex (Belogrudov and Hatefi 1996; Clason et al. 2007; Fecke et al. 1994; Ohnishi et al. 1985; Ragan et al. 1982; Zickermann et al. 2007). These three subunits were chosen out of the 45 subunits of complex I, as they constitute the suggested interaction site of complex I and DA (Ben-Shachar et al. 2004). In lymphocytes of schizophrenic patients, mRNA and protein levels of NDUFV1 and NDUFV2 subunits were significantly increased, with no change in NDUFS1 subunit, regardless of the state of the disease. Interestingly, in juvenile neuroleptic-naive schizophrenic patients an increase was observed in lymphocytes mRNA levels of the NDUFS1 subunit (Mehler-Wex et al. 2006). In brain, alterations in complex I subunits’ expression showed regional-specific alterations. Thus, a significant reduction in mRNA and protein levels of NDUFV1 and NDUFV2 subunits, but not of NDUFS1, was observed in the prefrontal cortex, in line with the hypofrontality observed in schizophrenia. In contrast, both subunits exhibited a significant increase in the parieto-occipital cortex shown to be involved in cognitive process of mental visual imagery (Barnes et al. 2000), which may be associated with psychotic hallucinations and paranoid delusions characteristic of schizophrenia (Aleman et al. 2002; Baethge et al. 2005; Frith and Dolan 1997). Abnormalities in the expression of complex I subunits were also observed in an additional anatomical substrate of schizophrenia the striatum, yet no change was observed in the cerebellum, which as will be discussed later, showed significant alterations in patients with affective disorders. The abnormalities in complex I subunits’ expression were associated with the distortion of the high and significant correlation between the three subunits of complex I in normal healthy subjects (Ben-Shachar and Karry 2007). The stoichiometry of NDUFV1, NDUFV2 and NDUFS1 is 1 mol of each subunit for 1 mol of the complex (Belogrudov and Hatefi 1994) suggesting that the deviation from this ratio observed in schizophrenia can lead to abnormal complex I activity. DA was shown to affect complex I activity, but preliminary studies in neuronal cell line do not support the involvement of DA in the altered expression of complex I subunits (Brenner-Lavie et al. 2009). One possible mechanism for the impairments in complex I subunits’ transcripts is an abnormal regulation by a transcription factor.
Sp1 and complex I subunit’s expression
Specificity protein 1 (Sp1) is the prototype of a family of zinc finger (Cys2/Hys2) DNA-binding transcription factors that binds to and acts through G-rich elements such as GC-box. It is generally accepted that this extremely versatile protein is involved in the expression of many different genes and can be regulated at the level of transcription and post-translational modifications such as phosphorylation and/or glycosylation (Suske 1999). Sp1 is involved in the regulation of many genes that have been implicated in schizophrenia such as reelin, GAD67, MAOA/B, NMDA-receptor subunits NR1 and NR2A/B, GABA A and DA receptors D1A and D2/3 (Chen et al. 2002; Liu et al. 2003; Ma et al. 2004; Okamoto et al. 2002; Shih et al. 1993; Szabo et al. 1996). In addition, Sp1 is involved in the regulation and coordination of nuclear-encoded mitochondrial genes including some which encode for OXPHOS proteins (Goffart and Wiesner 2003; Zaid et al. 1999). In line with the latter is our previous study, which has shown that Sp1 regulates the transcription of complex I subunits (Ben-Shachar and Karry 2007). In schizophrenia, Sp1 was abnormally expressed in both brain and periphery. Its mRNA alteration pattern paralleled that of NDUFV1 and NDUFV2, decreasing in the prefrontal cortex and the striatum, while increasing in the parieto-occipital cortex and in lymphocytes of schizophrenic patients as compared to controls. Moreover, a high and significant correlation between Sp1 and complex I subunits existed in normal subjects, but not in patients, further substantiating the role of Sp1 in the abnormal expression of complex I subunits. In addition, being involved in the transcription of many genes either as the main activator/repressor or in combination with additional transcription factors, and subjected to environmental stimuli, Sp1 can contribute to the polygenic and clinically heterogeneous nature of schizophrenia.
Disease specificity of mitochondrial dysfunction
The studies described hitherto presented mitochondrial abnormalities in schizophrenia.
However, numerous studies have implicated mitochondrial dysfunction, in general, and complex I, in particular, in neurodegenerative and in additional psychiatric disorders. Consequently, raising the question as to whether mitochondrial impairment displays disease-specific characteristics or is rather a general non-distinguishing pathology of these disorders. Mitochondrial impairment in neurodegenerative disorders has been reviewed by numerous studies (Berman and Hastings 1999; Chaturvedi and Beal 2008; Van Laar et al. 2008) and is beyond the scope of this review. However, in connection with this review, it is noteworthy that DA–mitochondrial interaction may provide a partial mechanistic explanation for the difference in mitochondrial pathology between DA-associated neurodegenerative and psychiatric disorders. Two mechanisms have been suggested for DA interference with mitochondrial respiration. The first, which involves DA enzymatic catabolism or autooxidation to highly reactive oxygen species (ROS) and has been suggested to underlie cell death, is more likely associated with neurodegenerative DA disorders such as Parkinson’s disease (Berman and Hastings 1999; Izumi et al. 2005; LaVoie and Hastings 1999; Van Laar et al. 2008). The second mechanism involves a direct reversible inhibition of complex I activity, which can disrupt mitochondrial activity leading to abnormal neuronal transmission rather than cell death, can better explain the pathology of non-degenerative DA disorders such as schizophrenia (Ben-Shachar et al. 2004) (Fig. 2).

Schematic presentation of the hypothesized interplay between mitochondrial complex I, DA and Sp1 in schizophrenia. a Under normal conditions, there exists a balanced bidirectional communication between the neuron and its mitochondria, which can affect and be affected by mitochondrial respiration. DA and Sp1 are examples of cellular factors that can modulate complex I activity and its subunit’s transcription, respectively. Complex I plays a major role in controlling oxidative phosphorylation and, therefore, any change in its activity may impinge on mitochondrial function and thereby on neuronal activity, which under normal conditions is re-balanced. b Under pathological conditions associated with increased DA transmission two different mechanisms can be exacerbated. One, in which DA enzymatic catabolism or autooxidation results in increased intra- and extracellular highly reactive oxygen species. This mechanism has been suggested to underlie cell death and is more likely associated with neurodegenerative DA disorders, such as Parkinson’s disease. The other, involves increased DA-induced inhibition of complex I activity and Sp1-dependent abnormal expression of complex I subunits. This can result in mitochondrial dysfunction leading to abnormal neuronal transmission rather than cell death. Such a mechanism can underlie malfunction of cognitive emotional and motor behaviors and better explain the pathology of non-degenerative DA disorders such as schizophrenia. The extent of complex I activity, DA concentration, ROS formation and Sp1 activity are represented by the intensity of their symbols and thickness of arrows
Mitochondrial dysfunction in additional mental disorders has been investigated using a wide array of experimental techniques ranging from imaging studies through ultrastructural methods to genetic and molecular means (Ben-Shachar and Karry 2008; Shao et al. 2008). Thus, in bipolar patients, mostly in medicated patients, 31P- and 1H-MRS imaging studies identified changes in different cellular factors tightly connected with mitochondrial function, including PCr, PMEs, intracellular pH, lactate and NAA in the prefrontal cortex, temporal cortex and in the hippocampus (Bertolino et al. 2003; Kato 2005, 2007; Stork and Renshaw 2005). In major depression, the current literature on MRS studies is sparse with large diversity between studies, some reporting no change, while others a decrease or even an increase in mitochondrial linked cellular factors in patients (Coupland et al. 2005; Kumar et al. 2002; Yildiz-Yesiloglu and Ankerst 2006). For example, a decrease in ATP and an increase in PME and in pH in the frontal cortex were reported (Kato et al. 1992; Volz et al. 2000). Mitochondrial gene expression studies were also performed in patients with affective disorder with some, yet not all, reporting alterations in mitochondrial-related genes and proteins. In bipolar disorder, a reduction in the expression level of mitochondrial-related genes in hippocampal and prefrontal postmortem specimens was observed (Iwamoto et al. 2005; Vawter et al. 2006), with one paper demonstrating reductions in genes of the OXPHOS in the prefrontal cortex (Konradi et al. 2004), while another reporting an increase in complex I subunits NDUFV1 and NDUFV2 in the parieto-occipital cortex (Karry et al. 2004). In major depression, although most studies did not show cortical modifications in mitochondrial-related genes, some reports suggest alterations in the expression of nuclear as well as in mitochondrial DNA-encoded genes in the prefrontal cortex (Karry et al. 2004; Vawter et al. 2006). In addition, it was demonstrated that muscle mitochondria in depressive patients produced less ATP and that the activity of the OXPHOS complexes I + III and II + III was impaired (Burnett et al. 2005). Finally, genetic studies, as mentioned above have implicated single nucleotide polymorphisms (SNPs) in complex I subunits ND3 and NDUFV2 in bipolar disorder (Martorell et al. 2006; McMahon et al. 2000).
These findings are in line with the hypothesis that mitochondrial alterations are secondary to other pathologies observed in these disorders. However, one should consider the effect of medication, since most studies have been conducted in medicated patients. As described above, antipsychotic drugs affect brain energy metabolism, mitochondrial respiration as well as complex I activity. The same is true for mood stabilizers and antidepressant drugs (Daley et al. 2005; Kato 2007; Souza et al. 1994; Weinbach et al. 1986). Thus, medication can blunt the differences in the core pathology of the mitochondria, which could be different between diseases. An additional explanation for limited specificity of the findings may be the known overlap of symptoms between the different disorders. Moreover, despite these cofounders and the similarities in the pathological processes in brain energy metabolism and mitochondrial function, the abnormalities observed are not identical in all three mental disorders. Our recent findings concerning brain mitochondrial complex I (Karry et al. 2004) may constitute one possible demonstration of disease-specific impairments in three major mental disorders, schizophrenia and bipolar disorder and major depression (Ben-Shachar and Karry 2008). We have shown that complex I subunits NDUFV1, NDUFV2 and NDUFS1 were altered in all three psychiatric disorders, albeit in a disease-specific neuroanatomical pattern. In schizophrenia, but not in affective disorders, a selective reduction in mRNA and protein levels of complex I subunits was observed in the prefrontal cortex and the striatum as described above. However, in both affective disorder reductions were observed specifically in the cerebellum with the major depression group demonstrating more consistent alterations. Bipolar disorder, displayed anatomical overlaps also with schizophrenia, as an increase in the expression of complex I subunits was observed in the parieto-occipital cortex of both disorders. This is in line with the similarities in clinical symptoms of bipolar disorder and the other two disorders. In lymphocytes, mitochondrial respiration, complex I activity and its interaction with DA showed schizophrenia-specific impairments with no change between patients with bipolar disorder or major depression and healthy subjects (Brenner-Lavie et al. 2008) (and unpublished data). Taken together, these results suggest that although the similarities in clinical symptoms and in treatment, between these three mental disorders are reflected in their pathophysiology, the pattern, or the extent of the biological impairment can differentiate between disorders. The prevailing concept is that brain circuitry rather than individual brain region that impacts behavioral outcomes, likewise the characteristics of a specific pathology rather than its nature may contribute to different symptom spectrum of these disorders.
Conclusions
The accumulating evidence reviewed by the present article on mitochondrial dysfunction and its abnormal interaction with DA and Sp1 in schizophrenia, substantiate a role for mitochondria in the complex process underlying the pathology of this disorder. Indeed, mitochondria have been implicated in the pathophysiology of schizophrenia and of several additional neuropsychiatric disorders. However, it is noteworthy that mitochondria display disease-specific abnormalities that may contribute to the evolution of the various symptom clusters. Mitochondria are responsible for many essential processes, such as energy production, intracellular calcium buffering, transmission of neurotransmitters, apoptosis and ROS production, all leading either to cell death or playing a role in synaptic plasticity. Synaptic plasticity underlies learning and memory that dictate adaptive or compensatory changes in emotional, cognitive or sensorimotor integration in response to internal or external stimuli. Consequently, impairment in processes regulating neuronal plasticity and remodeling of synapses can lead to the symptomology characteristic of schizophrenia.
The question as to the cause–effect relationship between the above processes remains. On the one hand, mitochondrial activities can be regulated by the metabolic needs of neurons, by neurotransmitters release, as well as by their receptor-induced ionic efflux and signal transduction. Thus, mitochondrial alterations in schizophrenia could be secondary to other pathologies observed in this disorder. Concomitantly, mitochondrial regulated factors can induce backwards effects on these same processes, leading to alterations in gene expression protein synthesis and neuronal activity. It is, therefore, difficult to posit mitochondrial role as an up/down stream process. Suffice it to say presently that mitochondria play a pivotal role in the pathophysiology of schizophrenia. Finally, the aforementioned two-way interactions can be acting synergistically to remodel synaptic connectivity in response to endogenous and/or exogenous environmental inputs.
References
Albensi BC, Sullivan PG, Thompson MB, Scheff SW, Mattson MP (2000) Cyclosporin ameliorates traumatic brain-injury-induced alterations of hippocampal synaptic plasticity. Exp Neurol 162:385–389
Aleman A, Bocker KBE, Hijman R, Kahn RS (2002) Hallucinations in schizophrenia: imbalance between imagery and perception. Schizophr Res 57:315–316
Altar CA, Jurata LW, Charles V, Lemire A, Liu P, Bukhman Y, Young TA, Bullard J, Yokoe H, Webster MJ, Knable MB, Brockman JA (2005) Deficient hippocampal neuron expression of proteasome, ubiquitin, and mitochondrial genes in multiple schizophrenia cohorts. Biol Psychiatry 58:85–96
Amar S, Shamir A, Ovadia O, Blanaru M, Reshef A, Kremer I, Rietschel M, Schulze TG, Maier W, Belmaker RH, Ebstein RP, Agam G, Mishmar D (2007) Mitochondrial DNA HV lineage increases the susceptibility to schizophrenia among Israeli Arabs. Schizophr Res 94:354–358
Andreasen NC, OwLeary DS, Flaum M, Nopoulos P, Watkins G, Boles Ponto LLB, Hichwa RD (1997) Hypofrontality in schizophrenia: disturbed dysfunctional circuits in neuroleptic-naive patients. Lancet 349:1730–1734
Baethge C, Baldessarini RJ, Freudenthal K, Streeruwitz A, Bauer M, Bschor T (2005) Hallucinations in bipolar disorder: characteristics and comparison to unipolar depression and schizophrenia. Bipolar Disord 7:136–145
Balijepalli S, Boyd MR, Ravindranath V (1999) Inhibition of mitochondrial complex I by haloperidol: the role of thiol oxidation. Neuropsychopharmacol 38:567–577
Bao L, Avshalumov MV, Rice ME (2005) Partial mitochondrial inhibition causes striatal dopamine release suppression and medium spiny neuron depolarization via H2O2 elevation, not ATP depletion. J Neurosci 25:10029–10040
Barnes J, Howard RJ, Senior C, Brammer M, Bullmore ET, Simmons A, Woodruff P, David AS (2000) Cortical activity during rotational and linear transformations. Neuropsychologia 38:1148–1156
Belogrudov G, Hatefi Y (1994) Catalytic sector of complex I (NADH:ubiquinone oxidoreductase): subunit stoichiometry and substrate-induced conformation changes. Biochemistry 33:4571–4576
Belogrudov GI, Hatefi Y (1996) Intersubunit interactions in the bovine mitochondrial complex I as revealed by ligand blotting. Biochem Biophys Res Commun 227:135–139
Ben-Shachar D (2002) Mitochondrial dysfunction in schizophrenia: a possible linkage to dopamine. J Neurochem 83:1241–1251
Ben-Shachar D, Karry R (2007) Sp1 expression is disrupted in schizophrenia; a possible mechanism for the abnormal expression of mitochondrial complex I genes, NDUFV1 and NDUFV2. PLoS One 2:e817
Ben-Shachar D, Karry R (2008) Neuroanatomical pattern of mitochondrial complex I pathology varies between schizophrenia, bipolar disorder and major depression. PLoS One 3:e3676
Ben-Shachar D, Zuk R, Glinka Y (1995) Dopamine neurotoxicity: inhibition of mitochondrial respiration. J Neurochem 64:718–723
Ben-Shachar D, Zuk R, Gazawi H, Reshef A, Sheinkman A, Klein E (1999) Increased mitochondrial complex I activity in platelets of schizophrenic patients. Int J Neuropsychopharmacol 2:245–253
Ben-Shachar D, Zuk R, Gazawi H, Ljubuncic P (2004) Dopamine toxicity involves mitochondrial complex I inhibition: implications to dopamine-related neuropsychiatric disorders. Biochem Pharmacol 67:1965–1974
Ben-Shachar D, Bonne O, Chisin R, Klein E, Lester H, Aharon-Peretz J, Yona I, Freedman N (2007) Cerebral glucose utilization and platelet mitochondrial complex I activity in schizophrenia: a FDG-PET study. Prog Neuropsychopharmacol Biol Psychiatry 31:807–813
Berman SB, Hastings TG (1999) Dopamine oxidation alters mitochondrial respiration and induces permeability transition in brain mitochondria: implications for Parkinson’s disease. J Neurochem 73:1127–1137
Bertolino A, Frye M, Callicott JH, Mattay VS, Rakow R, Shelton-Repella J, Post R, Weinberger DR (2003) Neuronal pathology in the hippocampal area of patients with bipolar disorder: a study with proton magnetic resonance spectroscopic imaging. Biol Psychiatry 53:906–913
Black JE, Zelazny AM, Greenough WT (1991) Capillary and mitochondrial support of neural plasticity in adult rat visual cortex. Exp Neurol 111:204–209
Breier A, Su TP, Saunders R, Carson RE, Kolachana BA, de Bartolomeis A, Weinberger DR, Weisenfeld N, Malhotra AK, Eckelman WC, Pickar D (1997) Schizophrenia is associated with elevated amphetamine-induced synaptic dopamine concentrations: evidence from a novel positron emission tomography method. Proc Natl Acad Sci USA 94:2569–2574
Brenner-Lavie H, Klein E, Zuk R, Gazawi H, Ljubuncic P, Ben-Shachar D (2008) Dopamine modulates mitochondrial function in viable SH-SY5Y cells possibly via its interaction with complex I: relevance to dopamine pathology in schizophrenia. Biochim Biophys Acta 1777:173–185
Brenner-Lavie H, Klein E, Ben-Shachar D (2009) Mitochondrial complex I as a novel target for intraneuronal DA: modulation of respiration in intact cells. Biochem Pharmacol 78:85–95
Brodin L, Bakeeva L, Shupliakov O (1999) Presynaptic mitochondria and the temporal pattern of neurotransmitter release. Philos Trans R Soc Lond B Biol Sci 354:365–372
Buchsbaum MS (1990) The frontal lobes, basal ganglia and temporal lobes as sites for schizophrenia. Schizophr Bull 16:377–387
Buchsbaum MS, Hazlett EA (1998) Positron emission tomography studies of abnormal glucose metabolism in schizophrenia. Schizophr Bull 24:343–346
Burkhardt C, Kelly JP, Lim YH, Filley CM, Parker WD (1993) Neuroleptic medications inhibit complex I of the electron transport chain. Ann Neurol 33:512–517
Burnett BB, Gardner A, Boles RG (2005) Mitochondrial inheritance in depression, dysmotility and migraine? J Affect Disord 88:109–116
Calabresi P, Gubellini P, Picconi B, Centonze D, Pisani A, Bonsi P, Greengard P, Hipskind RA, Borrelli E, Bernardi G (2001) Inhibition of mitochondrial complex II induces a long-term potentiation of NMDA-mediated synaptic excitation in the striatum requiring endogenous dopamine. J Neurosci 20:5110–5120
Cannon M, Jones PB, Murray RM (2002) Obstetric complications and schizophrenia: historical and meta-analytic review. Am J Psychiatry 159:1080–1092
Carlsson A (1988) The current status of the dopamine hypothesis of schizophrenia. Neuropsychopharmacol 1:179–186
Carter CS, Perlstein W, Ganguli R, Brar J, Mintun M, Cohen JD (1998) Functional hypofrontality and working memory dysfunction in schizophrenia. Am J Psychiatry 155:1285–1287
Cavelier L, Jazin E, Eriksson I, Prince J, Bave B, Oreland L, Gyllensten U (1995) Decreased cytochrome c oxidase activity and lack of age related accumulation of mtDNA in brain of schizophrenics. Genomics 29:217–228
Chan P, Di Monte DA, Luo JJ, DeLanney LE, Irwin I, Langston JW (1994) Rapid ATP loss caused by methamphetamine in the mouse striatum: relationship between energy impairment and dopaminergic neurotoxicity. J Neurochem 62:2484–2487
Chaturvedi RK, Beal MF (2008) Mitochondrial approaches for neuroprotection. Ann N Y Acad Sci 1147:395–412
Chen Y, Sharma RP, Costa RH, Costa E, Grayson DR (2002) On the epigenetic regulation of the human reelin promoter. Nucleic Acids Res 30:2930–2939
Clason T, Zickermann V, Ruiz T, Brandt U, Radermacher M (2007) Direct localization of the 51 and 24 kDa subunits of mitochondrial complex I by three-dimensional difference imaging. J Struct Biol 159:433–442
Cohen G, Farooqui R, Kesler N (1997) Parkinson’s disease: a new link between monoamine oxidase and mitochondrial electron flow. Proc Natl Acad Sci USA 94:4890–4894
Coupland NJ, Ogilvie CJ, Hegadoren KM, Seres P, Hanstock CC, Allen PS (2005) Decreased prefrontal Myo-inositol in major depressive disorder. Biol Psychiatry 57:1526–1534
Daley E, Wilkie D, Loesch A, Hargreaves IP, Kendall DA, Pilkington GJ, Bates TE (2005) Chlorimipramine: a novel anticancer agent with a mitochondrial target. Biochem Biophys Res Commun 328:623–632
Davey GP, Peuchen S, Clark JB (1998) Energy thresholds in brain mitochondria: potential involvement in neurodegeneration. J Biol Chem 273:12753–12757
Davis KL, Kann RS, Ko G, Davidson M (1991) Dopamine in schizophrenia: a review and reconceptualization. Am J Psychiatry 148:1474–1486
Deicken RF, Johnson C, Pegues M (2000) Proton magnetic resonance spectroscopy of the human brain in schizophrenia. Rev Neurosci 11:147–158
Dingman CW, McGlashan TH (1986) Discriminating characteristics of suicides. Chestnut Lodge follow-up sample including patients with affective disorder, schizophrenia and schizoaffective disorder. Acta Psychiatr Scand 74:91–97
Dror N, Klein E, Karry R, Sheinkman A, Kirsh Z, Mazor M, Tzukerman M, Ben-Shachar D (2002) State dependent alterations in mitochondrial complex I activity in platelets: a potential peripheral marker for schizophrenia. Mol Psychiatry 7:995–1001
Fecke W, Sled VD, Ohnishi T, Weiss H (1994) Disruption of the gene encoding the NADH-binding subunit of NADH: ubiquinone oxidoreductase in Neurospora crassa. Formation of a partially assembled enzyme without FMN and the iron–sulphur cluster N-3. Eur J Biochem 220:551–558
Feinberg AP (2007) Phenotypic plasticity and the epigenetics of human disease. Nature 447:433–440
Frith C, Dolan RJ (1997) Brain mechanisms associated with top–down processes in perception. Philos Trans R Soc Lond B Biol Sci 352:1221–1230
Fujimoto T, Nakano T, Takano T, Hokazono Y, Asakura T, Tsuji T (1992) Study of chronic schizophrenics using 31P magnetic resonance chemical shift imaging. Acta Psychiatr Scand 86:455–462
Fukuzako H, Fukuzako T, Hashiguchi T, Kodama S, Takigawa M, Fujimoto T (1999) Changes in levels of phosphorus metabolites in temporal lobes of drug-naive schizophrenic patients. Am J Psychiatry 156:1205–1208
Goffart S, Wiesner RJ (2003) Regulation and co-ordination of nuclear gene expression during mitochondrial biogenesis. Exp Physiol 88:33–40
Guo X, Macleod GT, Wellington A, Hu F, Panchumarthi S, Schoenfield M, Marin L, Charlton MP, Atwood HL, Zinsmaier KE (2005) The GTPase dMiro is required for axonal transport of mitochondria to Drosophila synapses. Neuron 47:379–393
Gur RE, Resnick SM, Alavi A, Gur RC, Caroff S, Dann R, Silver FL, Saykin AJ, Chwluk JB, Kudhner M (1987) Regional brain function in schizophrenia II: repeated evaluation with positron emission tomography. Arch Gen Psychiatry 44:126–129
Harrison PJ (1999) The neuropathology of schizophrenia. A critical review of the data and their interpretation. Brain 122(Pt 4):593–624
Harrison PJ, Weinberger DR (2005) Schizophrenia genes, gene expression, and neuropathology: on the matter of their convergence. Mol Psychiatry 10:40–68 (image 45)
Hatefi Y (1985) The mitochondrial electron transport and oxidative phosphorylation system. Annu Rev Biochem 54:1015–1069
Hazlett EA, Buchsbaum MS, Byne W, Wei TC, Spiegel-Cohen J, Geneve C, Kinderlehrer R, Haznedar MM, Shihabuddin L, Siever LJ (1999) Three-dimensional analysis with MRI and PET of the size, shape, and function of the thalamus in the schizophrenia spectrum. Am J Psychiatry 156:1190–1199
Hazlett EA, Buchsbaum MS, Jeu LA, Nenadic I, Fleischman MB, Shihabuddin L, Haznedar MM, Harvey PD (2000) Hypofrontality in unmedicated schizophrenia patients studied with PET during performance of a serial verbal learning tasks. Schizophr Res 43:33–46
Hevner RF, Wong-Riley M (1991) Neuronal expression of nuclear and mitochondrial genes for cytochrome oxidase (CO) subunits analyzed by in situ hybridization: comparison with CO activity and protein. J Neurosci 11:1942–1958
Iwamoto K, Bundo M, Kato T (2005) Altered expression of mitochondria-related genes in postmortem brains of patients with bipolar disorder or schizophrenia, as revealed by large-scale DNA microarray analysis. Hum Mol Genet 14:241–253
Izumi Y, Sawada H, Yamamoto N, Kume T, Katsuki H, Shimohama S, Akaike A (2005) Iron accelerates the conversion of dopamine-oxidized intermediates into melanin and provides protection in SH-SY5Y cells. J Neurosci Res 82:126–137
Jakob H, Beckmann H (1989) Gross and histological criteria for developmental disorders in brains of schizophrenics. J R Soc Med 82:466–469
Jayakumar PN, Venkatasubramanian G, Keshavan MS, Srinivas JS, Gangadhar BN (2006) MRI volumetric and 31P MRS metabolic correlates of caudate nucleus in antipsychotic-naive schizophrenia. Acta Psychiatr Scand 114:346–351
Jensen JE, Miller J, Williamson PC, Neufeld RW, Menon RS, Malla A, Manchanda R, Schaefer B, Densmore M, Drost DJ (2006) Grey and white matter differences in brain energy metabolism in first episode schizophrenia: 31P-MRS chemical shift imaging at 4 Tesla. Psychiatry Res 146:127–135
Kaminska B, Kaczmarek L, Larocque S, Chaudhuri A (1997) Activity-dependent regulation of cytochrome b gene expression in monkey visual cortex. J Comp Neurol 379:271–282
Kang JS, Tian JH, Pan PY, Zald P, Li C, Deng C, Sheng ZH (2008) Docking of axonal mitochondria by syntaphilin controls their mobility and affects short-term facilitation. Cell 132:137–148
Karry R, Klein E, Ben Shachar D (2004) Mitochondrial complex I subunits expression is altered in schizophrenia: a postmortem study. Biol Psychiatry 55:676–684
Kato T (2005) Mitochondrial dysfunction in bipolar disorder: from 31P-magnetic resonance spectroscopic findings to their molecular mechanisms. Int Rev Neurobiol 63:21–40
Kato T (2007) Mitochondrial dysfunction as the molecular basis of bipolar disorder: therapeutic implications. CNS Drugs 21:1–11
Kato T, Takahashi S, Shioiri T, Inubushi T (1992) Brain phosphorous metabolism in depressive disorders detected by phosphorus-31 magnetic resonance spectroscopy. J Affect Disord 26:223–230
Kato T, Kunugi H, Nanko S, Kato N (2001) Mitochondrial DNA polymorphisms in bipolar disorder. J Affect Disord 62:151–164
Khan FH, Sen T, Maiti AK, Jana S, Chatterjee U, Chakrabarti S (2005) Inhibition of rat brain mitochondrial electron transport chain activity by dopamine oxidation products during extended in vitro incubation: implications for Parkinson’s disease. Biochim Biophys Acta 1741:65–74
Kim JJ, Mohamed S, Andreasen NC, O’Leary DS, Watkins GL, Boles Ponto LL, Hichwa RD (2000) Regional neural dysfunctions in chronic schizophrenia studied with positron emission tomography. Am J Psychiatry 157:542–548
Kishimoto H, Yamada K, Iseki E, Kosaka K, Okoshi T (1998) Brain imaging of affective disorders and schizophrenia. Psychiatry Clin Neurosci 52:S212–S214
Kolomeet NS, Uranova NA (1999) Synaptic contacts in schizophrenia: studies using immunocytochemical identification of dopaminergic neurons. Neurosci Behav Physiol 29:217–221
Kolomeets NS, Uranova N (2009) Ultrastructural abnormalities of astrocytes in the hippocampus in schizophrenia and duration of illness: a postmortem morphometric study. World J Biol Psychiatry 99999:1–11
Konradi C, Eaton M, MacDonald ML, Walsh J, Benes FM, Heckers S (2004) Molecular evidence for mitochondrial dysfunction in bipolar disorder. Arch Gen Psychiatry 61:300–308
Kumar A, Thomas A, Lavretsky H, Yue K, Huda A, Curran J, Venkatraman T, Estanol L, Mintz J, Mega M, Toga A (2002) Frontal white matter biochemical abnormalities in late-life major depression detected with proton magnetic resonance spectroscopy. Am J Psychiatry 159:630–636
Kung L, Roberts RC (1999) Mitochondrial pathology in human schizophrenic striatum: a postmortem ultrastructural study. Synapse 31:67–75
Lahti AC, Holcomb HH, Medoff DR, Weiler MA, Tamminga CA, Carpenter WT Jr (2001) Abnormal patterns of regional cerebral blood flow in schizophrenia with primary negative symptoms during an effortful auditory recognition task. Am J Psychiatry 158:1797–1808
Laruelle M, Abi-Dargham A, Gil R, Kegeles L, Innis R (1999) Increased dopamine transmission in schizophrenia: relationship to illness phase. Biol Psychiatry 46:56–72
LaVoie MJ, Hastings TG (1999) Dopamine quinone formation and protein modification associated with the striatal neurotoxicity of methamphetamine: evidence against a role for extracellular dopamine. J Neurosci 19:1484–1491
Li Z, Okamoto K, Hayashi Y, Sheng M (2004) The importance of dendritic mitochondria in the morphogenesis and plasticity of spines and synapses. Cell 119:873–887
Liu A, Zhuang Z, Hoffman PW, Bai G (2003) Functional analysis of the rat N-methyl-d-aspartate receptor 2A promoter: multiple transcription starts points, positive regulation by Sp factors, and translational regulation. J Biol Chem 278:26423–26434
Ma L, Song L, Radoi GE, Harrison NL (2004) Transcriptional regulation of the mouse gene encoding the alpha-4 subunit of the GABAA receptor. J Biol Chem 279:40451–40461
Madhavarao CN, Chinopoulos C, Chandrasekaran K, Namboodiri MA (2003) Characterization of the N-acetylaspartate biosynthetic enzyme from rat brain. J Neurochem 86:824–835
Manoach DS, Press DZ, Thangaraj V, Searl MM, Goff DC, Halpern E, Saper CB, Warach S (1999) Schizophrenic subjects activate dorsolateral prefrontal cortex during a working memory task, as measured by fMRI. Biol Psychiatry 45:1128–1137
Martorell L, Segues T, Folch G, Valero J, Joven J, Labad A, Vilella E (2006) New variants in the mitochondrial genomes of schizophrenic patients. Eur J Hum Genet 14:520–528
Mattson MP (1999) Establishment and plasticity of neuronal polarity. J Neurosci 57:577–589
Maurer I, Zierz S, Moller H (2001) Evidence for a mitochondrial oxidative phosphorylation defect in brains from patients with schizophrenia. Schizophr Res 48:125–136
McGlashan TH (1988) A selective review of recent North American long-term follow-up studies of schizophrenia. Schizophr Bull 14:515–542
McGlashan TH, Fenton WS (1992) The positive/negative distinction in schizophrenia: review of natural history validators. Arch Gen Psychiatry 49:63–72
McMahon FJ, Chen YS, Patel S, Kokoszka J, Brown MD, Torroni A, DePaulo JR, Wallace DC (2000) Mitochondrial DNA sequence diversity in bipolar affective disorder. Am J Psychiatry 157:1058–1064
Mehler-Wex C, Duvigneau JC, Hartl RT, Ben-Shachar D, Warnke A, Gerlach M (2006) Increased mRNA levels of the mitochondrial complex I 75-kDa subunit : a potential peripheral marker of early onset schizophrenia? Eur Child Adolesc Psychiatry 15:504–507
Middleton FA, Mirnics K, Pierri JN, Lewis DA, Levitt P (2002) Gene expression profiling reveals alterations of specific metabolic pathways in schizophrenia. J Neurosci 22:2718–2729
Mizino Y, Suzuki K, Ohta S (1990) Postmortem changes in mitochondrial respiratory enzymes in brain and a preliminary observation in Parkinson’s disease. J Neurol Sci 96:49–57
Muir WJ, Pickard BS, Blackwood DH (2008) Disrupted-in-Schizophrenia-1. Curr Psychiatry Rep 10:140–147
Mulcrone J, Whatley SA, Ferrier IN, Marchbanks RM (1995) A study of altered gene expression in frontal cortex from schizophrenic patients using differential screening. Schizophr Res 14:203–213
Ohnishi T, Ragan CI, Hatefi Y (1985) EPR studies of iron–sulfur clusters in isolated subunits and subfractions of NADH-ubiquinone oxidoreductase. J Biol Chem 260:2782–2788
Okamoto S, Sherman K, Bai G, Lipton SA (2002) Effect of the ubiquitous transcription factors, SP1 and MAZ, on NMDA receptor subunit type 1 (NR1) expression during neuronal differentiation. Brain Res Mol Brain Res 107:89–96
Phillips LJ, Francey SM, Edwards J, McMurray N (2007) Stress and psychosis: towards the development of new models of investigation. Clin Psychol Rev 27:307–317
Potkin SG, Alva G, Fleming K, Anand R, Keator D, Carreon D, Doo M, Jin Y, Wu JC, Fallon JH (2002) A PET study of the pathophysiology of negative symptoms in schizophrenia. Positron emission tomography. Am J Psychiatry 157:227–237
Prabakaran S, Swatton JE, Ryan MM, Huffaker SJ, Huang JT, Griffin JL, Wayland M, Freeman T, Dudbridge F, Lilley KS, Karp NA, Hester S, Tkachev D, Mimmack ML, Yolken RH, Webster MJ, Torrey EF, Bahn S (2004) Mitochondrial dysfunction in schizophrenia: evidence for compromised brain metabolism and oxidative stress. Mol Psychiatry 9:684–697 (see also 643)
Prince JA, Yassin MS, Oreland L (1998) A histochemical demonstration of altered cytochrome oxidase activity in the rat brain by neuroleptics. Eur Neuropsychopharmacol 8:1–6
Prince JA, Blennow K, Gottfries CG, Karlsson I, Oreland L (1999) Mitochondrial function in differentially altered in the basal ganglia of chronic schizophrenics. Neuropsychopharmacol 21:372–379
Prince JA, Harro J, Blennow K, Gottfries CG, Karlsson I, Oreland L (2000) Putamen mitochondrial energy metabolism is highly correlated to emotional and intellectual impairment in schizophrenics. Neuropsychopharmacol 22:284–292
Przedborski S, Jackson-Lewis V, Muthane U, Jiang H, Ferreria M, Naini AB, Fahn S (1993) Chronic levodopa administration alters cerebral mitochondrial respiratory chain activity. Ann Neurol 34:715–723
Ragan CI, Galante YM, Hatefi Y (1982) Purification of three iron–sulfur proteins from the iron-protein fragment of mitochondrial NADH-ubiquinone oxidoreductase. Biochemistry 21:2518–2524
Reddy R, Keshavan MS (2003) Phosphorus magnetic resonance spectroscopy: its utility in examining the membrane hypothesis of schizophrenia. Prostaglandins Leukot Essent Fatty Acids 69:401–405
Rollins B, Martin MV, Sequeira PA, Moon EA, Morgan LZ, Watson SJ, Schatzberg A, Akil H, Myers RM, Jones EG, Wallace DC, Bunney WE, Vawter MP (2009) Mitochondrial variants in schizophrenia, bipolar disorder, and major depressive disorder. PLoS One 4:e4913
Seeman P (1987) Dopamine receptors and the dopamine hypothesis of schizophrenia. Synapse 1:133–152
Shao L, Martin MV, Watson SJ, Schatzberg A, Akil H, Myers RM, Jones EG, Bunney WE, Vawter MP (2008) Mitochondrial involvement in psychiatric disorders. Ann Med 40:281–295
Shenton ME, Dickey CC, Frumin M, McCarley RW (2001) A review of MRI findings in schizophrenia. Schizophr Res 49:1–52
Sherman SM, Spear PD (1982) Organization of visual pathways in normal and visually deprived cats. Physiol Rev 62:738–755
Shifman S, Bronstein M, Sternfeld M, Pisante-Shalom A, Lev-Lehman E, Weizman A, Reznik I, Spivak B, Grisaru N, Karp L, Schiffer R, Kotler M, Strous RD, Swartz-Vanetik M, Knobler HY, Shinar E, Beckmann JS, Yakir B, Risch N, Zak NB, Darvasi A (2002) A Highly Significant Association between a COMT Haplotype and Schizophrenia. Am J Hum Genet 71:1296–1302
Shih JC, Grimsby J, Chen K, Zhu QS (1993) Structure and promoter organization of the human monoamine oxidase A and B genes. J Psychiatry Neurosci 18:25–32
Souza ME, Polizello AC, Uyemura SA, Castro-Silva O, Curti C (1994) Effect of fluoxetine on rat liver mitochondria. Biochem Pharmacol 48:535–541
Stefansson H, Thorgeirsson TE, Gulcher JR, Stefansson K (2003) Neuregulin 1 in schizophrenia: out of Iceland. Mol Psychiatry 8:639–640
Stork C, Renshaw PF (2005) Mitochondrial dysfunction in bipolar disorder: evidence from magnetic resonance spectroscopy research. Mol Psychiatry 10:900–919
Stowers RS, Megeath LJ, Gorska-Andrzejak J, Meinertzhagen IA, Schwarz TL (2002) Axonal transport of mitochondria to synapses depends on Milton, a novel Drosophila protein. Neuron 36:1063–1077
Suske G (1999) The Sp-family of transcription factors. Gene 238:291–300
Szabo G, Katarova Z, Kortvely E, Greenspan RJ, Urban Z (1996) Structure and the promoter region of the mouse gene encoding the 67-kD form of glutamic acid decarboxylase. DNA Cell Biol 15:1081–1091
Tamminga CA, Thaker GK, Buchanan R, Kirkpatrick B, Alphs LD, Chase TN, Carpenter WT (1992) Limbic system abnormalities identified in schizophrenia using positron emission tomography with fluorodeoxyglucose and neocortical alterations with deficit syndrome. Arch Gen Psychiatry 49:522–530
Tsankova N, Renthal W, Kumar A, Nestler EJ (2007) Epigenetic regulation in psychiatric disorders. Nat Rev Neurosci 8:355–367
Uranova NA, Aganova EA (1989) Ultrastructure of synapses of the anterior limbic cortex in schizophrenia. Zh Nevropatol Psikhiatr Im S S Korsakova 89:56–59
Uranova N, Orlovskaya D, Vikhreva O, Zimina I, Kolomeets N, Vostrikov V, Rachmanova V (2001) Electron microscopy of oligodendroglia in severe mental illness. Brain Res Bull 55:597–610
Van Laar VS, Dukes AA, Cascio M, Hastings TG (2008) Proteomic analysis of rat brain mitochondria following exposure to dopamine quinone: implications for Parkinson disease. Neurobiol Dis 29:477–489
van Winkel R, Stefanis NC, Myin-Germeys I (2008) Psychosocial stress and psychosis: a review of the neurobiological mechanisms and the evidence for gene–stress interaction. Schizophr Bull 34:1095–1105
Vawter MP, Tomita H, Meng F, Bolstad B, Li J, Evans S, Choudary P, Atz M, Shao L, Neal C, Walsh DM, Burmeister M, Speed T, Myers R, Jones EG, Watson SJ, Akil H, Bunney WE (2006) Mitochondrial-related gene expression changes are sensitive to agonal-pH state: implications for brain disorders. Mol Psychiatry 11(615):663–679
Verstreken P, Ly CV, Venken KJ, Koh TW, Zhou Y, Bellen HJ (2005) Synaptic mitochondria are critical for mobilization of reserve pool vesicles at Drosophila neuromuscular junctions. Neuron 47:365–378
Volz HR, Riehemann S, Maurer I, Smesny S, Sommer M, Rzanny R, Holstein W, Czekalla J, Sauer H (2000) Reduced phosphodiesters and high-energy phosphates in the frontal lobe of schizophrenic patients: a 31P chemical shift spectroscopic-imaging study. Biol Psychiatry 47:954–961
Washizuka S, Kametani M, Sasaki T, Tochigi M, Umekage T, Kohda K, Kato T (2006) Association of mitochondrial complex I subunit gene NDUFV2 at 18p11 with schizophrenia in the Japanese population. Am J Med Genet B Neuropsychiatr Genet 141:301–304
Weeber EJ, Levy M, Sampson MJ, Anflous K, Armstrong DL, Brown SE, Sweatt JD, Craigen WJ (2002) The role of mitochondrial porins and the permeability transition pore in learning and synaptic plasticity. J Biol Chem 277:18891–18897
Weinbach EC, Costa JL, Nelson BD, Claggett CE, Hundal T, Bradley D, Morris SJ (1986) Effects of tricyclic antidepressant drugs on energy-linked reactions in mitochondria. Biochem Pharmacol 35:1445–1451
Weinberger DR, Egan MF, Bertolino A, Callicott JH, Mattay VS, Lipska BK, Berman KF, Goldberg TE (2001) Prefrontal neurons and the genetics of schizophrenia. Biol Psychiatry 50:825–844
Whatley SA, Curi D, Marchbanks RM (1996) Mitochondrial involvement in schizophrenia and other functional psychoses. Neuroch Res 21:995–1004
Whatley SA, Curi D, Das Gupta F (1998) Superoxide, neuroleptics and the ubiquinone and cytochrome b5 reductases in brain and lymphocytes from normals and schizophrenic patients. Mol Psychiatry 3:227–237
Wolkin A, Jaeger J, Brodie JD, Wolf AP, Fowler J, Rotrosen J, Gomez-Mont F, Cancro R (1985) Persistence of cerebral metabolic abnormalities in chronic schizophrenia as determined by positron emission tomography. Am J Psychiatry 142:564–571
Wong-Riley M (1989) Cytochrome c oxidase: an endogenous metabolic marker for neuronal activity. Trends Neurosci 12:94–101
Wright IC, Rabe-Hesketh S, Woodruff PW, David AS, Murray RM, Bullmore ET (2000) Meta-analysis of regional brain volumes in schizophrenia. Am J Psychiatry 157:16–25
Yang C, Silver B, Ellis SR, Mower GD (2001) Bidirectional regulation of mitochondrial gene expression during developmental neuroplasticity of visual cortex. Biochem Biophys Res Commun 287:1070–1074
Yildiz-Yesiloglu A, Ankerst DP (2006) Review of 1H magnetic resonance spectroscopy findings in major depressive disorder: a meta-analysis. Psychiatry Res 147:1–25
Zaid A, Li R, Luciakova K, Barath P, Nery S, Nelson BD (1999) On the role of the general transcription factor Sp1 in the activation and repression of diverse mammalian oxidative phosphorylation genes. J Bioenerg Biomembr 31:129–135
Zickermann V, Zwicker K, Tocilescu MA, Kerscher S, Brandt U (2007) Characterization of a subcomplex of mitochondrial NADH:ubiquinone oxidoreductase (complex I) lacking the flavoprotein part of the N-module. Biochim Biophys Acta 1767:393–400
Zubin J, Spring B (1977) Vulnerability––a new view of schizophrenia. J Abnorm Psychol 86:103–126
Acknowledgments
We acknowledge Rachel Karry (Ph.D.) and Natalie Dror who performed the molecular studies in postmortem specimens and blood cells, Hanit Brenner-Lavie (Ph.D.), Predrag Ljubuncic (Ph.D.), Haifa Gazawi (M.Sc.) and Rosa Zuk (M.Sc.) who performed the studies on complex I activity and characterized its interaction with DA. We acknowledge the assistance of Alon Reshef (MD), Ala Sheinkman MD, Marina Mazar (MD) and Zvi Kirsh (MD) for their contribution to blood samples collection and the clinical characterization of the patients and Ehud Klein (MD) for supervising the clinical part of the studies. Postmortem brain specimens were provided from the Stanley Foundation Neuropathology Consortium (Bethesda, MD). This project was supported by the by grants from The Chief Scientist Israel Ministry of Health, The Stanley Medical Research Institute grant and The NARSAD Independent Investigator Award.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ben-Shachar, D. The interplay between mitochondrial complex I, dopamine and Sp1 in schizophrenia. J Neural Transm 116, 1383–1396 (2009). https://doi.org/10.1007/s00702-009-0319-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00702-009-0319-5