
Abstract
Background
Three-dimensional (3-D) stereoscopic vision is theoretically superior to two-dimensional (2-D) vision in endoscopic endonasal surgery. However, only few reports have quantitatively compared endoscopic performance under the two visual conditions. We introduced a newly designed stereoendoscopic system with a “dual-lens and single camera” for endoscopic endonasal surgery and objectively compared the performances under 3-D and high-definition 2-D visualizations on a dry laboratory model.
Methods
Thirty subjects without experience performing endoscopic surgery, computer-simulated training or any 3-D video system were recruited and divided into two groups (Group A and Group B) for performing two different tasks. The novel 4.7-mm-diameter stereoendoscope provided high-definition (HD) images. In Task 1, Group A started the task under the 3-D condition followed by the 2-D condition, and Group B vice versa. In Task 2, Group A started the task under the 2-D condition followed by the 3-D condition, and Group B vice versa. The performance accuracy and speed under the two visual conditions were analyzed.
Results
Significant improvement in performance accuracy and speed was seen under 3-D conditions in the both “3-D first” and “2-D first” subgroups during both tasks (P < .001). Regardless of order, the inaccuracy rate and performance time under 3-D conditions was significantly lower than that under 2-D conditions in each subject.
Conclusions
We demonstrated the advantage of 3-D visualization over 2-D visualization for inexperienced subjects. Further quantitative clinical studies are required to confirm whether stereoendoscopy actually provides benefits in clinical settings.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The indications for endoscopic endonasal surgery (EES) have recently been extended beyond sinonasal and pituitary lesions to various skull base and intradural pathologies [4, 12, 13]. For meticulous dissection of neurovascular structures, it has been proposed that three-dimensional (3-D) visualization has advantages over two-dimensional (2-D) visualization [18]. However, the usage of stereoendoscopes has been limited because their diameter is too large for the nasal space and their resolution is not adequate. The advent of full high-definition (HD) endoscopy has not only resolved the latter problem but also somewhat rectified the lack of depth perception [8, 11]. To date, very few studies have objectively compared endoscopic performance under 3-D and 2-D visualization [8, 17]. Herein, we introduce a newly designed stereoendoscope with HD quality and evaluated the endoscopic performance during EES in novices under both 3-D and HD 2-D visualization conditions, considering ergonomic factors.
Methods
Stereoendoscopic system
We introduced a novel stereoendoscopic system for 3-D visualization for this study (manufactured by SHINKO OPTICAL Co., Ltd, Tokyo, Japan and distributed by MACHIDA Endoscope Co., Ltd., Tokyo, Japan). The stereoendoscopic system comprises a 0° and 30° rigid endoscope with an outer diameter of 4.7 mm, a 3-D video camera (model M3D-CAM), a 3-D converter (model M3D-CON), and a high-intensity xenon light source. This endoscope has the advantage of a “dual-lens and single camera” system with two lenses mounted on the tip of the endoscope (Fig. 1). The distance between the center of each lens is 2 mm. Separate images were captured on a charge-coupled device (CCD) image sensor of 2 megapixel and processed on a 3-D converter, achieving HD resolution. In addition, it can switch between 2-D and 3-D modes, both of which produce HD quality images. A 24-inch 3-D liquid crystal display (LCD) incorporates circular micropolarizing technology (model LMD-2451MT; SONY, Tokyo, Japan). This monitor converts 3-D image signals to a line-by-line format and utilizes a circular micro-polarizer filter over the face, alternating rows of pixels into two different polarization states; right-handed circular and left-handed circular. Passively polarized glasses allowed surgeons to perceive the 3-D image when one eye sees all the odd-numbered rows and the other eye sees all the even-numbered rows. Hence, in this study, the difference between 2-D and 3-D visualization was the presence or absence of binocular parallax, whereas the optical system (including the focal length, angle of view, and resolution of the image) was identical.

0° (left) and 30° (right) rigid endoscopes. Two lenses are mounted on the tip and the outer diameter of the endoscope is 4.7 mm
Training model
We set up a dry laboratory model for objective assessment of basic endoscopic skills (Fig. 2). A human nasal model for EES (SurgTrainer, Ltd., Ibaraki, Japan), developed by the National Institute of Advanced Industrial Science and Technology, Tokyo, Japan, was used [6, 23]. This dummy of the nasal cavities consists of two parts: an interchangeable nasal cavity module made of urethane resin and a non-interchangeable facial skin model made of silicon rubber similar to the actual human facial skin. The distance between the two nostrils of the facial skin model was 25 mm. We replaced the nasal cavity module with a home-made module for performance of the tasks (Fig. 2a, b). The endoscope was inserted and fixed through the right nostril at an angle of 45° to the horizontal (Fig. 2c). The task module was set so that the tasks could be performed bimanually at 80–100 mm from the nostril and at 10–30 mm from the tip of the endoscope, and this matched average distances in actual EES.

Dry laboratory training model using a human nasal model for endoscopic endonasal surgery (SurgTrainer, Ltd, Ibaraki, Japan). a A ready-made nasal cavity module was replaced with a home-made module for performing the tasks. b A face skin mask covered the model. c The 3-D endoscope was inserted and fixed through the right nostril of the dummy in position at an angle of 45° to the horizontal. A subject exercised the tasks with two-handed manipulation of instruments via both nostrils
Subjects and tasks
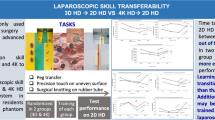
Subjects with no experience in performing endoscopic surgery, computer-simulated training, or any 3-D video system were recruited from our department. They were asked to execute two basic tasks, i.e., rubber doughnut ring transfer (Task 1) and peg alignment (Task 2) under both 3-D and 2-D visualization conditions (Fig. 3a). The method for evaluation of performance for each task had not been previously conveyed to the subjects. In Task 1, the subjects transferred a rubber doughnut ring from one peg to another consecutively for 3 minutes (Fig. 3b). Timing for this task was started when they grasped the first ring on the pegboard. The subjects were requested to grasp the ring first in their nondominant hand and to transfer it in mid-air to their dominant hand. The number of times the ring was transferred and the number of times the ring was dropped (considered a mistake) were recorded, from which the inaccuracy rate was calculated, given by [Inaccuracy rate] = [Number of Times Dropped] / [Number of Times Transferred]. In Task 2, the subjects grasped a peg from among a group of eight pegs in two lines on the sagittal plane in a staggered manner, picked it up, and placed it aside (Fig. 3c). The time taken to perform this task back and forth was measured. First of all, the subjects were divided into two groups (Group A and Group B). To minimize any order effect or carry-over effect, in Task 1, Group A started the task under the 3-D condition followed by the 2-D condition, and Group B started under the 2-D condition followed by the 3-D condition. Conversely, in Task 2, Group A started the task under the 2-D condition followed by the 3-D condition, and Group B started under the 3-D condition followed by the 2-D condition (Fig. 4). The interval of time between the task performances under each condition was more than 48 hours. The subjects were trained on how to perform each task and allowed to practice only once under direct vision prior to starting. All tasks were performed in the same room and the same layout in our faculty. All optical conditions were identical to each other except for the depth information. Each exercise was recorded and subsequently evaluated via video by an independent observer, who was blinded to the detail of our study design, including the order of the groups.

Pictures of the exercises. a A subject wearing passively polarizing glasses was positioned right in front of the display and performed the tasks under both two-dimensional (2-D) and 3-D visualizations. Stereo-pair images of b Task 1 and c Task 2. The image from the right lens is positioned on the right and that from the left lens is positioned on the left. The right and left images are reconstructed in the 3-D converter into 3-D image signals, which are transmitted to the 3-D display

Thirty novice participants were divided into two groups (Group A and Group B) for the performing of two different tasks. In Task 1, Group A started the task under the 3-D condition followed by the 2-D condition, and Group B vice versa. In Task 2, Group A started the task under the 2-D condition followed by the 3-D condition, and Group B vice versa
Statistical analysis
Values are expressed as mean ± standard deviation. Statistical analyses of within-subject differences between 2-D and 3-D performances were undertaken using a Wilcoxon signed-rank test. The differences in performance between the different task sequences were analyzed by a Mann–Whitney U test. The data were analyzed using the SAS 9.2 software package (SAS, Cary, NC, USA). A value of P < .05 was considered statistically significant.
Results
A total of 30 subjects were enrolled in this study, including 9 neuroscientists and 21 medical students, with a mean age of 28.0 ± 6.0 years (range 22–43 years; 26 male and 4 female). They were all right-handed. There were no significant differences in age between Group A and Group B (n = 15 and mean age of 27.8 ± 5.9 years in Group A; n = 15 and 28.2 ± 6.2 years in Group B). All subjects carried out each task without complaining of visual strain, headache, or physical discomfort during the task. All subjects preferred 3-D vision over 2-D vision for meticulous manipulation of instruments.
Subjects who performed their first task under the 3-D condition were referred to as the “3-D first” subgroup and those who performed their first task under the 2-D condition were the “2-D first” subgroup. For Task 1, in the “3-D first” and “2-D first” subgroups, the inaccuracy rate under the 3-D condition was significantly lower than that under the 2-D condition (Table 1; P < .001). Regardless of order, the inaccuracy rate under the 3-D condition was significantly lower than that under the 2-D condition in each subject (Fig. 5a; P < .001).

Graphs showing the change in inaccuracy rate in Task 1 (a) and performance time in Task 2 (b) within each subject under 2-D and 3-D visualization. a The overall inaccuracy rate with the 3-D visualization was significantly lower when compared with the 2-D visualization (P < .001). b The overall performance time with the 3-D visualization was significantly lower when compared with the 2-D visualization (P < .001). Large individual variations were demonstrated in both accuracy and speed of performance
For Task 2, the performance time of the “2-D first” and the “3-D first” subgroups also differed significantly between the two modes (Table 2; P < .001). Regardless of order, the performance time under the 3-D condition was significantly lower than that under the 2-D condition in each subject (Fig. 5b; P < .001). Comparing the two subgroups, the degree of difference between the two modes in each task was not significantly different (Table 3, P = .9181 for Task 1, P = .0782 for Task 2), meaning that neither a carry-over effect, nor an order effect, influenced the results of this study. These findings revealed that 3-D visualization could provide an improvement in accuracy and performance speed for inexperienced persons. However, large individual variations in performance were also demonstrated (Fig. 5).
Discussion
3-D endoscopic surgery
3-D visualization is thought to be helpful in acquiring depth perception and in shortening the learning curve for endoscopic surgery. A variety of studies in the field of laparoscopic surgery have shown that stereoendoscopic systems can provide the advantages of 3-D visualization, such as decreased operation times and better accuracy of surgery [7, 19, 20]. However, despite these advantages, the stereoendoscope is not popular nowadays for several reasons [5, 10, 22].
In EES, 3-D visualization has not yet been extensively evaluated because of the larger diameter of the endoscope for the narrow nasal cavity and less necessity for delicate manipulation of instruments in comparison to laparoscopic surgery [21]. Because EES is now indicated for skull base and intradural pathologies in addition to sinonasal lesions and pituitary tumors, more meticulous dissection of vital neurovascular structures and bimanual manipulation of instruments are needed [12, 13]. The clinical evaluation of 3-D visualization in EES is in its infancy, and the expectations are that it will provide greater accuracy and speed and decrease lengthy learning curves, demonstrating positive results in a subjective manner [3, 8, 16, 18, 21]. However, few studies have evaluated the benefits of stereoendoscopy in a laboratory or an objective setting [8, 17].
Development of a novel stereoendoscopic system for ESS
A newly-developed “dual-lens and single camera” stereoendoscopic system is now commercially available. This endoscope has an outer diameter of 4.7 mm and two object lenses are mounted on the tip. The parallel optical channels convey the separate images to a single CCD image sensor of 2 megapixels. This dual-lens system captures slightly different images, much like human binocular vision [7] and can create a more realistic life-like stereoscopic effect than “single-lens pseudo-stereoscopic” systems [1]. Furthermore, each separate image has a quality of 1 megapixel, or HD quality, and the processed 3-D image also has HD quality, which is superior to images created by existing stereoendoscopic systems. This stereoendoscopic system is combined with a 24-inch 3-D LCD, adopting circular micro-polarizing technology. Surgeons can see flicker-free 3-D images wearing lightweight passive polarizing glasses similar to lightly-tinted sunglasses. This system enables surgeons to switch between 3-D and 2-D content as well as view their surroundings without removing the glasses. In addition, the color reproduction such as red hues in this stereoendoscope may be superior to other existing stereoendoscopic systems for EES, although its outer diameter is a little larger than that of those systems [9].
Human factors associated with study design in the ergonomic research
We found in this study that 3-D visualization significantly improved the speed and accuracy of performance for the inexperienced subjects, which suggested that stereoendoscopy might offer a benefit to novice surgeons. However, in ergonomic research such as this study, it is difficult to objectively evaluate the feasibility of medical devices, because it is usually measured from a physician’s subjective standpoint and it can be influenced by some characteristic factors relevant to ergonomics such as order effect, carry-over effect, and learning effect. To minimize these issues [20], we tried to construct an objective and quantitative evaluation method in the light of ergonomic issues. We set two simple brief tasks that did not resemble actions that may be performed during a real EES. Furthermore, the subjects performed the tasks with an interval of more than 48 hours between the 3-D and 2-D modes. In addition, the subjects were able to practice only once under direct vision before the task to minimize a learning effect. Statistical analysis proved that these effects had not influenced the study results.
Previous reports have reported varied findings; therefore, the use of 3-D stereoendoscopes has been somewhat controversial. Some studies have described the superiority of the 3-D visualization over 2-D [3, 8, 16, 18, 19]; however, others have reported no advantage of 3-D over 2-D [5, 10, 17]. These conflicting results may be explained by the difference in 3-D imaging technology used, selection of study design and task, and original abilities of subjects to perceive depth information [11]. These factors are debatable and pose potential limitations of this study. First, the innate ability of stereopsis and hand–eye coordination vary widely among individuals [11, 19]. This was evident in this study (Fig. 5). Although stereoscopic ability of the subjects had not been objectively evaluated prior to the exercises in this study, all of them reported being able to perceive the 3-D image during the tasks under 3-D visualization. Hand–eye coordination also varies between individuals and can be positively influenced by activities such as video gaming, as recent studies have demonstrated [2, 14, 15]. Second, we only recruited inexperienced persons as subjects in this study, because our goal was to see how the visual condition itself influenced task performance and “experienced” surgeons may be highly individual in terms of experience of EES, leading to the inherent heterogeneity in the “experienced group”. Some studies have shown that experienced surgeons demonstrated no benefit with 3-D imaging [17, 20] because those referred to as “experienced surgeons” may have considerable variation in endoscopic skills and may have already been able to reconstruct 3-D images from 2-D images by integrating monocular depth cues [5, 14]. These factors can lead to a ceiling effect that influences the results of the study. Finally, the design of the tasks may still have room for improvement. The tasks in this study were based on those employed in training for laparoscopic surgery, and there may be more appropriate tasks for comparing basic performance under 2-D and 3-D conditions specifically for ESS.
Future demand for stereoendoscopy
In laparoscopic surgery, the necessity and importance of training are well established. Along with the innovation of technology and surgical concept, training systems have continued to develop and undergo modifications. In contrast, in ESS or neuroendoscopic surgery, the training of basic endoscopic skills has been less emphasized, probably because rhinologists routinely use endoscopes from their early residency period and a neuroendoscopist manipulates a single instrument in a simple to-and-fro movement in most situations. More complex procedures require meticulous manipulation in expanded EES inevitably demands that the surgeons have more advanced depth perception abilities and hand–eye coordination. Three-dimensional visualization technology is expected to be beneficial for improving depth perception and providing a shorter learning curve. In the current study, the merits of stereoendoscope were shown only in the fixed condition. It may be necessary to verify whether moving 3-D images would negate these merits and/or provoke eye strain or “simulator sickness,” although moving an endoscope may invoke motion parallax and help to reconstruct 3-D images in the brain in the 2-D setting. Future technological developments may provide us with an endoscope of smaller size dimensions, and better quality of 3-D vision, which could facilitate the clinical applications of a 3-D endoscopic system and allow further validation whether a 3-D system will shorten the learning curve of EES and enhance surgical safety and efficacy.
Conclusion
We constructed a method for objectively evaluating and comparing 3-D visualization and conventional 2-D visualization. A novel commercially available stereoendoscopic system was used for this purpose. This endoscope provides HD quality images under both 2-D and 3-D modes. Our laboratory study showed the advantage of 3-D visualization over conventional 2-D visualization for the inexperienced operator in the EES setting. This result does not conclusively prove that the stereoendoscopic system can offer comparable surgical efficiency, lower complication rates, or shorter learning curves. Further quantitative clinical studies should be designed to further investigate whether stereoendoscopy really provides benefits for patients.
References
Birkett DH, Josephs LG, Este-McDonald J (1994) A new 3-D laparoscope in gastrointestinal surgery. Surg Endosc 8(12):1448–1451
Boyle E, Kennedy AM, Traynor O, Hill AD (2011) Training surgical skills using nonsurgical tasks–can Nintendo Wii™ improve surgical performance? J Surg Educ 68(2):148–154
Brown SM, Tabaee A, Singh A, Schwartz TH, Anand VK (2008) Three-dimensional endoscopic sinus surgery: feasibility and technical aspects. Otolaryngol Head Neck Surg 138(3):400–402
Cappabianca P, Cavallo LM, Esposito F, De Divitiis O, Messina A, De Divitiis E (2008) Extended endoscopic endonasal approach to the midline skull base: the evolving role of transsphenoidal surgery. Adv Tech Stand Neurosurg 33:151–199
Chan AC, Chung SC, Yim AP, Lau JY, Ng EK, Li AK (1997) Comparison of two-dimensional vs three-dimensional camera systems in laparoscopic surgery. Surg Endosc 11(5):438–440
Chen G, Ling F (2010) A new plastic model of endoscopic technique training for endonasal transsphenoidal pituitary surgery. Chin Med J 123(18):2576–2579
Durrani AF, Preminger GM (1995) Three-dimensional video imaging for endoscopic surgery. Comput Biol Med 25(2):237–245
Fraser JF, Allen B, Anand VK, Schwartz TH (2009) Three-dimensional neurostereoendoscopy: subjective and objective comparison to 2D. Minim Invasive Neurosurg 52(1):25–31
Barkhoudarian G, Romero AD, Laws ER (2013) Evaluation of the Three-Dimensional Endoscope in Transsphenoidal Surgery. Neurosurgery DOI: 10.1227/NEU.0b013e31828ba962
Hanna GB, Shimi SM, Cuschieri A (1998) Randomised study of influence of two-dimensional versus three-dimensional imaging on performance of laparoscopic cholecystectomy. Lancet 351(9098):248–251
Hofmeister J, Frank TG, Cuschieri A, Wade NJ (2001) Perceptual aspects of two-dimensional and stereoscopic display techniques in endoscopic surgery: review and current problems. Semin Laparosc Surg 8(1):12–24
Kassam A, Thomas AJ, Snyderman C, Carrau R, Gardner P, Mintz A, Kanaan H, Horowitz M, Pollack IF (2007) Fully endoscopic expanded endonasal approach treating skull base lesions in pediatric patients. J Neurosurg 106(2 Suppl):75–86
Kassam AB, Gardner PA, Snyderman CH, Carrau RL, Mintz AH, Prevedello DM (2008) Expanded endonasal approach, a fully endoscopic transnasal approach for the resection of midline suprasellar craniopharyngiomas: a new classification based on the infundibulum. J Neurosurg 108(4):715–728
Kennedy AM, Boyle EM, Traynor O, Walsh T, Hill AD (2011) Video gaming enhances psychomotor skills but not visuospatial and perceptual abilities in surgical trainees. J Surg Educ 68(5):414–420
Rosenberg BH, Landsittel D, Averch TD (2005) Can video games be used to predict or improve laparoscopic skills? J Endourol 19(3):372–376
Roth J, Singh A, Nyquist G, Fraser JF, Bernardo A, Anand VK, Schwartz TH (2009) Three-dimensional and 2-dimensional endoscopic exposure of midline cranial base targets using expanded endonasal and transcranial approaches. Neurosurgery 65(6):1116–1128
Shah RN, Leight WD, Patel MR, Surowitz JB, Wong YT, Wheless SA, Germanwala AV, Zanation AM (2011) A controlled laboratory and clinical evaluation of a three-dimensional endoscope for endonasal sinus and skull base surgery. Am J Rhinol Allergy 25(3):141–144
Tabaee A, Anand VK, Fraser JF, Brown SM, Singh A, Schwartz TH (2009) Three-dimensional endoscopic pituitary surgery. Neurosurgery 64(5 Suppl 2):288–293
Taffinder N, Smith SG, Huber J, Russell RC, Darzi A (1999) The effect of a second-generation 3D endoscope on the laparoscopic precision of novices and experienced surgeons. Surg Endosc 13(11):1087–1092
Votanopoulos K, Brunicardi FC, Thornby J, Bellows CF (2008) Impact of three-dimensional vision in laparoscopic training. World J Surg 32(1):110–118
Wasserzug O, Margalit N, Weizman N, Fliss DM, Gil Z (2010) Utility of a three-dimensional endoscopic system in skull base surgery. Skull Base 20(4):223–228
Wedmid A, Llukani E, Lee DI (2011) Future perspectives in robotic surgery. BJU Int 108(6 Pt 2):1028–1036
Yamauchi Y, Yamashita J, Morikawa O, Hashimoto R, Mochimaru R, Fukui Y, Uno H, Yokoyama K (2002) Surgical Skill Evaluation by Force Data for Endoscopic Sinus Surgery Training System. Lecture Notes in Computer Science 2488:44–51
Acknowledgment
We thank MACHIDA Endoscope Co. Ltd. (Tokyo, Japan) and SHINKO OPTICAL Co. Ltd. (Tokyo, Japan) for allowing us to use their stereoendoscopic system for this study. We also thank the medical students who participated in this study.
Ethical standards
The authors declare that this work met all ethical standards for research and scientific publication.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kawanishi, Y., Fujimoto, Y., Kumagai, N. et al. Evaluation of two- and three-dimensional visualization for endoscopic endonasal surgery using a novel stereoendoscopic system in a novice: a comparison on a dry laboratory model. Acta Neurochir 155, 1621–1627 (2013). https://doi.org/10.1007/s00701-013-1757-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-013-1757-2