
Abstract
Purpose
Pancreatic ductal adenocarcinoma (PDAC) is the most common type of pancreatic cancer. It is an aggressive malignancy associated with poor prognosis because of recurrence, metastasis, and treatment resistance. Aberrant glycosylation of cancer cells triggers their migration and invasion and is considered one of the most important prognostic cancer biomarkers. The current study aimed to identify glycan alterations and their relationship with the malignant potential of PDAC.
Methods
Using a lectin microarray, we evaluated glycan expression in 62 PDAC samples. Expression of fucosyltransferase 8 (FUT8), the only enzyme catalyzing core fucosylation, was investigated by immunohistochemistry. The role of FUT8 in PDAC invasion and metastasis was confirmed using an in vitro assay and a xenograft peritoneal metastasis mouse model.
Results
The microarray data demonstrated that core fucose-binding lectins were significantly higher in carcinoma than in normal pancreatic duct tissues. Similarly, FUT8 protein expression was significantly higher in carcinoma than in normal pancreatic duct tissues. High FUT8 protein expression was significantly associated with lymph-node metastases and relapse-free survival. FUT8 knockdown significantly reduced the invasion in PDAC cell lines and impaired peritoneal metastasis in the xenograft model.
Conclusions
The findings of this study provide evidence that FUT8 plays a pivotal role in PDAC invasion and metastasis and might be a therapeutic target for this disease.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Surgical resection offers the only chance of cure for pancreatic ductal adenocarcinoma (PDAC), the most commonly diagnosed pancreatic cancer. Adjuvant chemotherapy following surgery may improve the prognosis; however, the 5-year survival rate is not more than 44% [1]. Despite improvements in chemotherapeutic agents, the overall survival of unresectable PDAC is only 8.5 months, which highlights the need for alternate therapeutic strategies.
We have investigated tumor-associated glycans; in particular, lectins, as potential new cancer therapeutic targets. Lectins are glycan-binding proteins that selectively bind particular glycan structures. Glycan profiling using lectin microarrays enables the detection of glycan variants in serum and tissues and provides useful information on biologically relevant glycosylation differences between normal and tumor tissues, requiring only a small sample [2]. In previous studies based on lectin microarray analysis, we identified key lectins that might serve as predictors of cancer recurrence in colorectal cancer and gastric cancer [3, 4]. We detected specific alterations in glycans in pancreatic cystic neoplasms and identified two particular lectins, Aspergillus oryzae lectin (AOL) and Aleuria aurantia lectin (AAL), that were associated with fucosylation [5]. AOL and AAL commonly recognize α-1,6-fucose (core fucose), the transfer of which is mediated by fucosyltransferase 8 (FUT8) [6]. Glycosylation is one of the most important cellular mechanisms to regulate several biological functions, and aberrant glycosylation, especially fucosylation, sialylation, and branched N-glycans, are associated with cancer-cell proliferation, migration, and invasion [7, 8]. Glycan alterations on glycoproteins or glycoconjugates are potentially useful, not only as biomarkers, but also as therapeutic targets [8, 9]. In pancreatic cancer, carbohydrate antigen 19-9 (CA19-9), a glycan known as the sialyl-Lewis A (sLeA) antigen, has been used for diagnostic screening and as a prognostic marker [10, 11], and fucosylation is also a promising candidate diagnostic marker or therapeutic target [12]. In our previous study, we found that FUT8 protein expression was significantly higher during the development of adenoma into carcinoma than that in normal pancreatic duct tissue [5]. However, the role of core fucosylation and the detailed underlying mechanism of malignant transformation are still unknown.
To our knowledge, lectin microarrays have not been used to analyze alterations in glycans in PDAC. We conducted the present study to analyze glycan alterations in PDAC by lectin microarray-based glycan profiling and to investigate the relationship between fucosylation, especially core fucosylation, and malignant potential, focusing on the cellular functions of FUT8, in vitro and in vivo.
Methods
Patients and clinical samples
We collected surgical specimens from 62 patients who underwent curative resection of PDAC at the Department of Gastroenterological and Pediatric Surgery, Oita University Faculty of Medicine, between June, 2006 and December, 2015 and for whom medical records were available. The patients included 26 women and 36 men, ranging in age from 42 to 84 years (mean ± standard deviation, 70 ± 8 years). The tumors were located in the pancreatic head (Ph) in 38 patients and in the body and tail (Pbt) in 24 patients. Tumor size ranged from 10 to 65 mm (31.0 ± 11.4 mm). Thirty-nine patients (63%) had lymph-node metastases and 54 patients (87%) received adjuvant chemotherapy after surgery. Tumor recurrence developed in 51 patients (82%). All samples were collected with informed consent from the patients.
Sample preparation and lectin microarray
Tissue samples were fixed in formalin, embedded in paraffin, and sectioned at a thickness of 5 μm. Deparaffinized sections were placed on dedicated glass slides and stained with hematoxylin and eosin (HE). Normal pancreatic duct and carcinoma sections were excised from the same sample using laser microdissection. Section areas of all samples were equalized [5].
Lectin microarray analysis using LecChip™ (GP Biosciences Ltd.), which contains 45 lectins, was conducted as described previously [3,4,5]. Briefly, cells from dissociated tissue samples were washed with phosphate-buffered saline (PBS), pelleted via centrifugation, solubilized in 20 μL of PBS containing 0.5% Nonidet P40, and sonicated in a Bioruptor UCW-310 (Cosmo Bio, Carlsbad, CA, USA). Glycoprotein fractions were labeled fluorescently with cyanine-3 dissolved at 250 ng/mL in probing solution (GP Biosciences Ltd., Yokohama, Japan) and applied to each well of a LecChip™, which was then incubated in the dark under > 80% humidity and at 20 °C for 15 h. Prior to sample application, the LecChip™ wells were washed three times with probing solution to reduce the background. After incubation, fluorescence images of the lectin arrays were acquired using an evanescent-field fluorescence scanner GlycoStation™ Reader 1200 (GP Biosciences Ltd.), and the data were analyzed using GlycoStation™ Tool Pro Suite 1.5.
Immunohistochemical analysis of FUT8 expression in PDAC
Immunohistochemical analysis of FUT8 was conducted as described previously [5]. Formalin-fixed, paraffin-embedded tissue specimens were cut into 3-μm slices and deparaffinized, and endogenous peroxidase activity was blocked for 20 min with 3% hydrogen peroxidase. Antigens were retrieved by autoclaving in 10 mM citrate buffer solution (105 °C, pH 6.0) for 5 min. The tissue sections were incubated with a primary rabbit polyclonal antibody against FUT8 (cat. no. HPA043410, 1:100; Atlas Antibodies). Tissue specimens were stained immunohistochemically using a standard avidin–biotin-peroxidase method. Antigen–antibody complexes were visualized with 3,3′-diaminobenzidine. The sections were counterstained with hematoxylin. Two investigators independently graded FUT8 tissue staining as 0 (negative), 1 (weak), 2 (moderate), or 3 (strong), as described previously [5, 13, 14], and the tumors were divided into low (score 0 or 1) or high (score 2 or 3) FUT8 protein expression groups. Few interobserver differences were observed in the staining judgments.
Cell lines
The human pancreatic cancer cell lines PANC-1, MIA-PaCa-2, and PK-1 were provided by the Japanese Cancer Research Bank (Tokyo, Japan). PK-8 was obtained from the Cell Resource Center for Biomedical Research Institute of Development, Tohoku University. PANC-1 and MIA-PaCa-2 cells were cultured in Dulbecco’s modified Eagle’s medium (FUJIFILM Wako Pure Chemical Corp., Osaka, Japan) containing 10% fetal bovine serum (FBS) and antibiotics, and PK-1 and PK-8 were cultured in Roswell Park Memorial Institute medium (RPMI 1640) (FUJIFILM Wako Pure Chemical Corp.) containing 10% FBS and antibiotics.
FUT8 RNA interference
Small interfering RNA (siRNA)-mediated FUT8 knockout was established as described previously [13]. Lipofectamine™ RNAiMAX Transfection Reagent (Thermo Fisher Scientific, Waltham, MA, USA) was used to transfect siRNA into the cells. Briefly, 6 μL of 10 μM negative control siRNA (NON-TARGETplus Non-Targeting siRNAs, D-001810–10-05, Dharmacon, Lafayette, CO, USA) or FUT8 siRNA (ON-TARGETplus Human FUT8 siRNA SMARTpool, L-003668-00-0005; Dharmacon) was mixed in 2000 μL of Opti-MEM with 10 μL Lipofectamine™ and added to a dish (100 mm diameter). After incubation at room temperature for 25 min, cultured cells (1 × 106) in 3000 μL of Opti-MEM were added. Regular medium (5000 μL) containing 20% FBS was added 3 h after transfection. Cells were harvested for quantitative reverse transcription (RT-q) PCR or western blotting 48 h after the addition of siRNA.
RT-qPCR
Total RNA was extracted from the pancreatic cancer cell lines using an RNeasy Mini Kit (Qiagen, Venlo, Netherlands) [15]. One microgram of total RNA was reverse-transcribed to cDNA using a Verso cDNA Synthesis Kit (Thermo Fisher Scientific). qPCRs were run in a LightCycler 96 Real-time PCR System (Roche, Basel, Switzerland). Primer sets for FUT8 and actin beta (ACTB) (FUT8-F, 5′-CAGACAGATGGAGCAGGTGA-3′ and FUT8-R, 5′-CCATAGCCACAGCCTTTGTT-3′; and ACTB-F, 5′-CGGCATCGTCACCAACTG-3′ and ACTB-R, 5′-AACATGATCTGGGTCATCTTCTC-3′) were obtained from Fasmac (Kanagawa, Japan). ACTB was used as an internal control for the normalization of FUT8 expression levels.
Western and lectin blot analysis
Western blot analysis was conducted as described previously [13]. FUT8-knockdown and control PK-1 and PK-8 cells were lysed in 1 × radioimmunoprecipitation (RIPA) buffer (Thermo Fisher Scientific) and incubated on ice for 10 min. The samples were then centrifuged at 15,000×g for 15 min. Protein concentrations were calculated using a BCA protein assay kit (Bio-Rad, Hercules, CA, USA). Samples were resuspended in RIPA buffer and heated to 96 °C for 5 min. Equal amounts of protein (20 μg) were separated by 4–15% sodium dodecyl sulfate–polyacrylamide gel electrophoresis and transferred onto Immobilon-P PVDF Membranes (Millipore, Billerica, MA). The membranes were blocked with PVDF Blocking Reagent for Can Get Signal (Toyobo Co., Ltd., Osaka, Japan) in PBS and 0.05% Tween-20 (PBS-T) at room temperature for 1 h and then incubated with an antibody against FUT8 (cat. no. HPA040863, 1:500; Atlas Antibodies) at 4 °C overnight. After three washes in PBS-T, the membranes were incubated with horseradish-peroxidase-conjugated anti-rabbit IgG antibody (Immuno-Biological Laboratories Co., Ltd., Gumma, Japan) in Can Get Signal® Immunoreaction Enhancer Solution (Cosmo Bio Co., Ltd., Tokyo, Japan). The membranes were washed three times with PBS-T and immunoreactive bands were then visualized using Immobilon Western Chemiluminescent HRP Substrate (Thermo Fisher Scientific). The membranes were stripped and probed with an anti-ACTB antibody (Wako Pure Chemical Industries, Ltd., Osaka, Japan) as a loading control. Lectin blot analysis was performed in the same manner as for western blot. After blocking, the membrane was incubated with biotinylated AAL (cat. no. B-1395, 1:400; Vector Laboratories, Inc., CA, USA) for 30 min at room temperature. After washing, lectin reactive proteins were detected using streptavidin-HRP and an enhanced chemiluminescence kit.
Cell proliferation assay
The proliferation of PK-1 and PK-8 cells was measured using a methylthiazole tetrazolium (MTT) assay (Sigma-Aldrich, St. Louis, MO, USA) following the manufacturer’s protocol. Briefly, off-target control siRNA- or FUT8 siRNA-transfected PK-1 and PK-8 cells (1000/well) were cultured in a 96-well plate in regular culture medium in triplicate for 24–96 h. An MTT-labeling reagent (10 μL) was added to each well of the plate. After 4 h’ incubation in a humidified atmosphere, solubilization solution was added to each well. After incubation overnight, the absorbance at 650 nm was measured using a microplate reader (Multiskan FC, Thermo Fisher Scientific).
Matrigel invasion assay
A Matrigel invasion assay was conducted as described previously [15, 16], using a 24-well BioCoat Matrigel Invasion Chamber with a pore size of 8 μm (BD Biosciences, San Jose, CA, USA) according to the manufacturer’s protocol. Before the experiment, the top chamber was rehydrated with RPMI 1640 at 37 °C for 1 h. Then, 1.0 × 104 cells in 500 μL of serum-free medium were placed in the top chamber. The bottom chamber contained 10% FBS as a chemoattractant. After 24 h’ incubation, non-invaded cells on the upper surface of the filter were removed using a cotton swab and cells that had migrated through the membrane were stained using Diff-Quick Stain™ (Sysmex, Kobe, Japan). The filter was excised from the chamber using a scalpel and the number of invaded cells was counted under a microscope.
Xenograft model
We used 5-week-old male BALB/c nu/nu mice (Japan SLC, Inc., Hamamatsu, Japan) to establish subcutaneous transplant and peritoneal dissemination mouse models of human pancreatic cancer. For the subcutaneous transplant model, 1 × 106 PK-1 cells suspended in 100 μL of PBS were injected subcutaneously using a 27-gauge needle. For the peritoneal dissemination model, 2 × 106 cells suspended in 100 μL of PBS were injected into the peritoneal cavity using a 27-gauge needle. The mice were killed 2 weeks after implantation to check for subcutaneous and metastatic tumors. The number of disseminated nodules per 1 cm2 in visceral peritoneum of the abdominal wall were counted at two sites in the same specimen. The average numbers in each specimen were compared between the control and KD groups. The animal experiments were approved by the Committee on the Use of Live Animals for Teaching and Research and were conducted in accordance with the Animal Care and Use Committee guidelines of Oita University.
Statistical analysis
Numerical data are expressed as the mean ± the standard deviation. Differences between two variables were compared using Fisher’s exact test or a Mann–Whitney test. Other data were evaluated using one-way analysis of variance and Bonferroni tests for multiple comparisons. Kaplan–Meier curves were created for overall survival and relapse-free survival, and survival data were analyzed using a log-rank test. All statistical analyses were performed using SPSS 23.0 (SPSS Inc., Chicago, IL, USA), and P < 0.05 was considered significant.
Results
Lectin microarray-based glycan profiling of PDAC samples
To characterize altered glycosylation patterns in PDAC, we performed lectin microarray-based glycan profiling of PDAC and normal pancreatic ductal tissues obtained from 62 patients. Table 1 summarizes the lectin-glycan binding signals for the 45 lectins in the microarray in normal pancreatic duct and carcinoma tissues. Twelve lectins yielded significantly different signals in the normal pancreatic duct and carcinoma tissues. The signals for AOL, AAL, phytohemagglutinin-L (PHA(L)), Hippeastrum hybrid lectin (HHL), and Bauhinia purpurea lectin (BPL) were obviously higher in carcinoma than in normal pancreatic duct (P < 0.001). AOL and AAL selectively bind to Fucα-1,6-GlcNAc, and PHA(L), HHL, and BPL bind to GlcNAcβ-1,6-Man, Manα-1,6-(Manα-1,3-)Man, and Galβ-1,3-GalNAc, respectively. These results suggested that several protein glycosylation pathways, including α-1,6-fucosylation, may be activated in the carcinoma tissue.
High FUT8 expression is associated with tumor recurrence and metastasis in PDAC
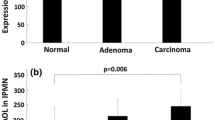
The lectin microarray-based glycan profiling revealed that distinct glycosylations, especially α-1,6-fucosylation mediated by FUT8 (α-1,6-fucosyltransferase), were increased in PDAC. Therefore, we examined FUT8 expression in carcinoma and normal pancreatic duct tissues by immunohistochemistry (IHC). Figure 1a shows representative brightfield FUT8 IHC images of normal pancreatic duct and carcinoma. FUT8 was strongly and locally expressed in carcinoma tissue, but not in the normal pancreatic duct. Figure 1b shows quantitative IHC data for the 62 patients. FUT8 protein expression was significantly higher in carcinoma than in normal pancreatic duct tissues.

Immunohistochemical analysis of fucosyltransferase 8 (FUT8) protein expression. a FUT8 protein expression in normal pancreatic duct and carcinoma tissues. Scale bar = 500 μm. b FUT8 expression was significantly higher in carcinoma than in normal pancreatic duct tissues (P < 0.01)
To investigate the potential relationship between FUT8 expression and clinicopathological features in the PDAC patients, we compared patient age and gender, tumor size and location, lymph-node metastasis, recurrence, and tumor markers (CEA and CA19-9) between low and high FUT8 expression groups (Table 2). We found a significant difference in the occurrence of lymph node metastasis in patients with low FUT8 expression and those with high FUT8 expression (P = 0.033). Tumor recurrence tended to develop more frequently in the high expression group (P = 0.059). Figure 2 shows the Kaplan–Meier survival curves for overall survival and relapse-free survival for the FUT8 high and low expression groups. There were no clear differences in overall survival (Fig. 2a); however, patients with high FUT8 expression showed significantly worse relapse-free survival than those with low expression (P = 0.039; Fig. 2b). Together, these results suggest strongly that FUT8 expression may affect tumor recurrence and metastasis in PDAC.

Overall survival and relapse-free survival of patients with pancreatic ductal adenocarcinoma (PDAC). a There was no significant difference between the high- and low-FUT8 expression groups of patients with PDAC (P = 0.415). b High FUT8 expression was significantly associated with worse relapse-free survival of patients with PDAC (P = 0.039)
FUT8 knockdown reduces tumor-cell invasion in vitro
To evaluate the role of α-1,6-fucosylation in tumor-cell growth, migration, and metastasis in vitro, we knocked down FUT8 using siRNA. First, we measured the FUT8 gene expression levels in the PDAC cell lines PANC-1, MIA-PaCa-2, PK-1, and PK-8, by RT-qPCR. FUT8 mRNA expression was significantly higher in the PK-1 and PK-8 cells than in the other cell lines (Fig. 3a). Downregulation of FUT8 expression after siRNA transfection in PK-1 and PK-8 cells was confirmed by RT-qPCR and western blot analysis (Fig. 3b, c). In lectin blot analysis, AAL was lower in FUT8 knockdown PK-1 cells than in normal PK-1 cells (Fig. 4). To evaluate the effect of FUT8 knockdown on cancer cell progression in PK-1 and PK-8 cells, we conducted cell proliferation and invasion assays. The MTT cell proliferation assay is used widely to measure cell viability. We observed no significant difference in cell proliferation between the control and FUT8 knockdown cells (Fig. 5). A Matrigel invasion assay revealed a remarkable decrease in cell migration upon FUT8 knockdown in both cell lines (Fig. 6).

FUT8 mRNA and protein expression in pancreatic cell lines. aFUT8 mRNA expression in the pancreatic cancer cell lines, PANC-1 and MIA-PaCa-2 (low FUT8 expression), and PK-1 and PK-8 (high FUT8 expression) as determined by RT-qPCR. FUT8 mRNA expression was significantly higher in PK-1 and PK-8 cells than in PANC-1 and MIA-PaCa-2 cells (n = 3, P < 0.05, PK-1 vs. PANC-1; PK-8 vs. PANC-1; PK-1 vs. MIA-PaCa-2; PK-8 vs. MIA-PaCa-2; PK-1 vs. PK-8). b Effect of siRNA-mediated FUT8 knockdown in PK-1 cells. FUT8 mRNA (left panel) and protein (right panel) were downregulated in the PK-1 cells (n = 4, P < 0.05; left panel). c Effect of siRNA-mediated FUT8 knockdown in PK-8 cells. FUT8 mRNA (left panel) and protein (right panel) expression were downregulated in PK-8 cells (n = 4, P < 0.05; left panel)

Lectin blot analysis using Aleuria aurantia lectin (AAL) in PK-1 cells. AAL binding was decreased in FUT8 knockdown PK-1 cells versus that in control PK-1 cells

Effect of FUT8 knockdown on cell proliferation in pancreatic cancer cells. aFUT8 knockdown did not affect cell proliferation in PK-1 cells (n = 3). bFUT8 knockdown did not affect cell proliferation in PK-8 cells (n = 3)

Effect of FUT8 knockdown on the invasiveness of pancreatic cancer cells. a Representative images of invaded cells in PK-1. Scale bar = 100 μm. b The number of invaded FUT8 siRNA-transfected cells was significantly lower than the number of invaded control PK-1 cells (n = 9, P < 0.01). c Representative images of invaded cells in PK-8. Scale bar = 100 μm. d The number of invaded FUT8 siRNA-transfected cells was significantly lower than the number of invaded control PK-8 cells (n = 5, P < 0.01)
FUT8 knockdown reduces peritoneal metastasis in vivo
For phenotypic characterization of xenograft tumors in vivo, we established and analyzed subcutaneous xenograft mouse models using PK-1 cells treated with non-targeting siRNA (n = 4) or FUT8 siRNA (n = 4). There were no significant differences in the size or histological morphology of subcutaneous tumor masses (data not shown). Next, we evaluated the effect of FUT8 knockdown in a peritoneal metastasis xenograft model of pancreatic cancer. Countless tumor nodules had formed in the visceral peritoneum of the abdominal wall of the mice injected intraperitoneally with non-targeting siRNA-transfected PK-1 cells (control group; n = 3), whereas in the mice inoculated with FUT8 siRNA-transfected PK-1 cells (KD group; n = 3), peritoneal nodules were rarely observed (Fig. 7). Figure 7a shows representative macroscopic views of the inner side of the abdominal wall in both groups. The abdominal wall surface was rougher in the control group than in the KD group (Fig. 7a). Microscopic images of HE-stained tissue slices confirmed that tumor nodule size and number were drastically decreased in the KD comparison with those in the control group (Fig. 7b, c and Fig. 8).

Effect of FUT8 knockdown in a xenograft mouse model of peritoneal dissemination. a Representative images of peritoneal dissemination in the xenograft model. Disseminated tumor nodules in the visceral peritoneum of the abdominal wall were obviously lower in the mice that had received FUT8 siRNA-transfected PK-1 cells than in the mice that had been injected with non-targeting siRNA-transfected control PK-1 cells. b Representative images of the histological findings from the abdominal wall of a mouse with HE staining. Solid masses were seen in the mice that had received control PK-1 cells (arrowheads), whereas nodules were barely seen in the mice that had received FUT8 siRNA-transfected PK-1 cells (arrowheads). Scale bar = 500 μm. c Enlarged images of the same samples as in (b). A solid mass invaded the peritoneum of mice that had received control PK-1 cells, whereas just small nodules adhered to the peritoneum of mice injected with FUT8 siRNA-transfected PK-1 cells. Scale bar = 100 μm

Quantitative analysis of the disseminated metastasis. The number of disseminated tumor nodules in the visceral peritoneum of the abdominal wall was significantly lower in the mice that had received FUT8 siRNA-transfected PK-1 cells than in the mice that had been injected with non-targeting siRNA-transfected control PK-1 cells (n = 3, P < 0.01)
Discussion
Glycans, consisting of monosaccharides, are expressed on the surface of cells, and glycosylation is a modification that involves the addition of glycans to proteins and lipids. Glycoproteins and glycolipids play important roles in cell recognition, interaction, and signaling [17, 18]. In cancer, glycosylation is a key cellular mechanism and may contribute to malignant transformation, tumor progression, and metastasis. Notably, sialylation, increased branched-glycan structures, and fucosylation occur frequently in cancer [7, 8]. Altered glycan structures also affect cellular signaling and tumor cell–cell adhesion, and are crucial in the interplay between cancer cells and their surrounding environment [18, 19]. Glycans interact with glycan-binding proteins called lectins, which selectively recognize glycan structures [2, 9]. Because of their specific affinity for distinct glycans, lectins can detect tumor-associated glycans and glycoproteins in clinical samples [20].
In the present study, we used a 45-lectin microarray to evaluate glycan expression in the surgical specimens of PDAC patients. The analysis revealed that lectin-glycan binding signals of AOL, AAL, PHA(L), HHL, and BPL were significantly higher in carcinoma than in normal pancreatic duct tissues (Table 1). PHA(L) and HHL have been correlated with colorectal cancer [3, 21], and an increased BPL signal has also been recognized in pancreatic cystic neoplasms [5]. We focused on AOL and AAL, which have the strongest preference for core fucosylation, also called α-1,6-fucosylation [6]. Core fucosylation comprises the transfer of α-1,6‐fucose to the innermost GlcNAc residue of N‐glycans by FUT8 [8, 22,23,24]. Core fucosylation mediated by FUT8 is one of the most important glycan modifications involved in cancer and inflammation [8, 25, 26]. Overexpression of core fucosylation structures and FUT8 have been reported in several cancers, including prostate cancer, non-small cell lung cancer, colon cancer, and breast cancer [13, 14, 27, 28]. In hepatocellular carcinoma (HCC), core fucosylated α-fetoprotein is a well-known biomarker for detecting early cancer. HCC is distinguished from liver cirrhosis depending on whether α-fetoprotein has a core fucose structure [29]. Fucosylated glycans are synthesized by a range of fucosyltransferases (FUT1–11). CA19-9 (sLeA), the most widely used biological marker in PDAC, is also a fucosylated glycan [10]; however, there have been few studies on the core fucosylation associated with PDAC. In this study, we identified core fucosylation as a specific glycan modification in PDAC by lectin microarray-based glycan profiling of clinical specimens.
We reported previously that FUT8 expression increases gradually from normal pancreatic duct to adenoma and then carcinoma in an intraductal papillary mucinous neoplasm, a mucinous cystic tumor of the pancreas with malignant transformation potential [5]. This suggests that increased FUT8 expression, and thus, activation of the core fucosylation reaction, may play a key role in the malignancy of pancreatic cancer. In the present study, FUT8 expression was also higher in carcinoma than in normal pancreatic duct in PDAC patients. Moreover, according to the clinicopathological analysis, high FUT8 expression in PDAC was associated with lymph-node metastasis. The recurrence rate also tended to be higher and the prognosis was likely to be worse under high FUT8 expression. Overall survival was not related to FUT8 expression, possibly because of improved chemotherapeutics, but relapse-free survival was significantly lower in the high-expression group. Chen et al. [14] reported that upregulation of FUT8 correlated with the development of distant metastasis and poor prognosis in patients with lung cancer. Agrawal et al. [30] demonstrated that FUT8 expression was higher in metastatic than in primary lesions of malignant melanoma, and concluded that FUT8 triggers tumor invasion and metastasis. Ito et al. [31] reported that high expression of FUT8 was linked to tumor size and lymph-node metastasis in thyroid cancer. To our best knowledge, the current study is the first to show that FUT8 expression is directly associated with cancer lymph-node metastasis and recurrence of PDAC. Future studies should focus on the cellular functions of FUT8 in distal metastasis and the possible mechanism underlying cancer recurrence.
We used siRNA-mediated gene knockdown in appropriate cancer cell lines and clinical models to reveal the cellular functions of FUT8 in vivo and in vitro. FUT8 knockdown reduced cell invasiveness, but not cell proliferation in PDAC cell lines. Furthermore, peritoneal metastasis was obviously suppressed in a xenograft mouse model. There have been a few recent reports on the molecular mechanism of FUT8 in cancer progression and metastasis. Cheng et al. [32] reported that HCC cells with high metastatic potential expressed higher levels of FUT8 than cells with low metastatic potential. In prostate cancer cell lines, FUT8 was overexpressed in aggressive cells, but was nearly undetectable in non-aggressive cells [13]. The suppression of FUT8 in aggressive prostate cancer cells decreased cell migration significantly, but did not affect cell proliferation [13]. These findings are consistent with our results in vitro. Several studies have also shown that FUT8 stimulates cancer invasiveness and metastasis by inducing epithelial–mesenchymal transition (EMT). Tu et al. [16] demonstrated that FUT8 is upregulated during EMT of cancer cells, and that core fucosylation of transforming growth factor-β (TGF-β) receptor complexes enhanced ligand binding and promoted downstream signaling in breast cancer cell lines. In malignant melanoma, core fucosylation impacted L1 cell adhesion molecule (L1CAM) cleavage and the ability of L1CAM to support melanoma invasion [30]. In pancreatic cancer, EMT is often implicated in the metastatic process and the TGF-β pathway is the master regulator of EMT [33]. L1CAM is also involved in the metastatic potential of pancreatic cancer [34]. Hence, our results suggest strongly that FUT8 and its transglycosylation activity play a pivotal role in PDAC; however, the target molecules of FUT8 and downstream signaling remain to be unraveled.
The present study had some limitations. First, we investigated FUT8 protein expression by IHC in PDAC specimens, but we did not evaluate FUT8 activity. Second, the number of patients was insufficient to establish clear associations between FUT8 and clinicopathological data. Finally, we did not demonstrate the quantitative in vivo data. Thus, the effect of FUT8 suppression should be investigated using quantitative evaluation on the basis of in-vivo images.
To our knowledge, this is the first study to demonstrate upregulation of FUT8 expression in PDAC. Our findings suggest that FUT8-mediated fucosylation is associated with cancer invasiveness, lymph-node metastasis, peritoneal metastasis, and the poor prognosis of PDAC. In conclusion, FUT8 may be related to the malignant potential of PDAC and could be a key driver of metastasis, associated with the poor prognosis of cancers. Further studies to establish new reliable diagnostic markers and effective therapeutics targeting core fucosylation in PDAC are ongoing.
References
Uesaka K, Boku N, Fukutomi A, Okamura Y, Konishi M, Matsumoto I, et al. Adjuvant chemotherapy of S-1 versus gemcitabine for resected pancreatic cancer: a phase 3, open-label, randomised, non-inferiority trial (JASPAC 01). Lancet. 2016;388:248–57.
Zhang L, Luo S, Zhang B. The use of lectin microarray for assessing glycosylation of therapeutic proteins. MAbs. 2016;8:524–35.
Nakajima K, Inomata M, Iha H, Hiratsuka T, Etoh T, Shiraishi N, et al. Establishment of new predictive markers for distant recurrence of colorectal cancer using lectin microarray analysis. Cancer Med. 2015;4:293–302.
Futsukaichi T, Etoh T, Nakajima K, Daa T, Shiroshita H, Shiraishi N, et al. Decreased expression of Bauhinia purpurea lectin is a predictor of gastric cancer recurrence. Surg Today. 2015;45:1299–306.
Watanabe K, Ohta M, Yada K, Komori Y, Iwashita Y, Kashima K, et al. Fucosylation is associated with the malignant transformation of intraductal papillary mucinous neoplasms: a lectin microarray-based study. Surg Today. 2016;46:1217–23.
Matsumura K, Higashida K, Ishida H, Hata Y, Yamamoto K, Shigeta M, et al. Carbohydrate binding specificity of a fucose-specific lectin from Aspergillus oryzae: a novel probe for core fucose. J Biol Chem. 2007;282:15700–8.
Christiansen MN, Chik J, Lee L, Anugraham M, Abrahams JL, Packer NH. Cell surface protein glycosylation in cancer. Proteomics. 2014;14:525–46.
Pinho SS, Reis CA. Glycosylation in cancer: mechanisms and clinical implications. Nat Rev Cancer. 2015;15:540–55.
Ho WL, Hsu WM, Huang MC, Kadomatsu K, Nakagawara A. Protein glycosylation in cancers and its potential therapeutic applications in neuroblastoma. J Hematol Oncol. 2016;9:100.
Munkley J. The glycosylation landscape of pancreatic cancer. Oncol Lett. 2019;17:2569–75.
Shibata K, Iwaki K, Kai S, Ohta M, Kitano S. Increased levels of both carbohydrate antigen 19–9 and duke pancreatic monoclonal antigen type 2 reflect postoperative prognosis in patients with pancreatic carcinoma. Pancreas. 2009;38:619–24.
Miyoshi E, Moriwaki K, Terao N, Tan CC, Terao M, Nakagawa T, et al. Fucosylation is a promising target for cancer diagnosis and therapy. Biomolecules. 2012;2:34–45.
Wang X, Chen J, Li QK, Peskoe SB, Zhang B, Choi C, et al. Overexpression of alpha (1,6) fucosyltransferase associated with aggressive prostate cancer. Glycobiology. 2014;24:935–44.
Chen CY, Jan YH, Juan YH, Yang CJ, Huang MS, Yu CJ, et al. Fucosyltransferase 8 as a functional regulator of nonsmall cell lung cancer. Proc Natl Acad Sci USA. 2013;110:630–5.
Ichimanda M, Hijiya N, Tsukamoto Y, Uchida T, Nakada C, Akagi T, et al. Downregulation of dual-specificity phosphatase 4 enhances cell proliferation and invasiveness in colorectal carcinomas. Cancer Sci. 2018;109:250–8.
Tu CF, Wu MY, Lin YC, Kannagi R, Yang RB. FUT8 promotes breast cancer cell invasiveness by remodeling TGF-beta receptor core fucosylation. Breast Cancer Res. 2017;19:111.
Glavey SV, Huynh D, Reagan MR, Manier S, Moschetta M, Kawano Y, et al. The cancer glycome: carbohydrates as mediators of metastasis. Blood Rev. 2015;29:269–79.
Rodrigues JG, Balmana M, Macedo JA, Pocas J, Fernandes A, de-Freitas-Junior JCM, et al. Glycosylation in cancer: selected roles in tumour progression, immune modulation and metastasis. Cell Immunol. 2018;333:46–57.
Oliveira-Ferrer L, Legler K, Milde-Langosch K. Role of protein glycosylation in cancer metastasis. Semin Cancer Biol. 2017;44:141–52.
Silsirivanit A. Glycosylation markers in cancer. Adv Clin Chem. 2019;89:189–21313.
Kim YS, Son OL, Lee JY, Kim SH, Oh S, Lee YS, et al. Lectin precipitation using phytohemagglutinin-L(4) coupled to avidin-agarose for serological biomarker discovery in colorectal cancer. Proteomics. 2008;8:3229–355.
Calderon AD, Liu Y, Li X, Wang X, Chen X, Li L, et al. Substrate specificity of FUT8 and chemoenzymatic synthesis of core-fucosylated asymmetric N-glycans. Org Biomol Chem. 2016;14:4027–31.
Takahashi M, Kuroki Y, Ohtsubo K, Taniguchi N. Core fucose and bisecting GlcNAc, the direct modifiers of the N-glycan core: their functions and target proteins. Carbohydr Res. 2009;344:1387–90.
Uozumi N, Yanagidani S, Miyoshi E, Ihara Y, Sakuma T, Gao CX, et al. Purification and cDNA cloning of porcine brain GDP-L-Fuc:N-acetyl-beta-d-glucosaminide alpha1–%3e6fucosyltransferase. J Biol Chem. 1996;271:27810–7.
Mas E, Pasqualini E, Caillol N, El Battari A, Crotte C, Lombardo D, et al. Fucosyltransferase activities in human pancreatic tissue: comparative study between cancer tissues and established tumoral cell lines. Glycobiology. 1998;8:605–13.
de Vries T, Knegtel RM, Holmes EH, Macher BA. Fucosyltransferases: structure/function studies. Glycobiology. 2001;11:119r–r12828.
Osumi D, Takahashi M, Miyoshi E, Yokoe S, Lee SH, Noda K, et al. Core fucosylation of E-cadherin enhances cell-cell adhesion in human colon carcinoma WiDr cells. Cancer Sci. 2009;100:888–95.
Yue L, Han C, Li Z, Li X, Liu D, Liu S, et al. Fucosyltransferase 8 expression in breast cancer patients: a high throughput tissue microarray analysis. Histol Histopathol. 2016;31:547–55.
Sato Y, Nakata K, Kato Y, Shima M, Ishii N, Koji T, et al. Early recognition of hepatocellular carcinoma based on altered profiles of alpha-fetoprotein. N Engl J Med. 1993;328:1802–6.
Agrawal P, Fontanals-Cirera B, Sokolova E, Jacob S, Vaiana CA, Argibay D, et al. A systems biology approach identifies FUT8 as a driver of melanoma metastasis. Cancer Cell. 2017;31(804–19):e7.
Ito Y, Miyauchi A, Yoshida H, Uruno T, Nakano K, Takamura Y, et al. Expression of alpha1,6-fucosyltransferase (FUT8) in papillary carcinoma of the thyroid: its linkage to biological aggressiveness and anaplastic transformation. Cancer Lett. 2003;200:167–72.
Cheng L, Gao S, Song X, Dong W, Zhou H, Zhao L, et al. Comprehensive N-glycan profiles of hepatocellular carcinoma reveal association of fucosylation with tumor progression and regulation of FUT8 by microRNAs. Oncotarget. 2016;7:61199–21414.
Whittle MC, Hingorani SR. Disconnect between EMT and metastasis in pancreas cancer. Oncotarget. 2015;6:30445–6.
Ben Q, An W, Fei J, Xu M, Li G, Li Z, et al. Downregulation of L1CAM inhibits proliferation, invasion and arrests cell cycle progression in pancreatic cancer cells in vitro. Exp Ther Med. 2014;7:785–90.
Acknowledgements
We thank Yuiko Aso, Mayumi Wada, and Kazuyuki Miura for their technical assistance with the experiments.
Funding
This work was supported by JSPS KAKENHI (Grant Number: JP17K10705).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author(s) declare that they have conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tada, K., Ohta, M., Hidano, S. et al. Fucosyltransferase 8 plays a crucial role in the invasion and metastasis of pancreatic ductal adenocarcinoma. Surg Today 50, 767–777 (2020). https://doi.org/10.1007/s00595-019-01953-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-019-01953-z