
Abstract
This report describes a rare case of hepatocellular carcinoma (HCC) producing granulocyte colony-stimulating factor (G-CSF). A 46-year-old male with chronic hepatitis B, who presented with fever, general malaise, loss of appetite, and weight loss, had a huge liver mass in the portal region. He had marked granulocytosis and his serum level of G-CSF was elevated. Complete tumor resection was performed, and the pathological assessment of the resected specimen revealed HCC with extensive sarcomatous changes and immunohistochemical staining for G-CSF and G-CSF receptor. Only a few cases of G-CSF-producing HCC have been reported, and this is the first case of G-CSF-producing HCC that also expressed G-CSF receptor.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Granulocyte colony-stimulating factor (G-CSF) is a naturally occurring glycoprotein that stimulates the proliferation and maturation of precursor cells in the bone marrow into fully differentiated neutrophils [1]. Marked leukocytosis without infection is sometimes found in patients with non-hematological malignancies. The cancer cells themselves may produce granulopoietic factors such as G-CSF. Asano et al. [2] first reported a case of G-CSF-producing lung cancer in 1977, and several studies have identified an aberrant expression and production of G-CSF by tumor cells in bladder cancer, osteosarcoma, thyroid cancer, gallbladder cancer, uterine cervical cancer, and especially lung cancer [3–8]. G-CSF-producing tumors grow rapidly and generally have a poor prognosis.
Hepatocellular carcinoma (HCC) is a common malignancy, and one of the major causes of death in Asian countries. HCC usually develops in patients with cirrhosis and chronic hepatitis caused by hepatitis B or C virus infection. Most cases of HCC are asymptomatic, but fatigue and abdominal right upper quadrant pain are sometimes noted. However, fever is a rare primary symptom in HCC. HCC with pyrexia has been reported in only a few studies [9, 10].
This report presents a rare case of HCC accompanied by a prolonged spiking fever, which disappeared after tumor resection. Immunohistochemical staining of HCC in this patient revealed the production of G-CSF and the expression of G-CSF receptor, and the patient experienced early recurrence of HCC and rapid regrowth.
Case report
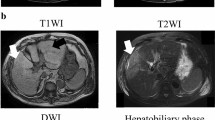
A 46-year-old male was admitted due to a prolonged high fever, general malaise, loss of appetite, and weight loss over the past 2 months. He had chronic hepatitis B when he was 40 years old, but he was not treated. He showed no signs of alcohol addiction. His mother had liver disease. His temperature was over 38.5 °C, and a physical examination revealed a hard mass palpable at the epigastric region, and a tattoo on his back. Hematological laboratory data upon admission were (Table 1): white blood cell count (WBC) 51670/μl (neutrophils 90.5 %), C-reactive protein (CRP) 27.43 mg/dl, α-fetoprotein (AFP) 386.4 ng/ml [fucosylated α-fetoprotein (AFP-L3) 84.3 %], and protein induced by the absence of vitamin K (PIVKA)-II 113 mAU/ml. Hepatitis B surface antigen (HBsAg) was positive. Computed tomography (CT) showed a peripherally enhanced, low-density mass, 10 cm in diameter, located in the hepatic portal region and derived from segment 4 (Fig. 1a). The center of the tumor was in a low-density area suggestive of necrosis or degeneration, whereas the surrounding area was enhanced in early phase, contrast-enhanced CT and washed out in the late phase. The tumor displaced the head of the pancreas left-dorsally, the descending duodenum dorsally, and the gallbladder and right liver lobe to the right side (Fig. 1b). Angiographic examination showed that the tumor had hypervascularity (Fig. 1c). Fluorodeoxyglucose positron emission tomography (FDG-PET) showed a hypermetabolic lesion [standardized uptake value (SUV)max = 25.0] in the area surrounding the tumor, and a diffusely abnormal accumulation of FDG in bone marrow throughout the body (Fig. 1d).

a, b CT findings. A tumor measuring 10 cm in diameter located in the hepatic portal region and derived from segment 4 (white arrow heads). The surrounding area of the tumor was enhanced in the early phase of contrast medium infusion (black arrow heads) and washed out in the late phase. c Abdominal angiography findings. Superior mesenteric artery (SMA) angiography showed inferior part of the tumor was hypervascular. d FDG-PET showed a hypermetabolic lesion (SUVmax = 25.0) in the area surrounding the tumor, and a diffusely abnormal accumulation of FDG in the bone marrow throughout the body (white arrow heads)
There was a possibility of co-infection or an association with the presence of hematological malignancy such as leukemia, because he had high fever, extreme leukocytosis, high serum levels of CRP, and a diffusely abnormal accumulation of FDG in bone marrow throughout the body identified by FDG-PET. Blood cultures were tested several times after admission, but were all negative for bacteria and fungi, and serum procalcitonin and endotoxin were all negative. No infective foci could be detected in any other organs by radiography or CT. Whole body bone scintigraphy showed no evidence of any abnormal accumulation that indicated bone metastasis. Bone marrow aspiration revealed hypercellularity of three series of hematopoietic cells with varying degrees of maturity. The number of neutrophils and megakaryocytes was increased. Hyperplastic changes related to the tumor were suspected. These findings indicated that he had no co-infection or hematological malignancies, and he was diagnosed with HCC and paraneoplastic syndrome.
His condition was explained to the patient and his family, and they provided informed consent for surgery. He underwent segment 4 partial hepatectomy. There was a small amount of ascites, but the cytological analysis revealed no malignant cells. The tumor was observed in segment 4 of the liver and expanded to the peritoneal cavity. There were severe adhesions around the tumor, stomach, duodenum and transverse colon, and the transverse colon was partially cut with the tumor. The tumor was resected, and his fever disappeared (<37.0 °C) by postoperative day 5 without any use of nonsteroidal anti-inflammatory drugs; WBC rapidly returned to the normal range (postoperative day 5: 7040/μl), and CRP dropped gradually from 20.38 (postoperative day 1) to 0.44 (postoperative day 14). He had an uneventful postoperative recovery without any complications and was discharged 15 days after surgery.
There was preoperative elevation of serum G-CSF, interleukin (IL)-6, IL-8 and tumor necrosis factor (TNF)-α to 195 pg/ml (normal value: <39.0 pg/ml), 168 pg/ml (normal value: <4.0 pg/ml), 245 pg/ml (normal value: <2.0 pg/ml) and 9.2 pg/ml (normal value: 0.6–2.8 pg/ml), respectively. However, IL-1α, IL-1β, interferon (IFN)-γ, and granulocyte–macrophage colony-stimulating factor (GM-CSF) were within the normal range (Table 1), the serum G-CSF, IL-6, IL-8 and TNF-α levels decreased 14 days after surgery to 20.1, 9.5, 3.4 and 4.3 pg/ml, respectively. FDG-PET after surgery showed that the diffusely abnormal accumulation of FDG in the bone marrow throughout the body, which was found before surgery, had disappeared.
The resected specimen revealed that the tumor (12.0 × 9.0 × 9.5 cm) protruded through segment 4 of the liver and expanded to the peritoneal cavity (Fig. 2). Direct invasion of the transverse colon was observed. The cut surface of the tumor was white and contained massive coagulation and necrosis. Microscopic findings revealed that the tumor was composed of sarcomatous spindle-shaped malignant cells, pleomorphic cells with bizarre nuclei and intense infiltration of neutrophils and histiocytes, and massive necrosis, focally admixed with moderately to poorly differentiated HCC with trabecular and compact patterns (Fig. 3a, b). The non-cancerous liver showed mild chronic inflammation with bridging fibrosis (A1, F3). Immunohistochemistry showed the ordinary HCC cells to be positive for hepatocyte, glypican-3 and CAM5.2 (focal), and the sarcomatous area was positive for vimentin and neural cell adhesion molecule (Fig. 3c). The sarcomatous component invaded the submucosa of the transverse colonic wall. The sarcomatous area was positive for G-CSF, and the nuclei of the tumor cells in the sarcomatous area were positive for G-CSF receptor (Fig. 3d, e). This demonstrated that the tumor produced G-CSF and expressed G-CSF receptor.

Macroscopic findings. The tumor (12.8 × 9.7 cm) protruded through segment 4 of the liver and expanded into the peritoneal cavity (black arrow heads). Direct invasion of the transverse colon was observed (red arrow head). The cut surface of the tumor was white and contained coagulation and necrosis

Histological examination. The tumor was composed of sarcomatous spindle-shaped malignant cells, pleomorphic cells with bizarre nuclei, an intense infiltration of neutrophils and histiocytes, and massive necrosis, focally admixed with moderately to poorly differentiated HCC with trabecular and compact patterns. a HCC component [hematoxylin and eosin (H&E) stain, ×100]. b Sarcomatous component (H&E, ×100). c Immunohistochemical staining of vimentin in the sarcomatous area of the tumor (×400). d Immunohistochemical staining of G-CSF in the sarcomatous area of the tumor (×400). e Immunohistochemical staining of G-CSF receptor in the sarcomatous area of the tumor (×400)
However, AFP and PIVKA-II were elevated again approximately 40 days after surgery and recurrence was detected in the locally resected portion and segment 7 of the liver. The doubling time of recurrent tumor in segment 7 of the liver was 7 days. He underwent transcatheter hepatic arterial infusion chemoembolization with miriplatin, radiotherapy and chemotherapy with gemcitabine and sorafenib, but the HCC grew very rapidly, and he died approximately 6 months after surgery.
Discussion
Okuda et al. [9] reported five HCC patients with pyrexia, with an incidence of <1 % in Japan. They also noted that very poorly differentiated sarcomatoid HCC can frequently appear with pyrexia and leukocytosis mimicking a liver abscess. Cancer cells produce humoral factors and cause paraneoplastic syndrome. The clinical symptoms and laboratory data showing fever and a high CRP level, which is not commonly observed in patients with HCC, are suspected to be due to humoral factors, especially inflammatory cytokines. G-CSF is responsible for this kind of paraneoplastic syndrome. Many cases of G-CSF-producing tumors have been reported since Asano et al. [2] reported the first case of a patient with lung cancer in 1977. However, G-CSF-producing HCC is extremely rare and only six cases have so far been documented in the English literature [11–16] (Table 2).
The immunohistochemical study in the current patient revealed G-CSF staining in the cytoplasm of the sarcomatous component of the tumor. Extreme leukocytosis and significant elevation of serum G-CSF were also noticed, and the serum WBC and G-CSF levels decreased after tumor resection. These findings confirm that the tumor was a G-CSF-producing tumor.
G-CSF-producing tumors grow rapidly and generally have a poor prognosis. G-CSF has been linked to tumor cell growth in vitro [17] and has also been shown to promote cancer progression [18], but the mechanism has yet to be elucidated. Although the mechanism by which certain liver cancers produce G-CSF remains unclear, there is an intimate relationship between the production of G-CSF in cancer cells and their dedifferentiation [11]. The cells might express bioactive G-CSF protein at more immature stages of HCC. However, Aita et al. [15] reported that G-CSF is associated with the growth and progression of epithelial elements. Further investigation is therefore necessary to clarify the relationship between G-CSF production and sarcomatous transformation of liver cancer.
The prognosis of G-CSF-producing HCC is very poor, and the majority of the patients die within a few months after the initial diagnosis. It is intriguing that four of six cases were negative for both hepatitis B and C virus antigens. This suggests that G-CSF-producing tumors have a different pathogenetic background from that of conventional HCC, which is associated with chronic hepatitis or cirrhosis. The current case was associated with chronic hepatitis B, and this is believed to be the first case of HCC associated with G-CSF production and hepatitis B virus antigen.
A simple regression analysis was performed to investigate the correlation between G-CSF levels and patient prognosis, using the 7 cases shown in Table 2. The analysis revealed no significant correlation, but a tendency between G-CSF levels and patient prognosis (R 2 = 0.54, P = 0.06). A significant correlation might be observed with a larger number of cases. G-CSF also stimulates non-hematopoietic tumor cells, which might explain the relationship between G-CSF and tumor growth. Tachibana et al. [4] reported that G-CSF-producing tumor cells express a G-CSF receptor that induces tumor cell growth by G-CSF via autocrine pathways. Therefore, G-CSF-producing tumors usually grow rapidly and the prognosis is extremely unfavorable. Joshita et al. [13] performed immunohistochemical staining for the G-CSF receptor, which yielded negative results. Their case had a more favorable prognosis (4 years) than other cases of G-CSF-producing tumors. They speculated that the absence of G-CSF receptors in the tumor caused a deficiency or the absence of autocrine growth, which led to a more favorable prognosis. Tumor cell nuclei in the sarcomatous area were positive for G-CSF receptor in the current case. G-CSF receptor is usually expressed in the cytoplasm [19], but some reports have shown that G-CSF receptor is expressed in the nuclei, especially in fetal tissues [20, 21]. Although the precise physiological significance of G-CSF receptor in non-hematopoietic tissues remains unclear, it is speculated that G-CSF receptor is associated with the proliferation and differentiation of immature tissues [20, 21]. This is the first case of G-CSF-producing HCC that also expressed G-CSF receptor.
This report presented the case of a patient with pyrexia, leukocytosis and high CRP, who had moderately to poorly differentiated HCC with extensive sarcomatous changes. The patient underwent surgical resection, but rapid tumor recurrence occurred. G-CSF production and the expression of G-CSF receptor were immunohistochemically revealed in this case and may have contributed to the high fever, high inflammatory reaction, and poor prognosis by G-CSF via autocrine pathways. Clinicians should thus consider G-CSF-producing HCC when encountering patients with a hepatic tumor with leukocytosis, and prompt therapy including radical surgery should be performed. Further investigation is necessary to further characterize G-CSF-producing HCC, and other effective treatments, such as immunotherapy, should be investigated.
References
Lieschke GJ, Burgess AW. Granulocyte colony-stimulating factor and granulocyte–macrophage colony-stimulating factor. N Engl J Med. 1992;327:28–35.
Asano S, Urabe A, Okabe T, Sato N, Kondo Y. Demonstration of granulopoietic factor(s) in the plasma of nude mice transplanted with a human lung cancer and in the tumor tissue. Blood. 1977;49:845–52.
Ito N, Matsuda T, Kakehi Y, Takeuchi E, Takahashi T, Yoshida O. Bladder cancer producing granulocyte colony-stimulating factor. N Engl J Med. 1990;323:1709–10.
Tachibana M, Miyakawa A, Tazaki H, Nakamura K, Kubo A, Hata J, et al. Autocrine growth of transitional cell carcinoma of the bladder induced by granulocyte-colony stimulating factor. Cancer Res. 1995;55:3438–43.
Thacker JD, Dedhar S, Hogge DE. The effect of GM-CSF and G-CSF on the growth of human osteosarcoma cells in vitro and in vivo. Int J Cancer. 1994;56:236–43.
Iwasa K, Noguchi M, Mori K, Ohta N, Miyazaki I, Nonomura A, et al. Anaplastic thyroid carcinoma producing granulocyte colony-stimulating factor (G-CSF): report of a case. Surg Today. 1995;25:158–60.
Furihata M, Sonobe H, Ohtsuki Y, Enzan H, Tokuoka H, Nakamura Y. An immunohistochemical study on a case of granulocyte-colony stimulating factor-producing gall-bladder carcinoma. Pathol Int. 1999;49:1010–3.
Kyo S, Kanaya T, Takakura M, Inoue M. A case of cervical cancer with aggressive tumor growth: possible autocrine growth stimulation by G-CSF and IL-6. Gynecol Oncol. 2000;78:383–7.
Okuda K, Kondo Y, Nakano M, Kage M, Arakawa M, Kojiro M, et al. Hepatocellular carcinoma presenting with pyrexia and leukocytosis: report of five cases. Hepatology. 1991;13:695–700.
Harimoto N, Shirabe K, Abe T, Kajiyama K, Nagaie T, Gion T, et al. Interleukin-8 producing hepatocellular carcinoma with pyrexia. HPB Surg. 2009;2009:461492.
Yamamoto S, Takashima S, Ogawa H, Kuroda T, Yamamoto M, Takeda A, et al. Granulocyte-colony-stimulating-factor-producing hepatocellular carcinoma. J Gastroenterol. 1999;34:640–4.
Araki K, Kishihara F, Takahashi K, Matsumata T, Shimura T, Suehiro T, et al. Hepatocellular carcinoma producing a granulocyte colony-stimulating factor: report of a resected case with a literature review. Liver Int. 2007;27:716–21.
Joshita S, Nakazawa K, Koike S, Kamijo A, Matsubayashi K, Miyabayashi H, et al. A case of granulocyte-colony stimulating factor-producing hepatocellular carcinoma confirmed by immunohistochemistry. J Korean Med Sci. 2010;25:476–80.
Amano H, Itamoto T, Emoto K, Hino H, Asahara T, Shimamoto F. Granulocyte colony-stimulating factor-producing combined hepatocellular/cholangiocellular carcinoma with sarcomatous change. J Gastroenterol. 2005;40:1158–9.
Aita K, Seki K. Carcinosarcoma of the liver producing granulocyte colony-stimulating factor. Pathol Int. 2006;56:413–9.
Hori S, Takebayashi J, Okamoto T, Setsu K, Senoh T. An autopsy case of hepatocellular carcinoma producing granulocyte colony-stimulating factor. Acta Hepatol Jpn. 1998;39:401–5.
Berdel WE, Danhauser-Riedl S, Steinhauser G, Winton EF. Various human hematopoietic growth factors (interleukin-3, GM-CSF, G-CSF) stimulate clonal growth of nonhematopoietic tumor cells. Blood. 1989;73(1):80–3.
Noda I, Fujieda S, Ohtsubo T, Tsuzuki H, Tanaka N, Sunaga H, Saito H. Granulocyte- colony-stimulating factor enhances invasive potential of human head-and-neck-carcinoma cell lines. Int J Cancer. 1999;80(1):78–84.
Tsuzuki H, Fujieda S, Sunaga H, Noda I, Saito H. Expression of granulocyte colony-stimulating factor receptor correlates with prognosis in oral and mesopharyngeal carcinoma. Cancer Res. 1998;58:794–800.
Calhoun DA, Donnelly WH Jr, Du Y, Dame JB, Li Y, Christensen RD. Distribution of granulocyte colony-stimulating factor (G-CSF) and G-CSF-receptor mRNA and protein in the human fetus. Pediatr Res. 1999;46:333–8.
Calhoun DA, Lunoe M, Du Y, Christensen RD. Granulocyte colony-stimulating factor is present in human milk and its receptor is present in human fetal intestine. Pediatrics. 2000;105(1):e7.
Acknowledgments
We thank Edanz Editing for critical comments on the manuscript.
Conflict of interest
Mikihiro Kohno and other co-authors have no conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kohno, M., Shirabe, K., Mano, Y. et al. Granulocyte colony-stimulating-factor-producing hepatocellular carcinoma with extensive sarcomatous changes: report of a case. Surg Today 43, 439–445 (2013). https://doi.org/10.1007/s00595-012-0202-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-012-0202-0