
Abstract
The authors report a case of pseudoaneurysm of the profunda femoris artery following fixation of an intertrochanteric hip fracture with a dynamic hip screw. Diagnosis and treatment of this rare complication are described.
Résumé
Les auteurs rapportent un cas de pseudoanévrisme de l’artère fémorale profonde après ostéosynthèse par vis plaque à compression d’une fracture trochantérienne. Le diagnostic et le traitement de cette complication rare sont abordés.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Injury to the femoral vessels is a rare complication after fractures of the hip. We report a case of pseudoaneurysm of the profunda femoris artery that presented 12 weeks following fixation of an intertrochanteric hip fracture with a dynamic hip screw (DHS). The diagnosis was confirmed by iliofemoral arteriography, and it was treated by transcatheter embolisation using thrombin and coil deployment.
Case report
A 78-year-old man sustained a displaced, unstable, closed four-part intertrochanteric fracture of the left hip (Fig. 1) along with ipsilateral Colles fracture following a fall. He had a history of atrial fibrillation and hypertension, which were well controlled. His Colles fracture was reduced in A&E under intravenous midazolam, and a below-elbow cast was given. The patient was operated on the following day for his hip fracture, and after closed reduction on the fracture table; the fracture was fixed internally with an AO DHS (Fig. 2). The operation was unremarkable, and no excessive bleeding from the wound was noted. Check radiograph was satisfactory, and the patient was discharged 10 days post-operatively to his residence. The plaster for his Colles fracture was removed after 6 weeks.

Radiograph showing intertrochanteric fracture of the left hip

Post-operative radiograph showing dynamic hip screw (DHS) in situ
Twelve weeks post-operatively, he presented with a 10×20 cm painless firm swelling in the left groin distal to inguinal ligament. The swelling itself was not pulsatile, but it had a palpable pulse over it. The distal pulses were normal. Haemoglobin on admission was 10.4. Radiological examination revealed collapse at the fracture site with implants in satisfactory position, but the lesser trochanteric fragment remained widely separated from the medial side of the femoral neck (Fig. 3). Duplex ultrasound of the femoral vessels demonstrated 7 cm swelling posterior to the common femoral and profunda femoris artery. With the assistance of general surgeons, the common femoral, superficial femoral and profunda femoris artery was explored. All the vessels were found to be patent. On the table, the mass was not pulsatile, and a sharp fragment of bone was noted, which was subsequently removed.

Twelve weeks post-fixation. Note that the lesser trochanter (arrow) has migrated proximally due to the pull of attached iliopsoas muscle
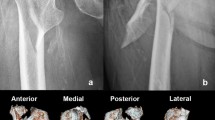
Five days after the operation, his groin swelling increased in size. Contrast enhanced CT scan revealed pseudoaneurysm in continuity with profunda femoris artery and its branches, i.e. medial and lateral circumflex femoral artery. Under local anaesthesia, left Iliofemoral arteriography was done, which revealed false aneurysm of the profunda femoris artery (Fig. 4a). Transcatheter embolisation of the false aneurysm was done using thrombin injection, and a single 7 mm×5 cm embolisation coil was deployed into the neck of the false aneurysm with little protrusion in the profunda femoris neck (Fig. 4b). Post-embolisation duplex ultrasound showed aneurysmal sac confirmed to be thrombosed with patent profunda femoris and superficial femoral artery, but there was thrombus in the mid-femoral vein and popliteal vein with some re-canalisation. In view of this deep vein thrombosis, an IVC filter was deployed on the third post-operative day, and the patient was commenced on warfarin 2 weeks post-embolisation. At the 4-month surgical and orthopaedic review, the patient was well with no thigh tenderness and good hip mobility.

Arteriogram of the profunda femoris artery showing a pseudoaneurysm (a) before and (b) after embolization
Discussion
The profunda femoris artery is the largest branch of the femoral artery. It supplies the muscles of the posterior and lateral thigh in conjunction with the gluteal, circumflex iliac, superficial femoral and popliteal vessels. The proximal segment is superficial, lies lateral to the femoral artery, and gives off two major branches—the medial and lateral circumflex arteries. The distal segment passes deep to the superficial femoral vessel and lies beneath the adductor longus muscle giving off four branches—the perforators that pass through the fascia of the adductor magnus and adductor brevis in the posterior thigh.
Arterial injury associated with hip fracture is usually due to iatrogenic trauma [6, 3] or rarely by bone spike [7]. Injury by bone spike may occur at the time of initial trauma, during reduction or post-operatively during mobilisation subsequent to the lesser trochanter fragment, which migrates with the movement of the hip due to the function of the attached iliopsoas muscle [2]. The diagnosis of false aneurysm is usually delayed, because pain, haematoma and unexplained anaemia are non-specific clinical signs. The diagnosis should be kept in mind if the thigh is noted to be swollen and painful after surgery or the patient is requiring repeated blood transfusions. Diagnosis can be confirmed by non-invasive (Duplex ultrasound) or invasively (conventional arteriography). Arteriography is usually done to define the point of origin of the pseudoaneurysm.
Management of the injury depends upon the site of the injury, the presence of pre-existing arterial disease in the limb and the patient’s general condition. Apart from transcatheter embolisation using thrombin [8], ligation of the PFA artery at the level of pseudoaneurysm [7], direct per cutaneous injection of thrombin [4, 5], Transcatheter fibrin adhesive and coils [1] have also been described.
This case highlights the rare complication of delayed pseudoaneurysm formation of the profunda femoris artery after femoral neck fracture operative fixation and its successful treatment by transcatheter embolisation.
References
Entwisle JJ, Mario de Nunzio, D.Hinwood (2001) Transcatheter embolization of Pseudoaneurysm of the profunda femoris artery complicating fracture of the Femoral neck. Clin Radiol 56:424–427
Keel JD, Eyres KS (1993) Vascular injury by an intertrochanteric fracture fragment. Injury 24:350–352
Kyu Hun, Yang Hui Van Park, Seong Jin Park (2002) Pseudoaneurysm of the superficial femoral artery after closed hip nailing with a Gamma nail. J Orthop Trauma 16:124–127
Kang SS (1999). Percutaneous thrombin injection of pseudoaneurysms. J Vasc Intervent Radiol 10[Suppl]:192–194
Liau CS, Ho FM, Chen MF (1997) Treatment of iatrogenic femoral artery pseudoaneurysms with percutaneous thrombin injection. Vasc Surg 26:18–23
Lazarides MK, Arvanitis DP, Dayantas JN (1991) Iatrogenic arterial trauma associated hip joint surgery: an overview. Eur J Vasc Surg 5:549–556
Murphy PG, Geoghegan JG, Austin O, More-O Ferrall R, Quinlan WR (1999) Pseudoaneurysm of the profunda femoris artery due to intertrochanteric fracture of the hip. Arch Orthop Trauma Surg 119:117–118
Walker TG, Geller SC, Brewster DC,(1987) Transcatheter occlusion of a profunda femoral artery pseudoaneurysm using thrombin. AJR 149:183–186
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Maheshwari, R., Pemmaraju, K., Sloan, R. et al. Pseudoaneurysm of profunda femoris artery following intertrochanteric fracture of the hip. Eur J Orthop Surg Traumatol 14, 192–194 (2004). https://doi.org/10.1007/s00590-004-0163-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-004-0163-0