
Abstract
An experimental in vitro biomechanical study was conducted on human cadaveric spines to evaluate the motion segment (C4–C5) and global subaxial cervical spine motion after placement of a cervical arthroplasty device (Altia TDI™,Amedica, Salt Lake City, UT) as compared to both the intact spine and a single-level fusion. Six specimens (C2–C7) were tested in flexion/extension, lateral bending, and axial rotation under a ± 1.5 Nm moment with a 100 N axial follower load. Following the intact spine was tested; the cervical arthroplasty device was implanted at C4–C5 and tested. Then, a fusion using lateral mass fixation and an anterior plate was simulated and tested. Stiffness and range of motion (ROM) data were calculated. The ROM of the C4–C5 motion segment with the arthroplasty device was similar to that of the intact spine in flexion/extension and slightly less in lateral bending and rotation, while the fusion construct allowed significantly less motion in all directions. The fusion construct caused broader effects of increasing motion in the remaining segments of the subaxial cervical spine, whereas the TDI did not alter the adjacent and remote motion segments. The fusion construct was also far stiffer in all motion planes than the intact motion segment and the TDI, while the artificial disc treated level was slightly stiffer than the intact segment. The Altia TDI allows for a magnitude of motion similar to that of the intact spine at the treated and adjacent levels in the in vitro setting.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cervical spondylosis causing radiculopathy or myelopathy is one of the most common problems seen by the spine surgeon and is often treated with anterior cervical diskectomy and fusion (ACDF). This procedure, although it is highly effective at decompressing neural elements and stabilizing the spine, is associated with significant short- and long-term morbidity, including postoperative dysphagia, promoted adjacent-level degeneration, and a high incidence of nonunion when multiple levels are treated [15, 18, 19, 28, 30].
Although ACDF has been the mainstay treatment for cervical disk disease since the 1950s [7, 29], interest in motion preservation in spinal surgery is almost as old. The first attempt at cervical arthroplasty reported by Fernstrom [14] in 1966 involved the placement of metallic ball bearings into the disk space of the treated segments. Clinical results were, however, disappointing because of a high incidence of segmental hypermobility, endplate subsidence, and clinical failure. Interest in cervical arthroplasty waned until the 1990s when a renewal of efforts was spurred by progress in lumbar arthroplasty with the Charite disk [5] and with increased recognition of long-term complications of cervical fusion surgery, specifically with regard to adjacent segment degeneration. Adjacent segment degeneration, reported to become clinically symptomatic in up to 25% of patients by 10 years of follow-up [6, 17–20], is believed to be promoted by increased stress and motion at these levels. These factors have been demonstrated to occur biomechanically and clinically [2, 3, 12, 13, 33, 35] and likely promote the degeneration by disrupting delicate nutrient pathways to the avascular nucleus pulposus [31, 32]. The goal of cervical arthroplasty is to restore normal biomechanics of the treated segment, thereby normalizing motion and stress in adjacent levels and reducing the incidence of long-term failure in the form of adjacent segment degeneration. Cervical arthroplasty might also have the added benefits of reducing incidence of postoperative dysphagia and complications associated with the treatment of multilevel disease [15, 21, 26, 28, 30].
The first modern cervical disk replacement to be tested clinically was the Cummins–Bristol artificial joint [9]. Although there were significant complications, including screw breakage and pullout, in this initial experience, 16 of 18 patients had continued motion at the treated joint and no patient had adjacent-level degeneration in up to 65 months of follow-up providing some initial optimism for the concept. The complications led to changes in the design that have demonstrated more favorable clinical results [33]. Similar clinical results have been reported in trials using several other designs, including the Bryan cervical disc [8, 16], porous coated motion (PCM) prosthesis [26], Frenchay artificial cervical joint [33, 34], Prestige II implant [27], and the ProDisc-C [4].
The Altia TDI™ (total disc implant) is a uniquely designed bi-saddle-shaped cervical arthroplasty device with distinctive biomechanical characteristics (Fig. 1). The goal of this design is to allow for slight translational motion during the flexion and extension and soft stops, using the ligamentous restraints of the motion segment. The device is composed of a silicon-nitride ceramic with superior wear characteristics than existing metal and polymer designs, while allowing for imaging the clarity of nearby structures with magnetic resonance imaging or computed tomography. Finally, the implant is engineered to have a low profile without protrusion from the disk space and is secured via one midline keel in the superior level and two laterally placed keels in the inferior level to avoid conflict when multiple levels are instrumented.

The Altia TDI has a unique bi-saddle-shaped design that forms the articulation between the two components. They are inserted simultaneously in the disc space C
Despite the promising early clinical results and obvious theoretical benefits, there is a paucity of in vitro biomechanical data characterizing cervical arthroplasty devices in the literature [11, 12, 22]. In this study, we detail the kinematics of the entire subaxial cervical spine from C2 to C7 with the middle segment intact, treated by fusion, or replaced with an artificial disc implant. Special attention is paid to adjacent segment motion with the implanted disk in comparison with a simulated fusion, the current standard of care.
Materials and methods
Six human cervical spine specimens (C2–C7) were used in the study. Each specimen was <65 years (mean age 53.3 ± 8.4 years) and was screened visually and with anterior–posterior and lateral radiographs to exclude signs of neoplasm, trauma, severe degeneration, or other factors that could effect their mechanical properties. In addition, each specimen was scanned using dual X-ray absorptiometry (DEXA) (General Electric Medical Systems, Madison, Wisconsin), and those with bone densities of >1.0 standard deviation below the pool of specimens were eliminated.
The specimens were kept frozen at −20°C in sealed plastic bags and were thawed at room temperature for 12 h before testing. On the day of testing, the specimens were prepared by removing all remaining skin and most of the paraspinal cervical musculature; care was taken to keep all ligaments, joint capsules, osseous components, and intervertebral discs intact. To supplement the potting fixation, three drywall screws were inserted radially into the vertebral bodies and lateral masses of C2 and C7. These end vertebrae were then placed into 4-cm deep polyvinyl chloride potting fixtures and were embedded to the middle of the vertebra in a two-part filler compound (Bondo body filler; Bondo, Atlanta, GA, USA).
Prior to testing, lateral mass screws were placed in each specimen at C4 and C5 bilaterally in preparation for the fusion part of the procedure. The screws were placed under fluoroscopic guidance in the standard manner [36] and did not interfere with normal range of motion (ROM).
Specimens were first tested in load control in our custom multiaxis spine simulator with infrared-emitting diodes screwed into the vertebral bodies of C3, C4, C5, and C6 to monitor angular motion between these vertebrae. Infrared-emitting diodes were additionally secured to the pots to record motion of levels C2 and C7. The spine simulator is composed of six feedback-controlled pneumatic actuators mounted on to two opposing 3-degree of freedom gimbals that control flexion/extension, lateral bending, and axial rotation moments at the upper and lower ends of the specimen. In addition, the upper gimbal is mounted on to a linear actuator to allow for change in height of the specimen as it moves under bending moments applied through either load or position control. A follower load apparatus is attached to the lower gimbal and applies a preload in line with the specimen through its full ROM. The custom spine simulator is controlled by two National Instruments 7344 series motion controllers and a PC computer running a custom-written National Instruments Labview VI program. There are two 6-Axis AMTI load cells, each positioned between the specimen and gimbal on either end, which provide feedback for the pneumatic actuators on that gimbal, and one position encoder per axis of motion for feedback when in position control. Data are collected via a National Instruments AT-MIO-64E-3 data acquisition board. All specimens were initially tested in the intact condition in load control with applied moments of 1.5 Nm in each respective plane of motion and 100 N of axial follower load applied. A 1.5 Nm moment was chosen because it falls within the range of moments used in other biomechanical tests (1.0–4.0 Nm) of the cervical spine and allows for safe, non-destructive testing of the destabilized specimen. Furthermore, this parameter allows for safe testing of the spine in position control after instrumentation has been added, a situation in which forces typically increase to approximately 3.0 Nm. Follower loads were applied through guides attached at each level through which a flexible cable was passed [25]. Guides are placed in the lateral masses at each segment through the center of rotation. Before any data were recorded, each spine was preconditioned with 30 cycles in each plane of motion to reduce the effects of the specimen freeze/thaw cycle. A second trial of five cycles in each axis was then used for data recording to determine the ROM of segments C2–C7 (ROMC2–C7). The spine simulator was then placed in position control with the ROMC2–C7 parameters being used for the treated spines under two conditions. A hybrid testing protocol, in which the initial ROM is determined under load control and treated conditions are tested under position control, is based on the assumption that an individual will attempt to regain preoperative function (i.e., ROM) after a procedure. First, a C4–C5 diskectomy was performed to implant the cervical arthroplasty device as described below. Second, a fusion was simulated by securing rods to the previously placed lateral mass screws and placing a custom anterior plate. The spines were subjected to five cycles of ROMC2–C7 in each axis of motion with 100 N of follower load (intact, fusion, implant). Data were collected on the fourth and fifth cycles of each axis (Fig. 2).

The cadaveric spine with the Altia TDI implant at the C4/5 level in the multiaxis spine simulator
To place the Altia TDI, a standard diskectomy at C4–C5 was undertaken. Distraction posts were used at the adjacent segments to provide better visualization for the diskectomy and to allow easier insertion of the device. The entire disk was evacuated in each case and the posterior longitudinal ligament was cut. A custom tool was then used to prepare the endplates, remove cartilage, and create parallel surfaces. A sizing probe in the shape of the implant was then inserted to measure the disk space. The implant consists of separate superior and inferior components that combine to form a disk replacement of varying height, width, and depth. Once size was determined, an appropriately sized cutting device was used to create grooves for the keels in the respective vertebral bodies. This device was tamped into the bone with a mallet; the device includes a stop feature to prevent over insertion. Using care to align the keels of the devices with the slots just created, the implant itself was then inserted into the disk space until flush with the anterior surface of the vertebral body.
Torque data from the multiaxis spine simulator and rotation data from the OptoTrak were recorded, processed, and analyzed on a personal computer with a National Instruments AT-MIO-64E-3 board (National Instruments, Austin, TX, USA) and LabView Software (National Instruments) that generated torque–rotation plots. ROM and stiffness were determined from the LabView graphs. Stiffness was determined by measuring the linear slope of the elastic zone from the torque rotation plots. All data were analyzed using a Wilcoxan-signed rank test with P values <0.05 considered statistically significant.
Results
Average motion was calculated for each segment under each condition (Table 1). Flexion/extension, lateral bending, and axial torsion motions are reported for not only the treated segment, but also for the adjacent and supra-adjacent segments.
Flexion/extension motion at C4–C5 with the Altia TDI was 5.9° ± 3.1°, 82% of the intact spine (7.1° ± 2.4°; P = 0.156). Motion of the C4–C5 fusion construct was less than that with either the Altia or the intact spine at 1.5° ± 1.2° (P = 0.031 and P = 0.031, respectively) (Fig. 3a).

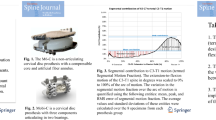
Graphs illustrating relative percentage motion under the tested conditions in flexion–extension (a), lateral bending (b), and axial rotation (c)
The intact spine allowed 5.1° ± 2.7° of motion in lateral bending. The arthroplasty device allowed 60% of this motion (3.0° ± 2.2°; P = 0.063), while the fusion construct allowed only 1.1° ± 0.9°; P = 0.031). Although the arthroplasty device allowed less motion than the intact spine; there was a trend towards more motion than the fusion construct (P = 0.063) (Fig. 3b).
Axial rotation was 9.2° ± 1.3° in the intact spine and 6.8° ± 2.7° with the arthroplasty device (74% of intact, P = 0.125). The fusion construct trended towards more limited rotation at C4–C5 to 1.8° ± 1.1°, less than the TDI or the intact spine (P = 0.063 and 0.063, respectively) (Fig. 3c).
Range of motion of the adjacent segments (C3–C4; C5–C6) and supra-adjacent segment (C2–3; C6–C7) with the arthroplasty device at C4–C5 was similar to those of the intact spine in all moments, with the exception of lateral bending at C3–C4, which was increased 13%. With fusion at C4–C5, the adjacent and supra-adjacent motion segments had significantly increased strain in all moments, with the exception of rotation and flexion/extension at C5/6 and lateral bending at C2/3 and C6/7, where differences in motion were noted, but did not reach significance.
Stiffness of each segment was calculated in Nm/deg and reported as normalized to intact (Fig. 4). Stiffness in flexion/extension at the treated level was 201% of intact with the Altia TDI and 774% of intact with the fusion construct. There was no significant difference between intact and the arthroplasty device, but a significant difference was realized between the fusion construct and the arthroplasty device and intact spine (P = 0.031 and P = 0.031).

Graph showing stiffness of intact spine, Altia TDI, and fusion construct. Data are presented normalized to intact specimen condition
Stiffness in lateral bending at the treated level was 236% of intact with the Altia TDI and 990% of intact with the fusion construct. There was no significant difference between the intact spine and the arthroplasty device, but a significant difference was realized between the fusion construct and the arthroplasty device and intact spine (P = 0.031 and P = 0.031).
Stiffness in axial rotation at the treated level was 175% of intact with the Altia TDI and 969% of intact with the fusion construct. There was no significant difference between intact and the cervical arthroplasty device, but a strong trend was detected between the fusion construct and the arthroplasty device and intact spine (P = 0.063 and P = 0.063).
Discussion
Anterior cervical diskectomy and fusion has been the mainstay of treatment for cervical myelopathy and radiculopathy since the 1950s. Although interest in motion preservation technologies is not new, increased recognition of the development of adjacent-level degeneration has led to a redoubling of efforts in the development of cervical arthroplasty. Despite the promising accumulating clinical experience with disk replacements of varying designs, little work has been done to characterize the in vitro biomechanical features of varying replacements. DiAngelo et al. [11] provided a biomechanical analysis of the ProDisc-C and demonstrated maintenance of normal motion at the treated and adjacent levels in all conditions except extension when compared with intact spines. Dmitriev et al. [12] showed that the PCM implant maintained normal ROM at the treated and adjacent segments as well as maintaining normal intradiscal pressure at adjacent segments, parameters that are both increased in a fusion construct. McAfee et al. [22] demonstrated similar results for ROM with the PCM disk, although they found an increased ROM in axial rotation at the treated segment in this study.
We examined ROM and stiffness of the cadaveric cervical spine under three conditions: intact, with Altia TDI at the C4–C5 level, and simulated fusion. Motion at the C4–C5 level in spines treated with the cervical arthroplasty device was comparable with motion in intact spines in flexion and extension, but was slightly decreased in both lateral bending and axial rotation. Stiffness of the treated segment was comparable with intact and significantly less than the fusion construct in all moments applied.
Examination of adjacent and supra-adjacent segments after treatment with the Altia TDI revealed motion similar to that of the intact specimen for all moments except lateral bending at C3–C4, which was slightly increased. The fusion construct was associated with significantly increased ROM at all adjacent segments, with the exception of axial rotation and flexion/extension at C5–C6, which were not significantly increased, and all supra-adjacent segments. Although changes in motion at supra-adjacent segments have not been examined in earlier studies and the significance of such findings remain to be unknown, we believe that our findings demonstrate the significant alteration of dynamics in a spine undergoing fusion at even one level. Conversely, the normalization of this motion with the cervical arthroplasty device demonstrates that the restoration of normal biomechanics at the treated level results in a global restoration of normal movement in the cervical spine.
The Altia TDI was designed to allow for near full ROM in flexion/extension and more limited ROM in lateral bending and rotation and these characteristics have been demonstrated in this study. Constraints to lateral bending and axial rotation are provided by the saddle-shaped articulations. Unconstrained prostheses in the lumbar spine have been shown to be associated with rotational instability [1, 10, 23, 24]. This problem has been analyzed biomechanically. McAfee et al. [23] demonstrated that the rotational instability endowed by such designs is additive over multiple-treated segments. Rotational stability of the cervical spine, however, is endowed primarily by the posterior elements, where strong capsular ligament and ligamentum flavum strength in combination with the large facet joint surface area and biomechanically advantageous angle of influence of the facet joint work to resist rotatory moments [23]. The contribution of the annulus and anterior longitudinal ligaments in the cervical spine are relatively less important, and rotational stability has been shown to be restored with unconstrained arthroplasty devices here after these structures are destroyed [23]. However, because rotational stability is largely dependent on the posterior elements, multilevel replacement with a device that allows greater than normal axial rotation may place undue stress on these structures and lead to premature facet and uncovertebral joint arthrosis. In addition, adjacent-level disk pressure under conditions of fusion and axial rotation were only marginally elevated compared with intact specimens [12]. Intradiscal pressures, on the other hand, are most dramatically raised in adjacent segments when undergoing flexion/extension. These factors lead to the conclusion that an ideal disk might possess semi-constrained characteristics in rotation, where the potential benefit of preventing increased facet stress appears to come at relatively little cost to adjacent segment stress and more freedom in flexion/extension, where maximal increases in intradiscal pressures are noted.
Conclusions
Biomechanical testing of the Altia TDI cervical arthroplasty implant revealed similar kinematic properties to those observed in the intact spine in flexion and extension, with slightly increased stiffness in lateral bending and rotation at the treated level. Mild constraint of motion in rotation and lateral bending may translate into increased rotational stability in multisegment cases and reduced stress on the facet joints, although the clinical implications of these properties have yet to be determined. Adjacent levels and supra-adjacent levels were largely found to maintain normal kinematics as well.
References
Aunoble S, Donkersloot P, Le Huec JC (2004) Dislocations with intervertebral disc prosthesis: two case reports. Eur Spine J 13:464–467. doi:10.1007/s00586-004-0687-3
Azmi H, Schlenk RP (2003) Surgery for postarthrodesis adjacent-cervical segment degeneration. Neurosurg Focus 15(3):E6. doi:10.3171/foc.2003.15.3.6
Baba H, Furusawa N, Imura S, Kawahara N, Tsuchiya H, Tomita K (1993) Late radiographic findings after anterior cervical fusion for spondylotic myeloradiculopathy. Spine 18:2167–2173
Bertagnoli R, Yue JJ, Pfeiffer F, Fenk-Mayer A, Lawrence JP, Kershaw T, Nanieva R (2005) Early results after ProDisc-C cervical disc replacement. J Neurosurg Spine 2:403–410
Buttner-Janz K, Schellnack K, Zippel H (1989) Biomechanics of the SB Charite lumbar intervertebral disc endoprosthesis. Int Orthop 13:173–176. doi:10.1007/BF00268042
Cherubino P, Benazzo F, Borromeo U, Perle S (1990) Degenerative arthritis of the adjacent spinal joints following anterior cervical spinal fusion: clinicoradiologic and statistical correlations. Ital J Orthop Traumatol 16:533–543
Cloward RB (1958) The anterior approach for removal of ruptured cervical disks. J Neurosurg 15:602–617
Coric D, Finger F, Boltes P (2006) Prospective randomized controlled study of the Bryan cervical disc: early clinical results from a single investigational site. J Neurosurg Spine 4:31–35. doi:10.3171/spi.2006.4.1.31
Cummins BH, Robertson JT, Gill SS (1998) Surgical experience with an implanted artificial cervical joint. J Neurosurg 88:943–948
David T (2005) Revision of a Charite artificial disc 9.5 years in vivo to a new Charite artificial disc: case report and explant analysis. Eur Spine J 14:507–511. doi:10.1007/s00586-004-0842-x
DiAngelo DJ, Foley KT, Morrow BR, Schwab JS, Song J, German JW, Blair E (2004) In vitro biomechanics of cervical disc arthroplasty with the ProDisc-C total disc implant. Neurosurg Focus 17(3):E7
Dmitriev AE, Cunningham BW, Hu N, Sell G, Vigna F, McAfee PC (2005) Adjacent level intradiscal pressure and segmental kinematics following a cervical total disc arthroplasty: an in vitro human cadaveric model. Spine 30:1165–1172. doi:10.1097/01.brs.0000162441.23824.95
Eck JC, Humphreys SC, Lim TH, Jeong ST, Kim JG, Hodges SD, An HS (2002) Biomechanical study on the effect of cervical spine fusion on adjacent-level intradiscal pressure and segmental motion. Spine 27:2431–2434. doi:10.1097/00007632-200211150-00003
Fernstrom U (1966) Arthroplasty with intercorporal endoprothesis in herniated disc and in painful disc. Acta Chir Scand Suppl 357:154–159
Geisler FH, Caspar W, Pitzen T, Johnson TA (1998) Reoperation in patients after anterior cervical plate stabilization in degenerative disease. Spine 23:911–920. doi:10.1097/00007632-199804150-00013
Goffin J, Van Calenbergh F, van Loon J, Casey A, Kehr P, Liebig K, Lind B, Logroscino C, Sgrambiglia R, Pointillart V (2003) Intermediate follow-up after treatment of degenerative disc disease with the Bryan cervical disc prosthesis: single-level and bi-level. Spine 28:2673–2678. doi:10.1097/01.BRS.0000099392.90849.AA
Gore DR, Sepic SB (1998) Anterior discectomy and fusion for painful cervical disc disease: a report of 50 patients with an average follow-up of 21 years. Spine 23:2047–2051. doi:10.1097/00007632-199810010-00002
Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH (1999) Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am 81:519–528
Hilibrand AS, Robbins M (2004) Adjacent segment degeneration and adjacent segment disease: the consequences of spinal fusion? Spine J 4:190S–194S. doi:10.1016/j.spinee.2004.07.007
Katsuura A, Hukuda S, Saruhashi Y, Mori K (2001) Kyphotic malalignment after anterior cervical fusion is one of the factors promoting the degenerative process in adjacent intervertebral levels. Eur Spine J 10:320–324. doi:10.1007/s005860000243
McAfee PC (2006) The advantages of cervical disc replacement for the treatment of degenerative disc disease. Curr Opin Orthop 17:233–239. doi:10.1097/01.bco.0000223531.42148.c6
McAfee PC, Cunningham B, Dmitriev A, Hu N, Woo Kim S, Cappuccino A, Pimenta L (2003) Cervical disc replacement-porous coated motion prosthesis: a comparative biomechanical analysis showing the key role of the posterior longitudinal ligament. Spine 28:S176–S185. doi:10.1097/01.BRS.0000092219.28382.0C
McAfee PC, Cunningham BW, Hayes V, Sidiqi F, Dabbah M, Sefter JC, Hu N, Beatson H (2006) Biomechanical analysis of rotational motions after disc arthroplasty: implications for patients with adult deformities. Spine 31:S152–S160. doi:10.1097/01.brs.0000234782.89031.03
McAfee PC, Cunningham BW, Lee GA, Orbegoso CM, Haggerty CJ, Fedder IL, Griffith SL (1999) Revision strategies for salvaging or improving failed cylindrical cages. Spine 24:2147–2153. doi:10.1097/00007632-199910150-00015
Miura T, Panjabi MM, Cripton PA (2002) A method to simulate in vivo cervical spine kinematics using in vitro compressive preload. Spine 27:43–48. doi:10.1097/00007632-200201010-00011
Pimenta L, McAfee PC, Cappuccino A, Bellera FP, Link HD (2004) Clinical experience with the new artificial cervical PCM (Cervitech) disc. Spine J 4:315S–321S. doi:10.1016/j.spinee.2004.07.024
Porchet F, Metcalf NH (2004) Clinical outcomes with the Prestige II cervical disc: preliminary results from a prospective randomized clinical trial. Neurosurg Focus 17(3):E6. doi:10.3171/foc.2004.17.3.6
Rhyne AL, Siddiqui F, Darden BV (2005) Incidence of post-operative dysphagia following total cervical disc replacement versus anterior cervical discectomy and fusion with instrumentation (abstract). In: 33rd Annual Cervical Spine Research Society, San Diego
Smith GW, Robinson RA (1958) The treatment of certain cervical–spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am 40-A:607–624
Swank ML, Lowery GL, Bhat AL, McDonough RF (1997) Anterior cervical allograft arthrodesis and instrumentation: multilevel interbody grafting or strut graft reconstruction. Eur Spine J 6:138–143. doi:10.1007/BF01358747
Urban JP, Holm S, Maroudas A, Nachemson A (1982) Nutrition of the intervertebral disc: effect of fluid flow on solute transport. Clin Orthop Relat Res (170):296–302
Urban JP, Holm S, Maroudas A, Nachemson A (1977) Nutrition of the intervertebral disk: an in vivo study of solute transport. Clin Orthop Relat Res (129):101–114
Wigfield C, Gill S, Nelson R, Langdon I, Metcalf N, Robertson J (2002) Influence of an artificial cervical joint compared with fusion on adjacent-level motion in the treatment of degenerative cervical disc disease. J Neurosurg 96:17–21
Wigfield CC, Gill SS, Nelson RJ, Metcalf NH, Robertson JT (2002) The new Frenchay artificial cervical joint: results from a two-year pilot study. Spine 27:2446–2452. doi:10.1097/00007632-200211150-00006
Wigfield CC, Skrzypiec D, Jackowski A, Adams MA (2003) Internal stress distribution in cervical intervertebral discs: the influence of an artificial cervical joint and simulated anterior interbody fusion. J Spinal Disord Tech 16:441–449. doi:10.1097/00024720-200310000-00002
Xu R, Ebraheim NA, Klausner T, Yeasting RA (1998) Modified Magerl technique of lateral mass screw placement in the lower cervical spine: an anatomic study. J Spinal Disord 11:237–240. doi:10.1097/00002517-199806000-00011
Acknowledgments
We thank Kristin Kraus, M.Sc., for her editorial assistance in preparing this paper. The experiments described in this paper comply with the current laws of the United States.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Finn, M.A., Brodke, D.S., Daubs, M. et al. Local and global subaxial cervical spine biomechanics after single-level fusion or cervical arthroplasty. Eur Spine J 18, 1520–1527 (2009). https://doi.org/10.1007/s00586-009-1085-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-009-1085-7