
Abstract
Introduction
Chronic anemia is a common, coinciding or presenting diagnosis in patients with paraesophageal hernia (PEH). Presence of endoscopically identified ulcerations frequently prompts surgical consultation in the otherwise asymptomatic patient with anemia. Rates of anemia resolution following paraesophageal hernia repair (PEHR) often exceed the prevalence of such lesions in the study population. A defined algorithm remains elusive. This study aims to characterize resolution of anemia after PEHR with respect to endoscopic diagnosis.
Materials and methods
Retrospective review of a prospectively maintained database of patients with PEH and anemia undergoing PEHR from 2007 to 2018 was performed. Anemia was determined by preoperative labs: Hgb < 12 mg/dl in females, Hgb < 13 mg/dl in males, or patients with ongoing iron supplementation. Improvement of post-operative anemia was assessed by post-operative hemoglobin values and continued necessity of iron supplementation.
Results
Among 56 identified patients, 45 were female (80.4%). Forty patients (71.4%) were anemic by hemoglobin value, 16 patients (28.6%) required iron supplementation. Mean age was 65.1 years, with mean BMI of 27.7 kg/m2. One case was a Type IV PEH and the rest Type III. 32 (64.0%) had potential source of anemia: 16 (32.0%) Cameron lesions, 6 (12.0%) gastric ulcers, 12 (24.0%) gastritis. 10 (20.0%) had esophagitis and 4 (8%) Barrett’s esophagus. 18 (36%) PEH patients had normal preoperative EGD. Median follow-up was 160 days. Anemia resolution occurred in 46.4% of patients. Of the 16 patients with pre-procedure Cameron lesions, 10 (63%) had resolution of anemia. Patients with esophagitis did not achieve resolution. 72.2% (13/18) of patients with no lesions on EGD had anemia resolution (p = 0.03).
Conclusion
Patients with PEH and identifiable ulcerations showed 50% resolution of anemia after hernia repair. Patients without identifiable lesions on endoscopy demonstrated statistically significant resolution of anemia in 72.2% of cases. Anemia associated with PEH adds an indication for surgical repair with curative intent.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Paraesophageal hernia (PEH), encompassing type II-IV hiatal hernias, are due to enlargement of the space between the diaphragmatic crura, resulting in protrusion of the stomach into the mediastinal space. Combined, these three types comprise 5% of hiatal hernias, while the remaining 95% are type 1, or sliding hiatal hernias [1, 2]. The development of paraesophageal hernias are thought to be secondary to increased intraabdominal pressure creating a pressure gradient between the thoracic and abdominal cavities, weakening the phrenoesophageal ligament and pleuroperitoneal membrane, and widening the diaphragmatic hiatus. The GEJ remains in the intraabdominal location, fixed by the posterolateral attachments of the phrenoesophageal ligaments; however, the fundus and body of the stomach may herniate into the thorax potentially resulting in [1] clinical sequelae including symptoms of dysphagia, regurgitation, vomiting, chest pain, upper GI bleeding, and iron deficiency anemia.
The association between paraesophageal hernia and anemia has been well documented for decades. Anemia is three times more frequent in patients with true paraesophageal hernia as compared to sliding hiatal hernia [2]. Previously hypothesized correlation between the presence of endoscopic findings of Cameron lesions and anemia in the setting of PEH may be true [3, 4]. Cameron lesions are linear erosions of the gastric mucosal folds, located at or near the level of the diaphragm, that frequently cause chronic iron deficiency anemia, occult bleeding, and occasionally life-threatening upper GI hemorrhage [3]. The lesions are attributed to mechanical trauma at the herniation site, although focal mucosal ischemia and gastric acid secretion are also associated [2, 3]. The lesions demonstrate a female predominance at 75% and tend to occur in patients over the age of 60. Recent studies have shown Cameron lesions to correlate with hernia size, with their presence noted in 10–20% of hiatal hernias over 5 cm in size [5].
In a study assessing resolution of anemia after PEHR, 88% of patients who had preoperative esophagogastric erosion or ulceration had resolution of their anemia post-operatively. This is compared to only 50% anemia resolution in patients without ulceration or erosion (p = 0.015) [2]. Another review cited the presence of Cameron lesions varying between 27 and 45% in patients with anemia undergoing any hiatal hernia repair, with post-operative resolution ranging from 60 to 100% [6,7,8,9]. Camus et al. attempted to quantify the utility of surgical repair versus PPI therapy in patients with bleeding Cameron’s lesions but did not detect any statistical difference between the two groups [4]. Furthermore, association with iron deficiency anemia and esophagitis has been studied with increased hazard ratio but without statistical significance [10].
Materials and methods
A retrospective review of a prospectively maintained IRB-approved UCSD database was performed of 154 patients who underwent laparoscopic or robotic repair of a paraesophageal hernia from April 2007 to January 2018. A paraesophageal hernia was defined as a type II, III, or IV hiatal hernia. PEH was diagnosed via barium swallow and upper endoscopy. Patient characteristics collected included age, sex, BMI, medical comorbidities, past surgical history, and ASA score. Additionally, data on initial symptomatic presentation and duration of symptomatology were collected. Presenting signs, symptoms, and preexisting comorbidities were collected, along with duration of symptoms prior to surgical intervention, and presence of esophageal or gastric ulcers or erosions by endoscopy. Prior history of anemia was documented, along with prior need for blood transfusion. Anemia was defined using the 2011 WHO guidelines: Hgb < 12 mg/dl in females, and Hgb < 13 mg/dl in males. Type of surgical repair was documented and included our standard approach with full mobilization of esophagus as required to attain intraabdominal position of the esophagus and GEJ. This was combined with primary crural repair with non-absorbable heavy suture and biosynthetic mesh crural reinforcement with suture or surgical glue fixation in all but one case. Alloderm (Allergan) was used in all cases in 2007, while BioA (Gore) mesh was utilized in cases from 2008 to 2018. Nissen or Toupet fundoplication was performed based on preoperative manometry or clinical status. Resolution or persistence of anemia, and continued need for iron supplementation were assessed. A p value of 0.05 was considered significant. Patients were also assessed for proton pump inhibitor (PPI) use before and after surgery. Finally, the cohort was then divided into anemia based on Hgb levels and anemia based on iron supplementation requirements.
Results
A total of 154 patients underwent laparoscopic or robotic paraesophageal hernia repair between April 2007 and January 2018. Within this group, a total of 56 (36.6%) patients met criteria for anemia: 40 (71.4%) were anemic by hemoglobin value, and 16 (28.6%) were on iron supplementation for documented iron deficiency anemia. The mean age was 65.1 (range 35–89) and mean BMI was 27.7 kg/m2 (range 17.8–39.6). Forty-five patients were female (80.4%). All patients had type III and IV hernias with rates of 98.2% and 1.8%, respectively. We had a 0% 30-day mortality rate and 3.6% (2/56) complication rate including dysphagia necessitating dilation, and left pneumothorax (Clavien-Dindo 3a,b, 4). Length of stay was median 2 days (range 0–25), and median follow-up time was 160 days (range 10–2179) (Table 1).
Preoperative esophagoduodenoscopy (EGD) was performed in 50 (89.3%) patients. According to EGD results, 32 patients (64%) had a potential identifiable source for their anemia. 16 patients (32%) had Cameron lesions, 6 patients (12%) had gastric ulcers, and 10 patients (20%) had esophagitis. The remaining 18 patients (36%) had no abnormal findings on EGD apart from the hernia itself (Table 2).
Resolution of anemia occurred in 26 of the total 56 patients (46.4%) (Table 3). Of those who had demonstrated Cameron’s lesions or gastric ulcers on EGD, 10/16 patients (63%) had anemia resolution. Uncomplicated esophagitis was refractory to surgical treatment, as 100% of patients with preprocedure esophagitis did not demonstrate an improvement in anemia (p = 0.001). 25% (1/4) of patients with Barrett’s esophagus had resolution of anemia post-procedure. 13/18 patients (72.22%) with no preoperative findings on EGD demonstrated resolution of anemia following PEHR (p =0.03) (Table 4).
Outcomes in those anemic patients presenting with low hemoglobin levels compared to those on iron supplementation were similar. The rates of resolution were 18/40 (45%) and 8/16 (50%), respectively (Tables 3a, b). When assessed based on EGD findings there remained no notable difference in outcomes (Table 4a, b).
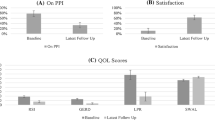
Finally, the use of PPI in the group was 91.1% (51/56) prior to surgical intervention. Of these patients, 51 were followed for post-operative use of PPI and 49% (25/51) were able to discontinue PPI therapy. However, only 11/25 (44%) showed resolution of their anemia. Of the remaining 26 patients who continued PPI therapy from the preoperative to post-operative phase, 46% (12/26) had resolution of anemia (Table 5).
Discussion
The association between paraesophageal hernia and chronic anemia is well documented [11, 12]. In the literature, anemia prevalence in patients with paraesophageal hernia is reported to be between 27 and 45%. This is in keeping with our observed value of 36.6%. In the absence of other identifiable sources of iron deficiency anemia, the role of surgical repair of paraesophageal hernias has been a poorly outlined treatment. Several studies have depicted successful results with high to complete resolution of anemia in the setting of surgical repair [8, 9, 13, 14]. Others allude to a potential toward resolution but fail to quantify these findings [6, 15]. The American Gastroenterology Association in 2000 highlighted PEHR in the algorithm of obscure GI bleeding lending to anemia, but this has yet to be widely adapted and seems to have been lost in more recent guidelines [16].
Endoscopic findings in patients with PEH, seemingly causative contributors to anemia, may direct medical or surgical management. Cameron’s lesions are a recurring discussion with regard to etiology of anemia with respect to large (> 5 cm) hernias. The obvious mechanical shearing at the level of the diaphragmatic pinch is only one proposed mechanism. Our prevalence of detectable Cameron’s lesions was only 32% which is lower than other studies and deserves further discussion [15]. Perhaps nomenclature for gastric ulcers is misleading but this is difficult to discern in this retrospective review. If these patients are included, the rates of Cameron’s lesions detected on EGD would be 44%. Other factors lending to anemia may involve mucosal ischemia and injury due to acid secretion. This has prompted many evaluations of the role of acid reduction therapy via H2 blockers or PPI as a treatment for anemia in this subset of patients with varying results and no strong evidence supporting superiority of surgical repair [4, 17]. The role of acid suppression may also be supported by the decreased use of PPI in the post-operative setting with PEH repair [18]. Our results did not support any trend toward resolution based on acid suppression in the pre- or post-operative setting. One could consider further evaluation in this regard focusing more specifically on medical versus surgical intervention with more objective follow-up. Finally, malabsorption with a chronically incarcerated stomach may be a provoking factor but one would suspect this would resolve with surgery.
Haurani et al. separated their study population of 68 patients with PEH and anemia into patients with and without evidence of Cameron lesions on preoperative upper endoscopy. They found that 88% of patients with esophagogastric erosion or ulceration achieved a normal hemoglobin level after surgical repair, while 50% of the patients without preoperative endoscopic findings were able to achieve normalization of their hemoglobin levels. With regard to preoperative esophagitis our findings are consistent with other studies with low to zero association with PEHR in the setting of anemia [10]. This was a statistically significant finding.
Our study demonstrates a more conservative finding with regard to anemia resolution in the setting of a known PEH, with or without preoperative endoscopic findings. The results draw to light a lack of confidence in PEHR for the treatment of anemia, given our 50% anemia resolution rate post-procedure. However, resolution pattern in the patients with no preoperative endoscopic findings was significant with a rate of 72.2% (p = 0.03). It also highlights the potential for cure in patients where no bleeding source is found. This “flip-of-the-coin” outcome could be due to the multifactorial etiology of the anemia itself. Formal pan-endoscopy, thorough overt bleeding history, and small bowel evaluation may tailor the patient population further adding diagnostic certainty prior to surgical evaluation. Practices of preoperative evaluation vary, but consideration of all causes of overt bleeding should be considered. However, investigations should be kept on balance with the probability of detection as well as overall preoperative symptomatology to avoid undue cost.
Further studies may look prospectively into medical versus surgical management based on the presence of endoscopic abnormalities in the setting of an otherwise asymptomatic PEH with close objective endoscopic and laboratory follow-up. Additionally, there may be utility in consistent intraoperative performance of prefundoplication endoscopy to again assess for abnormalities.
Limitations to our study include the retrospective nature of the data review leaving us without a true control group, lack of formal objective follow-up, and limited sample size. Additionally, the patient groups investigated for this study were heterogenous in nature, with some taking iron supplementation and PPI, and others without. While this might initially appear concerning for applicability of the study findings to a broader population, it should be noted that this heterogeneity reflects the characteristics of patients presenting to our clinic. Lastly, we do not routinely perform post-operative endoscopy to assess for healing of the Cameron lesions after PEH repair. The preoperative evaluation in otherwise asymptomatic patients aside must be thorough as there may be other underlying causes of obscure bleeding [19]. There are no guidelines as to the formal testing necessary and certainly the expense of exhaustive testing must be balanced with the rate of detection that is clinically relevant. Based on our outcomes, patients with PEH who have no underlying detectable cause for iron deficiency anemia and no endoscopic abnormalities may find resolution with surgical correction challenging the role of exhaustive testing.
The increasing use of minimally invasive surgical techniques in PEHR has provided a less morbid operative repair [20, 21]. Based on our outcomes, this should also be considered when assessing risk/benefit of a surgical intervention and management plan should be tailored to individual patients.
Conclusion
PEHR in anemic patients, with endoscopically identifiable sources, may lend to resolution of anemia in 50% of cases. The presence of Cameron’s ulcers portends a higher resolution rate of 63%. Patients with no abnormalities on endoscopy demonstrated a resolution rate of 72.2% (p = 0.03) Esophagitis remains a non-contributing source of anemia in these patients with 0% resolution following repair (p = 0.001). Preoperative workup and surgical intervention should remain individualized. However, in the absence of other identifiable etiologies of overt bleeding, PEHR may be considered a viable surgical option for anemia treatment with low perioperative risk. Anemia associated with PEH adds an indication for surgical repair with curative intent.
References
Dangleben DA, Du C (2017) Paraesophageal hernia. Acute Care Gen Surg 95(3):101–106. https://doi.org/10.1016/j.suc.2015.02.008
Haurani C, Carlin AM, Hammoud ZT, Velanovich V (2012) Prevalence and resolution of anemia with paraesophageal hernia repair. J Gastrointest Surg 16(10):1817–1820
Fiorini G, Lahner E, Annibale B, Zullo A, De Francesco V, Vaira D et al (2018) Cameron lesions: a still overlooked diagnosis Case report and systematic review of literature. Clin Res Hepatol Gastroenterol 42(6):604–609. https://doi.org/10.1016/j.clinre.2018.05.002
Wideman TH, Zautra AJ, Edwards RR (2014) Re-thinking the fear avoidance model: toward a multi-dimensional framework of pain-related disability. NIH Public Access 154(11):2262–2265
Maganty K, Smith RL (2008) Cameron lesions: unusual cause of gastrointestinal bleeding and anemia. Digestion 77(3–4):214–217
Carrott PW, Hong J, Kuppusamy M, Koehler RP, Low DE (2012) Clinical ramifications of giant paraesophageal hernias are underappreciated: Making the case for routine surgical repair. Ann Thorac Surg 94(2):421–428. https://doi.org/10.1016/j.athoracsur.2012.04.058
Velanovich V, Karmy-Jones R (2003) Surgical Management of paraesophageal hernias: outcome and quality of life analysis/with invited commentary. Dig Surg 18(6):432–438
Skipworth RJE, Staerkle RF, Leibman S, Smith GS (2014) Transfusion-dependent anaemia: an overlooked complication of paraoesophageal hernias. Int Sch Res Not 2014:1–4
Hayden H, Jamieson J (2005) Diseases of the esophagus effect on iron deficiency anemia of laparoscopic repair of large paraesophageal hernias. Dis Esophagus 18(5):329–331
Ruhl CE, Everhart JE (2001) Relationship of iron-deficiency anemia with esophagitis and hiatal hernia: hospital findings from a prospective, population-based study. Am J Gastroenterol 96(2):322–326
Windsor CW, Collis JL (1967) Anaemia and hiatus hernia: experience in 450 patients. Thorax 22(1):73–78
Carrott PW, Markar SR, Hong J, Kuppusamy MK, Koehler RP, Low DE (2013) Iron-deficiency anemia is a common presenting issue with giant paraesophageal hernia and resolves following repair. J Gastrointest Surg 17(5):858–862
Eubanks TR, Pellegrini CA, Jacobsen G, Horgan S, Omelanczuk P (2002) Repair of paraesophageal hernias. Am J Surg 177(5):354–358
Trastek VF, Allen MS, Deschamps C, Pairolero PC, Thompson A, Altorki N (1996) Diaphragmatic hernia and associated anemia: response to surgical treatment. J Thorac Cardiovasc Surg 112(5):1340–1345
Chevrollier GS, Brown AM, Keith SW, Szewczyk J, Pucci MJ, Chojnacki KA et al (2019) Preoperative anemia: a common finding that predicts worse outcomes in patients undergoing primary hiatal hernia repair. Surg Endosc. 33(2):535–542. https://doi.org/10.1007/s00464-018-6328-4
Zuckerman GR, Prakash C, Askin MP, Lewis BS (2000) AGA technical review on the evaluation and management of occult and obscure gastrointestinal bleeding. Gastroenterology 118(1):201–221
Delle Fave G, Annibale B, Di Giulio E, Capurso G, Baccini F, Panzuto F et al (2004) Large hiatal hernia in patients with iron deficiency anaemia: a prospective study on prevalence and treatment. Aliment Pharmacol Ther 19(6):663–670
El Khoury R, Ramirez M, Hungness ES, Soper NJ, Patti MG (2015) Symptom relief after laparoscopic paraesophageal hernia repair without mesh. J Gastrointest Surg 19(11):1938–1942
D’Ambra G, Fave GD, Lahner E, Capurso G, Di Giulio E, Annibale B et al (2003) Role of small bowel investigation in iron deficiency anaemia after negative endoscopic/histologic evaluation of the upper and lower gastrointestinal tract. Dig Liver Dis 35(11):784–787
Karmali S, McFadden S, Mitchell P, Graham A, Debru E, Gelfand G et al (2008) Primary laparoscopic and open repair of paraesophageal hernias: a comparison of short-term outcomes. Dis Esophagus 21(1):63–68
Hinojosa MW, Reavis KM, Parikh D, Varela E, Nguyen NT (2012) Utilization and outcomes of laparoscopic versus open paraesophageal hernia repair. Am Surg 2014:90035
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr. Horgan has stock options with TORAX™ Medical Inc. Dr. Jacobsen has two grants with TORAX™ Medical Inc, the first for The CALIBER Study: Randomized Controlled Trial of LINX versus Double-Dose Proton Pump Inhibitor Therapy for Reflux Disease, and the second for A Post-Approval Study of the LINX®Reflux management system. Drs. Cheverie, Broderick, Lam, Lee, Neki, Matsuzaki, Cubas, Sandler, and Fuchs have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Cheverie, J.N., Lam, J., Neki, K. et al. Paraesophageal hernia repair: a curative consideration for chronic anemia?. Surg Endosc 34, 2243–2247 (2020). https://doi.org/10.1007/s00464-019-07014-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-019-07014-3