
Abstract
Background
To improve patient safety, training of psychomotor laparoscopic skills is often done on virtual reality (VR) simulators outside the operating room. Haptic sensations have been found to influence psychomotor performance in laparoscopy. The emulation of haptic feedback is thus an important aspect of VR simulation. Some VR simulators try to simulate these sensations with handles equipped with haptic feedback. We conducted a survey on how laparoscopic surgeons perceive handles with and without haptic feedback.
Methods
Surgeons with different levels of experience in laparoscopy were asked to test two handles: Xitact IHP with haptic feedback and Xitact ITP without haptic feedback (Mentice AB, Gothenburg, Sweden), connected to the LapSim (Surgical Science AB, Sweden) VR simulator. They performed two tasks on the simulator before answering 12 questions regarding the two handles. The surgeons were not informed about the differences in the handles.
Results
A total of 85 % of the 20 surgeons who participated in the survey claimed that it is important that handles with haptic feedback feel realistic. Ninety percent of the surgeons preferred the handles without haptic feedback. The friction in the handles with haptic feedback was perceived to be as in reality (5 %) or too high (95 %). Regarding the handles without haptic feedback, the friction was perceived as in reality (45 %), too low (50 %), or too high (5 %). A total of 85 % of the surgeons thought that the handle with haptic feedback attempts to simulate the resistance offered by tissue to deformation. Ten percent thought that the handle succeeds in doing so.
Conclusions
The surveyed surgeons believe that haptic feedback is an important feature on VR simulators; however, they preferred the handles without haptic feedback because they perceived the handles with haptic feedback to add additional friction, making them unrealistic and not mechanically transparent.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Technical ability is an important part of surgical competence [1, 2]. To improve patient safety, training of psychomotor skills can be done outside the operating room (OR) on virtual reality (VR) simulators or box trainers [3, 4]. The nature of image-based minimally access surgery—for example, laparoscopy, where surgeons insert instruments through small incisions or natural orifices and use perioperative images to guide the intervention—makes it amenable to VR simulation [5, 6]. The VR simulator uses a computer and physical interfaces representing surgical instruments and instrument ports to simulate a virtual surgical environment with which the user can interact [6–8].
An important aspect of VR simulators is the reproduction of the challenges a surgeon encounters during surgery—challenges related to vision and touch [9]. The sensation of touch and proprioception, or haptic sensations [10–12], are weaker in laparoscopy compared to open surgery [11, 13, 14]. Nevertheless, the surgeon can still perceive haptic sensations through the instruments as they touch the trocars, the abdominal wall, organs, and other physical objects within the surgical environment [15]. The control of forces related to grasping and pulling is essential when performing surgery; the inability to control these forces may result in tissue slippage if the applied pinching forces are too small, or tissue damage if the forces are too high [16]. As such, the training of skills related to haptic sensations is essential [14, 17–19], and the emulation of virtual haptic feedback is an important feature of a VR simulator [20]. A number of VR simulators try to simulate haptic sensations [7, 21] with actuators (motors) built into the device imitating the trocar. The actuators exert a force on the instrument to create vibrations and resistance, giving the user the illusion of touch when interacting with virtual objects (Fig. 1) [11].

Simplified model of a haptic feedback device. The actuators in the imitated trocar exert a force on the instrument depending on the characteristics of the virtual object and the force applied to the instrument by the user
The word haptic is of Greek origin and relates to the sense of touch—that is, the perception and manipulation of objects using the senses of touch and proprioception, which further can be divided into what is felt by the cutaneous receptors located in the skin allowing the detection of pressure, vibration, texture, heat, and pain and the kinesthetic receptors in muscles and joints that sense the position and movements of muscles and bones [11]. In laparoscopy, the haptic sensations felt by the surgeon are tool mediated [22]; that is, they are felt through the laparoscopic instruments. This makes the haptic interaction less complex to simulate than with direct contact interaction, as is the case in open surgery where the surgeon interacts with tissue directly with his or her gloved fingers. The virtual reproduction of the tactile and kinesthetic sensory input in laparoscopy therefore consists of imposing to the laparoscopic instrument mock-up the same forces that a real instrument would undergo as it interacted with the surgical environment.
For tool-mediated interaction, a kinesthetic haptic interface is, in theory, relatively straightforward: it ought to emulate perfect rigidity when in contact with a virtual rigid object and be mechanically transparent when moving through empty space. In practice, though, realistic haptic feedback on VR simulators is difficult to achieve [13, 21], due to insufficient mechanical performance of the device, in terms of frequency response, fidelity in force reproduction and force resolution [22]. In addition, this technology is usually an expensive add-on [13, 23–25] to these systems. Because little is known about how laparoscopic surgeons perceive VR simulators with and without haptic feedback, we conducted a survey to investigate it.
Methods
Surgeons with different levels of experience in laparoscopy were asked to try two instrument ports commonly used in VR simulators [21] and to give an opinion on them: the Xitact IHP (instrument haptic port) with haptic feedback (Fig. 2) and the Xitact ITP (instrument tracking port) without haptic feedback (Fig. 3) (Mentice AB, Gothenburg, Sweden). The instrument ports were connected to the LapSim VR simulator (Surgical Science AB, Gothenburg, Sweden). Throughout, we use the common term handle to describe the instrument mock-up including the instrument port imitating the trocar, the instrument shaft, and the grip (e.g., a pistol grip).

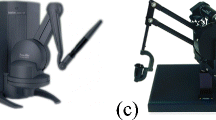
XitactTM instrument haptic ports (IHP) with haptic feedback (courtesy Mentice AB)

XitactTM instrument tracking port (ITP) without haptic feedback (courtesy Mentice AB)
The surgeons performed two tasks: fine dissection, and lifting and grasping. The order of testing the handles and the tasks were randomized. The surgeons were not informed about the differences in the handles. After testing the two handles, they answered a questionnaire containing seven questions related to their background and 12 questions related to their perception of the two handles. All questions were closed format—that is, they did not allow additional text to be added. Questions related to the two handles consisted of two 5-point rating scale questions, two bipolar questions, and two dichotomous questions, including a “do not know” option. The questions were phrased in common language, avoiding terms like haptic feedback. The questionnaire was anonymous. The answers were summarized with descriptive statistics and nonparametric tests at significance level 0.05 by SPSS software, version 19.0 (IBM, Armonk, NY, USA).
Results
Twenty surgeons with experience in laparoscopy participated in the survey. Eleven had performed fewer than 100 laparoscopic procedures; five between 101 and 1,000 laparoscopic procedures; and four more than 1,000 laparoscopic procedures. All participants completed the survey. There were 15 men and five women. Eleven participants had previous experience with VR simulators. Fourteen were between 30 and 40 years old, and six were older than 41.
No statistically significant differences were found when comparing the answers from men and women, from those with and without previous experience with VR simulators, or from members of the two age groups. One question was answered by 19 surgeons, whereas the other questions were answered by 20 surgeons.
Fifteen of 19 surgeons (79 %) claimed that handles with haptic feedback on VR simulators are important, given that they feel realistic (score 4 or 5, where 5 is the most important) (Fig. 4). Eighty-five percent of the participants stated that it is important that a handle that tries to imitate and provide the perception of tissue stiffness feels realistic—that is, that the forces felt when holding the handle are realistic and proportional to the stiffness of the tissue that the handle touches virtually (Fig. 4). Fourteen surgeons (70 %) thought the handle without haptic feedback felt most realistic, while four (20 %) of the participants said that the handles with haptic feedback imitated reality best. Two participants (10 %) thought both handles imitated reality equally well (P < 0.02, one-sample Chi-square test) (Fig. 5).

The surgeons’ answers to the questions, “How important it is that the handle has haptic feedback given that it is realistic” and “How important it is that a handle with haptic feedback feels realistic” on a scale of 1 (unimportant) to 5 (very important). The results are presented as box plots where the middle band shows the median value, the bottom and top of the boxes show the 25th and 75th percentiles, and the ends of the whiskers show the 5th and 95th percentile. Outliers are plotted as circles

Surgeons’ answers to which of the two handles they thought imitated reality the best (error bars with P = 0.05)
After the test, the surgeons were informed that one of the handles tries to simulate the resistance offered by tissue when deformed. When asked which handle they thought it was, 85 % (n = 17) of them answered the Xitact IHP (the handle with haptic feedback), 5 % (n = 1) answered the Xitact ITP, and 10 % (n = 2) answered that they did not know (P < 0.00, one-sample Chi-square test). Of the 17 surgeons who thought that the Xitact IHP handles provided haptic feedback, two (12 %) thought the handles succeeded in doing so. Eighteen (90 %) of the surgeons preferred the handles without haptic feedback, while two surgeons (10 %) favored both equally well (P < 0.00, one-sample binominal test) (Fig. 6).

Number of surgeons who preferred one of the handles or both equally well (error bars with P = 0.05)
The friction when using the handles with haptic feedback was perceived to be as in reality (n = 1, 5 %) or too high (n = 19, 95 %) (Fig. 7). Regarding the handles without haptic feedback, the friction was perceived to be as in reality (n = 9, 45 %), too low (n = 10, 50 %), or too high (n = 1, 5 %) (Fig. 7). Eighty-five percent (n = 17) of the participants thought they performed best with the handles without haptic feedback, while 10 % (n = 2) thought they performed best using the handles with haptic feedback. One participant (5 %) did not notice a difference (P < 0.00, one-sample Chi-square test).

Repartition of number of surgeons who found the friction in the mimicked trocars to be “as in reality,” “too low,” or “too high” for each of the two handles
Discussion
Haptic sensations in laparoscopy are limited compared to open surgery [11, 13, 14] but are stronger compared to robotic surgery, where they are almost nonexistent [26]. Although they are still not completely understood [9, 12, 15, 17, 25], haptic sensations have been found to be an important part of laparoscopy [14, 17, 18]. Studies showed that for maneuvers such as grasping and pulling, although changed as they are mediated through the laparoscopic instruments, how to perform them is better retained when learned on training devices with realistic haptic feedback [17, 27–29]. Haptic feedback is thus an important add-on for VR simulators in laparoscopic skills training [7, 20, 28–30]. Similarly, in this survey, most of the surgeons (79 %) believed that it is important that a VR simulator has haptic feedback.
It has been found that haptic devices not only influence how skills are acquired and transferred to the OR, but also that they influence performance scores [31, 32]. As such, care should be taken when comparing results from the same VR simulator, but equipped with different kinds of handles (with and without haptic feedback). Buzink et al. [31] performed a study on the SimSurgery SEP VR simulator with Xitact IHP haptic feedback instrument ports and found that the participants’ performance scores were inferior to those obtained when performing the same tasks on the SEP simulator with the original handles without haptic feedback from Simpack. This correlates with the results of our study, which demonstrated that 85 % of the surveyed surgeons had the impression that they performed better with the handles without haptic feedback.
The results of this study are in large part unidirectional and show statistically significant results. They indicate that attention should be paid not only to the validation of simulated training tasks, but also to the validation of the whole training setup, including the presence of haptic feedback. More confidence in the findings can be gained by conducting a multicenter study with a larger number of participants. We did not inform the participants about the differences in the handles before the test. The physical differences, although minor, were visible to the participants. This might have influenced the way they perceived the handles.
Despite the importance of haptic feedback on training results, it is not always explicitly described in the literature whether the handles in the training setup include haptic feedback [33]. This makes it difficult for the surgical community to compare results obtained in different studies and to make correct use of them. Of 17 construct validity studies on the LapSim VR simulator [34–50], seven studies did not explicitly describe the type of handles used [34, 39, 41–44, 50]. In three other studies [23–25], it was found that having the haptic feedback software activated did not make a difference. None of the three studies, however, described the hardware of the handles, nor did they mention the influence of the haptic hardware.
Haptic devices [51] try to simulate haptic sensations felt by cutaneous receptors, primarily sensations felt by the fingertips (tactile devices) or by simulating sensations felt by kinesthetic receptors in muscles and bones (kinesthetic or force feedback devices). In laparoscopy, the haptic sensations are limited compared to open surgery, mainly because the cutaneous receptors in the fingertips are not in direct contact with the organs, limiting direct palpations. The haptic sensations still present in laparoscopy are therefore primarily kinesthetic sensations, making a haptic device on a laparoscopic VR simulator mainly a force feedback device. In the literature related to haptic sensations in laparoscopy, the terms tactile feedback [10, 15], force feedback [14, 17, 21], or simply haptic feedback [20, 21, 23, 28, 52] are used. We chose throughout the study to use the term haptic feedback to include both force and tactile feedback. In the questionnaire, we phrased the questions omitting words like haptic, tactile, or force feedback, instead using phrases like, “Do you think the handle succeeds in giving a sensation of tissue stiffness?” We did this to avoid misunderstandings related to the different terms.
A VR simulator has many advantages compared to other training modalities like box trainers, such as highly developed assessment tools [53], built-in formative feedback [21], and the possibility of simulating complex procedural tasks [33]. One of its disadvantages compared to box trainers is the lack of natural haptic feedback [27]. Several studies have investigated the differences in skill acquisition [17, 28, 54–56] and in the capability of detecting differences in levels of surgical experience [57] between VR simulators without haptic feedback and box trainers with natural haptic feedback. The results diverge, but three studies found that haptic feedback aids in the retention of skills [17, 28, 56], one study found that there were no differences [54], and Tanoue et al. [55] found that training on VR simulators and box trainers is complementary, and a combination of them should be included in a training curriculum. Avgerinos et al. [57] found that a box trainer is more sensitive in detecting differences in surgical experience than a VR simulator without haptic feedback. In a study by Youngblood et al. [58] where a VR simulator with haptic feedback was compared to a box trainer, they found that skills were better retained on the VR simulator. Botden et al. [35] and Zhou et al. [28] compared an augmented reality trainer to a VR trainer without haptic feedback and found that the augmented reality trainer was perceived as a better training tool, probably because of the natural force feedback [35], and that learning with haptic feedback was more efficient during the first 5 h of training [28]. An augmented reality trainer uses physical objects and standard laparoscopic instruments like a box trainer, but in addition incorporates tracking of the instruments to score training performance.
Realistic haptic feedback is desired, but it has been technically difficult to achieve in VR simulators [13, 21]. To simulate haptic feedback, the interaction between the physical representation of the surgical tools and the virtual tissue and organs must be tracked to detect collisions at interactive frame rates. A haptic device has to be updated with a frequency of 1 kHz to seem real and stable, compared to 30 Hz for a visual display [5, 20, 52]. Further, the tissue properties of the virtual object and the corresponding virtual forces of resistance offered by tissue to deformation need to be calculated to find the magnitude of haptic feedback—that is, the force reflected to the user [12, 20, 52]. The haptic device needs a mechanism to transmit the virtual reflected forces to the user through the instrument. A possible way of transmitting the reflected forces is to have actuators in the device imitating the trocar (Fig. 1), as the Xitact IHP does. The actuators exert a force on the instrument depending on the virtual reflected forces, creating an illusion of touch when interacting with virtual objects. The difficulty with such a solution is to achieve mechanical transparency when moving through empty space. Our study shows that realistic haptic feedback has not been achieved in the tested handles, and that the Xitact IPH handles are not perceived as mechanically transparent. A total of 95 % of the surgeons in our study found that the simulation of haptic feedback by the Xitact IHP added unrealistic high friction when moving the instruments in and out of the device, imitating the trocars. On the other hand, half of the surgeons found that the friction in the handles without haptic feedback was too low.
Today there is limited knowledge of how unrealistic haptic feedback influences skills acquisition and transfer to the OR [17]. Future studies should include analysis of the way haptic sensations affect the performance of laparoscopy and the acquisition of laparoscopic skills, together with how a VR simulator could implement haptic feedback to best enhance laparoscopic skills training. Technological advances on haptic devices, together with results from randomized, controlled studies on haptic feedback, will help us develop efficient and effective training curricula and establish the true value of costly equipment in training and assessing laparoscopic skills.
References
van Hove PD, Tuijthof GJ, Verdaasdonk EG, Stassen LP, Dankelman J (2010) Objective assessment of technical surgical skills. Br J Surg 97:972–987
Reznick RK, MacRae H (2006) Teaching surgical skills—changes in the wind. N Engl J Med 355:2664–2669
Gallagher AG, Traynor O (2008) Simulation in surgery: opportunity or threat? Ir J Med Sci 177:283–287
Aggarwal R, Mytton OT, Derbrew M, Hananel D, Heydenburg M, Issenberg B, MacAulay C, Mancini ME, Morimoto T, Soper N, Ziv A, Reznick R (2010) Training and simulation for patient safety. Qual Saf Health Care 19(suppl 2):i34–i43
Liu A, Tendick F, Cleary K, Kaufmann C (2003) A survey of surgical simulation: applications, technology, and education. Presence Teleop Virt 12:599–614
Seymour NE (2008) VR to OR: a review of the evidence that virtual reality simulation improves operating room performance. World J Surg 32:182–188
Schijven M, Jakimowicz J (2003) Virtual reality surgical laparoscopic simulators. Surg Endosc 17:1943–1950
Satava RM (2001) Surgical education and surgical simulation. World J Surg 25:1484–1489
Picod G, Jambon AC, Vinatier D, Dubois P (2005) What can the operator actually feel when performing a laparoscopy? Surg Endosc 19:95–100
Ottermo MV, Ovstedal M, Lango T, Stavdahl O, Yavuz Y, Johansen TA, Marvik R (2006) The role of tactile feedback in laparoscopic surgery. Surg Laparosc Endosc Percutan Tech 16:390–400
Westebring-van der Putten EP, Goossens RH, Jakimowicz JJ, Dankelman J (2008) Haptics in minimally invasive surgery—a review. Minim Invasive Ther Allied Technol 17:3–16
Lamata P, Gomez EJ, Sanchez-Margallo FM, Lamata F, Antolin M, Rodriguez S, Oltra A, Uson J (2006) Study of laparoscopic forces perception for defining simulation fidelity. Stud Health Technol Inform 119:288–292
van der Meijden OA, Schijven MP (2009) The value of haptic feedback in conventional and robot-assisted minimal invasive surgery and virtual reality training: a current review. Surg Endosc 23:1180–1190
Tholey G, Desai JP, Castellanos AE (2005) Force feedback plays a significant role in minimally invasive surgery: results and analysis. Ann Surg 241:102–109
Bholat OS, Haluck RS, Murray WB, Gorman PJ, Krummel TM (1999) Tactile feedback is present during minimally invasive surgery. J Am Coll Surg 189:349–355
Westebring-van der Putten EP, van den Dobbelsteen JJ, Goossens RH, Jakimowicz JJ, Dankelman J (2009) Effect of laparoscopic grasper force transmission ratio on grasp control. Surg Endosc 23:818–824
Chmarra MK, Dankelman J, van den Dobbelsteen JJ, Jansen FW (2008) Force feedback and basic laparoscopic skills. Surg Endosc 22:2140–2148
van den Dobbelsteen JJ, Schooleman A, Dankelman J (2007) Friction dynamics of trocars. Surg Endosc 21:1338–1343
Sjoerdsma W, Herder JL, Horward MJ, Jansen A, Bannenberg JJG, Grimbergen CA (1997) Force transmission of laparoscopic grasping instruments. Minim Invasive Ther 6:274–278
Basdogan C, De S, Kim J, Muniyandi M, Kim H, Srinivasan MA (2004) Haptics in minimally invasive surgical simulation and training. IEEE Comput Graph Appl 24:56–64
Lamata P, Gomez EJ, Bello F, Kneebone RL, Aggarwal R, Lamata F (2006) Conceptual framework for laparoscopic VR simulators. IEEE Comput Graph 26:69–79
El Saddik A (ed) (2012) Haptics rendering and applications. InTech, faridabad, p 246
Salkini MW, Doarn CR, Kiehl N, Broderick TJ, Donovan JF, Gaitonde K (2010) The role of haptic feedback in laparoscopic training using the LapMentor II. J Endourol 24:99–102
Panait L, Akkary E, Bell RL, Roberts KE, Dudrick SJ, Duffy AJ (2009) The role of haptic feedback in laparoscopic simulation training. J Surg Res 156:312–316
Thompson JR, Leonard AC, Doarn CR, Roesch MJ, Broderick TJ (2011) Limited value of haptics in virtual reality laparoscopic cholecystectomy training. Surg Endosc 25:1107–1114
Okamura AM (2009) Haptic feedback in robot-assisted minimally invasive surgery. Curr Opin Urol 19:102–107
Botden SM, Torab F, Buzink SN, Jakimowicz JJ (2008) The importance of haptic feedback in laparoscopic suturing training and the additive value of virtual reality simulation. Surg Endosc 22:1214–1222
Zhou M, Tse S, Derevianko A, Jones DB, Schwaitzberg SD, Cao CG (2012) Effect of haptic feedback in laparoscopic surgery skill acquisition. Surg Endosc 26:1128–1134
Strom P, Hedman L, Sarna L, Kjellin A, Wredmark T, Fellander-Tsai L (2006) Early exposure to haptic feedback enhances performance in surgical simulator training: a prospective randomized crossover study in surgical residents. Surg Endosc 20:1383–1388
Yiasemidou M, Glassman D, Vasas P, Badiani S, Patel B (2011) Faster simulated laparoscopic cholecystectomy. Open Access Surg 4:39–44
Buzink SN, Goossens RH, De Ridder H, Jakimowicz JJ (2010) Training of basic laparoscopy skills on SimSurgery SEP. Minim Invasive Ther Allied Technol 19:35–41
Vapenstad C, Hofstad EF, Bo LE, Chmarra MK, Kuhry E, Johnsen G, Marvik R, Lango T (2012) Limitations of haptic feedback devices on construct validity on the LapSim® virtual reality simulator. Surg Endosc. doi:10.1007/s00464-012-2621-9
Vapenstad C, Buzink SN (2012) Procedural virtual reality simulation in minimally invasive surgery. Surg Endosc. doi:10.1007/s00464-012-2503-1
Ro CY, Toumpoulis IK, Ashton RC Jr, Jebara T, Schulman C, Todd GJ, Derose JJ Jr, McGinty JJ (2005) The LapSim: a learning environment for both experts and novices. Stud Health Technol Inform 111:414–417
Botden SM, Buzink SN, Schijven MP, Jakimowicz JJ (2007) Augmented versus virtual reality laparoscopic simulation: what is the difference? A comparison of the ProMIS augmented reality laparoscopic simulator versus LapSim virtual reality laparoscopic simulator. World J Surg 31:764–772
Ahlberg G, Enochsson L, Gallagher AG, Hedman L, Hogman C, McClusky DA 3rd, Ramel S, Smith CD, Arvidsson D (2007) Proficiency-based virtual reality training significantly reduces the error rate for residents during their first 10 laparoscopic cholecystectomies. Am J Surg 193:797–804
van Dongen KW, Tournoij E, van der Zee DC, Schijven MP, Broeders IA (2007) Construct validity of the LapSim: can the LapSim virtual reality simulator distinguish between novices and experts? Surg Endosc 21:1413–1417
Aggarwal R, Tully A, Grantcharov T, Larsen CR, Miskry T, Farthing A, Darzi A (2006) Virtual reality simulation training can improve technical skills during laparoscopic salpingectomy for ectopic pregnancy. BJOG 113:1382–1387
Aggarwal R, Grantcharov TP, Eriksen JR, Blirup D, Kristiansen VB, Funch-Jensen P, Darzi A (2006) An evidence-based virtual reality training program for novice laparoscopic surgeons. Ann Surg 244:310–314
Larsen CR, Grantcharov T, Aggarwal R, Tully A, Sorensen JL, Dalsgaard T, Ottesen B (2006) Objective assessment of gynecologic laparoscopic skills using the LapSimGyn virtual reality simulator. Surg Endosc 20:1460–1466
Hassan I, Maschuw K, Rothmund M, Koller M, Gerdes B (2006) Novices in surgery are the target group of a virtual reality training laboratory. Eur Surg Res 38:109–113
Woodrum DT, Andreatta PB, Yellamanchilli RK, Feryus L, Gauger PG, Minter RM (2006) Construct validity of the LapSim laparoscopic surgical simulator. Am J Surg 191:28–32
Eriksen JR, Grantcharov T (2005) Objective assessment of laparoscopic skills using a virtual reality stimulator. Surg Endosc 19:1216–1219
Langelotz C, Kilian M, Paul C, Schwenk W (2005) LapSim virtual reality laparoscopic simulator reflects clinical experience in German surgeons. Langenbecks Arch Surg 390:534–537
Sherman V, Feldman LS, Stanbridge D, Kazmi R, Fried GM (2005) Assessing the learning curve for the acquisition of laparoscopic skills on a virtual reality simulator. Surg Endosc 19:678–682
Duffy AJ, Hogle NJ, McCarthy H, Lew JI, Egan A, Christos P, Fowler DL (2005) Construct validity for the LAPSIM laparoscopic surgical simulator. Surg Endosc 19:401–405
van Dongen KW, Ahlberg G, Bonavina L, Carter FJ, Grantcharov TP, Hyltander A, Schijven MP, Stefani A, van der Zee DC, Broeders IA (2011) European consensus on a competency-based virtual reality training program for basic endoscopic surgical psychomotor skills. Surg Endosc 25(1):166–171
Hassan I, Sitter H, Schlosser K, Zielke A, Rothmund M, Gerdes B (2005) A virtual reality simulator for objective assessment of surgeons’ laparoscopic skill. Chirurg 76:151–156
Danila R, Gerdes B, Ulrike H, Dominguez Fernandez E, Hassan I (2009) Objective evaluation of minimally invasive surgical skills for transplantation. Surgeons using a virtual reality simulator. Chirurgia (Bucur) 104:181–185
Tanoue K, Uemura M, Kenmotsu H, Ieiri S, Konishi K, Ohuchida K, Onimaru M, Nagao Y, Kumashiro R, Tomikawa M, Hashizume M (2010) Skills assessment using a virtual reality simulator, LapSim, after training to develop fundamental skills for endoscopic surgery. Minim Invasive Ther Allied Technol 19:24–29
Salisbury K, Conti F, Barbagli F (2004) Haptic rendering: introductory concepts. IEEE Comput Graph Appl 24:24–32
Liu P, Zheng W, Chebbi B (2007) Surgical simulation with high-fidelity haptic feedback. Int J Robot Autom 22:59–68
Hofstad EF, Vapenstad C, Chmarra MK, Lango T, Kuhry E, Marvik R (2012) A study of pshycomotor skills in minimally invasive surgery: what differntiates expert and non-expert performance. Surg Endosc. doi:10.1007/s00464-012-2524-9
Munz Y, Kumar BD, Moorthy K, Bann S, Darzi A (2004) Laparoscopic virtual reality and box trainers: is one superior to the other? Surg Endosc 18:485–494
Tanoue K, Ieiri S, Konishi K, Yasunaga T, Okazaki K, Yamaguchi S, Yoshida D, Kakeji Y, Hashizume M (2008) Effectiveness of endoscopic surgery training for medical students using a virtual reality simulator versus a box trainer: a randomized controlled trial. Surg Endosc 22:985–990
Hiemstra E, Terveer EM, Chmarra MK, Dankelman J, Jansen FW (2011) Virtual reality in laparoscopic skills training: is haptic feedback replaceable? Minim Invasive Ther Allied Technol 20(3):179–184
Avgerinos DV, Goodell KH, Waxberg S, Cao CG, Schwaitzberg SD (2005) Comparison of the sensitivity of physical and virtual laparoscopic surgical training simulators to the user’s level of experience. Surg Endosc 19:1211–1215
Youngblood PL, Srivastava S, Curet M, Heinrichs WL, Dev P, Wren SM (2005) Comparison of training on two laparoscopic simulators and assessment of skills transfer to surgical performance. J Am Coll Surg 200:546–551
Acknowledgments
We thank all those who participated in the study. The work has been supported by the National Centre for Advanced Laparoscopic Surgery, SINTEF, the National Competence Services for Ultrasound and Image guided Therapy, the Norwegian University of Science and Technology (NTNU), Trondheim, Norway; and the Marie Curie ITN EU project “Integrated Interventional Imaging Operating System” (project 238802).
Disclosures
C. Våpenstad, E. F. Hofstad, T. Langø, R. Mårvik, and M. K. Chmarra have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Våpenstad, C., Hofstad, E.F., Langø, T. et al. Perceiving haptic feedback in virtual reality simulators. Surg Endosc 27, 2391–2397 (2013). https://doi.org/10.1007/s00464-012-2745-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-012-2745-y