
Abstract
Background
Endoscopic submucosal dissection (ESD) yields substantially high rates for curative resection of early gastric cancer (EGC). It is suggested that larger, ulcerative, or upper EGCs may prevent successful ESD. A detailed analysis of factors associated with the curability of ESD was performed.
Methods
Endoscopic submucosal dissection was performed for patients with EGC that fulfilled the expanded criteria, which specified mucosal cancer without ulcer findings irrespective of tumor size, mucosal cancer with ulcers 3 cm in diameter or smaller, and minute submucosal invasive cancer 3 cm or smaller. Resectability (en bloc or by piecemeal resection), curability (curative or non-curative), and complications were assessed, and logistic regression analysis was used to analyze the related factors.
Results
Ulcerative EGCs showed a significantly higher risk associated with ESD on multivariate analysis. When the risk factors (tumor size, location, and ulcer findings) were combined, the larger EGCs (>30 mm) located in the upper third or ulcerative tumors located in the upper and middle portion of the stomach were at significantly higher risk of non-curative resection. Such lesions also were associated with increased risk of procedure-related perforation.
Conclusions
When risk factors including positive ulcer findings and larger size and upper location of tumors are combined, ESD should be performed more carefully.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Early gastric cancer (EGC) is defined as gastric cancer confined to the mucosa or submucosa (T1 cancer) irrespective of whether regional lymph node metastases is present [1]. Currently, almost 10,000 cases of EGC are detected annually in Japan, accounting for 40% to 50% of all gastric cancers [2].
Because endoscopic mucosal resection (EMR) is minimally invasive, safe, and convenient, it is widely accepted as a standard treatment for EGC with nominal risk of lymph node metastasis [3, 4]. However, the snaring procedure is not reliable for lesions larger than 20 mm in diameter or lesions with ulcer findings [5, 6]. Conventional EMR is associated with a high risk of local recurrence (range, 2–35%) in such cases, especially when resections are not accomplished en bloc or the margins are not clear [7].
Endoscopic submucosal dissection (ESD) was developed for direct dissection along the submucosal layer using specialized devices, including an insulation-tipped diathermy knife (IT knife; Olympus Optical Co., Ltd, Tokyo, Japan) [8, 9]. The ESD procedure allows precise histologic assessment of the resected specimens and may prevent residual disease and local recurrence [4, 6, 7]. Preliminary studies have been published showing the advantage of ESD over conventional EMR for removing larger or ulcerated EGC lesions in an en bloc manner [5, 10, 11].
In a large consecutive series of EGCs treated by ESD, Oda et al. [12] documented that each parameter including upper and middle stomach location, tumor size greater than 21 mm, and positive ulcer findings was associated with piecemeal resection, affecting ESD curability. In another series, EGCs with ulceration or larger than 21 mm prevented their complete removal [5]. However, these studies used only univariate analysis, whereas multivariate analysis is needed to evaluate fully the impact of the factors on curability of ESD. In addition, the effect that combinations of factors have on the curative resection rates needs to be considered.
The current study aimed to assess the curability of ESD for the treatment of EGC using logistic regression analysis, with special reference to tumor size, tumor location, and ulcer findings.
Patients and methods
Patients
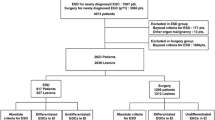
A total of 601 EGCs in 559 consecutive patients were treated by ESD at the hospitals of the Nagasaki University School of Medicine from June 2003 to May 2008. The study excluded patients for whom clinicopathologic data were not fully available. In these cases, curability could not be evaluated due to difficulties in histopathologic assessment resulting from the burn effect or insufficient reconstruction of the piecemeal fragments.
The patients were enrolled according to the criteria proposed by Gotoda et al. [4, 13], which required well and moderately differentiated gastric cancers (tubular adenocarcinoma and papillary adenocarcinoma) with no lymphatic–vascular involvement and thus a nominal risk of lymph node metastasis. These cancers included mucosal cancer without ulcer findings irrespective of tumor size, mucosal cancer with ulcer findings 3 cm in diameter or smaller, and minute submucosal invasive cancer 3 cm in size or smaller (<500 μm from the muscularis mucosae) (sm1).
Patients with EGCs that did not fall into one of these categories were excluded from the study and urged to receive a gastrectomy with removal of lymph nodes. Written informed consent was obtained from all the patients before ESD.
ESD
First, EGCs were identified and demarcated using white-light endoscopy and chromoendoscopy with indigo-carmine solution. Marking around the lesions then was performed with spotty cautery using a needleknife. Next, glyceol (10% glycerol and 5% fructose; Chugai Pharmaceutical Co, Tokyo, Japan) was injected into the submucosal layer to lift the mucosa. A circumferential mucosal incision was made around the lesion using the IT knife. Submucosal dissection was performed for complete removal of the lesion using the IT knife and the hook knife (Olympus). High-frequency generators (ICC200 or VIO 300D; ERBE Elektromedizin GmbH, Tübingen, Germany) were used during marking, incision of the gastric mucosa, and exfoliation of the gastric submucosa.
Procedure-related bleeding after ESD was defined as bleeding that required transfusion or surgical intervention or bleeding that caused the hemoglobin level to fall by 2 g/dl [12]. Perforation was diagnosed endoscopically or by the presence of free air on an abdominal plain radiograph or computed tomogram (CT).
Clinicopathologic evaluation
The EGC lesions were classified according to their main location in the upper, middle, or lower thirds of the stomach. They also were classified in terms of their location in the anterior wall, posterior wall, major curvature, or minor curvature. The macroscopic type of EGC was divided into the elevated type and the flat/depressed type. Moreover, the predominant macroscopic appearance was classified as I, IIa, IIb, IIc, or III in accordance with the Japanese Classification of Gastric Carcinoma.
The excised specimens were sectioned perpendicularly at 2-mm intervals and classified histologically as differentiated adenocarcinoma (well or moderately differentiated adenocarcinoma or papillary adenocarcinoma) or undifferentiated adenocarcinoma (poorly differentiated adenocarcinoma or signet-ring-cell carcinoma). The tumor size, depth of invasion, presence of ulcerative changes, lymphatic and vascular involvement, and tumor involvement to the lateral and vertical margins were assessed.
En bloc resection refers to a resection in one piece [12]. When the lesion had to be removed in multiple segments, the piecemeal-resected specimens were reconstructed as completely as possible.
The ESD was classified as either curative or noncurative [12, 14]. Resections were deemed curative when the removal was achieved with tumor-free lateral and vertical margins and there was no submucosal invasion deeper than 500 μm from the muscularis mucosae and no lymphatic and vascular involvement. Noncurative resection was defined as one that did not meet the curative criteria or one in which compartments of undifferentiated carcinoma were found.
Statistical analysis
The significance of differences in patient characteristics and clinicopathologic features was determined using Fisher’s exact test, the chi-square test, the Mann–Whitney U test, or the Student’s t-test, as appropriate. Factors associated with curability of ESD were analyzed using logistic regression analysis. Odds ratios (OR) together with 95% confidence intervals (95% CI) were calculated to estimate the relative risk of noncurative resection and their associations with various parameters.
Results
Of the 601 EGCs treated by ESD, 23 lesions diagnosed as having undifferentiated cancer based on the resected specimens were excluded from the study. An additional 49 lesions were excluded because of detected lymphatic or vascular invasion. The study also excluded 19 EGCs with massive submucosal invasion, 6 with minute submucosal invasion exceeding 30 mm in size, and 9 with intramucosal cancer and ulcer findings exceeding 30 mm in size.
Thus, 468 patients with a total of 495 EGC lesions were enrolled in the study. These patients had median age of 72 years (mean, 71 years; range, 38–92 years), and a male/female ratio of 2.57:1 (337:131).
By definition, 476 (96%) of the 495 lesions were resected curatively. Table 1 shows the clinicopathologic characteristics of the 495 EGCs according to the curability of ESD. Significant differences in age, the presence of ulcer findings, and the depth of tumor invasion were found between the curative and the noncurative resection groups (p < 0.05 for each). En bloc resection was achieved for 474 (95.8%) of the 495 lesions. The one-piece resection rate was significantly higher in the curative resection group (96.4%, 459/476) than in the noncurative resection group (78.9%, 15/19; p < 0.01).
Table 2 summarizes the association between the clinicopathologic parameters and the curability of ESD. Univariate analysis showed that older age, positive ulcer findings, minimal invasion, and piecemeal resection were significant contributors to noncurative resection. According to multivariate regression analysis, age, resectability, and the presence of ulcer findings had a significant impact on ESD curability.
Next, we analyzed the curability of ESD when the study factors (tumor size and location and ulcer findings) were combined in the same patient (Table 3). The larger EGCs (>30 mm) located in the upper third of the stomach were at significantly higher risk of noncurative resection (Table 3a). The ulcerative tumors located in the upper and middle portions also were associated with a significantly higher risk of noncurative resection (Table 3b and c).
Procedure-related bleeding was seen in seven patients (1.4%). All hemorrhagic episodes were successfully treated by endoscopic clipping or coagulation. Perforations related to ESD occurred in 21 patients (4.2%) and also could be managed by conservative medical treatment after endoscopic closure with clipping. Procedure-related bleeding was not associated with any clinicopathologic characteristics. Among the various clinicopathologic parameters, univariate analysis showed that upper location and tumor size had an impact on ESD-related perforation. Lesions in the upper third (odds ratio [OR], 13.35; 95% confidence interval [95% CI], 2.81–63.50; p < 0.01) and EGCs larger than 30 mm (OR, 3.34; 95% CI, 1.32–8.49; p < 0.05) were the significant risk factors for ESD-related perforation. On the other hand, upper location of the tumors was the sole contributor to procedure-related perforation according to multivariate analysis (OR, 14.67; 95% CI, 2.74–78.60; p < 0.01).
Next, we analyzed the risk of procedure-related perforation when the study factors (tumor size and location and ulcer findings) were combined (Table 4). As shown in Table 4a, EGCs larger than 30 mm or smaller than 20 mm in the upper third of the stomach were at significantly higher risk of perforation. Ulcerative EGCs in the upper third also were associated with a significantly higher risk of perforation (Table 4b).
Discussion
Despite the increasing use of ESD for EGC, the factors related to curability of ESD have not been analyzed in detail. En bloc resection of ESD provides much higher curative resection rates than piecemeal resection [12], as confirmed in the current study. In addition, ESD permits precise histopathologic examination of curability to guide further management and to stratify a patient’s risk for the development of metastases, offering successful outcomes after ESD [4, 7].
Logistic regression analysis was used to assess the impact of various clinicopathologic parameters on the curability of ESD. Besides piecemeal resection, older age, positive ulcer findings, and minute submucosal invasion were significant risk factors for noncurative resection according to univariate analysis.
Multivariate analysis showed that the absence of ulcer findings was the sole contributor to curative ESD. Oda et al. [12] documented that EGCs located in the upper and middle stomach, those larger than 21 mm, and those with ulcer findings were associated with piecemeal resection, thus affecting ESD curability. Oka et al. also showed that ulceration prevented complete removal of EGCs, notably with lesions larger than 21 mm [5]. A similar tendency was seen in EGC patients treated with ESD for recurrent EGC after previous EMR [14]. Thus, it is of clinical importance to assess such risk factors, particularly ulcer findings, to predict ESD curability.
The current study analyzed curability when tumor location and size were combined with ulcer findings in the same patient. The findings showed that EGCs larger than 30 mm located in the upper third and ulcerative tumors located in the upper and middle stomach were at significantly greater risk of noncurative resection. The curative resection rates for such lesions were rather low, ranging from 83.3% to 88.9%. These intractable lesions that prevented successful ESD also were associated with ESD-related perforation, with the odds ratios varying from 11.27 to 64.55. Higher levels of endoscopic skill and experience are required for such high-risk EGCs.
By combining the risk factors, clinicians should be able to predict the curability of ESD and the complications before performing the procedure. Less invasive surgery under laparoscopic assistance may be chosen in certain cases considering the high risks of noncurative resection and procedure-related perforation with the use of ESD.
The ESD procedure still had a relatively high procedure-related bleeding rate (1.4%) in the current study. Oda et al. [12] reported that post-ESD bleeding was seen in 6% of cases, significantly associated with upper third location. However, procedure-related bleeding was not associated with any clinicopathologic characteristics in the current series.
The limitation of the current study was its relatively small sample size, especially with respect to EGCs with ulcer findings. Obviously, further confirmation with a larger cohort is required. However, larger or ulcerative EGCs in the upper stomach can be carefully treated as long as the patients are given sufficient information with respect to the risk of incomplete removal and the higher incidence of related complications before they give their informed consent.
In conclusion, EGCs with ulcer findings were at higher risk of noncurative resection. When the factors of positive ulcer findings are combined with larger size and upper location of the tumors, the risks of noncurative resection and perforation increased. Therefore, only skilled and experienced endoscopists should treat such risky EGCs. The findings of the current study also may be useful information for education and training in the use of ESD for EGCs.
References
Sano T, Kobori O, Muto T (1992) Lymph node metastasis from early gastric cancer: endoscopic resection of tumour. Br J Surg 79:241–244
Shimizu S, Tada M, Kawai K (1995) Early gastric cancer: its surveillance and natural course. Endoscopy 27:27–31
Rembacken BJ, Gotoda T, Fujii T, Axon AT (2001) Endoscopic mucosal resection. Endoscopy 33:709–718
Soetikno R, Kaltenbach T, Yeh R, Gotoda T (2005) Endoscopic mucosal resection for early cancers of the upper gastrointestinal tract. J Clin Oncol 23:4490–4498
Oka S, Tanaka S, Kaneko I, Mouri R, Hirata M, Kanao H, Kawamura T, Yoshida S, Yoshihara M, Chayama K (2006) Endoscopic submucosal dissection for residual/local recurrence of early gastric cancer after endoscopic mucosal resection. Endoscopy 38:996–1000
Takenaka R, Kawahara Y, Okada H, Hori K, Inoue M, Kawano S, Tanioka D, Tsuzuki T, Yagi S, Kato J, Uemura M, Ohara N, Yoshino T, Imagawa A, Fujiki S, Takata R, Yamamoto K (2008) Risk factors associated with local recurrence of early gastric cancers after endoscopic submucosal dissection. Gastrointest Endosc 68:887–894
Gotoda T (2007) Endoscopic resection of early gastric cancer. Gastric Cancer 10:1–11
Gotoda T, Kondo H, Ono H, Saito Y, Yamaguchi H, Saito D, Yokota T (1999) A new endoscopic mucosal resection procedure using an insulation-tipped electrosurgical knife for rectal flat lesions: report of two cases. Gastrointest Endosc 50:560–563
Ono H, Kondo H, Gotoda T, Shirao K, Yamaguchi H, Saito D, Hosokawa K, Shimoda T, Yoshida S (2001) Endoscopic mucosal resection for treatment of early gastric cancer. Gut 48:225–229
Oka S, Tanaka S, Kaneko I, Mouri R, Hirata M, Kawamura T, Yoshihara M, Chayama K (2006) Advantage of endoscopic submucosal dissection compared with EMR for early gastric cancer. Gastrointest Endosc 64:877–883
Takeuchi Y, Uedo N, Iishi H, Yamamoto S, Yamamoto S, Yamada T, Higashino K, Ishihara R, Tatsuta M, Ishiguro S (2007) Endoscopic submucosal dissection with insulated-tip knife for large mucosal early gastric cancer: a feasibility study (with videos). Gastrointest Endosc 66:186–193
Oda I, Gotoda T, Hamanaka H, Eguchi T, Saito Y, Matsuda T, Bhandari P, Emura F, Saito D, Ono H (2005) Endoscopic submucosal dissection for early gastric cancer: technical feasibility, operation time, and complications from a large consecutive series. Dig Endosc 17:54–58
Gotoda T, Yanagisawa A, Sasako M, Ono H, Nakanishi Y, Shimoda T, Kato Y (2000) Incidence of lymph node metastasis from early gastric cancer: estimation with a large number of cases at two large centers. Gastric Cancer 3:219–225
Yokoi C, Gotoda T, Hamanaka H, Oda I (2006) Endoscopic submucosal dissection allows curative resection of locally recurrent early gastric cancer after prior endoscopic mucosal resection. Gastrointest Endosc 64:212–218
Author information
Authors and Affiliations
Corresponding author
Additional information
Ken Ohnita, Hajime Isomoto, and Naoyuki Yamaguchi equally contributed to this work.
Rights and permissions
About this article
Cite this article
Ohnita, K., Isomoto, H., Yamaguchi, N. et al. Factors related to the curability of early gastric cancer with endoscopic submucosal dissection. Surg Endosc 23, 2713–2719 (2009). https://doi.org/10.1007/s00464-009-0473-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-009-0473-8