
Abstract
Background
The standard treatment for clinical submucosal invasive (cT1b) early gastric cancer is gastrectomy. However, Japanese gastric cancer treatment guidelines list endoscopic submucosal dissection (ESD) as an option for treating limited early gastric cancer cases. ESD can be curative depending on the pathological characteristics of resected specimens. Thus, we aimed to clarify the benefits and disadvantages of preceding ESD for early gastric cancer.
Methods
We retrospectively analyzed patients who underwent ESD or curative gastrectomy for cT1b gastric cancer with differentiated adenocarcinoma 30 mm or less in diameter. Patients who underwent ESD irrespective of undergoing gastrectomy were assigned to the ESD group (n = 107), and those who underwent gastrectomy without undergoing ESD were assigned to the non-ESD group (n = 181). Clinicopathological characteristics were assessed, and the short-term and long-term outcomes of patients were compared.
Results
The criteria for curative resection were satisfied by 83 patients (28.8%), and preceding ESD did not affect the surgical outcomes of gastrectomy. Two patients (1.9%) who underwent ESD had an unscheduled total gastrectomy. The en bloc and complete resection rates of ESD were 99.0% and 84.1% respectively. Nine patients (8.4%) experienced intraprocedure perforation and postprocedure bleeding caused by ESD. Overall survival (hazard ratio 1.38; P = 0.302) and cause-specific survival (hazard ratio 0.96; P = 0.944) were comparable between groups.
Conclusions
The stomach was preserved in 28.8% of patients, and preceding ESD did not show obvious disadvantages. Therefore, diagnostic ESD should be considered as an initial treatment for limited cT1b gastric cancer cases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastric cancer is one of the major causes of cancer deaths worldwide [1]. Endoscopic submucosal dissection (ESD) is widely used to treat early gastric cancer showing a negligible risk of lymph node metastasis [2, 3], thus avoiding gastrectomy if the resection is deemed to be curative according to the Japanese gastric cancer treatment guidelines published by the Japanese Gastric Cancer Association (JGCA) [4, 5].
The JGCA guidelines also recommend treating patients in whom early gastric cancer confined to the mucosa (T1a) has been clinically diagnosed with either endoscopic resection or gastrectomy; however, gastrectomy is the only recommendation for tumors confined to the submucosa (T1b) [5]. The Japanese Gastroenterological Endoscopy Society has also developed guidelines detailing indications for ESD based on tumor-related characteristics established from clinical diagnosis. It also proposes recommendations for evaluating curability whereby ESD can be classified as either curative or noncurative on the basis of the pathological characteristics of the resected specimens [4].
The choice between endoscopic treatment and surgical treatment for cases of early gastric cancer is therefore considered during the pretreatment clinical diagnosis, and gastrectomy without ESD sometimes includes lesion resections that could have been considered for curative resection under the JGCA guidelines. Consequently, gastrectomy may be considered a dispensable and overzealous treatment if ESD can be performed as a successful initial therapy for these lesions.
The indications for ESD are expanded in cases assumed to have a low risk of lymph node metastasis [4]. Lesions in these cases can be considered for curative resection under the following circumstances: the pathological depth of invasion is T1b, lesions removed by en bloc resection have cancer-free margins, there is no lymphovascular infiltration, the diameter is less than 30 mm, the lesion tissue is predominantly differentiated, and it is classified as SM1 (submucosal invasion of 500 µm or less from the muscularis mucosae) [4, 6].
Despite these recommendations and guidelines, the short-term and long-term outcomes of ESD without gastrectomy for patients with early gastric cancer with submucosal invasion are still unclear [7,8,9]. Although the benefits of ESD as an initial treatment for cT1b gastric cancer include preservation of the stomach, possible risks include an increase in postoperative complications, the risk of upgrading from a partial gastrectomy to a total gastrectomy, complications directly caused by the ESD procedure, and recurrence of pathological T1b gastric cancer. In this study, we therefore evaluated the efficacy of ESD as an initial treatment for cT1b early gastric cancer. We investigated the frequency of cases in which the stomach was preserved if ESD was performed as an initial treatment. We also evaluated the shortcomings of preceding ESD as a treatment strategy.
Methods
Patients
Nine hundred thirty-nine patients who underwent ESD or curative gastrectomy for cT1b early gastric cancer between September 2002 and December 2012 at Shizuoka Cancer Center were identified from a prospectively maintained database. Patients were excluded if their lesions were not classified as adenocarcinoma (n = 14), they had other cancer (n = 121), or they had received chemotherapy (n = 1) before ESD or gastrectomy. Of the remaining 803 patients, only 288 fulfilled all of the relevant criteria at their pretreatment diagnosis and were included in the present study. The criteria were as follows: clinically negative lymph node metastasis (cN0), tumor diameter diagnosed by endoscopy of 30 mm or less, and differentiated adenocarcinoma diagnosed from a biopsy specimen. This study was approved by the Institutional Review Board of Shizuoka Cancer Center (approval number 27-J168-27-1).
Determination of preoperative staging
Pathological tumor depth, nodal status, and curability of surgery were assigned according to the Union for International Cancer Control TNM classification of malignant tumors [10]. Histological type was classified according to the JGCA classification of gastric carcinoma [11]. When the histological type was mixed in resected and biopsy specimens, the predominant type was adopted. Esophagogastroduodenoscopy and computed tomography scans were performed on all patients before treatment, and pretreatment histopathological diagnoses were derived from endoscopic biopsy specimens. From 2008, we used aggressive endoscopic ultrasonography (EUS) to determine the indications for ESD when clinical diagnosis of the tumor depth in early gastric cancer could not readily distinguish between T1a and T1b gastric cancer by conventional endoscopy. Patients scheduled to undergo gastrectomy also received an gastrointestinal X-ray.
Preoperative tumor depth classification was determined by the following criteria with a combination of conventional endoscopy with additional indigocarmine dye spraying, EUS, and gastrointestinal X-ray [12]. Computed tomography was not used for diagnosis of T1b gastric cancer, because it is known to be of limited value in T1 gastric cancer staging.
When type 0 cancer (superficial, flat tumors with or without minimal elevation or depression) was diagnosed, a case was classified as cT1. Even in early cancer types, tumor depth was considered deeper than cT2 (tumor invades the muscularis propria) if mucosal convergence was significant, a submucosal-tumor-like image was noted, or extensive submucosal tumor spreading was suspected. For elevated types, the depth was classified as cT1a if the cancers were pedunculated. In sessile elevated types, the classification was cT1a for tumors not larger than 3 cm and cT1b for tumors larger than 3 cm [12].
When gastrointestinal X-ray showed a deeper invasion of advanced cancer than that shown by endoscopy, the radiographic diagnosis took precedence. EUS was performed to assess the gastric wall on the basis of the standard five-layer sonographic structure. When EUS detected a change in the third layer, cT1b was defined. A multidisciplinary team including surgeons, endoscopists, medical oncologists, radiologists, and pathologists made the final decision regarding clinical stage of the gastric cancer.
Treatment of early gastric cancer
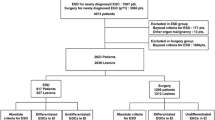
ESD or gastrectomy with lymph node dissection was generally performed according to the JGCA guidelines [5]. We proposed gastrectomy for patients with cT1b early gastric cancer, but provided ESD as a treatment option for patients who refused surgery, and for patients in whom cT1b gastric cancer had been clinically diagnosed that fulfilled the criteria of cN0, tumor diameter diagnosed by endoscopy of 30 mm or less, and differentiated adenocarcinoma diagnosed from a biopsy specimen. Of the 288 patients enrolled in this study, 107 underwent ESD irrespective of undergoing gastrectomy, and were assigned to the ESD group (Fig. 1). The remaining 181 patients underwent gastrectomy without ESD and were assigned to the non-ESD group.

Flowchart of enrolled patients undergoing surgery or endoscopic submucosal dissection (ESD) for cT1b early gastric cancer. This is based on criteria set out in the Japanese Gastric Cancer Association treatment guidelines. cDifferentiated differentiated adenocarcinoma diagnosed from a biopsy specimen, ≤c30 mm tumor diameter diagnosed by endoscopy of 30 mm or less
Endoscopically resected specimens were cut into 2-mm slices after fixation, and size, histological type, tumor depth, lymphatic and venous invasion, lateral and vertical margins, and ulceration were evaluated. ESD is considered curative when en bloc resection shows negative horizontal or vertical margins, there is no lymphovascular infiltration, and the lesion satisfies any of the following conditions: differentiated type assessed as pT1a and no ulceration; differentiated type assessed as pT1a, 30 mm or less in diameter, and ulceration; differentiated type assessed as pT1b (submucosal invasion 500 µm or less) and 30 mm or less in diameter; or undifferentiated type assessed as pT1a, 20 mm or less in diameter, and no ulceration [5]. Resections that did not satisfy any of the curative resection criteria were considered noncurative. Patients with noncurative resections were recommended for additional gastrectomy. However, patients who refused surgical treatment or had been judged as unsuitable for surgery because of poor general condition received follow-up only.
Patient characteristics and treatment outcomes in the ESD and non-ESD groups
Clinical and pathological characteristics before and after treatment and the short-term and long-term outcomes of ESD or gastrectomy were evaluated. Overall survival and cause-specific survival after initial treatment (ESD or gastrectomy) were investigated as long-term outcomes. Clinicopathological characteristics, operative procedure, and the short-term and long-term outcomes were compared between the ESD group and the non-ESD group. Data regarding operative procedures and short-term outcomes of gastrectomy were excluded for six patients who underwent gastrectomy at other hospitals.
Statistical analysis
All continuous variables are presented as the median, mean, range, and 25th and 75th percentiles. Statistical analyses were performed with Fisher’s exact test, the t test, and the Mann–Whitney test. Survival data were analyzed by the Kaplan–Meier method, and the log-rank test was used to compare the groups. A two-tailed P value less than 0.05 was considered significant. All statistical analyses were conducted with R version 3.2.0.
Results
A flowchart illustrating the treatment modalities for the 288 patients involved in this study is presented in Fig. 1. Eighty-three patients (28.8%) satisfied the JGCA’s curative criteria for endoscopic resection. Of the 288 patients, 107 patients (37.2%) initially underwent ESD, and of these, 46 patients subsequently underwent gastrectomy. The total number of patients receiving gastrectomy was 227 (78.8%). Resections were judged as noncurative in 73 patients, although 27 of these patients (9.4%) did not undergo a subsequent gastrectomy. All gastrectomy procedures, including additional surgery, were curative (R0 surgery).
Clinicopathological characteristics
Table 1 lists the clinicopathological characteristics of all patients. EUS was performed in 103 patients (35.8%). The patients were significantly younger (P < 0.001) and the tumor diameter diagnosed by endoscopy was significantly larger (P < 0.001) in the non-ESD group. There was no difference in comorbidity. Pathological tumor size was also significantly larger (P = 0.004) in the non-ESD group. Adenocarcinomas diagnosed as differentiated type before treatment were diagnosed as undifferentiated type following examination of resected specimens in 27 patients. The prevalence of undifferentiated-type adenocarcinomas was significantly greater in the non-ESD group (P = 0.005). The pathological depth of tumor invasion was T1a in 93 patients (32.3%), T1b in 167 patients (58.0%), T2 in 21 patients (7.3%), T3 in six patients (2.1%), and T4 in one patient (0.3%). There was no significant difference in curability rate between the 49 patients in the non-ESD group and the 34 patients in the ESD group who had curative resections. There was a significant difference between the groups in clinical tumor location, but no difference was detected in clinical tumor size after comparison of tumor factors between patients who did and did not satisfy the JGCA’s curative criteria for endoscopic resection (Table S1).
Short-term outcomes
The surgical procedures and the short-term outcomes of gastrectomy are shown in Table 2. Laparotomy and D2 lymph node dissection were significantly more frequent in the ESD group. There were no significant differences in operation time, blood loss, number of harvested lymph nodes, or postoperative complications between the groups. Therefore, the adverse effects of ESD before surgery appeared to be limited.
Treatment for two patients (1.9%) in the ESD group was revised to a total gastrectomy, even though this was not the original intention. In the first patient, the proximal distance of the lesion was initially estimated to be 5 cm from the cardia. However, an artificial ulcer caused by ESD resulted in a fibrotic contraction, and the proximal margin could not be preserved; therefore, the scheduled distal gastrectomy was changed to a total gastrectomy. The second patient needed to undergo a total gastrectomy with D2 lymphadenectomy because the pathological depth of the tumor near the cardia was suspected to be T2.
The median procedure time of ESD was 50 min for the 107 patients who underwent ESD. Positive lateral and vertical margins were detected in 6 patients (5.6%) and 14 patients (13.1%) respectively by pathological evaluation of endoscopically resected specimens. The en bloc and complete resection rates were 99.0% and 84.1% respectively. Curative resection was achieved in 34 patients (31.8%). Intraprocedure perforation and postprocedure bleeding occurred in nine patients (8.4%); however, urgent surgery was not needed.
Long-term outcomes
The median follow-up period was 60.6 months in the non- ESD group and 60.8 months in the ESD group. Gastric cancer recurred in 15 patients (5.2%), and 42 patients (14.6%) died during the study period (Table 3). The patterns of recurrence were hematogenous (n = 7), locoregional (n = 4), peritoneal (n = 3), and distant lymph node (n = 1) recurrence. Twelve patients (4.2%) died of gastric cancer. Although the mortality rate due to gastric cancer was similar in each treatment group, the mortality rate due to other diseases was higher in the ESD group. Twelve patients died of gastric cancer. Among those patients in whom pathological T1 gastric cancer had been diagnosed, there were five deaths in the non-ESD group (n = 156) and four in the ESD group (n = 104), whereas in patients with pathological T2 or higher stage gastric cancer, there were three deaths in the non-ESD group (n = 25) and none in the ESD group (n = 3). Figure 2 shows that there was no significant difference in overall survival between the groups [hazard ratio (HR) 1.38; 95% condidence interval (CI) 0.75–2.54; P = 0.302]. In multivariate analysis, ESD was not significantly associated with overall survival (HR 0.86; 95% CI 0.30–2.44; P = 0.772) (Table 4). Figure 3 shows that there was no significant difference in cause-specific survival between the groups (HR 0.96; 95% CI 0.28–3.28; P = 0.944).

Overall survival of the endoscopic submucosal dissection (ESD) group and the non-ESD group (hazard ratio 1.38; 95% confidence interval 0.75–2.54; P = 0.302)

Cause-specific survival of the endoscopic submucosal dissection (ESD) group and the non-ESD group (hazard ratio 0.96; 95% confidence interval 0.28–3.28; P = 0.944)
Discussion
The present study revealed that 28.8% of patients in whom cT1b early gastric cancer had been diagnosed who fulfilled our criteria for curative endoscopic resection could avoid gastrectomy. The potential benefit of preserving the stomach may make ESD a valid initial treatment strategy for selected patients, although ESD might still be unnecessary for some patients. The number of unnecessary ESD procedures undertaken becomes unacceptable if ESD is performed as an initial treatment for all cT1b gastric cancer patients. From these results, this study showed that restricting this treatment to patients with tumors fulfilling strict criteria may reduce the number of unnecessary ESD procedures by approximately 70%.
Preoperative diagnoses are not always accurate. There are usually discrepancies between preoperative and postoperative tumor-size measurements, with tumor size often underestimated [13,14,15]. We limited the preoperative tumor size to less than 30 mm in diameter to satisfy the JCGA’s curative resection criteria. As with other studies, we found that the estimated preoperative tumor size was smaller than the pathological size, indicating that it should be rare for cases excluded from receiving ESD to have tumors that actually meet the size criteria for curative resection. Endoscopic biopsy specimens do not always represent the most dominant histological type; therefore, preoperative histopathological diagnoses are not always accurate [16, 17]. Only a low number of patients in this study had their preoperative tumor diagnosis changed from differentiated type to undifferentiated type after resection, suggesting that our criteria efficiently selected a group of patients who could avoid gastrectomy. In contrast, it is difficult to determine a clinically precise depth of invasion diagnosis before treatment [18]. Our pretreatment diagnoses for cT1b early gastric cancer that was cN0, had a tumor diameter diagnosed by endoscopy of 30 mm or less, and was differentiated adenocarcinoma diagnosed from a biopsy specimen were 58.0% accurate, as determined by the pathological T1b results. A pathological depth of invasion of T1a was seen in 32.3% of patients, which indicated candidacy for curative resection.
The short-term outcomes of gastrectomy were equal between the ESD group and the non-ESD group, with no significant differences recorded in operation time, blood loss, or postoperative complication rate. A high prevalence of D2 lymphadenectomy was recorded because we used this treatment strategy for all cases with positive vertical margins even though the patients had early gastric cancer. We reported previously that it is rare for preceding ESD to necessitate alterations in gastric resection [19]. Forced conversion to total gastrectomy due to the effects of preceding ESD is a potential risk for patients, and this occurred in only one patient in the present study. We also have safety concerns about worsening short-term outcomes of ESD because cT1b early gastric cancer requires deeper resection than cT1a early gastric cancer [20]. Nevertheless, our complication and procedure time outcomes were comparable with T1a early gastric cancer outcomes reported in previous studies [21].
The mortality rate due to gastric cancer was equal and satisfactory in the ESD group and the non-ESD group. We focused on patients in whom with pathological T1 gastric cancer had been diagnosed, and investigated the rate of gastric cancer death, because the pathological stage of gastric cancer in the non-ESD group was more advanced. The rate of gastric cancer death among pathological T1 gastric cancer cases was comparable between the groups. Non-gastric-cancer deaths were frequent in the ESD group, which we attributed to the overall older age of the ESD group. The lack of significant differences in the overall survival and the cause-specific survival between the two groups also supports the view that the risk of recurrence is not elevated by a preceding ESD. Suzuki et al. [20] reported that ESD was an ineffective treatment for patients with operable cT1b early gastric cancer, because their 5-year cause-specific survival rate of 91.8% was lower than the survival rate of 96.7% reported in another study. However, they did not compare the patients directly, and only 64.7% of their patients with noncurative resection underwent additional gastrectomy. On the basis of these results, the ineffectiveness of ESD has not been shown.
Recently, the indications for ESD have expanded, although there is no convincing evidence for equivalent long-term outcomes between ESD and gastrectomy [4, 22]. When ESD is performed on the basis of the expanded indications, the frequency of noncurative resections increases. The efficacy of additional gastrectomy after noncurative resection has been proven [8, 23, 24], but some patients refuse to undergo additional surgery, confirming the importance of explaining to all patients that additional gastrectomy is crucial if the outcome of initial ESD therapy is considered noncurative.
Our study has strength because it includes all patients with cT1b gastric cancer undergoing ESD alone, gastrectomy alone, or both ESD and gastrectomy. Moreover, it includes both curative and noncurative resections. Previous studies have focused on a narrower range of patients with T1b early gastric cancer [8, 20, 24]. We also included patients who refused additional surgery or had been judged as unsuitable for surgery despite undergoing a noncurative resection. Consequently, these results reflect actual clinical practice more precisely than other studies. Our study also has limitations. First, this study is retrospective and was performed at a single institution. Second, there is a selection bias between the groups in that pathological tumor depth in the non-ESD group was greater than that in the ESD group. Therefore, the incomplete resection rate and complication rate of ESD, and the number of gastric cancer deaths, might have increased if ESD was performed before gastrectomy in the non-ESD group. Third, because the study focused on early gastric cancer, resulting in few cases of recurrence or death, its statistical power to investigate long-term survival is low.
Conclusion
It is possible that the stomach can be preserved in approximately 30% of patients in whom cT1b early gastric cancer has been diagnosed who fulfill all of the following criteria: cN0, tumor diameter diagnosed by endoscopy of 30 mm or less, and differentiated adenocarcinoma diagnosed from a biopsy specimen. Adverse effects of ESD as an initial treatment before gastrectomy were insignificant, and the procedure did not result in increased complications. Performing ESD before gastrectomy did not elevate the risk of recurrence or death from gastric cancer compared with performing gastrectomy alone. Therefore, diagnostic ESD should be considered as an initial treatment for cT1b early gastric cancer patients who fulfill the criteria of cN0, tumor diameter diagnosed by endoscopy of 30 mm or less, and differentiated adenocarcinoma diagnosed from a biopsy specimen.
References
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–86.
Ono H, Kondo H, Gotoda T, Shirao K, Yamaguchi H, Saito D, et al. Endoscopic mucosal resection for treatment of early gastric cancer. Gut. 2001;48:225–9.
Gotoda T. Endoscopic resection of early gastric cancer. Gastric Cancer. 2007;10:1–11.
Ono H, Yao K, Fujishiro M, Oda I, Nimura S, Yahagi N, et al. Guidelines for endoscopic submucosal dissection and endoscopic mucosal resection for early gastric cancer. Dig Endosc. 2016;28:3–15.
Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer. 2017;20:1–19.
Gotoda T, Yanagisawa A, Sasako M, Ono H, Nakanishi Y, Shimoda T, et al. Incidence of lymph node metastasis from early gastric cancer: estimation with a large number of cases at two large centers. Gastric Cancer. 2000;3:219–25.
Choi J, Jeon S, Cho K, Park K, Park C, Chung Y, et al. Non-curative endoscopic resection does not always lead to grave outcomes in submucosal invasive early gastric cancer. Surg Endosc. 2015;29:1842–9.
Kim ER, Lee H, Min BH, Lee JH, Rhee PL, Kim JJ, et al. Effect of rescue surgery after non-curative endoscopic resection of early gastric cancer. Br J Surg. 2015;102:1394–401.
Kakushima N, Hagiwara T, Tanaka M, Sawai H, Kawata N, Takizawa K, et al. Endoscopic submucosal dissection for early gastric cancer in cases preoperatively contraindicated for endoscopic treatment. United Eur Gastroenterol J. 2013;1:453–60.
Sobin LH, Gospodarowicz MK, Wittekind C, editors. TNM classification of malignant tumours. 7th ed. New York: Wiley-Blackwell; 2010. p. 310.
Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011;14:101–12.
Bando E, Makuuchi R, Tokunaga M, Tanizawa Y, Kawamura T, Terashima M. Impact of clinical tumor–node–metastasis staging on survival in gastric carcinoma patients receiving surgery. Gastric Cancer. 2017;20:448–56.
Choi J, Kim SG, Im JP, Kim JS, Jung HC. Endoscopic estimation of tumor size in early gastric cancer. Dig Dis Sci. 2013;58:2329–36.
Shim C, Song M, Kang D, Chung H, Park J, Lee H, et al. Size discrepancy between endoscopic size and pathologic size is not negligible in endoscopic resection for early gastric cancer. Surg Endosc. 2014;28:2199–207.
Kim JM, Sohn JH, Cho MY, Kim WH, Chang HK, Jung ES, et al. Pre- and post-ESD discrepancies in clinicopathologic criteria in early gastric cancer: the NECA-Korea ESD for Early Gastric Cancer Prospective Study (N-Keep). Gastric Cancer. 2016;19:1104–13.
Takao M, Kakushima N, Takizawa K, Tanaka M, Yamaguchi Y, Matsubayashi H, et al. Discrepancies in histologic diagnoses of early gastric cancer between biopsy and endoscopic mucosal resection specimens. Gastric Cancer. 2012;15:91–6.
Min B-H, Kang K, Lee J, Kim E, Min Y, Rhee P-L, et al. Endoscopic resection for undifferentiated early gastric cancer: focusing on histologic discrepancies between forceps biopsy-based and endoscopic resection specimen-based diagnosis. Dig Dis Sci. 2014;59:2536–43.
Sano T, Okuyama Y, Kobori O, Shimizu T, Morioka Y. Early gastric cancer. Endoscopic diagnosis of depth of invasion. Dig Dis Sci. 1990;35:1340–4.
Kawata N, Kakushima N, Tokunaga M, Tanaka M, Sawai H, Takizawa K, et al. Influence of endoscopic submucosal dissection on additional gastric resections. Gastric Cancer. 2015;18:339–45.
Suzuki H, Oda I, Nonaka S, Yoshinaga S, Saito Y. Is endoscopic submucosal dissection an effective treatment for operable patients with clinical submucosal invasive early gastric cancer? Endoscopy. 2013;45:93–7.
Oda I, Gotoda T, Hamanaka H, Eguchi T, Saito Y, Matsuda T, et al. Endoscopic submucosal dissection for early gastric cancer: technical feasibility, operation time and complication from large consecutive series. Dig Endosc. 2005;17:54–8.
Kang MS, Hong SJ, Kim DY, Han JP, Choi MH, Kim HK, et al. Long-term outcome after endoscopic submucosal dissection for early gastric cancer: focusing on a group beyond the expanded indication. J Dig Dis. 2015;16:7–13.
Katsube T, Murayama M, Yamaguchi K, Usuda A, Shimazaki A, Asaka S, et al. Additional surgery after non-curative resection of ESD for early gastric cancer. Anticancer Res. 2015;35:2969–74.
Hoteya S, Iizuka T, Kikuchi D, Ogawa O, Mitani T, Matsui A, et al. Clinicopathological outcomes of patients with early gastric cancer after non-curative endoscopic submucosal dissection. Digestion. 2016;93:53–8.
Acknowledgement
This research was supported in part by the Practical Research for Innovative Cancer Control of the Japan Agency for Medical Research and Development (15ck0106043h0002).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standards
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Fujiya, K., Takizawa, K., Tokunaga, M. et al. The value of diagnostic endoscopic submucosal dissection for patients with clinical submucosal invasive early gastric cancer. Gastric Cancer 21, 124–132 (2018). https://doi.org/10.1007/s10120-017-0724-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10120-017-0724-7