
Abstract
Introduction
Robotic technology has been postulated to improve performance in advanced surgical skills. We utilized a novel computerized assessment system to objectively describe the technical enhancement in task performance comparing robotic and laparoscopic instrumentation.
Methods and procedures
Advanced laparoscopic surgeons (2–10 yrs experience) performed three unique task modules using laparoscopic and Telerobotic surgical instrumentation (Intuitive Surgical, Sunnyvale, CA). Performance was evaluated using a computerized assessment system (ProMIS, Dublin, Ireland) and results were recorded as time (s), path (mm) and precision. Each surgeon had an initial training session followed by two testing sessions for each module. A paired Student’s t-test was used to analyze the data.
Results
Ten surgeons completed the study. 8/10 surgeons had significant technical enhancement utilizing robotic technology.
Conclusions
The ProMIS computerized assessment system can be modified to objectively obtain task performance data with robotic instrumentation. All the tasks were performed faster and with more precision using the robotic technology than standard laparoscopy.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Modern laparoscopic surgery came into being with the development of the miniature computer chip television camera and high-intensity light sources, which improved the visualization of the surgical field through enhanced illumination and superior resolution [1]. As the advantages of laparoscopic surgery were realized, it became the preferred operative approach for many procedures. However, as with any new approach there are limitations that become apparent over a course of time and experience. Laparoscopic surgery was not an exception to this rule. Ballantyne [2] described some of the pitfalls of laparoscopic surgery, including an unstable camera platform, the loss of degrees of freedom, two-dimensional imaging, and poor ergonomics for the surgeon.
Standard laparoscopic surgery requires the use of long rigid instruments, which leads to a reduction in dexterity. The increased length also amplifies the small inherent tremors of the hand, making it difficult to perform complex tasks such as suturing and knot tying [3]. Also the surgeon’s movements are reversed by the fulcrum effect of the abdominal wall. Open surgery allows the surgeon to have seven degrees of freedom whereas, with laparoscopic surgery, the surgeon is reduced to four degrees of freedom. Robotic technology can play a crucial role in overcoming some of these limitations . Robotic assisted surgery enables the operator to perform the operation with greater accuracy, improved camera stability, improved visualization, and greater dexterity than conventional laparoscopic surgery.
We know from past studies that laparoscopic skills enhancement can occur through a structured skills acquisition course, which can help with the development of dexterity and improve task performance in residents and fellows [4]. Although the robotic systems were designed to overcome some of the obstacles of standard laparoscopy, the operator still needs to acquire a different skill set. Previous validation studies of the laparoscopic skills set have utilized box trainers and the surgical simulator systems such as ProMIS [10]. However, objective validation of the robotic skills assessment with such simulators has not been well established. This is the next logical step in the surgical education of future generations.
At present, surgeons utilizing the robot are accomplished advanced laparoscopic surgeons and their experience helps shorten the learning curve. Therefore, to shorten the learning curve for the future generations of surgeons, it is necessary for the robotic training to begin outside the operating room. The use of advanced technology, such as virtual environments and computer-based simulators in surgery training programs is gaining popularity. Surgery programs are incorporating a curriculum for the training of their residents in laparoscopic skills. For basic laparoscopic skills, the laparoscopic trainers and the virtual-reality/computer-based models are good. However, for advanced laparoscopic skills the use of robotic systems might prove to be advantageous especially in conjunction with virtual-reality simulators.
Hypothesis
Complex laparoscopic skills are more efficiently acquired with a robotic system when compared to skill acquisition using standard laparoscopic instrumentation.
Methods
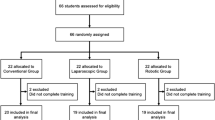
Ten surgeons with advanced laparoscopic skills performed three open module tasks using both the simulator (ProMIS, Haptica, Dublin, Ireland) and the robotic system (Da Vinci Surgical System, Intuitive Surgical Inc., Sunnyvale, CA). Half the surgeons performed the laparoscopic arm of the study first followed by the robotic arm, while the other half performed the tasks vice versa. Both arms of the study used the simulator for recording the test parameters. The positions of the instruments captured on the system were recorded, segmented and analyzed according to three parameters. This was done on real tasks and on virtual tasks. The three parameters measured by the ProMIS simulator: elapsed time, length, and precision.
The time was recorded in seconds and the path in millimeters. ProMIS defines precision as the degree of smoothness demonstrated while performing the tasks, and is based on the velocity of the instruments. therefore, this value is a measure of the steadiness with which the surgeon perfoms the task. When using two instruments, the reported metrics from both instruments were combined. Elapsed time was common between them. The path length was added. The number of movements was added.
The participants performed all three of the modules on both the ProMIS simulator and the Da Vinci robotic system. Each participant had the opportunity to do a training session followed by two testing sessions. All sessions were performed consecutively. Analysis of these tasks was performed to ascertain the usefulness of the robotic instrumentation in teaching of advanced laparoscopic skills in surgery training/fellowship programs. Data was analyzed using a Student’s paired t-test.
Participants
Ten surgeons, all with advanced laparoscopic experience (2–10 years).
Module 1: Suturing/knot tying (Figure 1)
The surgeon completed intracorporeal suturing and knot tying using a 3–0 silk suture on a SH needle. The module was already set up with the needle and suture in place. The artificial skin simulated a tear. The task began when the surgeon had loaded the needle on the needle driver. The needle had to be perpendicular to the skin and pass through both the edges. After this, a surgeon’s knot had to be performed, followed by three more throws in a square knot fashion, leading to the second part of this exercise. The surgeon had to connect ten 1 mm wide dots spaced 3–5 mm apart on the artificial skin in a running suture manner to conclude the task. The instruments used in the simulator included a needle driver in the dominant hand and a Maryland grasper in the other hand. Whereas, in the robot, the Cartier along with the Debakey grasper was used in the dominant hand. The Da Vinci requires the use of the 30° camera as well. Once the task has concluded the simulator tabulated the data.

Suturing and knot typing (module 1).
Module 2: Suture passing (Figure 2)
The surgeon passed a curved needle and suture through six keyholes using Cartier and Debakey graspers. The suture again was 3–0 silk on an SH needle, passed in a clockwise manner. This required the surgeon to use both hands in concert to accomplish the task. The simulator calculated the time, path and smoothness of the movements.

Suture passing (module 2).
Module 3: Object positioning (Figure 3)
The surgeon had five bins in this module, each with a different height, width and depth. The largest bin contained eight beads measuring 0.5 x 1.0 cm, which had to be placed in various other bins. This had to be done using both hands equally, with four beads per hand. This was done using the Cardiere in both hands for the robot and endograspers for the simulator. The computer then tabulated the data.

Object positioning (module 3).

Da Vinci robot docked with the ProMIS surgical simulator.
Results
Ten surgeons completed the study. The group consisted of eight staff surgeons with minimally invasive surgery training and two laparoscopic fellows. The group had a median of 6 yrs postgraduate training and 5 yrs of laparoscopic training. All the data is presented as laparoscopic versus robotic instrumentation.
Objective assessment of the data is presented in Table 1.
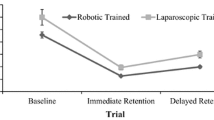
All the results were statistically significant with p values of either p < 0.009 or p < 0.001. All the surgeons showed significant improvement in the test parameters over the three consecutive sessions. This was true for both the laparoscopic and the robotics arms of the study taken separately. However, when the two arms of the study were compared, 8/10 surgeons had significant technical enhancement utilizing robotic instrumentation. In module 1, the median improvement was 15–50%; in module 2, it was 35–68%; and in module 3, it was 23–40%. All the improvement in time, path and precision were in favor of robotic instrumentation for all the tasks.
Discussion
Minimally invasive surgery is based on the ability to perform small and precise movements to manipulate tissue in a confined space [4]. In order to accomplish this task, the surgeon has to rely on the proper instrumentation coupled with the degrees of freedom. In laparoscopic surgery this is made difficult by inadequate instrument design and the loss of dexterity inherent to laparoscopic instrumentation. Surgical robotic systems offer advantages that may help alleviate these problems. However, to date, few studies have shown the advantages of robotic instrumentation over standard laparoscopy [5]. Recent studies have commented on both sides of this issue. Melvin et al. [6] looked at antireflux surgery and found there to be no advantage offered by the use of a robotic surgical system over the conventional laparoscopic approach. Other studies have shown significant improvement with robotic instrumentation. In the setting of surgically naïve subjects, the improvement in the learning curve has been shown to be more significant with robotics than with laparoscopy, suggesting that basic skills set is learned more quickly with robotics [7, 8]. Nio et al. [9] looked at the efficiency of manual laparoscopy versus robotic instrumentation for standardized tasks such as bead dropping, rope passing, needle capping, suturing and cholecystectomy, and they found the robotics required fewer movements to complete the tasks. All these studies looked at the time required to perform the tasks and with what accuracy it could be performed. None of these studies looked at clinical outcomes long term. Our pilot study will look not only at acquiring the skills set needed to perform complex laparoscopic tasks, but also will help us in the longterm to determine the learning curve need to acquire this skill set. This study brings us to the future of surgical training, and addresses the growing concern and need for hands-on operative experience.
As technology advances, the use of robotics in conjunction with box trainers and virtual simulator environments is the next logical threshold to cross in surgical education and training. Our study incorporates the use of the ProMIS surgical simulator in concert with the Da Vinci robotic surgical system to look at advanced laparoscopic skill set acquisition. The results of our study were very encouraging, in that the skill set was definitely learned faster and with more precision by surgeons using robotics than standard laparoscopy. This was true for both arms of the study even though half the surgeons performed the tasks with laparoscopic instrumentation first. Those in the laparoscopic arm of the study may have become acclimated to the tasks and hence shown an improvement when completing the robotic arm of the study. This still does not account for the better performance noted in the group that used robotic instrumentation first. The improvement in the study as a whole still favored robotic instrumentation over standard laparoscopy: 80% of the subjects improved with robotic instrumentation in all three testing parameters. Not only were the results statistically significant when compared with laparoscopic instrumentation but, within the individual arms of the study (laparoscopic and robotic), there was improvement with each consecutive session. This we knew from our earlier data [7]; however, we also found that the improvement in the robotics group was significantly higher when comparing task performance in the first session to the third session for all three of the modules. Another factor that may have contributed to the robotic arm of the study performing better was the resolution of the ProMIS image. Subjectively, all the surgeons felt it to be grainy and of lower resolution as compared to the Da Vinci three-dimensional (3D) high-definition image. This is something to account for in future studies utilizing the ProMIS simulator.
The use of the ProMIS surgical simulator makes our study unique. ProMIS afforded us the flexibility and ability to set up advanced free-standing modules to be used in a virtual-reality environment without compromising the collection of data in an objective manner. The built in software gave us the ability to analyze the real time movements recorded by the simulator. This was useful both in comparing the skills set of the subjects as well as in the teaching of the desired task. Validation of the ProMIS surgical simulator has been accomplished previously with laparoscopic tasks by the group at Emory University [10]. However, the validation of ProMIS for robotic instrumentation has not been done. Our study is the starting point for accomplishing this task This pilot study gives us the insight that using virtual reality environments with robotics is a novel approach for not only skills acquisition of the advanced laparoscopic tasks, but it can be utilized to plot learning curves that can help with setting up a curriculum for robotic surgical training for residents and fellows alike.
Conclusions
The ProMIS computerized assessment system can be modified to objectively obtain task performance data with robotic instrumentation. All the tasks were performed faster and with more precision using the robotic technology than standard laparoscopy. ProMIS simulator technology is indeed useful in plotting the leaning curves for robotic skills training. Once this technology is successfully incorporated with the robotic surgical system, it could change the way we learn, teach and practice the art of surgery.
References
Chang L, Satava RM, Pellegrini CA, Sinanan MN (2003) Robotic Surgery – Identifying the learning curve through objective measurement of skill. Surg Endosc 17:1744–1748
Ballantyne GH (2002) The pitfalls of laparoscopic surgery: challenges for robotics and telerobotic surgery. Surg Lap Endosc Perc Tech 12:1–5
Pagni S, Qagish NK, Senior DG, Spence PA (1997) Anastomotic complications in minimally invasive coronary bypass grafting. Ann Thorac Surg 63:S64–67
Melvin WS, Johnson JA, Ellison EC (1996) Laparoscopic Skills Enhancement. Am J Surg 172:377–379
Rosser JC, Rosser LE, Savalgi RS (1997) Skill acquisition and assessment for laparoscopic surgery. Arch Surg 132:200–204
Dakin GF, Gagner M (2003) Comparison of laparoscopic skills performance between standard instruments and two surgical robotic systems. Surg Endosc 17:574–579
Melvin WS, Needleman BJ, Krause KR, Schneider C, Ellison EC (2002) Computer enhanced versus standard laparoscopic antireflux surgery. J Gastrointest Surg 6:11–16
Strayer MP, et al. (2001) Computer enhanced “robotic “ telesurgery versus standard laparoscopy: performance on a skills test. [Abstract] – SAGES Annual meeting, St Louis, MO, USA
Yohannes P, Rotariu P, Pinto P, Smith AD, Lee BR (2002) Comaprison of robotic versus laparoscopic skills : is there a difference in the learning curve? Urology 60: 39–45
Nio D, Bemelman WA, Boer KT, Dunker MS, Gouma DJ, Gulik TM (2002) Efficiency of manual versus robotically assist laparoscopic sugery in the performance of standardized tasks. Surg Endosc 16: 412–415
Van Sickle KR, McClusky DA 3rd, Gallagher AG, Smith CD (2005) Construct validation of the ProMIS simulator using a novel laparoscopic suturing task. Surg Endosc 19: 1227–1231
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Narula, V.K., Watson, W.C., Davis, S.S. et al. A computerized analysis of robotic versus laparoscopic task performance. Surg Endosc 21, 2258–2261 (2007). https://doi.org/10.1007/s00464-007-9363-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-007-9363-0