
Abstract
Swallowing problems occur in 37–78 % of stroke patients. Evidence points to multiple factors contributing to the development of pneumonia in the first week post stroke, of which the presence of dysphagia is one. A heightened understanding of the very acute phase (first 7 days post stroke) is required to improve management of this population. We conducted a retrospective review of 536 stroke patients admitted to Australian hospitals in 2010. Data were collected on 37 clinical and demographic parameters. Descriptive statistics and univariate and multivariate logistic regression analyses were performed. Dysphagia was present in 58.5 % of admissions. For those patients remaining in the study for the full week there was a recovery rate from dysphagia of 30.5 %. Overall incidence of respiratory infection was 11 %. Respiratory infections developed in 17 % of patients with dysphagia. Impaired Glasgow Coma Scale, ischemic stroke, and significantly impaired mobility were associated with swallowing difficulties. Being nil by mouth and insertion of a nasogastric tube were significant predictors for respiratory infections. This study of a large cohort of acute stroke patients supports research indicating that aspiration pneumonia is multifactorial in nature and the incidence of respiratory infection is significant in the very acute stroke period.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dysphagia is a frequent occurrence post stroke. Swallowing problems are reported in 37–78 % of stroke patients depending on the timing of screening and assessments used [1]. Half of acute stroke patients recover from dysphagia in the first 2 weeks, with the other half having chronic dysphagia [2, 3]. Research into predictors of dysphagia in stroke have identified older age (>70 years) and more severe strokes to be associated with swallowing complications [4]. Dysphagia may increase length of stay in hospital by 73 %, with only 14 % of patients without dysphagia requiring ongoing hospitalisation longer than 7 days [5].
Current dysphagia management involves reducing aspiration risk through diet and fluid modification, compensatory manoeuvres and positional changes, and rehabilitation exercises [6]. Patients with dysphagia have an increased risk of developing a respiratory infection [1, 7, 8]. Up to 48 % of dysphagic stroke patients develop aspiration pneumonia; however, up to half of stroke patients who develop pneumonia do not have dysphagia. Instrumental evaluations that directly demonstrate dysphagia show little correlation between aspiration and development of aspiration pneumonia [9], supporting the hypothesis that other factors are involved [10, 11]. Recently, factors such as decreased mobility, poor oral hygiene, and feeding tubes have been investigated [12].
Some stroke patients with dysphagia are made to go nil by mouth (NBM) to substantially restrict oral intake and reduce the risk of aspiration. These patients will often have feeding tubes inserted to meet their nutrition and hydration requirements. However, despite the perception that by making a patient NBM the risk of aspiration is decreased, the relationship between aspiration and development of respiratory infections has been shown to be complicated by several other factors, including the bacterial load in the oral cavity, with poor oral hygiene and number of decayed teeth found to be significantly associated with an increased risk of developing respiratory infections [9]. In fact, the presence of feeding tubes has been investigated for a possible link to developing aspiration pneumonia. Nakajoh et al. [13] found the frequency of pneumonia was significantly higher in patients with dysphagia who were fed orally than in those who were tube fed. In contrast, another study found that patients with dysphagia who were dependent on tube feeding were significantly more likely to receive antibiotics for respiratory infections than orally fed counterparts [12]. Tube feeding does not alter the risk of aspiration of refluxed gastric contents resulting in aspiration pneumonia [9]. Langdon et al. [12] suggested postponing enteral feeding in patients with dysphagia who are unable to safely tolerate oral intake for the first few days after stroke; they stated that feeding tubes offer no protection from aspiration of oral secretions and may promote colonisation of the oral cavity by pathogenic bacteria as biofilms that harbor bacteria form on the tubes within 24 h of insertion [12]. A significant correlation between the presence of pathogenic bacteria in the oral cavity and the occurrence of pneumonia has been demonstrated, while increased attention to oral hygiene is linked to a reduced pneumonia incidence [14, 15].
The impact of dysphagia and aspiration pneumonia on healthcare costs is significant and is expected to increase as the population ages [16]. A heightened understanding of the very acute (up to 7 days) stroke period and the relationship between dysphagia and aspiration pneumonia can lead to improved management of stroke patients. Research into risk factors for aspiration pneumonia is a first step in discovering strategies to reduce post-stroke infections.
This article hypotheses that (1) 50 % or more of acute stroke hospital admissions will be dysphagic, (2) a significant proportion of patients will have their dysphagia resolve in the first week, and (3) factors other than dysphagia will be significant predictors of patients developing respiratory infections.
Materials and Methods
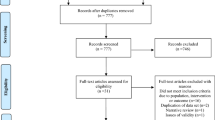
A retrospective medical record review was undertaken on patients admitted to Australian tertiary hospitals in 2010 with a primary diagnosis of “Stroke” or “CVA.” All stroke patients were included regardless of stroke history; however, patients presenting with a subarachnoid or subdural haemorrhage were excluded. We reviewed the medical records of 536 patients from six hospitals who agreed to participate in the study. Medical admission data and standard of care were similar across settings, making collection and standardization of data possible. Data that were not in the medical record were marked as “not recorded.” Data were collected from medical records by speech pathologists using a standardised de-identified data collection form. Collected data included (1) demographic details (age, gender), (2) stroke type (Oxford Stroke Classification), (3) stroke severity [Glasgow Coma Scale (GCS) on arrival, continence status on arrival, Barthel score], (4) premorbid living arrangement and level of support, (5) number of medications per day, (6) presence or absence of comorbidities (smoking, diabetes, respiratory, or GI disorder), (7) mobility (premorbid, on admission, and at day 7), (8) dysphagia documented by speech pathologist in the medical record (premorbid, on admission, days 3–4, and days 6–7), (9) NBM (days 1–2, days 3–4, and day 6–7), (10) requiring modified diet or fluids and type (days 1–2, days 3–4, and days 6–7), (11) presence or absence of a NGT during the first week, (12) presence or absence of enteral feeding during the first week, (13) presence or absence of infection, type, and day of diagnosis, and (14) discharge destination. These variables were chosen because they have been shown in previous studies [8, 9, 17] to be associated with increased risk of respiratory infections. Dysphagia and the time point were marked as recorded based on a documented diagnosis by the treating speech pathologist in the medical record entry. Standard practice for diagnosing a patient with dysphagia was used, including, but not limited to, clinical bedside evaluation of swallowing. Specific criteria for diagnosis were not specified. All patients who were NBM were recorded irrespective of whether it was because of dysphagia.
All data were entered into a central electronic file and analysed using the R environment for statistical computing [18] and SPSS Statistics for Windows (IBM Corp., Armonk, NY, USA). Of the 536 cases, 3 were excluded as they developed more than one infection. The relationship between clinical factors, dysphagia, and respiratory infections was analysed using univariate and multivariate binary logistics. Variable selection was carried out using an information criteria approach and the graphical techniques described in medical statistics [19]. Adjusted and unadjusted odds ratios (OR) and associated 95 % confidence intervals (CI) are presented.
Results
Demographics and Dysphagia
The sample comprised 292 (54.8 %) men and 241 (45.2 %) women with an average of 71 years (SD = ±14.9). There were 339 (63.6 %) ischemic strokes, 139 (26.1 %) haemorrhagic strokes, and 55 (10.3 %) marked as “not recorded.” During the first week 40 (7.5 %) deaths occurred. Preadmission dysphagia was recorded for 23 (4.3 %) patients and there were 68 (12.8 %) patients who were “not recorded.” Dysphagia was recorded in 312 (58.5 %) stroke patients on admission, with an average age of 73 years (SD = ±13.8). The average age for patients without dysphagia was 67 years (SD = ±15.5). There were 4 patients who were marked as “not recorded” for dysphagia on admission.
There were 378 patients who were followed up for the full 7 days of the study. Figure 1 shows the decrease in the proportion of patients with dysphagia over the first week. The percentage of these patients with dysphagia on admission was 67.2 %, which decreased to 52.1 % on days 3–4 and further decreased to 46.0 % on day 7. There were 35 % of patients who were dysphagic on admission who had resolved their swallowing problems within the first week.

Dysphagia in the first week
There were 98 (18.4 %) follow-up patients who had a NGT inserted during the first week and one patient was “not recorded.” Of those who had a NGT inserted during the first week, there were 93 (95.9 %) patients who were dysphagic on admission. On days 1–2 post stroke, 228 (73.1 %) patients with dysphagia were NBM. Of the 254 patients who were dysphagic on admission and remained in the study for the full week, there were 186 (73.2 %) patients who were NBM on days 1–2; by day 7, a total of 132 (71.0 %) of these patients were no longer NBM. The highest percentage of dysphagic stroke patients were still inpatients at the end of the first week (124 patients, 39.7 %), followed by 74 (23.7 %) who went to a rehabilitation destination, 61 (19.6 %) went home, 36 (11.5 %) died, and 17 (5.5 %) went to residential care. In comparison, in the stroke patients with no dysphagia recorded, there were 3 (1.4 %) deaths in the first week and 65 (30 %) remained in hospital.
Predictors of Dysphagia
Univariately, the proportion of individuals with dysphagia differed by age, incontinence (79 % being incontinent, 46 % not), GCS (91 % with severe, 83 % with mild, and 48 % with normal), sex (58 % males, 67 % females), and admission mobility (91 % requiring full assistance, 54 % using aid, and 31 % independent). Multivariately, after adjusting for all other variables, mild GCS compared to normal GCS [OR 2.59; 95 % CI (1.36,4.92); p = 0.0037], ischaemic strokes compared to haemorrhagic strokes [4.01; 95 % CI (2.06,7.81); p < 0.0001], and full assistance with mobility compared to independent mobility [OR 30.09 (95 % CI (12.34,73.35); p < 0.0001] were all associated with dysphagia (Table 1).
Respiratory Infection
Respiratory infections developed in 60 (11.3 %) patients and in 52 (16.7 %) patients with dysphagia. Univariately, the proportion of individuals with an infection differed with respect to mobility at admission (24 % requiring full assistance, 4 % using aids, and 1 % being independent), dysphagia at admission (17 % with dysphagia and 3 % with no dysphagia), GCS (34 % with severe, 19 % with mild, and 5 % with normal), incontinence (22 % being incontinent and 3 % not), dysphagia at any time point (17 % with dysphagia and 0.5 % without), NGT (37 % with NGT and 5 % without), and NBM (21 % NBM and 2 % not). However, looking at admission variables only multivariately, after adjusting for all other variables the odds of respiratory infection were 6.48 times [95 % CI (1.35,31.16); p = 0.0198] higher for patients requiring full assistance with mobility compared to patients independently mobilising and 3.21 times [95 % CI (1.16,8.87); p = 0.025] higher if they were incontinent.
During the first week post stroke, multivariately dysphagia ceased to be significantly associated with stroke, while NGT [OR 3.91; 95 % CI (1.73,8.80); p = 0.001] and being NBM [OR 5.62; 95 % CI (1.54,20.46); p = 0.0089] were independently associated (Table 2).
Discussion
We analysed the incidence and associations between dysphagia and respiratory infections in acute stroke patients in the first 7 days post stroke. Dysphagia was determined using clinical bedside assessments and was reported in 58 % of stroke patients, supporting our hypothesis that 50 % or more of acute stroke hospital admissions will be dysphagic. It is commonly reported that clinical bedside assessments of swallowing underestimate the real incidence of dysphagia when compared to instrumental evaluation; therefore, the actual incidence may be higher [2]. In the first 2 days after stroke, 73 % of patients were NBM. As part of the stroke protocol, many stroke patients are NBM while waiting for swallowing assessment, overinflating the incidence. Prior studies of recovery rate in the first week post stroke report quite variable rates of between 19 and 51 %, with residual dysphagia on day 7 [8, 17]. In our sample, 33 % were recorded as having ongoing dysphagia on day 7, the disparity likely reflecting methodological differences among studies. Mortality rates in this study were similar to those in prior research [8]. One week post stroke, dysphagic patients were more likely to still be in hospital, be discharged to residential care, or deceased compared to their nondysphagic counterparts, which is in keeping with previous reports [20].
Dysphagia was not a significant independent predictor for respiratory infection in this study. Of note, patients who were immobile or incontinent were more likely to get a respiratory infection than a patient with dysphagia. Patients with a NGT were significantly more likely to develop respiratory infections than survivors fed orally, replicating the findings of other studies [9, 12, 21]. However, as 95 % of patients with a NGT were dysphagic, we cannot determine whether increased dysphagia severity, and hence having a NGT in situ, accounts for the relationship between having a NGT and respiratory infection. A 38 % incidence of pneumonia in acute NGT-fed patients warrants further investigation into the management of these patients. Challenges include distinguishing whether pathogenesis of respiratory infections is aspiration of refluxed tube feedings or bacteria-laden saliva [9]. Stroke patients are immunocompromised and often elderly or dependent on others for oral care, contributing to an increased risk of colonisation in the oropharynx [17].
Stroke survivors who need full assistance with mobility were 6.5 times more likely to develop a chest infection than independently mobilising patients. Decreased mobility may relate to decreased air entry and impaired drainage of secretions from the lungs, contributing to increased rates of pneumonia. Rotating immobile patients in bed has been proven to prevent and treat chest infections [22]. Another independent predictor of respiratory infection was incontinence on admission, with 70 % of this group developing a chest infection. Incontinence on admission may be a measure of stroke severity and when linked with stroke-induced immunosuppression, severe stroke patients may be more susceptible to infections [10, 23].
To our knowledge this is the first documented finding of ischemic stroke type being an independent predictor of dysphagia. This may be because many prior studies have not compared ischemic stroke with haemorrhagic stroke with dysphagia, including only the more common ischemic strokes. Haemorrhagic strokes have been reported to cause more severe dysphagia [24, 25] and are associated with increased mortality. Total anterior circulation infarct (TACI) strokes have also been reported to have an increased likelihood of dysphagia [17].
The above evidence highlights the multifactorial nature of aspiration pneumonia. Dysphagia may be a contributing but not the only factor in causing pneumonia, supporting earlier work in this field [9, 12]. We advocate for continued research into the factors contributing to aspiration pneumonia. We propose that being immunocompromised post stroke, poor oral hygiene, use of a feeding tube, and poor mobility have significant roles to play. Further investigation into these factors may contribute toward prevention of pneumonia in this vulnerable population.
Limitations
The main limitation of this study is its design. Our study was a retrospective chart review that relies on accurate reporting and classification and is subject to errors in documentation. All patients who were NBM were recorded irrespective of whether this was related to dysphagia. Including patients who were NBM due to dysphagia would assist only in clarifying the relationship and is a potential area for future study. A standardised measure of dysphagia, such as the gold standard videofluoroscopy, was not used in this study due to the retrospective nature of a chart review; therefore, reliability of diagnosis cannot be determined. Similarly, criteria for diagnosing aspiration pneumonia relied on medical expertise and were not specified. Documented infections were presumed to occur after stroke onset; however, the possibility that infections were present prior to the stroke cannot be excluded.
Conclusion
In a cohort of 536 patients, 58.8 % were diagnosed with dysphagia in the first week post stroke. Of the stroke survivors with dysphagia, 17 % were diagnosed with a respiratory infection. A very high incidence of respiratory infection was seen in immobile patients with an associated risk ratio of 6.5. Dysphagia was not identified as a significant predictor of respiratory infection on multivariate analysis. However, being NBM (RR 3.91) or having a nasogastric tube inserted (RR 5.62) was significantly associated with developing respiratory infection. This research reinforces the hypothesis that aspiration pneumonia is a multifactorial phenomenon and that being immunocompromised, poor oral hygiene, use of a feeding tube, and poor mobility are contributing factors in the acute stroke period. Further studies should examine the potential of modifying risk factors to decrease infections.
References
Martino R, Foley N, Bhogal S, Diamant N, Speechley M, Teasell R. Dysphagia after stroke: incidence, diagnosis and pulmonary complications. Stroke. 2005;36:2756–63.
Mann G, Hankey GJ, Cameron D. Swallowing disorders following acute stroke: prevalence and diagnostic accuracy. Cerebrovasc Dis. 2000;10:380–6.
Ickenstein GW, Höhlig C, Prosiegel M, Koch H, Dziewas R, Bodechtel U, Müller R, Reichmann H, Riecker A. Prediction of outcome in neurogenic oropharyngeal dysphagia within 72 hours of acute stroke. J Stroke Cerebrovasc Dis. 2011;21:1–8.
Mann G, Hankey GJ, Cameron D. Swallowing function after stroke: prognosis and prognostic factors at 6 months. Stroke. 1999;30:744–8.
Altman K, Yu G, Schaefer SD. Consequence of dysphagia in the hospitalized patient. Arch Otolaryngol Head Neck Surg. 2010;136:784–9.
Langdon C, Blacker D. Dysphagia in stroke: a new solution. Stroke Res Treat. 2010. doi:10.4061/2010/570403.
Masiero S, Pierobon R, Previato C, Gomiero E. Pneumonia in stroke patients with oropharyngeal dysphagia: a six month follow-up study. J Neurol Sci. 2008;29:139–45.
Langdon PC, Lee AH, Binns CW. A critical period of susceptibility to infection in acute ischemic stroke. J Med Speech Lang Pathol. 2009;17:55–61.
Langmore SE, Terpenning MS, Schork A, Chen YL, Murray JT, Lopatin D, Loesche WJ. Predictors of aspiration pneumonia: how important is dysphagia? Dysphagia. 1998;13:69–81.
Westendorp WF, Nederkoorn PJ, Vermeij J, Dijkgraaf MG, Van de Beek D. Post-stroke infection: a systematic review and meta-analysis. BMC Neurol. 2011;11:110.
Emsley HC, Hopkins SJ. Acute ischaemic stroke and infection: recent and emerging concepts. Lancet Neurol. 2008;7:341–53.
Langdon PC, Lee AH, Binns CW. High incidence of respiratory infections in ‘nil by mouth’ tube-fed acute ischemic stroke patients. Neuroepidemiology. 2009;32:107–13.
Nakajoh K, Nakagawa T, Sekizawa K, Matsui T, Arai H, Sasaki H. Relation between the incidence of pneumonia and protective reflexes in post-stroke patients with oral or tube feeding. J Intern Med. 2000;247:39–42.
Abe S, Ishihara K, Adachi M, Okuda K. Tongue coating as risk indicator for aspiration pneumonia in edentate elderly. Arch Gerontol Geriatr. 2009;47:267–75.
Adachi M, Ishihara K, Abe S, Okuda K. Professional oral health care by dental hygienists reduced respiratory infections in elderly persons requiring nursing care. Int J Dent Hyg. 2007;5:69–74.
Martino R, Martin RE, Black S. Dysphagia after stroke and its management. CMAJ. 2012;184(10):1127–8.
Langdon C, Lee AH, Binns CW. Dysphagia in acute ischaemic stroke: severity, recovery and relationship to stroke subtype. J Clin Neurosci. 2007;14:630–4.
R Core Team. R: a language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2012.
Murray K, Heritier S, Muller S. Graphical tools for model selection in generalized linear models. Stat Med. 2013. doi:10.1002/sim.5855.
Smithard DG, O’Neill PA, Parks C, Morris J. Complications and outcome after acute stroke. Does dysphagia matter? Stroke. 1996;27:1200–4.
Dziewas R, Ritter M, Schilling M, Konrad C, Oelenberg S, Nabavi DG, Stögbauer F, Ringelstein EB, Lüdemann P. Pneumonia in acute stroke patients fed by nasogastric tube. J Neurol Neurosurg Psychiatry. 2004;75:852–6.
Goldhill DR, Imhoff M, McLean B, Waldmann C. Rotational bed therapy to prevent and treat respiratory complications: a review and meta-analysis. Am J Crit Care. 2007;16:50–61.
Wartenberg KE, Stoll A, Funk A, Meyer A, Schmidt JM, Berrouschot J. Infection after acute ischemic stroke: risk factors, biomarkers, and outcome. Stroke Res Treat. 2011;2011:830614.
Remesso GC, Fukujima MM, Chiappetta AL, Oda AL, Aguiar AS, Oliveira Ade S, do Prado GF. Swallowing disorders after ischemic stroke. Arq Neuropsiquiatr. 2011;69:785–9.
Suntrup S, Warnecke T, Kemmling A, Teismann IK, Hamacher C, Oelenberg S, Dziewas R. Dysphagia in patients with acute striatocapsular hemorrhage. J Neurol. 2012;259:93–9.
Conflict of interest
The authors have no conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brogan, E., Langdon, C., Brookes, K. et al. Respiratory Infections in Acute Stroke: Nasogastric Tubes and Immobility are Stronger Predictors than Dysphagia. Dysphagia 29, 340–345 (2014). https://doi.org/10.1007/s00455-013-9514-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00455-013-9514-5