
Abstract
Objective
In order to evaluate the prescribing pattern in the Italian paediatric population, prescriptions involving 923,353 children under 14 years old and dispensed during 2006 by the retail pharmacies of 22 Italian local health units were analysed.
Materials and methods
A total of 561,237 children (61%) received at least one drug prescription. The prescription prevalence rate was highest in children 3 years of age (78%), decreased with increasing age and was higher in boys than in girls (χ2 = 655; p << 0.001). Each treated child received an average of 3.2 prescriptions and 4.8 boxes.
Results
Antibiotics and anti-asthmatics were the more prescribed therapeutic classes and represented 80% of prescriptions. Amoxicillin+clavulanic acid was the most prescribed drug (24% of the overall population; 17% of all boxes), followed by inhaled beclometasone and amoxicillin. A total of 620 different drugs were prescribed and the ten leading drugs represented 64% of the prescribed boxes. Six of the ten most prescribed drugs were the same in all age groups. Wide differences were found in the prevalence rate between the different local health units; these ranged between 50.1 and 68.4% (p << 0.001). The prescription prevalence increased in the 2000–2002 period (from 62.2 to 68.3%) and slightly decreased afterwards.
Conclusion
Despite some limitations, the systematic monitoring of prescriptions is a valuable tool for evaluating the appropriateness of the care.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Although the importance of obtaining evidence for a more rational use of medicines for children, infants and neonates is widely recognised among professionals and lay people (parents, patients and politicians), a dearth of information on the safety and efficacy of drugs in childhood exists [10, 32]. Many aspects can contribute to this understudied position of children with respect to optimal drug therapies, some of which include: the different pharmacokinetic and pharmacodynamic profiles during growth and development; ethical and financial reasons; resources and research capabilities; and regulatory guidelines and constraints [39]. More efforts are, thus, needed to guarantee that children receive medications that are appropriate (safe and effective) to their clinical conditions, in doses and formulations suitable to their personal requirements, for adequate periods of time, and at the lowest cost to their families and communities, i.e. a rational drug use [38]. In such a context, pharmacoepidemiology is a useful tool [21] that, with the appropriate methodologies, can improve the effectiveness and efficiency of healthcare interventions [36]. Patterns of drug prescribing and use in developed and developing countries have been studied extensively [20], but, to date, the drug profiles in children continue to remain a rarity instead of a routine approach [6].
In order to evaluate the prescribing pattern in the Italian paediatric population, an analysis of the data collected in a large prescription database was performed.
Methods
The Italian health system framework
Italian healthcare is provided free or at a nominal charge through a network of 195 local health units (LHUs) covering an average of 290,000 citizens. Every Italian resident is registered with a family (paediatric or general) practitioner. There are about 7,450 primary care paediatricians caring for over 7 million children, the majority of whom are less than 6 years old. Children are assigned to a paediatrician until they are 6 years old; afterwards, the parents can choose to register a child with a general practitioner. A national formulary is available, in which drugs are categorised into two classes: class A includes essential drugs that patients do not have to pay for and class C contains drugs not covered by the National Health Service. Some drugs are reimbursed for some indications only. Most antibiotics and nearly all chronic disease therapies are free of charge.
Data source: the ARNO database
The ARNO database is a population-oriented database that collects information on drug use outside the hospital setting in Italy. The system, active since 1988, is run by CINECA, a National Interuniversity Consortium, and merges information regarding prescriptions, the population, geographical areas and the community setting into a single database.
The analysis involved all paediatric prescriptions reimbursed by the National Health Service and dispensed by the retail pharmacies of 22 Italian LHUs (which were part of the ARNO project) between 1 January 2006 and 31 December 2006. LHUs were located in six Italian regions from the northern, central and southern areas, and were representative of urban and rural settings.
The data were managed and analysed using an anonymous patient code, after obtaining each LHU director’s authorisation.
The study population was composed of 923,353 children under 14 years of age living in the 22 LHUs’ areas. The study sample represented 14% of the Italian paediatric population and the male/female ratio was 1.06. The gender and age distribution of the sample was not different from that of the Italian paediatric population.
The prescribed drugs were classified according to the International Anatomic Therapeutical Classification system (ATC).
The number of boxes was used as an indicator to evaluate the pharmaceutical consumption.
Prevalence data by sex and age were calculated by dividing the number of drug users by the total number of male and female residents in each age group. A Mantel-Haentzel χ2 test was performed to compare the drug prescription prevalence in boys and girls.
The area under the prevalence–time curve (AUC) from time 0 to 14 years (data plotted at the mid-time interval) were calculated according to the linear trapezoidal rule and compared by the paired t-test. The decreasing phases of the prevalence versus time curve were estimated by log-linear least square fitting of the 3- and 13-year age points. Comparisons were made using the t-test.
The relation between the prevalence rates of the most prescribed therapeutic classes by LHU was investigated using the non-parametric Spearman rank correlation test.
Statistical analysis was performed using SPSS 10.1 software and IBM DB2 Intelligent Miner for Data version 6. WinNonlin version 4.1 was used in calculating the AUC.
A p-value <0.05 was considered to be statistically significant.
Results
Prescribing pattern during 2006
During 2006, 561,237 children (61% of the population) received at least one drug prescription. The highest prevalence was observed in the 1–4 years old period (average value 76%); it then decreased according to a two-phase slope: the 4–7 years old (76 to 58%) period was faster than the 7–13 years old period (58 to 43%) (p < 0.0001) (Fig. 1).

Prescription prevalence rate and the average number of prescriptions/treated child by gender and age
The prevalence was slightly higher in boys than in girls for all ages (χ2 = 655; p << 0.001), but had the same profile. The AUC0–14 male/female ratio was 1.04.
In all, 1,117 paediatricians prescribed drugs to 77% of the children, while to 19% of the children, drugs were prescribed by 5,871 general practitioners. A total of 1,805,521 prescriptions were dispensed, corresponding to 2,697,979 boxes. Each treated child received an average of 3.2 prescriptions (median 3) and 4.8 boxes (median 3) during the one-year study period. Boys received a greater average number of prescriptions (3.3 versus 3.1) and boxes (5.0 versus 4.6) than girls.
The highest number of prescriptions/treated child was observed in children age 3–4 years old (3.8; median 3). While prescription prevalence decreased steadily in the 7–13 years old period, the decrease in the average number of prescriptions per treated child was less prominent.
A total of 22% of treated children received only one box, while 27% received more than five (and ten or more boxes were dispensed to 11%). The rate of children receiving six or more boxes was higher in males than in females (28 versus 25%; χ2=862; p << 0.001), and in children aged 1–4 years old (33%) compared to those <1 year (18%) and ≥5 years (23%) (p << 0.001) of age.
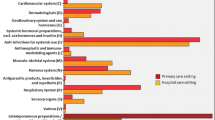
Antibiotics were the most prescribed therapeutic class (52% of the population), followed by anti-asthmatics (26%), systemic corticosteroids (8%) and anti-histamines (6%). Altogether, these four therapeutic classes comprised 90% of the prescribed boxes.
Most children received drugs belonging to one therapeutic class only (52% of treated children), while 32% received drugs belonging to two classes (mainly antibiotics and anti-asthmatics, prescribed to 26% of treated children), and 16% to three or more classes (8% received antibiotics, anti-asthmatics and systemic steroids).
Figure 2 reports the prevalence trend by gender and age of the four most prescribed therapeutic classes. The trend for antibiotics is similar to the overall trend, while the highest value of anti-asthmatic and systemic steroid prevalence was observed at 1 year of age (40 and 13%, respectively). The prevalence of anti-asthmatics reached a second age-dependent peak at 3 years of age (39%), while the systemic steroid prevalence progressively decreased after 1 year of age.

Prescription prevalence rate by age of the four most prescribed therapeutic classes
The prevalence of anti-histamines increased with increasing age, reaching a maximum of 7% at 4 years of age, and then slightly decreased.
The AUC0–14 male/female ratio ranged between 1.03 for the antibiotics and 1.30 for the anti-histamines classes.
Among the most prescribed therapeutic classes, antibiotics were associated with the highest average number of boxes per treated child (3.2), while systemic steroids were associated with the lowest (1.7). The greatest proportion of children receiving more than five boxes was observed among antibiotic users (14%), followed by anti-asthmatic users (9%). On the contrary, 65% of children treated with systemic steroids received only one box, compared to 54% of those treated with anti-histamines, 43% of those treated with anti-asthmatics and 31% of children treated with antibiotics.
Penicillins were the most prescribed antimicrobial class (65% of the antibiotic users), followed by cephalosporins (39%) and macrolides (37%).
A total of 86% of anti-asthmatic users received at least one prescription of inhaled steroids, while 54% received adrenergic drugs (alone or in fixed combination with other anti-asthmatics).
A total of 620 drugs were prescribed. Amoxicillin+clavulanic acid was the most common (24% of children), followed by inhaled beclometasone (15%) and amoxicillin (14%) (Table 1).
The ten most prescribed drugs, six of which were antibiotics, represented 64% of the prescribed boxes and covered 89% of children receiving at least one drug prescription.
A total of 41 drugs, belonging to 12 main ATC therapeutic groups, comprised 90% of the prescribed boxes. In particular, 15 were antibiotics, eight were anti-asthmatics and six were anti-histamines.
Beclometasone was the most prescribed drug in children under 1 year old, while amoxicillin+clavulanic acid was the leading drug in children ≥1 year of age. Although the prevalence rates differed across ages, six of the ten most prescribed drugs were the same in all ages. It can, thus, be concluded that a total of 15 drugs would suffice to address the main therapeutic needs of children, independently of age.
Four age groups shared the same most prescribed drugs. Flunisolide, budesonide and salbutamol in fixed combination with other anti-asthmatics ranked among the top ten drugs only in children <1 year old, cefixime, azithromycin and ceftibuten in those ≥1 year of age, while cetirizine and fluticasone were among the most prescribed in children ≥7 years and ≥12 years of age, respectively (Table 1).
A total of 38% of treated children received one drug, 24% two, 15% three and 23% four or more different drugs. The proportion of children receiving four or more drugs was higher in boys compared to in girls (25% versus 22%; χ2 = 748; p << 0.001) and in children 1–4 years old (30%) compared to children <1 year (22%) and ≥5 years (17%) (p << 0.001) of age.
Distribution of prevalence by LHU
Wide differences were found in the prevalence rates between different LHUs; these ranged between 50.1 and 68.4% (p << 0.001). The mean prevalence rate was 59.5% (median 60.3%).
The greatest difference was observed between systemic steroid prevalence, which ranged between 1.1 and 19.9%, with a median of 2%.
Geographical differences were also found. Prescription prevalence was lower in northern Italy (57.3%) and higher in the two LHUs in southern Italy (68.3%).
A statistically significant correlation between rank distributions at the LHU level of the overall prevalence rate and of the prevalence of the four most prescribed therapeutic classes was found. The rank correlation was close, especially with antibiotics (r s = 0.99) and systemic steroids (r s = 0.82), as well as between antibiotic and systemic steroid prevalence (r s = 0.84). On the contrary, no statistically significant rank correlation was found between anti-asthmatic and systemic steroid prevalence (r s = 0.37) and between anti-asthmatic and anti-histamine prevalence (r s = 0.42).
Trends in the 2000–2006 period
Prescription prevalence increased between 2000–2002 from 61.5 to 66.9% and decreased afterwards. The prevalence of antibiotics and anti-asthmatics increased in 2006 by 6 and 19%, respectively, compared to 2000.
A total of eight of the ten most prescribed drugs for each year were the same in the 2000–2006 period.
Beclometasone was the most prescribed drug in 2000 and 2001, while it was replaced by amoxicillin+clavulanic acid from 2002 onwards. The prescription prevalence trend for the ten most prescribed drugs was quite similar to the overall trend, with the exception of amoxicillin+clavulanic acid, whose prevalence increased steadily from 13.2 to 24.4%. The 2006 prevalence was higher than in 2000 for most of these drugs, with the exception of cefaclor and ceftibuten, whose prevalence decreased, and beclometasone, whose prevalence did not change. Amoxicillin+clavulanic acid and salbutamol were the drugs with the highest percentage increase in prevalence rate (86 and 73%, respectively).
Expenditure
The total expenditure in 2006 was €37 million (2.4% of the overall pharmaceutical expenditure in the ARNO sample). The mean expenditure for each treated child was €66, was higher for males than females (€70 versus €60) and increased with increasing age, reaching the highest value in 13-year-old children (€85).
Amoxicillin+clavulanic acid was the drug with the highest expenditure (14.5% of the overall expenditure), followed by clarithromycin (11.6%) and azithromycin (7.1%). A total of six drugs (the three just mentioned plus beclometasone, cefixime and montelukast) accounted for 50% of the expenditure, while the first 30 drugs in the order of expenditure accounted for 90%.
Discussion
The size (nearly 1 million children) and geographical distribution of the population are among this study’s major strengths.. Despite some limitations, the findings are representative of prescribing patterns in the Italian outpatient population. The profile observed in this study is quite similar, in terms of rate, gender and age differences and therapeutic classes most frequently prescribed, to those previously observed in national and international settings [1, 9, 19, 22, 24, 26, 31–33].
Some findings seem to be specific to Italy, however.
First of all, Italian children are exposed to a high number of drugs. Nearly 1/4 of the children treated received four or more drugs and 1/10 more than nine boxes (corresponding to a prevalence of 7% in the paediatric population).
Pre-schoolers are the most exposed to drugs, especially children aged 3–4 years old, a finding consistent with the increased incidence of infections upon entry into the community. However, the finding that 1/3 of children aged 1–4 years old needing a drug therapy received more than five boxes/year and more than four different medications is of concern.
The huge number of drugs prescribed (620) is another finding that seems peculiar to the Italian situation. Despite this plethora of medications, the first 41 drugs (7%) in the order of prevalence, 29 of which were antibiotics, anti-asthmatics and anti-histamines, covered 90% of the dispensed boxes. Moreover, 15 drugs seem to be sufficient to cover the most common diseases, independently of age.
Antibiotics were the most prescribed type of drugs: they were prescribed to nine of ten children receiving a prescription. The prevalence reported in the Italian paediatric population is 3–4-fold higher than that in the Netherlands or United Kingdom [30]. Despite this fact, a 6% increase in the antibiotic prevalence rate was observed in the 2000–2006 period.
Amoxicillin+clavulanic acid was the most prescribed drug and its prevalence nearly doubled in the 2000–2006 period; on the contrary, several international guidelines consider amoxicillin alone as the first choice of treatment for the most common childhood infections (acute otitis media, pharyngo-tonsillitis, sinusitis) [2, 3, 11, 34, 35]. Despite the fact that, in other countries, amoxicillin is the most prescribed antibiotic [30], in Italy, amoxicillin+clavulanic acid was probably preferred due to its twice-daily schedule regimen that is supposed to give a better compliance compared to the amoxicillin dosage schedule, to an unproved concern of beta-lactamase-producing bacteria and to the market availability (since 2002) of a more tolerable suspension with an amoxicillin:clavulanic acid ratio of 7:1 instead of 4:1
Moreover, nearly 40% of children receiving antibiotics were prescribed cephalosporins or macrolides, second line agents likely chosen, more often than not, not on the basis of safety and efficacy data, but because of palatability and shorter length of therapies.
The profile of anti-asthmatic drug prescriptions was similar to that previously described (frequent use of inhaled steroids, in particular, nebulised beclometasone, occasionally prescribed to pre-school children) and suggests that the prescriptions concerning these drugs are often inappropriate [12].
The prevalence of anti-asthmatic drug prescriptions was higher than both the prevalence of asthma in Italy and the estimated rate in other paediatric contexts [4, 5, 14, 16, 18, 25, 27]. Furthermore, 60% of the children treated with anti-asthmatics are under 6 years old, while most episodes of wheezing that appear in pre-school children disappear with age and it is difficult to diagnose asthma in children under 6 years of age [17, 23, 37].
Moreover, the lack of correlation between the anti-asthmatic and anti-histamine or systemic steroid prevalence rate is indicative of the fact that anti-asthmatic drugs are often prescribed for diseases different from asthma, as observed in other studies that reported a wide use of nebulised steroids in Italy as prophylaxis or treatment for viral wheezing [9]. The fact that, in Italy, nebulised beclometasone is also licensed for rhino-pharyngitis and the misbelief that it could relieve inflammation due to infections could have contributed to its high prescription prevalence.
The prescribing pattern of systemic steroids also appears inappropriate, since 65% of treated youths received only one box and the highest prevalence was observed in 1-year-old children. The most prescribed drug was betamethasone (96% of systemic steroid users), available in Italy as dispersible tablets and often prescribed for the treatment of upper respiratory tract infections [9]. Steroid prevalence varied widely between LHUs, with a 19:1 ratio between the highest and lowest values. Moreover, it is interesting to note the strong correlation between antibiotic and systemic steroid prevalence and its geographical clustering, which are two findings that support the hypothesis that it is used for the treatment of respiratory infections and the fact that inappropriate drug use is more frequent in a few contexts.
The youngest children, in particular, infants, are more likely to receive drugs with a questionable evidence base. The population of children <1 year of age was, in fact, characterised by a wide use of steroids, either as an inhaled formulation or as systemic use.
Beclometasone was the most prescribed drug in children <1 year of age (prevalence 21%). Flunisolide and budesonide can be considered as quite “typical” of this population, since they ranked among the ten most prescribed drugs only in children <1 year of age, with a prevalence of 6% and 4%, respectively. Moreover, 9% of infants were prescribed betamethasone.
Prescription prevalence did not change in the 2000–2006 period. Periodic reports have been released since 2000 with the aim to share data collected by the ARNO database with healthcare professionals at the national and local levels and to implement the rational use of drugs in the paediatric population [13, 29]. Furthermore, several Italian drug utilisation studies were published in the last six years (in particular, concerning antibiotics and anti-asthmatics) [8, 9, 12, 15, 28], but they had little impact on the prescribing habits of practitioners, at least according to these findings.
The case of beclometasone is emblematic: an open letter was published in 2001 to warn paediatricians about the overuse of this drug [7]; despite this initiative, its prevalence did not change, even after five years.
Moreover, in 2003, the Italian Ministry of Health published a paediatric formulary entitled “Guida all’uso dei farmaci per i bambini” [Guide to the use of drugs for children], a translation and adaptation to the Italian context of “Medicines for Children” and sent it to healthcare professionals. Only 42% of the drugs prescribed during 2006 were quoted in the formulary. Although “Medicines for Children” may reflect attitudes different from those of Italian practitioners, this figure indicates that many drugs have a questionable evidence base.
The expenditure for drugs prescribed to children is negligible when compared with the overall pharmaceutical expenditure (2.4%). Since the need to reduce expenditure is one of the main determinants of programmes to implement the rational use of drugs, a very low expenditure could paradoxically represent a reason to not address the problem. However, the findings from this study indicate that a significant reduction of expenditure could be achieved by simply choosing the less expensive drug among a plethora of “me-too” medications.
This study has some limitations. The first, common to many studies based on prescription databases, is the lack of information concerning the diseases for which drugs are prescribed.
The second is the lack of data concerning drugs without state reimbursement and over-the-counter drugs. It was, therefore, not possible to evaluate the prescription pattern of some drugs commonly prescribed to children, e.g. paracetamol and antitussive medications.
The decrease in the prevalence rate observed after 2002 may be, at least in part, due to a change in the list of the drugs reimbursed by the Italian National Health Service that was made during 2003, with the exclusion of some classes (e.g. anti-histamines, prokinetics etc.) [13]. Nowadays, anti-histamines can be reimbursed, but with restrictions (chronic treatment for moderate to severe allergies) and their prevalence may, therefore, be underestimated. In this regard, it is interesting to note that, despite the limitation to chronic treatment, 54% of those treated with anti-histamines received only one box.
Conclusions
Despite some limitations, the ARNO database is a valuable tool for evaluating therapeutic needs and the appropriateness of care. The analysis of the 2006 data confirms previous findings: many drugs, belonging to only a few therapeutic classes, are prescribed, and often without an evidence-based indication. The use of a wide range of drugs, related to a limited number of very common childhood diseases, and the lack of compliance with therapeutic guidelines suggest the need for continuous audit and educational programmes (also and especially) in paediatric general practice. Prescribing physicians and children’s parents should, therefore, make an effort to achieve a more rational drug use.
Abbreviations
- AUC:
-
Area under the curve
- ATC:
-
Anatomic therapeutic chemical
- CINECA:
-
Interuniversity Consortium
- LHU:
-
Local health unit
References
Abi Khaled L, Ahmad F, Brogan T, Fearnley J, Graham J, MacLeod S, McCormick J (2003) Prescription medicine use by one million Canadian children. Paediatr Child Health 8(Suppl A):6A–56A
American Academy of Pediatrics. Subcommittee on Management of Sinusitis and Committee on Quality Improvement (2001) Clinical practice guideline: management of sinusitis. Pediatrics 108:798–808
American Academy of Pediatrics Subcommittee on Management of Acute Otitis Media (2004) Diagnosis and management of acute otitis media. Pediatrics 113:1451–1465
Barbato A, Panizzolo C, Biserna L, Cantarutti L, Giaquinto C, Frati F, Marcucci F, Monciotti C, Testi R, di Blasi P, Sturkenboom MC; Pedianet Family Pediatricians Asthma Study Group (F-PASG) (2003) Asthma prevalence and drug prescription in asthmatic children. Eur Ann Allergy Clin Immunol 35:47–51
Beimfohr C, Maziak W, von Mutius E, Hense HW, Leupold W, Hirsch T, Keil U, Weiland SK (2001) The use of anti-asthmatic drugs in children: results of a community-based survey in Germany. Pharmacoepidemiol Drug Saf 10:315–321
Bonati M (1994) Epidemiologic evaluation of drug use in children. J Clin Pharmacol 34:300–305
Bonati M, Clavenna A, Rocchi F (2001) Corticosteroidi in età pediatrica. Marketing e prescrizione. Informazioni sui Farmaci 2–3:79–82
Borgnolo G, Simon G, Francescutti C Lattuada L, Zanier L (2001) Antibiotic prescription in Italian children: a population-based study in Friuli Venezia Giulia, north-east Italy. Acta Paediatr 90:1316–1320
Cazzato T, Pandolfini C, Campi R, Bonati M; ACP Puglia-Basilicata Working Group (2001) Drug prescribing in out-patient children in Southern Italy. Eur J Clin Pharmacol 57:611–616
Choonara I, Nunn AJ, Kearns G (eds) (2003) Introduction to paediatric and perinatal drug therapy. Nottingham University Press, Nottingham, UK
Cincinnati Children’s Hospital Medical Center (2006) Evidence-based care guideline for management of acute bacterial sinusitis in children 1–18 years of age. Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, 7 July 2006
Clavenna A, Rossi E, Berti A Pedrazzi G, De Rosa M, Bonati M; ARNO Working Group (2003) Inappropriate use of anti-asthmatic drugs in the Italian paediatric population. Eur J Clin Pharmacol 59:565–569
Clavenna A, Bonati M, Rossi E, Berti A, De Rosa M (2004) Il profilo prescrittivo della popolazione pediatrica italiana nelle cure primarie. Ric Prat 20:224–244
Furu K, Skurtveit S, Langhammer A, Nafstad P (2007) Use of anti-asthmatic medications as a proxy for prevalence of asthma in children and adolescents in Norway: a nationwide prescription database analysis. Eur J Clin Pharmacol 63:693–698
Gagliotti C, Morsillo F, Resi D, Milandri M, Moro ML (2005) A three-year population-based study of antibiotic treatments for children. Acta Paediatr 94:1502–1504
Galassi C, De Sario M, Biggeri A, Bisanti L, Chellini E, Ciccone G, Petronio MG, Piffer S, Sestini P, Rusconi F, Viegi G, Forastiere F (2006) Changes in prevalence of asthma and allergies among children and adolescents in Italy: 1994–2002. Pediatrics 117:34–42
The Global Initiative for Asthma (2007) Global Strategy for Asthma Management and Prevention 2007. Home page at: http://www.ginasthma.com
Goodman DC, Lozano P, Stukel TA, Chang Ch, Hecht J (1999) Has asthma medication use in children become more frequent, more appropriate, or both? Pediatrics 104:187–194
Hahn GH, Koch A, Melbye M, Mølbak K (2005) Pattern of drug prescription for children under the age of four years in a population in Greenland. Acta Paediatr 94:99–106
Le Grand A, Hogerzeil HV, Haaijer-Ruskamp FM (1999) Intervention research in rational use of drugs: a review. Health Policy Plan 14:89–102
MacLeod SM (1991) Pharmacoepidemiology: a health imperative. J Clin Epidemiol 44:1285–1286
Madsen H, Anderson M, Halls J (2001) Drug prescribing among Danish children: a population-based study. Eur J Clin Pharmacol 57:159–165
Martinez FD, Wright AL, Taussig LM, Holberg CJ, Halonen M, Morgan WJ (1995) Asthma and wheezing in the first six years of life. The Group Health Medical Associates. N Engl J Med 332:133–138
McIntyre J, Conroy S, Avery A, Corns H, Choonara I (2000) Unlicensed and off label prescribing of drugs in general practice. Arch Dis Child 83:498–501
Moth G, Vedsted P, Schiøtz PO (2007) Identification of asthmatic children using prescription data and diagnosis. Eur J Clin Pharmacol 63:605–611
Niclasen BV-L (2006) Changes in drug prescription over a decade in an Arctic child population. Acta Paediatr 95:1456–1460
Rabe KF, Vermeire PA, Soriano JB, Maier WC (2000) Clinical management of asthma in 1999: the asthma insight and the reality in Europe (AIRE) study. Eur Respir J 16:802–807
Resi D, Milandri M, Moro ML; Emilia Romagna Study Group on the Use of Antibiotics in Children (2003) Antibiotic prescriptions in children. J Antimicrob Chemother 52:282–286
Rossi E, De Rosa M, Bonati M, Covezzoli A, Busca P, Addis A, Tognoni G, Gruppo di Lavoro USL (2001) La prescrizione farmaceutica pediatrica nell’ambito delle cure primarie. Rapporto dalla banca dati ARNO. G Ital Farm Clin 15:26–29
Rossignoli A, Clavenna A, Bonati M (2007) Antibiotic prescription and prevalence rate in the outpatient paediatric population: analysis of surveys published during 2000–2005. Eur J Clin Pharmacol 63:1099–1106
Sanz EJ (2003) Concordance and children’s use of medicines. BMJ 327:858–860
Sanz E, Hernández MA, Ratchina S, Stratchounsky L, Peiré MA, Lapeyre-Mestre M, Horen B, Kriska M, Krajnakova H, Momcheva H, Encheva D, Martínez-Mir I, Palop V (2004) Drug utilisation in outpatient children. A comparison among Tenerife, Valencia, and Barcelona (Spain), Toulouse (France), Sofia (Bulgaria), Bratislava (Slovakia) and Smolensk (Russia). Eur J Clin Pharmacol 60:127–134
Schirm E, van den Berg P, Gebben H, Sauer P, de Jong-van den Berg L (2000) Drug use of children in the community assessed through pharmacy dispensing data. Br J Clin Pharmacol 50:473–478
Scottish Intercollegiate Guidelines Network (SIGN) (1999) Management of sore throat and indication for tonsillectomy. A national clinical guideline. SIGN, Edinburgh, Scotland
Scottish Intercollegiate Guidelines Network (SIGN) (2003) Diagnosis and management of childhood otitis media in primary care. A national clinical guideline. SIGN, Edinburgh, Scotland
The U.S. Pharmacopeia Drug Utilization Review Advisory Panel (2000) Drug utilization review: mechanisms to improve its effectiveness and broaden its scope. J Am Pharm Assoc (Wash) 40:538–545
Townshend J, Hails S, Mckean M (2007) Diagnosis of asthma in children. BMJ 335:198–202
World Health Organization/Action Programme on Essential Drugs (WHO/DAP) (1995) Operational research projects in DAP: an inventory. WHO/DAP
Wong I, Sweis D, Cope J, Florence A (2003) Paediatric medicines research in the UK: how to move forward? Drug Saf 26:529–537
Acknowledgements
Dr. Antonio Clavenna holds a fellowship granted by Boehringer Ingelheim Italia.
The authors would like to acknowledge all of the people involved with the ARNO working group.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Clavenna, A., Berti, A., Gualandi, L. et al. Drug utilisation profile in the Italian paediatric population. Eur J Pediatr 168, 173–180 (2009). https://doi.org/10.1007/s00431-008-0725-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-008-0725-y