
Abstract
Purpose
The role of subcutaneous prophylactic drainage in preventing postoperative abdominal wound complications is still controversial. We aimed to elucidate whether any difference in the incidence of surgical site infection (SSI) exists between patients with or without subcutaneous suction drain following clean-contaminated abdominal surgery.
Methods
PubMed, EMBASE, and the CENTRAL were systematically searched for randomized controlled trials (RCT) comparing drained with undrained surgeries featuring gastrointestinal (GI) tract opening. The aim of the analysis was to assess the incidence of wound infection. A meta-analysis of relevant studies was performed using RevMan 5.3.
Results
A total of 8 studies, including 2833 patients, were considered eligible to collect data necessary. Globally, 187 patients (83 drained versus 104 undrained) experienced some SSI during the postoperative period. The use of subcutaneous suction drains did not exhibit any significant differences between drained and undrained patients in developing SSI (odds ratio 0.76, 95% CI 0.56–1.02; p = 0.07).
Conclusions
According to the available, high-level evidence, the use of subcutaneous drains should not be encouraged on a routine basis, as it does not confer any advantage in preventing postoperative wound infection following clean-contaminated abdominal surgery. However, this does not exclude that there might be a benefit in a specific risk group of patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Surgical site infection (SSI) is considered a postoperative complication after surgery that increases patient morbidity and mortality rates. Some authors suggest the use of subcutaneous drain to prevent wound infection. Contrariwise, large review studies affirm that prophylactic drain does not give significative advantage on preventing SSI. Clean-contaminated surgery, such as abdominal surgery with opening of GI tract, carries higher risk of SSI compared with other surgical procedures [1,2,3,4]. A relative scarcity of specific evidence exists on the argument, with most data returning from low-level analyses and only a few randomized studies returning non-univocal results. As a consequence, the actual role of prophylactic subcutaneous drain is still controversial. Accordingly, the aim of our study is to aggregate the available, high-level evidence from the medical literature to elucidate whether any difference in incidence of SSI exists between patients with or without subcutaneous suction drain placement following clean-contaminated abdominal surgery.
Materials and methods
PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) [5] guidelines were followed in order to identify RCTs comparing drained with undrained surgical incisions after abdominal surgery with opening of GI tract. Before data collection, an itemized protocol to perform the analysis was produced (protocol registered on PROSPERO). Data for meta-analysis were extrapolated from the included studies following the pre-established pattern. Two authors (DC, FG) performed an independent literature search up to September 2018. The PubMed/MEDLINE, EMBASE, and CENTRAL electronic databases [6] were utilized with a combination of the following search words: “subcutaneous,” “suction drain,” “prophylactic,” “drainage,” and “abdominal wound.” All articles dealing with GI surgery (colorectal and lower GI, hepatobiliary, pancreatic, and upper GI surgical procedures) were considered eligible. Full-text papers considered for inclusion were appraised and the relative references were hand-searched to find additional, eligible works. Potentially suitable studies were investigated and eventually included in the analysis if were in the English language; RCT with a comparison between a subcutaneous suction drained group and an undrained group was present; adult patients undergoing clean-contaminated abdominal surgical procedures, either with an open or a minimally invasive approach in elective setting. Emergency GI interventions and ileostomy takedown considered by definition contaminated or dirty surgery have been excluded. Two reviewers (CDB and GG) extrapolated data for meta-analysis from the studies that were eventually included. All disagreements concerning inclusion were solved by consensus, involving all authors. According to the pre-established pattern, the retrieved data were the following: study design, clinical characteristics such as age, body mass index (BMI), number of patients in each group, risk factors, type of surgical procedures, antibiotic prophylaxis, time of drain removing, and diagnosis of SSI. The Center for Diseases Control and Prevention’s definition of SSI [7] was reported by more recent studies [8,9,10,11,12]: purulent drainage with or without laboratory confirmation from the superficial incision; organisms isolated from an aseptically obtained culture of fluid or tissue from the superficial incision; at least one of the following signs or symptoms of infection: pain/tenderness, local swelling, redness, or heat which require deliberately opening of the superficial incision by surgeon, unless incision is culture-negative; diagnosis of superficial SSI by the surgeon or attending physician. Diagnosis of SSI was described in older papers as clinical/cultural evidence of infection like discharge of pus spontaneously or after opening of the incision or in the presence of positive bacterial cultures [13,14,15]. The difference in incidence of SSI between the two groups was considered the main endpoint.
Statistical analysis
Data are presented in descriptive statistics. Meta-analysis was performed using Review Manager 5.3 (Cochrane Collaboration, Oxford, England). Estimated effect measures were calculated for event-related outcomes as odds ratio (OR). By inspecting the forest plots and I2 statistics, a statistical heterogeneity was obtained. ORs were identified and reported with 95% confidence interval (CI). The Z-test for overall effect and its two-sided p value were also assessed. Statistical significance was set at the 0.05 probability level.
Results
Study selection and quality assessment
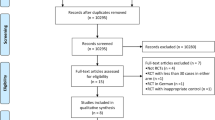
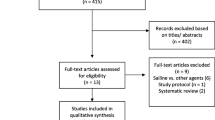
The first electronic search yielded 3759 records. After the evaluation of abstracts, full-texts, and references, 21 potentially relevant papers were identified. Only 8 studies, including a total of 2833 patients, met the inclusion criteria and entered the meta-analysis [8,9,10,11,12,13,14,15], 1441 in the drain group and 1392 in the control group (Fig. 1 depicts our search strategy). In the analysis, the inspection of forest plots and the I2 index revealed a low risk of heterogeneity (I2 = 17%). We performed a quality analysis assessing risk of bias according the Cochrane tool [16] (Fig. 2 depicts risk of bias summary) and we appreciated blinding in the included studies [17].Only one paper reports detailed data showing no blinding of investigators or patients [12].

Flow chart of the search strategy

Risk of bias summary of the included studies
Characteristics of studies and surgical procedures
Three of the included studies were from Europe [8,9,10], two from the USA [13, 15], two from Asia [11, 12], and one from Australia [13]. All patients received an elective open or minimally invasive surgical procedure featuring an opening of GI tract. In all RCTs, suction drains were placed in the primary incision after open surgical procedures or in the incision employed for the anastomosis/specimen extraction after minimally invasive interventions. Overall, there was high variability among surgical procedures; only five studies provided detailed data about surgical procedures [8, 9, 11,12,13] holding 931 patients. In particular, 297 patients (31.9%; 143 drained versus 154 undrained) underwent colorectal and lower GI surgery, 386 patients (41.5%; 192 drained versus 194 undrained) received hepatobiliary and pancreatic surgery, 228 patients (24.5% 122 drained versus 106 undrained) underwent upper GI surgery, and 20 patients (2.1% 11 drained versus 9 undrained) had other GI surgical procedures. Only five studies did provide detailed data on risk factors as immunosuppression, diabetes mellitus (DM), corticosteroids, concomitant, or prior chemoradiotherapy and obesity. [9,10,11,12, 15]. Data about time of drain removal varied significantly among studies. Particularly, the decision to remove drains was made according to the output of the drain [15], to postoperative day (POD) [9, 10, 12,13,14], or a combination thereof [8, 11]. Overall, the median time to drain removal was 3rd POD (range 1–5). In all studies, patients received antibiotic prophylaxis (Table 1).
Outcomes evaluation
Overall, 187 (6.6%) patients had SSI, whereby 83 patients (5.8%) in the drained group and 104 (7.5%) in the undrained group. This difference did not reach statistical significance (OR 0.76, 95% CI 0.56–1.02: p = 0.07; I2 = 17%) (Fig. 3). It has not been possible to meta-analyze data about SSI for type of surgical procedures because of lack of detailed parting within the individual studies. Patients’ general characteristics were similar between the two groups. Of note, overall preoperative risk factors as obesity, immunosuppression, DM, corticosteroids use, and concomitant or prior chemoradiotherapy did not show statistically significant difference between the relative incidences (42% in the drained group versus 38% in the undrained group OR = 1.25, p = 0.10) .

Forest plot showing OR for SSI
Discussion
The role of prophylactic subcutaneous drain has been evaluated by many authors among different types of surgical procedures that tried to answer the question if drained wound give better results in terms of SSI and the different experiences gave variable outcomes. Within GI surgery in the past 30 years, some studies suggest routine placement of subcutaneous suction drain to reduce postoperative SSI [8, 12] but others sustain its irrelevance [9,10,11, 13,14,15]. In contaminated and dirty surgery, such as emergency surgery or ileostomy reversal, wound drain had shown advantage in preventing SSI [18, 19]. Overall, our review does not support the routine use of subcutaneous drain following elective clean-contaminated abdominal surgery, as no statistical difference was noted between drained and undrained patients. Manzoor et al. [1] in their recent review on the use of subcutaneous wound drain after laparotomy conclude that there is no statistical difference between drained and undrained wound and suggest that drain is not necessary for all patients but useful in contaminated wounds. A systematic review and meta-analysis by Kosin et al. [20], analyzing the different types of cutaneous incisions and surgical procedures, concluded that drain is not mandatory also in clean-contaminated surgical procedures. However, in this study, data concerning the type of drain used (if suction or not) were not specified. Our paper aimed to make the sample as homogeneous as possible selecting all RCTs about clean-contaminated surgery with positioning of a suction drain and only in elective setting. To the best of our knowledge, this is the first meta-analysis reporting on the highest-quality evidence on this topic. Nevertheless, some limitations to the present analysis are to be acknowledged. Firstly, the included studies cover a time frame of 30 years during which the attention paid on SSI is changed far, hand in hand with rules and strategies to prevent them. Secondly, a certain variability among studies in terms of surgical procedures and postoperative drain management removal may have, at least in part, modified our results. The included studies in our meta-analysis treat about visceral surgical procedures which have different SSI incidences if separately considered. Due to the lack of detailed grouping within drained and undrained patients in individual studies, it was not possible to calculate difference in SSI for each type of surgical procedure. Finally, the lack of detailed data has prevented a subgroup analysis investigating specific risks for SSI in particular immunosuppression, DM, corticosteroid use, chemoradiotherapy, and obese patients which should be analyzed in specific subgroup. These could have a key role on wound healing and could have influence on the final results. Only one study [15] reports specific data on obese patients, other works analyze obesity as a risk factor without reporting specific data or subgroup. We regroup the risk factors adding them together within the two groups and made the analysis of available data.
Conclusions
According to the highest-quality evidence data in literature, the presence of prophylactic subcutaneous suction drain does not impact significantly on the incidence of SSI in clean-contaminated abdominal surgery. The lack of specific data precludes the possibility to reach definitive conclusions on whether subcutaneous drain may confer advantages in specific subgroups of patients.
References
Manzoor B, Heywood N, Sharma A (2015) Review of subcutaneous wound drainage in reducing surgical site infections after laparotomy. Surg Res Pract 2015:715803
Watanabe A, Kohnoe S, Shimabukuro R, Yamanaka T, Iso Y, Baba H, Higashi H, Orita H, Emi Y, Takahashi I, Korenaga D, Maehara Y (2008) Risk factors associated with surgical site infection in upper and lower gastrointestinal surgery. Surg Today 38(5):404–412
Smith RL, Bohl JK, McElearney ST, Friel CM, Barclay MM, Sawyer RG, Foley EF (2004) Wound infection after elective colorectal resection. Ann Surg 239(5):599–607
Satyanarayana V, Prashanth HV, Bhandare B, Kavyashree AN (2011) Study of surgical site infections in abdominal surgeries. J Clin Diagn Res 5(5):935–939
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. Ann Intern Med 18(151):W65–W94
Goossen K, Tenckhoff S, Probst P, Grummich K, Mihaljevic AL, Büchler MW, Diener MK (2018 Feb) Optimal literature search for systematic reviews in surgery. (2018). Langenbeck's Arch Surg 403(1):119–129
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR (1999) Guideline for prevention of surgical site infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol 20(4):250–278 quiz 279–80
Arer IM, Yabanoglu H, Aytac HO, Ezer A (2016) The effect of subcutaneous suction drains on surgical site infection in open abdominal surgery. A prospective randomized study. Ann Ital Chir 87:49–55
Baier PK, Glück NC, Baumgartner U, Adam U, Fischer A, Hopt UT (2010) Subcutaneous Redon drains do not reduce the incidence of surgical site infections after laparotomy. A randomized controlled trial on 200 patients. Int J Color Dis 25:639–643
Kaya E, Paksoy E, Ozturk E, Sigirli D, Bilgel H (2010) Subcutaneous closed-suction drainage does not affect surgical site infection rate following elective abdominal operations: a prospective randomized clinical trial. Acta Chir Belg 110:457–462
Nakayama H, Takayama T, Okubo T, Higaki T, Midorikawa Y, Moriguchi M, Aramaki O, Yamazaki S (2014) Subcutaneous drainage to prevent wound infection in liver resection: a randomized controlled trial. J Hepatobiliary Pancreat Sci 21:509–517
Watanabe J, Ota M, Kawamoto M, Akikazu Y, Suwa Y, Suwa H, Momiyama M, Ishibe A, Watanabe K, Masui H, Nagahori K (2017) A randomized controlled trial of subcutaneous closed-suction Blake drains for the prevention of incisional surgical site infection after colorectal surgery. Int J Colorectal Dis 32(3):391–398
Farnell MB, Worthington-Self S, Mucha P Jr, Ilstrup DM, McIlrath DC (1986) Closure of abdominal incisions with subcutaneous catheters. A prospective randomized trial. Arch Surg 121:641–648
Lubowski D, Hunt DR (1987) Abdominal wound drainage—a prospective, randomized trial. Med J of Aust 146(3):133–135
Shaffer D, Benotti PN, Bothe A Jr, Jenkins RL, Blackburn GL (1987) A prospective, randomized trial of abdominal wound drainage in gastric bypass surgery. Ann Surg 206:134–137
Higgins JPT, Sterne JAC, Savović J, Page MJ, Hróbjartsson A, Boutron I, et al. (2016) A revised tool for assessing risk of bias in randomized trials In: Chandler J, McKenzie J, Boutron I, Welch V . Cochrane Methods. Cochrane Database of Systematic Reviews, Issue 10 (Suppl 1)
Probst P, Zaschke S, Heger P, Harnoss JC, Hüttner FJ, Mihaljevic AL, Knebel P, Diener MK (2019) Evidence-based recommendations for blinding in surgical trials. Langenbecks Arch Surg 404(3):273–284
Kumar S, Chatterjee S, Gupta S, Satpathy, Chatterjee S, Ray U (2017) Role of subcutaneous closed vacuum drain in preventing surgical site infection in emergency surgery for perforative peritonitis: a randomized control study. Bangladesh J Med Sci 16(1):85–90
Pan HD, Wang L, Peng YF, Li M, Yao YF, Zhao J et al (2015) Subcutaneous vacuum drains reduce surgical site infection after primary closure of defunctioning ileostomy. Int J Color Dis 30(7):977–982
Kosins AM, Scholz T, Cetinkaya M, Evans GRD (2013) Evidence-based value of subcutaneous surgical wound drainage: the largest systematic review and meta-analysis. Plast Reconstr Surg 132(2):443–450
Author information
Authors and Affiliations
Contributions
Study conception and design: DC, CDB, and FG. Acquisition of data: CDB and GG. Analysis and interpretation of data: DC and FG. Drafting of manuscript: DC. Critical revision of manuscript: DC, CDB, GG, and FG.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Not applicable. This article does not contain any studies with human or animal participants performed by any of the authors.
Informed consent
Not applicable. For this type of study, formal consent in not required.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Coletta, D., Del Basso, C., Giuliani, G. et al. Subcutaneous suction drains do not prevent surgical site infections in clean-contaminated abdominal surgery—results of a systematic review and meta-analysis. Langenbecks Arch Surg 404, 663–668 (2019). https://doi.org/10.1007/s00423-019-01813-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-019-01813-x