
Abstract
Purpose
The purpose of the present study was to investigate the effect of high-dose inhaled terbutaline on muscle strength, maximal sprinting, and time-trial performance in trained men.
Methods
Nine non-asthmatic males with a \(\dot{V}O_{2max}\) of 58.9 ± 3.1 ml min−1 kg−1 (mean ± SEM) participated in a double-blinded randomized crossover study. After administration of inhaled terbutaline (30 × 0.5 mg) or placebo, subjects’ maximal voluntary isometric contraction (MVC) of m.quadriceps was measured. After MVC, subjects performed a 30-s Wingate test. Sixty minutes following the Wingate test, subjects exercised for 10 min at 80 % of \(\dot{V}O_{2max}\) and completed a 100-kcal time trial. Aerobic contribution was determined during the Wingate test by indirect calorimetry. Furthermore, plasma terbutaline, lactate, glucose, and K+ were measured.
Results
Inhalation of 15 mg terbutaline resulted in systemic concentrations of terbutaline of 23.6 ± 1.1 ng ml−1 30 min after administration, and elevated plasma lactate (P = 0.001) and glucose (P = 0.007). MVC was higher for terbutaline than placebo (738 ± 64 vs. 681 ± 68 N) (P = 0.007). In addition, Wingate peak power and mean power were 2.2 ± 0.8 (P = 0.019) and 3.3 ± 1.0 % (P = 0.009) higher for terbutaline than placebo. Net accumulation of plasma lactate was higher (P = 0.003) for terbutaline than placebo during the Wingate test, whereas \(\dot{V}O_{2}\) above baseline was unchanged by terbutaline (P = 0.882). Time-trial performance was not different between treatments (P = 0.236).
Conclusion
High-dose inhaled terbutaline elicits a systemic response that enhances muscle strength and sprint performance. High-dose terbutaline should therefore continue to be restricted in competitive sport.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The 2014 World Anti-doping Agency (WADA) prohibited list restricts use of all beta2-agonists, apart from salbutamol, salmeterol, and formoterol that are allowed by inhalation in therapeutic doses within defined therapeutic thresholds (www.wada-ama.org). Other beta2-agonists, such as terbutaline, are only allowed if the athlete acquires a therapeutic use exemption by clinical proof of asthma or exercise-induced bronchoconstriction. While several studies have investigated effects of clinical therapeutic inhalation of beta2-agonists (2–4 puffs) on submaximal, supramaximal, and time-trial performance (Sporer et al. 2008; van Baak et al. 2004; McKenzie et al. 1983; Carlsen et al. 1997; Signorile et al. 1992), effects of supratherapeutic high-dose inhalation of beta2-agonists are inadequately explored. To our knowledge, only one study by Elers et al. (2012b), has investigated the effects of high-dose inhalation of salbutamol (40 × 200 µg) on incremental exercise performance, whereas no studies exist investigating the effects of high-dose inhaled beta2-agonist on muscle strength and supramaximal exercise performance.
Elite athletes commonly use beta2-agonists due to the high prevalence of asthma and exercise-induced bronchoconstriction in the athletic population (McKenzie and Fitch 2011; Helenius et al. 1998; Langdeau et al. 2000). As a consequence of the high use, it is widely debated whether beta2-agonists enhance performance (Backer et al. 2007; Pluim et al. 2011; Wolfarth et al. 2010; Kindermann 2007). While most studies show no ergogenic effects of inhaled beta2-agonists on exercise performance (Wolfarth et al. 2010; Pluim et al. 2011), oral salbutamol increases muscle strength (van Baak et al. 2000), maximal sprint performance (Collomp et al. 2005; Le Panse et al. 2007; Sanchez et al. 2012), and exercise endurance (Collomp et al. 2000; van Baak et al. 2000). The discrepancies between inhaled and oral administration of beta2-agonists on performance are commonly believed to be a consequence of the route of administration (Wolfarth et al. 2010; Sanchez et al. 2012, 2013). However, the studies showing performance-enhancing effects of oral salbutamol administered doses ranging from 4 to 6 mg (Sanchez et al. 2012; van Baak et al. 2000; Collomp et al. 2000), whereas most studies investigating effects of inhaled salbutamol used doses ranging between 200 and 800 µg (Pluim et al. 2011). From a pharmacological viewpoint, lack of performance-enhancing effects after inhalation of beta2-agonists might therefore simply reflect low-dose administration eliciting a limited systemic response. Indeed, Elers et al. (2012a) observed that inhalation of 2 mg terbutaline gave similar systemic concentrations as oral administration of 10 mg terbutaline. Moreover, if calculating the area under the curve (AUC) of the systemic concentrations of terbutaline in the study by Elers et al. (2012a), results indicate a higher systemic bioavailability following inhalation, with AUC being 25.1 ± 5.6 ng ml−1 h after inhalation of 2 mg and 24.6 ± 7.1 ng ml−1 h after oral administration of 10 mg. Schmekel et al. (1992) also observed that the peak systemic concentrations of terbutaline achieved after inhalation of 1 mg terbutaline equivocated with that observed by Bengtsson and Fagerstrom (1982) after administration of 5 mg oral terbutaline (Schmekel et al. 1992; Bengtsson and Fagerstrom 1982). It is therefore possible that supratherapeutic high-dose inhalation of beta2-agonists imposes a similar systemic response as that observed from oral administration (Elers et al. 2012a, c), hence being performance enhancing. In support of this proposition, Kalsen et al. (2013) recently observed that inhalation of three different beta2-agonists in combination increased quadriceps muscle strength and arm ergometer sprint performance in elite swimmers.
Thus, the primary purpose of the present study was to examine systemic effects of high-dose inhaled terbutaline on muscle strength and maximal sprint performance. Secondary objectives were to investigate effects of terbutaline on energy expenditure during submaximal exercise and time-trial performance.
Materials and methods
Subjects
Nine trained males with a maximal oxygen uptake (\(\dot{V}O_{2max}\)) of 58.9 ± 3.1 ml min−1 kg−1 participated in the study. Subjects were recreationally engaged in cycling, running, and resistance training on a non-competitive level. Subject characteristics are presented in Table 1. Subjects had no history of asthma and had never used beta2-agonists. Each subject received oral and written information about the aims and contents of the study and the possible risks involved. Prior to inclusion, subjects gave their oral and written informed consent. The study was performed in accordance with the Helsinki II declaration and was approved by the regional ethics committee of Copenhagen.
Design
The study was designed as a randomized crossover study with two treatment allocations (terbutaline vs. placebo). Before the start of the intervention, subjects performance and \(\dot{V}O_{2max}\) were determined in an incremental exercise test on a bike ergometer (Model 839E, Monark, Stockholm, Sweden) starting at 150 W with a stepwise increase of 30 W every min until exhaustion. During the test, pulmonary gas exchange was measured breath-by-breath with a gas analyzer system (Oxycon Pro, CareFusion, San Diego, USA). Prior to tests, the bike ergometer was calibrated; the saddle height, handlebar height and distance between saddle and handlebar were adjusted to the subjects’ leg and arm lengths. Before start of the test, subjects completed a warm-up at 150 W for 10 min followed by 4 min of recovery. Subjects were told to keep a cadence of 80–90 rpm. Exhaustion was defined as the point where pedaling frequency fell below 70 rpm for more than 5 s despite strong verbal encouragement. \(\dot{V}O_{2max}\) was determined as the highest value recorded in any 30-s period. A plateau in \(\dot{V}O_{2}\) despite an increased power output and a respiratory exchange ratio (RER) above 1.15 were used as criteria for \(\dot{V}O_{2max}\) achievement. After the incremental test, subjects completed the protocol used in the intervention.
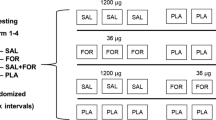
The intervention consisted of two visits (terbutaline vs. placebo) separated by 16.8 ± 2.5 days. The experimental protocol is illustrated in Fig. 1. During each visit, subjects reported to the laboratory and had a catheter inserted in the antecubital vein for venous blood sampling. Afterwards, study drugs, 30 × 0.5 mg inhaled terbutaline (Bricanyl® Turbohaler, AstraZeneca) or 30 puffs of a placebo turbohaler (AstraZeneca, Sweden) were randomly administered during supervision in a double-blinded manner.

Experimental protocol used in the intervention. Subjects inhaled either 30 × 0.5 mg terbutaline (Bricanyl Turbohaler, AstraZeneca) or 30 puffs of a placebo turbohaler (AstraZeneca)
Following administration of study drug, subjects warmed up on a bike ergometer (Model 839E, Monark, Stockholm, Sweden) for 15 min at 150 W followed by a 10-s sprint. After four min, subjects were placed on a table with an adjustable chair back and the right leg fixed in knee and hip joint angles of 90° of flexion and the ankle attached just superior to the malleoli to a strain gauge (Tedea-Huntleigh, United Kingdom). Subjects’ then performed three to four 3- to 4-s maximal voluntary contractions (MVC) with 1 min of rest in between. To ensure that the subjects remained in the same position during the MVC three Velcro strips were tied around the chest, hip and thighs. To reduce day-to-day variation, the exact body position of the subjects was registered and used throughout the entire experiment. Before the MVC measurements, the subjects performed two submaximal isometric contractions at approximately 60 % of MVC for a duration of 5 s.
Six minutes following the MVC, subjects completed a 30-s Wingate test. Wingate protocol was custom-made in Monark 839E analysis software. Subjects would pedal against a passive resistance for 30 s, in which subjects were told to find and maintain a cadence of 80–90 rpm. After 30 s, brake force increased to 0.90 N × kgbw and subjects sprinted as fast as possible for 30 s. Subjects were instructed to remain seated throughout the entire test. Cadence and power output were recorded by a computer with a sampling frequency of 1 Hz. After the test, peak power was calculated as the highest power achieved for 5 consecutive seconds and mean power as the average power output during the 30 s of maximal sprinting. The bike ergometer was calibrated prior to the test. Subjects used same geometric setup, as well as their own pedals and shoes during the test. Pulmonary gas exchange was measured breath-by-breath 4 min prior to the Wingate test up until 60 min following the test. All data were automatically collected within an electronic database with subject ID and date of testing.
In the 60 min following cessation of the Wingate test, subjects rested in a supine position. Blood samples (1 ml) were drawn from the antecubital vein before start of the Wingate test (pre), immediately after the Wingate test (post), and 1, 3, 5, 10, 15, 20, 25, 30, 35, 40, 45, 50, 55, and 60 min following the Wingate for analysis of venous lactate, glucose, and K+.
After the 60 min of rest, subjects warmed up for 4 min at 150 W after which they performed 10 min of submaximal exercise at an intensity corresponding to 80 % of subjects \(\dot{V}O_{2max}\) determined from the incremental test, corresponding to a workload of 266 ± 11 W. When subjects completed the 10-min submaximal exercise, the intensity was set free, and subjects carried on to complete a 100-kcal time trial as fast as possible. Pulmonary gas exchange was measured breath-by-breath during submaximal exercise and time trial for determination of the mean \(\dot{V}O_{2}\), RER, and ventilation during the tests.
Subjects were told to avoid exercise, caffeine, nicotine and alcohol 48 h prior to each visit. Furthermore, subjects registered food and fluid consumed 48 h before the first visit were asked to duplicate this before the second visit.
All subjects completed the study. One subject felt discomfort following the Wingate test and did not complete the submaximal exercise protocol and time trial.
Study medication
Active substance (Terbutaline, Bricanyl Turbohaler 0.5 mg) was delivered by the Pharmacy of RegionH, Copenhagen, Denmark. Inhaled terbutaline has been shown to be quickly absorbed, reaching peak systemic concentrations (C max) 30 min (T max) following administration (Elers et al. 2012a). The onset of action of inhaled terbutaline is within a few minutes with a duration of action of up to 6 h (datasheet, Bricanyl® Turbohaler, AstraZeneca). Placebo turbohalers were kindly delivered by AstraZeneca, Sweden. A blood sample was drawn 30 min following administration of study drug to determine systemic concentrations of terbutaline and to confirm randomization. Concentrations of terbutaline were analyzed by the WADA accredited doping control laboratory in Norway (Norwegian Doping Control Laboratory) at Oslo University Hospital. Samples were shipped (World Courier) on dry ice from Copenhagen. Concentrations of terbutaline in serum were analyzed by liquid chromatography-tandem mass spectrometry (LC–MS/MS) as described by Elers et al. (2012a). A person with no involvement in other parts of the experimental procedures administered the study drugs. Subjects were familiar with the side effects of terbutaline. Randomization procedures were performed in Microsoft Excel (Microsoft, Redmond, WA, US). Upon completion of the study, each subject was asked about side effects. Seven out of nine subjects reported tremor and tachycardia after terbutaline.
Calculations
Net accumulation of plasma lactate was calculated as the difference between the lactate concentration before the Wingate test (pre) and the peak lactate concentration after the Wingate test. Lactate area under the curve (AUCPRE-15 min) was calculated by the trapezoidal rule as the integral of the plasma lactate concentrations plotted against time points before the Wingate test (pre) and sampling points until 15 min after the Wingate test. Aerobic contribution during the Wingate test was calculated as the mean \(\dot{V}O_{2}\) during the test subtracted by the baseline \(\dot{V}O_{2}\) immediately before the start of the test.
Statistical analysis
Statistical analysis and randomization were performed with SPSS 22.0 software (IBM Software, Chicago, Illinois, USA). Data were tested for normality by a Sharipo–Wilk test and Q–Q plots. Data were normally distributed and are presented in mean ± standard error of the mean (SEM). Effects of terbutaline on Wingate peak power and mean power, quadriceps muscle strength, time-trial performance, aerobic energy contribution, net accumulation of plasma lactate and lactate AUC(PRE-15 min) were tested with a paired t test. Differences in plasma lactate, glucose, and K+ between terbutaline and placebo were tested in a repeated measure analysis of variance (ANOVA) with treatment and time as the two factors. In case of a significant ANOVA, a Bonferroni post hoc test was used.
Results
Systemic concentrations of terbutaline
Serum terbutaline was 23.6 ± 1.1 and 0.0 ± 0.0 ng ml−1 30 min after administration of terbutaline and placebo, respectively.
Quadriceps muscle strength and Wingate power output
Terbutaline enhanced quadriceps muscle strength by 8.4 ± 3.0 % compared with placebo (P = 0.007) (Fig. 2a). Wingate peak power and mean power increased by 2.2 ± 0.8 (P = 0.019) and 3.3 ± 1.0 % (P = 0.009) following inhalation of terbutaline compared with placebo (Fig. 3a). Terbutaline increased total work during the Wingate test compared with placebo, being 21.9 ± 0.7 kJ for terbutaline and 21.2 ± 0.7 kJ for placebo (P = 0.009).

Maximal voluntary contraction after inhalation of terbutaline or placebo. a Mean ± SEM of all subjects. **Different (P < 0.01) from placebo. b Representative recordings from one subject

Wingate power output after inhalation of terbutaline (filled bars) or placebo (open bars) (n = 9). a Mean ± SEM of all subjects. *Different (P < 0.05) from placebo. **Different (P < 0.01) from placebo. b Representative recordings from one subject
Aerobic contribution and lactate accumulation during the Wingate test
Terbutaline elevated baseline \(\dot{V}O_{2}\) compared with placebo (752 ± 49 vs. 660 ± 37 ml min−1) (P = 0.006). \(\dot{V}O_{2}\) above baseline during the Wingate test was not different between treatments, being 2,287 ± 115 ml min−1 for terbutaline and 2,278 ± 134 ml min−1 for placebo (P = 0.882).
Terbutaline elevated net accumulation of plasma lactate compared with placebo (12.1 ± 0.7 vs. 10.9 ± 0.6 mmol l−1) (P = 0.003). Lactate AUC(PRE-15 min) was larger for terbutaline than placebo, being 198 ± 14 mmol l−1 min for terbutaline and 162 ± 9 mmol l−1 min for placebo (P < 0.001).
Measurements of pulmonary gas exchange during submaximal exercise at 80 % of \(\dot{V}O_{2max}\)
Terbutaline elevated \(\dot{V}O_{2}\) during submaximal exercise compared with placebo (3,852 ± 163 vs. 3,740 ± 149 ml min−1) (P = 0.015). RER was not different between treatments, being 0.98 ± 0.01 for terbutaline and 1.00 ± 0.02 for placebo (P = 0.185). Mean ventilation tended to be higher during submaximal exercise for terbutaline than placebo (120 ± 8 vs. 115 ± 8 l min−1) (P = 0.077).
Time-trial performance with measurements of pulmonary gas exchange
Time-trial performance did not differ between treatments, being 293 ± 15 and 286 ± 14 s for terbutaline and placebo, respectively (P = 0.236). RER was lower for terbutaline than placebo during the time trial (0.97 ± 0.02 vs. 1.02 ± 0.02) (P = 0.009). \(\dot{V}O_{2}\) was not different between treatments during the time trial (P = 0.905).
Plasma lactate, glucose, and K+
Terbutaline elevated plasma lactate (f = 27.80, P = 0.001) and glucose (f = 14.48, P = 0.007), and lowered plasma K+ (ƒ = 14.90, P = 0.006) during the Wingate test and in the recovery period following the Wingate test compared with placebo (Fig. 4a–c). Likewise, terbutaline elevated plasma lactate (ƒ = 25.56, P = 0.001) and glucose (ƒ = 21.00, P = 0.003), and lowered plasma K+ (ƒ = 37.84, P < 0.001) before, during and after submaximal exercise at 80 % of \(\dot{V}O_{2max}\) and time trial compared with placebo (Fig. 4d–f).

Plasma concentrations of lactate, K+ and glucose after inhalation of terbutaline (solid circles) or placebo (open circles) (n = 8). Plasma lactate (a), K+ (b) and glucose (c) before and after the Wingate test. Terbutaline elevated plasma lactate (ƒ = 27.80, P = 0.001) and glucose (ƒ = 14.48, P = 0.007), and lowered plasma K+ (ƒ = 14.90, P = 0.006). Plasma lactate (d), K+ (e) and glucose (f) before, during and after submaximal exercise at 80 % of \(\dot{V}O_{2max}\) and 100 kcal time trial. Terbutaline elevated plasma lactate (ƒ = 25.56, P = 0.001) and glucose (ƒ = 21.00, P = 0.003), and lowered plasma K+ (ƒ = 37.84, P < 0.001). *Different (P < 0.05) from placebo. **Different (P < 0.01) from placebo. Mean ± SEM
Discussion
To our knowledge, the present study is the first to investigate performance-enhancing effects of high-dose inhaled terbutaline (30 × 0.5 mg). The most important findings of the present study were that high-dose inhaled terbutaline elicited a high systemic response that increased muscle strength and enhanced power output during a Wingate test, whereas no effect was observed on time-trial performance.
The high-dose inhaled terbutaline administered in the present study resulted in high systemic concentrations of terbutaline (23.6 ± 1.1 ng ml−1) 30 min following administration. Noteworthy, the systemic concentrations observed were 4 times higher than that observed by Elers et al. (2012a) after oral administration of 10 mg terbutaline with reported peak systemic concentrations of only 6.2 ± 4.8 ng ml−1 (median ± interquartile range). Likewise, we observed several indications of systemic effects of inhaled terbutaline, including elevated \(\dot{V}O_{2}\) at rest and during submaximal exercise at 80 % of \(\dot{V}O_{2max}\), along with lowered systemic concentrations of K+ and elevated concentrations of glucose and lactate. Therefore, our data indicate that high-dose inhaled terbutaline elicits a significant systemic response.
We observed enhanced Wingate peak power and mean power with high-dose inhaled terbutaline. A well-known effect of oral salbutamol (4–6 mg) is enhanced peak power and mean power during 30-s maximal bike ergometer sprinting (Collomp et al. 2005; Le Panse et al. 2007; Sanchez et al. 2012). However, Sanchez et al. (2013) recently observed no effects of 8 mg oral terbutaline on maximal power output during 4 s of maximal sprinting on a bike ergometer. The inconsistency between the present study and the study by Sanchez et al. (2013) on sprinting peak power may be a consequence of dose and systemic response. As such, the 8 mg oral terbutaline administered by Sanchez et al. (2013) would approximately give systemic concentrations of 5–6 ng ml−1, being much lower than those observed in the present study. Moreover, Sanchez et al. (2013) observed side effects in several of their subjects, which also could explain the discrepancy. Nevertheless, our observations of higher Wingate power output after inhalation of high-dose terbutaline are also consistent with recent findings from Kalsen et al. (2013) in which inhalation of three different beta2-agonists in combination increased arm ergometer sprint performance in elite swimmers (Kalsen et al. 2013). Furthermore, Decorte et al. (2013) recently observed increased quadriceps muscle endurance following inhalation of 800 µg salbutamol (Decorte et al. 2013). Based on the present study along with the studies by Decorte et al. (2013) and Kalsen et al. (2013), supratherapeutic inhalation of beta2-agonists elicits a high systemic response that can be performance enhancing. In future studies, it would therefore be interesting to examine whether lower doses of inhaled terbutaline or salbutamol could increase supramaximal performance. Indeed, Signorile et al. (1992) found that inhaled albuterol (360 µg) enhanced power output during four 15-s maximal sprints in healthy males and females.
Despite increased mean power and total work with terbutaline during the Wingate test, we observed no differences in the aerobic contribution between treatments, indirectly suggesting a larger anaerobic contribution with terbutaline. Likewise, terbutaline elevated net accumulation of plasma lactate and lactate AUC(PRE-15 min) by 1.2 ± 0.3 mmol l−1 and 36 ± 6 mmol l−1 min compared with placebo during the Wingate test. As lactate AUC(PRE-15 min) reflects the average concentration of plasma lactate during and up until 15 min after the Wingate test, the large difference in lactate AUC(PRE-15 min) observed between treatments indicates an apparent effect of terbutaline on anaerobic lactic acid production of exercising muscles. This observation might reflect adrenergic effects of terbutaline on skeletal muscle glycolytic rate through regulation of glycolytic enzymes. Infusion of epinephrine with adrenergic actions on alpha- and beta2-adrenoceptors has thus been shown to elevate glycolytic activity of skeletal muscles during exercise through regulation of glycolytic enzymes (Watt et al. 2001; Gomes Alves and Sola-Penna 2003; Kjaer et al. 2000). A larger anaerobic energy production from glycolytic formation of lactate may as such partly explain the improved mean power during the Wingate test observed with terbutaline in the present study. Future studies should elaborate on the present and previous findings with measurements of lactate and other glycolytic metabolites from muscle biopsies of exercising subjects.
Apart from beta2-adrenergic actions on rate of glycolysis, enhancing effects of beta2-agonist on sprinting peak power and mean power have been suggested to be attributed to improved Ca2+ handling from the sarcoplasmic reticulum of skeletal muscles mediated by cAMP-dependent phosphorylation of proteins associated with the sarcoplasmic reticulum (Sanchez et al. 2012; Kalsen et al. 2013; Collomp et al. 2005). Indeed, in animal models, beta2-adrenergic stimulation increases contractile force through a larger Ca2+ release and fastens rate of force relaxation through increased Ca2+ uptake (Andersson et al. 2012; Slack et al. 1997; Rudolf et al. 2006; Cairns and Dulhunty 1993b). During dynamic contractions, such as sprinting, improved Ca2+ dynamics might benefit coordination of muscle contraction and relaxation (Seebacher et al. 2012) thus explaining the improved sprint performance with beta2-agonist (Crivelli et al. 2013). In support of the latter, Crivelli et al. (2011) has shown that rate of force relaxation is faster after administration of oral salbutamol (6 mg) in humans. Moreover, beta2-agonists have been shown to counteract contraction-induced accumulation of extracellular K+ through stimulation of Na+/K+-ATPase-activity, thus protecting against muscle fatigue caused by membrane inexcitability (Cairns and Dulhunty 1994; Clausen and Flatman 1980; Juel 1988). However, in humans, M-wave amplitudes have been shown to be unaltered by administration of beta2-agonists, suggesting unchanged sarcolemma excitability (Crivelli et al. 2011, 2013). Nevertheless, it is unclear whether the muscular effects of beta2-agonists observed in animal models also apply to humans and studies investigating these effects in humans are thus warranted.
We observed enhanced quadriceps muscle strength following inhalation of high-dose inhaled terbutaline. Enhancement in muscle strength in the present study was similar with that observed by Kalsen et al. (2013) showing increased quadriceps muscle strength following inhalation of three different beta2-agonists in elite swimmers (Kalsen et al. 2013). Furthermore, oral administration of 4 mg salbutamol was shown to increase isokinetic muscle strength in male subjects (van Baak et al. 2000). Nevertheless, it is important to emphasize that other studies did not find an effect of neither oral terbutaline (8 mg) nor oral salbutamol (6 mg) on muscle strength (Crivelli et al. 2011, 2013). Moreover, Decorte et al. (2008) found no effect of 200 and 800 µg inhaled salbutamol on quadriceps contractile force, although a non-significant increase of 22 ± 34 % in quadriceps twitch force was observed with 800 µg salbutamol (Decorte et al. 2008). Effects of beta2-agonist on muscle strength may therefore, apart from the dose administered, be dependent on the training status of the included subjects and the muscle group involved. Indeed, the observations by Crivelli et al. (2013) would suggest a weakening effect of oral terbutaline (8 mg) on the contractile machinery of the predominantly slow twitch muscle m. soleus, thus contrasting with that observed by the same researchers when investigating m. quadriceps (Crivelli et al. 2011). In addition, van Baak et al. (2004) observed that the ergogenic response to 800 µg inhaled salbutamol was highest in the subjects with the poorest performance. Since beta2-adrenoceptor content is lower in athletic subjects than in non-athletic (Butler et al. 1982), training status may as such influence the response toward beta2-agonists. In any case, animal models suggest that enhancements in contractile force elicited by beta2-agonists are caused by higher amplitudes of Ca2+ transients from the sarcoplasmic reticulum, thus elevating availability of Ca2+ for troponin C (Cairns and Dulhunty 1993a; Andersson et al. 2012). Still, these effects are unexplored in humans.
Although high-dose inhaled terbutaline elicited a significant systemic response, we observed no effect of terbutaline on 100 kcal time-trial performance. As the duration of action of inhaled terbutaline is up to 6 h and that the half-life of terbutaline is 11–16 h, we are confident that the lack of an effect of terbutaline on time-trial performance was not due to the 90 min that had surpassed since administration of the study drug. Moreover, plasma glucose and lactate were still elevated by terbutaline immediately prior to and during the time trial, and \(\dot{V}O_{2}\) was elevated with terbutaline during the 10-min submaximal exercise at 80 % of \(\dot{V}O_{2max}\) preceding the time trial. On the contrary, to the present observations, oral salbutamol (4–6 mg) has been shown to improve bike ergometer exercise performance at intensities ranging from 70 to 85 % of \(\dot{V}O_{2max}\) (Collomp et al. 2000; van Baak et al. 2000). It has been suggested that performance enhancements associated with oral salbutamol are attributed to higher systemic availability of circulating glucose and increased glycolytic activity in skeletal muscles (van Baak et al. 2000; Arlettaz et al. 2009; Collomp et al. 2000). However, while our plasma lactate data indicate elevated anaerobic energy production from exercising muscles with terbutaline, our observations show that terbutaline is without an effect on time-trial performance and may even have a negative impact on submaximal exercise performance by elevating energy expenditure (i.e., higher \(\dot{V}O_{2}\)). Another possibility for the discrepancy on performance might be related to side effects associated with high-dose beta2-agonist. Side effects have been suggested to play a negative role on performance in some subjects, thus blunting a potential ergogenic effect of beta2-agonists (van Baak et al. 2000; Sanchez et al. 2013). Nevertheless, despite seven out of nine subjects reported minor side effects (tachycardia and tremor) in the present study, we observed no association between reported side effects and performance during the time trial. Our observations are also consistent with previous studies showing no performance-enhancing effects of inhalation of neither salbutamol nor terbutaline in different test protocols, varying from time trials (Sporer et al. 2008; Norris et al. 1996) to incremental (Elers et al. 2012b) and submaximal bike ergometer tests to exhaustion (Pluim et al. 2011; Goubault et al. 2001; Sandsund et al. 1998). Furthermore, Carlsen et al. (1997) even observed reduced endurance performance after inhalation of 800 µg salbutamol. Likewise, Heir and Stemshaug (1995) reported a close to significant reduction in endurance time at 110 % of \(\dot{V}O_{2max}\) following nebulization of 0.05 mg kg−1 salbutamol (Carlsen et al. 1997; Heir and Stemshaug 1995). Nonetheless, the recent studies by Decorte et al. (2013) and Kalsen et al. (2013) could suggest that effects of beta2-agonists might vary depending on the muscle groups activated (i.e., whole-body exercise vs. isolated muscle contractions). Indeed, quadriceps muscle endurance was shown by Decorte et al. (2013) to be increased with inhalation of 800 µg salbutamol during incremental and localized fatiguing submaximal contractions in endurance-trained athletes. Lastly, as discussed above, the administered dose along with training status of included subjects and muscle type investigated might explain some of the discrepancies in the literature. Future studies are thus needed investigating the effects of beta2-agonists on localized and whole-body exercise performance in other setups before any conclusions can be drawn.
Conclusions
In summary, high-dose inhaled terbutaline leads to high systemic concentrations of terbutaline, causing elevated \(\dot{V}O_{2}\) at rest and during submaximal exercise at 80 % of \(\dot{V}O_{2max}\) along with lowered systemic concentrations of K+ and elevated concentrations of glucose and lactate. Furthermore, high-dose inhalation of terbutaline increases Wingate power output and quadriceps muscle strength. Higher Wingate mean power elicited by high-dose inhaled terbutaline is associated with elevated anaerobic energy production as terbutaline elevated net accumulation of plasma lactate during the Wingate test with no changes in aerobic contribution. High-dose inhaled terbutaline has no effect on 100 kcal time-trial performance. As high-dose inhalation of terbutaline gave side effects and enhanced Wingate power output and quadriceps muscle strength, the present observations support WADA’s restriction of terbutaline on the list of prohibited substances.
Abbreviations
- ANOVA:
-
Analysis of the variance
- AUC:
-
Area under the curve
- MVC:
-
Maximal voluntary Contraction
- RER:
-
Respiratory exchange ratio
- \(\dot{V}O_{2}\) :
-
Oxygen uptake
- \(\dot{V}O_{2max}\) :
-
Maximal oxygen uptake
- WADA:
-
World Anti-doping Agency
References
Andersson DC, Betzenhauser MJ, Reiken S, Umanskaya A, Shiomi T, Marks AR (2012) Stress-induced increase in skeletal muscle force requires protein kinase A phosphorylation of the ryanodine receptor. J Physiol 590(Pt 24):6381–6387. doi:10.1113/jphysiol.2012.237925
Arlettaz A, Le Panse B, Portier H, Lecoq AM, Thomasson R, De Ceaurriz J, Collomp K (2009) Salbutamol intake and substrate oxidation during submaximal exercise. Eur J Appl Physiol 105(2):207–213. doi:10.1007/s00421-008-0891-7
Backer V, Lund T, Pedersen L (2007) Pharmaceutical treatment of asthma symptoms in elite athletes-doping or therapy? Scand J Med Sci Sports 17(6):615–622. doi:10.1111/j.1600-0838.2007.00711.x
Bengtsson B, Fagerstrom PO (1982) Extrapulmonary effects of terbutaline during prolonged administration. Clin Pharmacol Ther 31(6):726–732
Butler J, O’Brien M, O’Malley K, Kelly JG (1982) Relationship of beta-adrenoreceptor density to fitness in athletes. Nature 298(5869):60–62
Cairns SP, Dulhunty AF (1993a) Beta-adrenergic potentiation of E-C coupling increases force in rat skeletal muscle. Muscle Nerve 16(12):1317–1325. doi:10.1002/mus.880161208
Cairns SP, Dulhunty AF (1993b) The effects of beta-adrenoceptor activation on contraction in isolated fast- and slow-twitch skeletal muscle fibres of the rat. Br J Pharmacol 110(3):1133–1141
Cairns SP, Dulhunty AF (1994) Beta-adrenoceptor activation shows high-frequency fatigue in skeletal muscle fibers of the rat. Am J Physiol 266(5 Pt 1):C1204–C1209
Carlsen KH, Ingjer F, Kirkegaard H, Thyness B (1997) The effect of inhaled salbutamol and salmeterol on lung function and endurance performance in healthy well-trained athletes. Scand J Med Sci Sports 7(3):160–165
Clausen T, Flatman JA (1980) Beta 2-adrenoceptors mediate the stimulating effect of adrenaline on active electrogenic Na-K-transport in rat soleus muscle. Br J Pharmacol 68(4):749–755
Collomp K, Candau R, Collomp R, Carra J, Lasne F, Prefaut C, De Ceaurriz J (2000) Effects of acute ingestion of salbutamol during submaximal exercise. Int J Sports Med 21(7):480–484. doi:10.1055/s-2000-7422
Collomp K, Le Panse B, Portier H, Lecoq AM, Jaffre C, Beaupied H, Richard O, Benhamou L, Courteix D, De Ceaurriz J (2005) Effects of acute salbutamol intake during a Wingate test. Int J Sports Med 26(7):513–517. doi:10.1055/s-2004-821223
Crivelli G, Millet GP, Gremion G, Borrani F (2011) Effects of salbutamol on the contractile properties of human skeletal muscle before and after fatigue. Acta Physiol (Oxf) 203(2):311–320. doi:10.1111/j.1748-1716.2011.02302.x
Crivelli G, Borrani F, Capt R, Gremion G, Maffiuletti NA (2013) Actions of beta2-Adrenoceptor Agonist Drug on Human Soleus Muscle Contraction. Med Sci Sports Exerc. doi:10.1249/MSS.0b013e318284706a
Decorte N, Verges S, Flore P, Guinot M, Wuyam B (2008) Effects of acute salbutamol inhalation on quadriceps force and fatigability. Med Sci Sports Exerc 40(7):1220–1227. doi:10.1249/MSS.0b013e31816b87aa
Decorte N, Bachasson D, Guinot M, Flore P, Levy P, Verges S, Wuyam B (2013) Impact of Salbutamol on Neuromuscular Function in Endurance Athletes. Med Sci Sports Exerc. doi:10.1249/MSS.0b013e3182951d2d
Elers J, Hostrup M, Pedersen L, Henninge J, Hemmersbach P, Dalhoff K, Backer V (2012a) Urine and serum concentrations of inhaled and oral terbutaline. Int J Sports Med 33(12):1026–1033. doi:10.1055/s-0032-1311590
Elers J, Morkeberg J, Jansen T, Belhage B, Backer V (2012b) High-dose inhaled salbutamol has no acute effects on aerobic capacity or oxygen uptake kinetics in healthy trained men. Scand J Med Sci Sports 22(2):232–239. doi:10.1111/j.1600-0838.2010.01251.x
Elers J, Pedersen L, Henninge J, Hemmersbach P, Dalhoff K, Backer V (2012c) The pharmacokinetic profile of inhaled and oral salbutamol in elite athletes with asthma and nonasthmatic subjects. Clin J Sport Med Off J Can Acad Sport Med 22(2):140–145. doi:10.1097/JSM.0b013e31823513e1
Gomes Alves G, Sola-Penna M (2003) Epinephrine modulates cellular distribution of muscle phosphofructokinase. Mol Genet Metab 78(4):302–306
Goubault C, Perault MC, Leleu E, Bouquet S, Legros P, Vandel B, Denjean A (2001) Effects of inhaled salbutamol in exercising non-asthmatic athletes. Thorax 56(9):675–679
Heir T, Stemshaug H (1995) Salbutamol and high-intensity treadmill running in nonasthmatic highly conditioned athletes. Scand J Med Sci Sports 5(4):231–236
Helenius IJ, Tikkanen HO, Sarna S, Haahtela T (1998) Asthma and increased bronchial responsiveness in elite athletes: atopy and sport event as risk factors. J Allergy Clin Immunol 101(5):646–652. doi:10.1016/S0091-6749(98)70173-3
Juel C (1988) The effect of beta 2-adrenoceptor activation on ion-shifts and fatigue in mouse soleus muscles stimulated in vitro. Acta Physiol Scand 134(2):209–216. doi:10.1111/j.1748-1716.1988.tb08481.x
Kalsen A, Hostrup M, Bangsbo J, Backer V (2013) Combined inhalation of beta-agonists improves swim ergometer sprint performance but not high-intensity swim performance. Scand J Med Sci Sports. doi:10.1111/sms.12096
Kindermann W (2007) Do inhaled beta(2)-agonists have an ergogenic potential in non-asthmatic competitive athletes? Sports Med 37(2):95–102
Kjaer M, Howlett K, Langfort J, Zimmerman-Belsing T, Lorentsen J, Bulow J, Ihlemann J, Feldt-Rasmussen U, Galbo H (2000) Adrenaline and glycogenolysis in skeletal muscle during exercise: a study in adrenalectomised humans. J Physiol 528(Pt 2):371–378
Langdeau JB, Turcotte H, Bowie DM, Jobin J, Desgagne P, Boulet LP (2000) Airway hyperresponsiveness in elite athletes. Am J Respir Crit Care Med 161(5):1479–1484. doi:10.1164/ajrccm.161.5.9909008
Le Panse B, Arlettaz A, Portier H, Lecoq AM, De Ceaurriz J, Collomp K (2007) Effects of acute salbutamol intake during supramaximal exercise in women. Br J Sports Med 41(7):430–434. doi:10.1136/bjsm.2006.033845
McKenzie DC, Fitch KD (2011) The asthmatic athlete: inhaled Beta-2 agonists, sport performance, and doping. Clin J Sport Med Off J Can Acad Sport Med 21(1):46–50. doi:10.1097/IAE.0b013e318203c0ef
McKenzie DC, Rhodes EC, Stirling DR, Wiley JP, Dunwoody DW, Filsinger IB, Jang F, Stevens A (1983) Salbutamol and treadmill performance in non-atopic athletes. Med Sci Sports Exerc 15(6):520–522
Norris SR, Petersen SR, Jones RL (1996) The effect of salbutamol on performance in endurance cyclists. Eur J Appl Physiol 73(3–4):364–368
Pluim BM, de Hon O, Staal JB, Limpens J, Kuipers H, Overbeek SE, Zwinderman AH, Scholten RJ (2011) Beta (2)-Agonists and physical performance: a systematic review and meta-analysis of randomized controlled trials. Sports Med 41(1):39–57. doi:10.2165/11537540-000000000-00000
Rudolf R, Magalhaes PJ, Pozzan T (2006) Direct in vivo monitoring of sarcoplasmic reticulum Ca2+ and cytosolic cAMP dynamics in mouse skeletal muscle. J Cell Biol 173(2):187–193. doi:10.1083/jcb.200601160
Sanchez AM, Collomp K, Carra J, Borrani F, Coste O, Prefaut C, Candau R (2012) Effect of acute and short-term oral salbutamol treatments on maximal power output in non-asthmatic athletes. Eur J Appl Physiol 112(9):3251–3258. doi:10.1007/s00421-011-2307-3
Sanchez AM, Borrani F, Le Fur MA, Le Mieux A, Lecoultre V, Py G, Gernigon C, Collomp K, Candau R (2013) Acute supra-therapeutic oral terbutaline administration has no ergogenic effect in non-asthmatic athletes. Eur J Appl Physiol 113(2):411–418. doi:10.1007/s00421-012-2447-0
Sandsund M, Sue-Chu M, Helgerud J, Reinertsen RE, Bjermer L (1998) Effect of cold exposure (−15 degrees C) and salbutamol treatment on physical performance in elite nonasthmatic cross-country skiers. Eur J Appl Physiol 77(4):297–304
Schmekel B, Borgstrom L, Wollmer P (1992) Exercise increases the rate of pulmonary absorption of inhaled terbutaline. Chest 101(3):742–745
Seebacher F, Pollard SR, James RS (2012) How well do muscle biomechanics predict whole-animal locomotor performance? The role of Ca2 + handling. J Exp Biol 215(Pt 11):1847–1853. doi:10.1242/jeb.067918
Signorile JF, Kaplan TA, Applegate B, Perry AC (1992) Effects of acute inhalation of the bronchodilator, albuterol, on power output. Med Sci Sports Exerc 24(6):638–642
Slack JP, Grupp IL, Luo W, Kranias EG (1997) Phospholamban ablation enhances relaxation in the murine soleus. Am J Physiol 273(1 Pt 1):C1–C6
Sporer BC, Sheel AW, McKenzie DC (2008) Dose response of inhaled salbutamol on exercise performance and urine concentrations. Med Sci Sports Exerc 40(1):149–157. doi:10.1249/mss.0b013e3181591df7
van Baak MA, Mayer LH, Kempinski RE, Hartgens F (2000) Effect of salbutamol on muscle strength and endurance performance in nonasthmatic men. Med Sci Sports Exerc 32(7):1300–1306
van Baak MA, de Hon OM, Hartgens F, Kuipers H (2004) Inhaled salbutamol and endurance cycling performance in non-asthmatic athletes. Int J Sports Med 25(7):533–538. doi:10.1055/s-2004-815716
Watt MJ, Howlett KF, Febbraio MA, Spriet LL, Hargreaves M (2001) Adrenaline increases skeletal muscle glycogenolysis, pyruvate dehydrogenase activation and carbohydrate oxidation during moderate exercise in humans. J Physiol 534(Pt 1):269–278
Wolfarth B, Wuestenfeld JC, Kindermann W (2010) Ergogenic effects of inhaled beta2-agonists in non-asthmatic athletes. Endocrinol Metab Clin North Am 39 (1):75–87, ix. doi:10.1016/j.ecl.2009.10.005
Acknowledgments
The study was supported by a grant from the World Anti-doping Agency (WADA).
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Nicolas Place.
Rights and permissions
About this article

Cite this article
Hostrup, M., Kalsen, A., Bangsbo, J. et al. High-dose inhaled terbutaline increases muscle strength and enhances maximal sprint performance in trained men. Eur J Appl Physiol 114, 2499–2508 (2014). https://doi.org/10.1007/s00421-014-2970-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-014-2970-2