
Abstract
In order to test the hypothesis that salbutamol would change substrate oxidation during submaximal exercise, eight recreationally trained men twice performed 1 h at 60% VO2 peak after ingestion of placebo or 4 mg of salbutamol. Gas exchange was monitored and blood samples were collected during exercise for GH, ACTH, insulin, and blood glucose and lactate determination. With salbutamol versus placebo, there was no significant difference in total energy expenditure and substrate oxidation, but the substrate oxidation balance was significantly modified after 40 min of exercise. ACTH was significantly decreased with salbutamol during the last 10 min of exercise, whereas no difference was found between the two treatments in the other hormonal and metabolic parameters. The theory that the ergogenic effect of salbutamol results from a change in substrate oxidation has little support during relatively short term endurance exercise, but it is conceivable that longer exercise duration can generate positive findings.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Beta-2 adrenergic agonists are drugs that are used frequently for the prevention of exercise-induced asthma. Due to the fear of the ergogenic doping effects demonstrated after both acute (Van Baak et al. 2000; Collomp et al. 2000a, 2002; Le Panse et al. 2007) and chronic (Collomp et al. 2000b; Le Panse et al. 2005, 2006) systemic abuse, the World antidoping agency (WADA) has put certain restrictions upon the use of beta-2 agonists and presently list four beta-agonists (i.e., salbutamol, terbutaline, formoterol and salmeterol) as a legal medication, permitted in the aerosol form only with a abbreviated therapeutic use exemption (TUE), whereas systemic use is completely banned.
However, mechanism(s) implicated in the performance improvement obtained after systemic abuse remained largely unknown, especially during endurance exercise. A possible explanation is a beta-adrenergic stimulation on energy expenditure with increase in fat and/or carbohydrate oxidation during submaximal exercise. Indeed, beta-2 agonists are known to increase at rest energy and fat metabolism (Schiffelers et al. 1999, 2001; Hoeks et al. 2003).
In a previous paper (Collomp et al. 2000a), the effects of acute oral salbutamol intake (6 mg) on performance and metabolism during submaximal exercise were assessed at a power corresponding to 80–85% VO2 max. Cycling performance was significantly improved with salbutamol, with concomitant higher exercise lactate and free fatty acid (FFA) concentrations during the last part of exercise. However, Van Baak et al. tested the effects of both acute salbutamol intake (4 mg) (Van Baak et al. 2000) and of a supra-therapeutic salbutamol inhalation dose (800 μg) (Van Baak et al. 2004) and also reported improvement in performance without any significant change in FFA during exercise performed, respectively at 70% W max and during another trial where the subjects had to perform a certain amount of work as fast as possible on a cycle ergometer. Blood lactate concentrations appear either increased in the first study (Van Baak et al. 2000) aforementioned (70% W max) or unchanged in the 2nd study mentioned (Van Baak et al. 2004).
However, to our knowledge, no published study has investigated the impact of acute salbutamol intake on energy expenditure and substrate oxidation during exercise in humans. Therefore, in order to provide a more precise insight into the influence of salbutamol intake on exercise energy metabolism and regulation, eight healthy recreationally trained men twice performed in a fasting state submaximal exercise (1 h at a power corresponding to 60% VO2 peak) after ingestion of placebo or 4 mg of salbutamol, according to a double blind and randomized protocol. Gas exchange was monitored for calculation of carbohydrate (CHO) and fat oxidation rates as well as energy cost and blood samples were collected during exercise for GH, ACTH, insulin, blood glucose and lactate determination.
Methods
Subjects
Eight healthy moderately trained men participated in this study. Their mean (and SE) age, mass, and peak oxygen consumption were 22.9 (1.4) year, 69.6 (1.9) kg, and 4.09 (0.33) L min−1, respectively. All subjects were physically active and trained three times per week in various sports such as athletics, cycling and ball-games for at least 3 years. They were asked not to change their dietary habits or their physical activity during the entire test period. They were also asked to refrain from vigorous exercise and to abstain from alcohol and caffeine for a minimum of 24 h before each laboratory visit to avoid eventual interactions. The test subject sample size was determined on the basis of a previous study in our laboratory (Arlettaz et al. 2008). We estimated that eight subjects would be sufficient to detect a significant between treatment difference in energy expenditure and substrate oxidation.
The subjects were screened by medical history and physical examination to exclude those subjects with a history of bronchospasm or atopy. Exclusion criteria were respiratory tract infection during the previous month, regular use of tobacco, regular use of any medical drug, recognized asthma or allergy during the 5 years prior to the study, or a restriction in forced expiratory volume during 1-s (FEV1) of more than 10% after the incremental maximal exercise performed in the month before the experiment.
The protocol was approved by the Ethics Committee of Tours Hospital. Each subject signed a consent form that outlined possible risks due to the procedure, being informed of the nature of the experiments.
Exercise
All the subjects had previously participated in physical exercise experiments in the laboratory. In the month before the first treatment, an incremental test for maximum oxygen uptake (VO2 peak) was conducted on a Monark cycle ergometer (model 918E, Monark-Crescent AB, Varberg, Sweden), following a standard laboratory procedure. The exercise test consisted of 3 min of cycling at 50 W followed by a progressive increase in exercise intensity whereby the work rate was increased as a ramp function (20–30 W/min) to volitional fatigue. The highest VO2 averaged over a 10-s interval was taken as VO2 peak and was used to select a power output in watts eliciting 60% VO2 peak (W60).
Salbutamol
Salbutamol (Sal, trade name: SALBUMOL 2 mg, Glaxo-Wellcome Laboratory, Paris) and placebo (Pla, lactose) capsules were prepared with the same packaging to permit a double-blind administration.
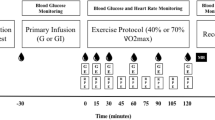
Protocol
Trials were conducted in random order, according to a double-blind procedure, and separated by 72 h intervals, permitting the complete elimination of the drugs between the trials.The protocol for each trial was identical. Trials were held at the same time of day (9:00 AM–10:00 AM) for each subject in order to prevent diurnal variations in hormonal responses.
On the actual test days, subjects arrived after an overnight fast to the laboratory at 8:00 AM–9:00 AM, 2 h after ingestion of salbutamol or placebo capsules. After insertion of a catheter into a superficial forearm vein (8:30 AM–9:30 AM), subjects then rested 30 min, and at 9:00 AM–10:00 AM steady exercise at W60 was started. Blood samples were taken at rest just before exercise and every 10 min during exercise. The pedaling rate of the subjects (70 rpm) was strongly controlled during all the exercise in order to ascertain an identical workload between the trials. The subjects and the investigators were both blinded to the medication given until the completion of the entire study.
Indirect calorimetry and substrate oxidation measurements
Gas exchange data were recorded from 5 min before exercise (rest values) until the end of the steady-state exercise and averaged on every 5 min. Calculation of carbohydrate (CHO) and lipid oxidation were assessed from gas exchange measurements according to the table of nonprotein respiratory quotient (Perronet and Massicotte 1991) (RER, i.e., VCO2/VO2)
The percentage of CHO and lipid oxidation were calculated by using the following equation:
Total energy expenditure (TEE) was calculated by using this formula:
Blood analysis
Blood samples (5 ml) were immediately separated into two aliquots, promptly centrifuged, 10 min at 4°C, 3,000 rpm, and stored at −72°C until assays. Three ml were placed in a chilled sodium heparinized tube for growth hormone (GH), insulin (Ins) and blood glucose (Glu) determination and the last 2 ml in a chilled EDTA-aprotinin tube for ACTH and blood lactate (Lac).
ELISA (Enzyme-Linked Immunosorbent Assay) tests were used for the hormone analyses: ACTH: kits from Biomerica, USA; GH and insulin: kits from DSL, Germany. Blood lactate and blood glucose were analyzed, respectively by electro-enzymatic (Microzym, Biosentec, France) and by classic enzymatic method. All assays were made in duplicate. Coefficients of variation (inter- and intra-assay) for all parameters were always <10%.
Statistics
Data are presented as mean values ± standard error of the mean (SE). A specific test for crossover trials was used to determine whether significant differences existed between Pla and Sal for total exercise energy expenditure and substrate oxidation in order to check for absence of rank order effect. For all the variables, a repeated measure ANOVA with two within factors (time and treatment) was used to compare the dependent measures. A Newman-Keuls multiple comparison test was performed to determine the location of the differences, in the event of an ANOVA revealing a significant main effect.
The null hypothesis was rejected at P < 0.05.
Results
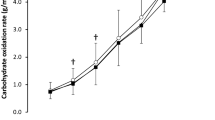
Substrate oxidation during rest and exercise (Table 1; Figs. 1, 2)
No rank effect was detected. There was no significant difference after Sal versus Pla in resting energy expenditure (9.2 ± 0.6 kcal vs. 9.3 ± 0.8 kcal) or in resting CHO and fat oxidation. No interaction between time and treatment was found. During the 1 h exercise, there was a tendency but not a significant increase in TEE (Table 1; Fig. 1) after Sal intake versus Pla (P = 0.066). No significant modification in total CHO and fat oxidation or in the substrate oxidation balance was found between the two treatments during exercise taken as the whole (Table 1). However, the substrate oxidation balance was significantly modified by salbutamol after 40 min of exercise, with significant decrease in % energy expenditure from CHO oxidation and a significant increase in % energy expenditure from fat oxidation (Fig. 2, P < 0.05).

Total energy expenditure (TEE) (kcal) during the 60 min steady-state exercise with placebo (Pla) and salbutamol (Sal) intake

Percentage energy expenditure (EE) from CHO and fat oxidation (means ± SE) with placebo (Pla) and salbutamol (Sal) intake during the 60 min steady-state exercise
Hormonal concentrations (Fig. 3)
ACTH
Baseline ACTH values did not differ significantly between Sal and Pla. On Pla, ACTH increased from 25.4 ± 6.0 to 72.5 ± 33.0 pg ml−1 at 60 min (P < 0.05). On Sal, ACTH values remained unchanged over the entire time. Sal induced significantly lower ACTH concentrations (P < 0.05) compared to Pla from 50 min of exercise until the end of exercise.

ACTH, GH and insulin responses (means ± SE) at rest (0) and during exercise with placebo (Pla) and salbutamol (Sal) intake. *Significant difference between Pla and Sal (P < 0.05)
GH
Baseline and exercise GH values did not differ significantly between Sal and Pla. On Sal and on Pla, exercise induced a significant increase in resting GH concentrations which started to be significant after 20 min of exercise (P < 0.05).
Insulin
The ANOVA did not reveal any significant treatment effect in Ins concentrations. Exercise significantly decreased Ins after 10 min (P < 0.05).
Metabolic data (Fig. 4)
Blood glucose
Sal did not alter resting and exercise blood glucose concentrations. Exercise did not induce any significant alteration in resting Glu concentrations whatever the treatment administered.

Blood glucose (Glu) and lactate (Lac) (means ± SE) at rest (0) and during exercise with placebo (Pla) and salbutamol (Sal) intake
Lactate
There was no significant difference in resting and exercise Lac values between the two treatments. Resting Lac concentrations increased significantly after 10 min of exercise after both Pla and Sal and remained significantly higher throughout exercise (P < 0.05).
Discussion
At the start of the study we hypothesized that acute systemic administration of salbutamol would modify substrate oxidation with enhancement in energy production. With salbutamol versus placebo, there was no significant difference in TEE and substrate oxidation during a work at 60% of VO2 peak for 1 h, but the substrate oxidation balance was significantly modified after 40 min of exercise. ACTH was significantly decreased with Sal at the end of the exercise, whereas no variation was found in the other hormonal and metabolic parameters investigated between the two treatments.
In humans, beta-2 adrenergic stimulation has been shown to increase basal energy expenditure. Besides this increasing energy expenditure, both beta-1 and beta-2 adrenergic stimulations also increase adipose tissue lipolysis (Schiffelers et al. 1999, 2001), and it has been shown that the increased lipolysis is responsible for a great part of the increase in energy expenditure after beta-1 adrenergic stimulation (Schiffelers et al. 1998). However, since beta-2 adrenergic receptors are mainly localized in skeletal muscle and not in adipocytes, it was hypothesized that beta-2 adrenergic stimulation may exert a direct effect on energy expenditure. In a previous study, Hoeks et al. (2003) demonstrated that 3 h of infusion of salbutamol (77 ng/kgFFM min) increased energy expenditure and fat oxidation, independently of plasma FFA levels. On the same way, Schiffelers et al. (2001) reported that salbutamol (consecutive infusion of 50 ng and 100 ng/kgFFM min during 45 min) increased significantly energy expenditure, lipid oxidation, and plasma nonesterified fatty acids and glycerol concentrations in lean sedentary humans. However, we did not find in the present study with recreationally trained subjects any significant difference in basal energy expenditure or lipid oxidation after salbutamol intake, whereas FFA concentrations were unfortunately not investigated. This discrepancy cannot be explained by the dose administered, which appeared more or less comparable in the different studies. It may, however, be hypothetized that the route as well as the mode of administration (perfusion vs. oral intake) might play an important part in the potency of beta-2 agonists in increasing basal energy expenditure and fuel oxidation. Alternative explanations may be the physical status of our subjects. Indeed, a beta-adrenoceptor adaptation to physical activity (Werle et al. 1990) may represent one of the mechanisms underlying the lack of change in the energy parameters investigated after salbutamol intake.
Our results on the impact of submaximal exercise at W60 on CHO and lipid metabolism are similar to available data. Substrate utilization during exercise is determined by the intensity and duration of exercise as well as by training status and the availability of substrate. The major energy source at rest and during low intensity exercise is fat oxidation while oxidation of carbohydrates and anaerobic energy utilization predominates at higher intensities (Sahlin 1990; Green et al. 1995; Carter et al. 2001). Recently, Stisen et al. (2006) investigated the differences in fat oxidation between endurance trained and untrained women both at moderate (40–60% VO2 max) and high intensities (65–80% VO2 max). According to previous studies, the authors reported that endurance trained women had a higher fat oxidation at moderate and high-exercise intensity but that the relative exercise intensity that elicited the highest rate of fate oxidation was the same (53–56% VO2 max) for all subjects. It appears therefore that our subjects are closed to their maximal fat oxidation rates.
To our knowledge, no previous work has quantified the impact of acute salbutamol intake on energy cost and substrate oxidation during exercise in humans. Indeed, only one study (Van Baak et al. 2000) has investigated the effect of salbutamol on endurance performance at a workload representing 70% of their W max, with in parallel, measurement of gas exchange during the first part of exercise (30 min), but energy expenditure was not quantified. The authors reported that salbutamol did not affect VO2, respiratory exchange ratio, or plasma FFA but blood lactate appeared significantly increased during this exercise. It must be, however, noticed that findings on the effects of salbutamol on FFA and on lactate during exercise are inconsistent, other studies reporting no change or significant increase in these parameters after salbutamol administration at higher intensities (Van Baak et al. 2000, 2004; Collomp et al. 2000a, b, 2002, 2005).
The results obtained in the present study are concordant with the aforementioned study of Van Baak et al. (2000), except for lactate data. Exercise energy production at W60 was slightly but not significantly increased by acute salbutamol intake in our healthy, recreationally trained subjects. In the same way, both relative and absolute rate of energy production from CHO and fat did not significantly change during exercise taken as the whole. Therefore, the theory that the ergogenic effect of salbutamol results from a change in substrate oxidation has little support during relatively short term endurance exercise (around 1 h). However, in view of the increase in % energy expenditure from fat oxidation after salbutamol intake which starts to be significant after 40 min of exercise, it is conceivable that longer exercise duration can generate positive findings.
Although stimulation of central alpha 1-adrenergic mechanisms results in secretion of ACTH in man, presumably by increased release of a corticotrophin-releasing factor, beta-2 adrenergic agonist drugs had no effect on the secretion of ACTH at rest (Al-Damluji et al. 1987). However, to the best of our knowledge, the effects of salbutamol on ACTH secretion have never been investigated during submaximal exercise, whereas no change was shown in ACTH secretion after supramaximal exercise (Le Panse et al. 2007). In the present study, ACTH concentrations during the last 10 min of exercise were significantly decreased after salbutamol intake versus placebo. It seems therefore that salbutamol did alter ACTH secretion during this type of exercise in recreationally trained men but the exact mechanism(s) implicated need further investigations.
We demonstrated in the present study no significant change in GH concentrations by salbutamol intake either at rest or during exercise. The earlier limited data on the effects of acute salbutamol on GH in humans (Giustina et al. 1995; Collomp et al. 2005; Le Panse et al. 2006) have found acute salbutamol administration to decrease exercise GH concentrations, probably via enhanced somatostatin secretion and/or activity. In healthy subjects, acute β2 stimulation blunts the physiological GH response to both maximal (Collomp et al. 2002) and supramaximal exercise (Le Panse et al. 2007). It may than be suggested that a higher intensity of exercise is necessary to reveal a blunted effect of acute salbutamol on GH secretion. Moreover, this lack of change in GH concentration appears consistent with the lack of significant change in fat oxidation with salbutamol observed in the present study.
Although hyperglycaemia and hyperinsulinemia have been reported to be associated with the acute use of beta-2 adrenergic agonists at rest (Wager et al. 1982; Rolf Smith and Kendall 1984), there is a paucity of data on the effects of acute salbutamol intake on insulin and blood glucose during submaximal exercise. As a matter of fact, only two studies (Collomp et al. 2000a, 2002) investigated these parameters and showed that systemic salbutamol intake increases C-peptide or insulin concentrations without significant change in blood glucose concentrations during 80–85% VO2 max submaximal exercise or a mock test. In the present work, we did not find any significant change in either blood glucose or insulin concentrations after salbutamol intake compared to placebo. The most plausible explanation seems to be the relative low intensity of exercise.
Conclusion
Our data show that energy metabolism and regulation are not significantly affected by acute therapeutic salbutamol intake during a work at 60% of VO2 peak for 1 h in recreationally trained men after an overnight fast. Further studies will be necessary to study the effect of salbutamol on these parameters in other conditions, in particular in elite athletes under longer exercise durations.
References
Al-Damluji S, Perry L, Tomlin S, Bouloux P, Grossman A, Rees LH, Besser GM (1987) Alpha-adrenergic stimulation of corticotropin secretion by a specific central mechanism in man. Neuroendocrinology 45:68–76
Arlettaz A, Portier H, Lecoq A-M, Labsy Z, De Ceaurriz J, Collomp K (2008) Effects of acute prednisolone intake on substrate utilization during submaximal exercise. Int J Sports Med 29:21–26
Carter SL, Rennie C, Tarnopolsky MA (2001) Substrate utilization during endurance exercise in men and women after endurance training. Am J Physiol Endocrinol Metab 280:E898–E907
Collomp K, Candau R, Collomp R, Carra J, Lasne F, Préfaut C, De Ceaurriz J (2000a) Effects of acute ingestion of salbutamol during submaximal exercise. Int J Sports Med 21:480–484
Collomp K, Candau R, Lasne F, Labsy Z, Ch Préfaut, De Ceaurriz J (2000b) Effects of short-term oral salbutamol administration on exercise endurance and metabolism. J Appl Physiol 89:430–436
Collomp K, Candau R, Millet G, Mucci P, Borrani F, Préfaut C, De Ceaurriz J (2002) Effects of salbutamol and caffeine ingestion on exercise metabolism and performance. Int J Sports Med 23:549–554
Collomp K, Le Panse B, Portier H, Lecoq AM, Jaffre C, Richard O, Benhamou L, Courteix D, De Ceaurriz J (2005) Effects of acute salbutamol intake during a Wingate test. Int J Sports Med 26:513–517
Giustina A, Malerba M, Bresciani E, Desenzani P, Licini M, Zaltieri G, Grassi V (1995) Effect of two β2-agonist drugs, salbutamol and broxaterol, on the growth hormone response to exercise in adult patients with asthmatic bronchitis. J Endocrinol Invest 18:847–852
Green HJ, Jones S, Ball-Burnett M, Farrance B, Ranney D (1995) Adaptations in muscle metabolism to prolonged voluntary exercise and training. J Appl Physiol 78:138–145
Hoeks J, Van Baak M, Hesselink M, Hul G, Vidal H, Saris W, Schrauwen P (2003) Effect of β1- and β2-adrenergic stimulation on energy expenditure, substrate oxidation, and UCP3 expression in humans. Am J Physiol Endocrinol Metab 285:E775–E782
Le Panse B, Collomp K, Portier H, Lecoq AM, Jaffre C, Beaupied H, Richard O, Benhamou L, De Ceaurriz J, Courteix D (2005) Effects of short-term salbutamol ingestion during a Wingate test. Int J Sports Med 26:518–523
Le Panse B, Arlettaz A, Portier H, Lecoq AM, De Ceaurriz J, Collomp K (2006) Short term salbutamol ingestion and supramaximal exercise in healthy women. Br J Sports Med 40:627–631
Le Panse B, Arlettaz A, Portier H, Lecoq AM, De Ceaurriz J, Collomp K (2007) Effects of acute salbutamol intake during supramaximal exercise in women. Br J Sports Med 41:430–434
Perronet F, Massicotte D (1991) Table of nonprotein respiratory quotient: an update. Can J Sport Sci 16:23–29
Rolf Smith S, Kendall M (1984) Metabolic responses to β2 stimulants. J R Coll Chest Physiol 18:190–194
Sahlin K (1990) Muscle glucose metabolism during exercise. Ann Med 22:85–89
Schiffelers S, Brouwer E, Saris W, Van Baak M (1998) Inhibition of lipolysis reduces beta1-adrenoceptor-mediated thermogenesis in man. Metabolism 47:1462–1467
Schiffelers S, Saris W, Boomsma F, Van Baak M (2001) Beta(1)- and beta(2)-adrenoceptor-mediated thermogenesis and lipid utilization in obese and lean men. J Clin Endocrinol Metab 86:2191–2199
Schiffelers S, Van Harmelen V, De Grauw H, Saris W, Van Baak M (1999) Dobutamine as selective β1-adrenoceptor agonist in in vivo studies on human thermogenesis and lipid utilization. J Appl Physiol 87:977–981
Stisen A, Stougaard O, Langfort J, Helge J, Sahlin K, Madsen K (2006) Maximal fat oxidation rates in endurance trained and untrained women. Eur J Appl Physiol 98:497–506
Van Baak M, Mayer L, Kempinski R, Hartgens F (2000) Effect of salbutamol on muscle strength and endurance performance in nonasthmatic men. Med Sci Sports Exerc 32:1300–1306
Van Baak M, de Hon O, Hartgens F, Kuipers H (2004) Inhaled salbutamol and endurance cycling performance in non-asthmatic athletes. Int J Sports Med 25:533–538
Wager J, Fredholm B, Lunell N, Persson B (1982) Metabolic and circulatory effects of intravenous and oral salbutamol in late pregnancy in diabetic and non-diabetic women. Acta Obstet Gynecol Scand Suppl 108:41–46
Werle E, Strobel G, Weicker H (1990) Decrease in rat cardiac beta1- and beta2-adrenoceptors by training and endurance exercise. Life Sci 46:9–17
Acknowledgments
The authors wish also to express their gratitude to the subjects for their dedicated performance. In addition we likewise thank the CHR of Orléans, Nathalie Crépin, Sandra Ferary, Patrick Guenon, Nicole Chevrier and Dr M. Ferry for their assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Arlettaz, A., Le Panse, B., Portier, H. et al. Salbutamol intake and substrate oxidation during submaximal exercise. Eur J Appl Physiol 105, 207–213 (2009). https://doi.org/10.1007/s00421-008-0891-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-008-0891-7