
Abstract
Knee pain is a common symptom of different knee pathologies, affecting muscle strength and force generation. Although the control of precise three-dimensional forces is essential for the performance of functional tasks, current evidence of pain effects in force variability is limited to single-directional assessments of contractions at moderate force levels. This study assessed the effects of experimental knee joint pain in the three-dimensional force variability during isometric knee extensions at a wide range of target forces (2.5–80 % of maximal voluntary contraction, MVC). Fifteen healthy subjects performed contractions before, immediately following, and after injections of hypertonic (painful) or isotonic (control) saline into the infrapatellar fat pad. Pain intensity was measured on a 10-cm visual analogue scale. Force magnitude, direction, and variability were assessed using a six-axis force sensor while activity of quadriceps and hamstring muscles was recorded by surface electromyography. Significant correlation was found between tangential force displacements and variability of quadriceps muscle activity. Experimental knee pain increased the variability of the task-related force component at all force levels, while variability of tangential force components increased at low forces (≤5 % of MVC). The mean quadriceps activity decreased during painful contractions only at 80 % of MVC. Pain adaptations underlying increased force variability at low contraction levels probably involve heterogeneous reorganization of muscle activity, which could not be detected by surface electrodes. These findings indicate a less efficient motor strategy during knee joint pain, suggesting that pain relief may enhance training for the control of smooth forces by knee pain patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Knee pain is the most predominant and disabling symptom in knee osteoarthritis (OA) (Felson 2005), affecting muscle coordination (Hodges et al. 2009) and force generation (Slemenda et al. 1998; Henriksen et al. 2011). As a consequence, patients with knee OA demonstrate higher force fluctuations during knee extensions compared with healthy subjects (Hortobágyi et al. 2004), suggesting impaired motor performance. Increased force fluctuations of the quadriceps muscle have been associated with higher risk of falls (Carville et al. 2007) and reduced performance at functional tasks such as chair rising and stair climbing (Seynnes et al. 2005; Pua et al. 2010). Therefore, force steadiness has been suggested as an index of task stability to identify pain-related impairments in the motor system associated with knee OA and other musculoskeletal disorders (Pua et al. 2010).
Reports regarding effects of chronic pain on force steadiness are so far limited and not very consistent. Hortobágyi et al. (2004) observed impaired force steadiness in knee OA patients compared with non-symptomatic subjects during dynamic knee extensions, while isometric contractions were not significantly affected. Decreased steadiness has also been reported in subjects with chronic neck pain during isometric cervical flexion (Muceli et al. 2011), but not consistently in subjects with subacromial impingement syndrome performing shoulder abduction (Bandholm et al. 2006). While the tasks performed in these studies were limited to moderate force levels (~10–40 % of maximal voluntary force), investigations using delayed onset muscle soreness, a well known endogenous pain and soreness model, have shown greater exercise-induced force variability during contractions below 10 % of maximal voluntary force (Semmler et al. 2007), which could partially explain the inconsistency across previous investigations.
Multiple factors may introduce inter-subject variability when assessing muscle function during chronic pain conditions, such as structural damage, inflammation and muscle weakness. Experimental pain models are advantageous in this respect because they allow the assessment of the isolated effects of pain in healthy individuals. Previous studies using intramuscular injections of algesic substances to investigate motor output variability have focused primarily on the upper limbs, demonstrating that even short-term muscle pain is able to elicit significant impairments in the steadiness of force (Del Santo et al. 2007; Bandholm et al. 2008) and movement (Ervilha et al. 2004; Madeleine et al. 2008). Recent findings showed that acute muscle pain may increase variability not only in the normal, task-related force component but also in tangential force components during isometric contractions of the upper and lower limbs (Salomoni and Graven-Nielsen 2012a). However, injection of hypertonic saline in the muscle may affect other receptors besides nociceptors due to changes in ion concentration, causing sensorimotor changes independent of pain effects (Hodges et al. 2009). Moreover, the sources of pain in many clinical conditions, such as knee OA, are not the muscles, but articular-related structures (Dye et al. 1998). Given the high prevalence of chronic knee pain conditions, it is important to assess how pain per se affects the stability of forces around the knee joint when present in non-muscular tissues. Although it has been shown that experimental anterior knee pain elicits heterogeneous reorganization of motor unit population during isometric knee extensions (Tucker and Hodges 2010), the impact of knee joint pain on the steadiness of the resultant force vector is yet to be investigated.
Since reorganization of activity within and between muscles is known to modulate both the intensity and the direction of force fluctuations (Kouzaki et al. 2004; Kutch et al. 2008), the current study assessed the effects of experimental knee pain on the distribution and steadiness of three-dimensional (task-related and tangential) forces during submaximal isometric knee extensions at low, moderate and high target forces. The hypothesis investigated was that, compared with baseline, acute knee pain is linked with reorganized muscle activity eliciting higher variability of the task-related and tangential force components during knee extensions.
Methods
Subjects
Fifteen young volunteers (12 males, age 27.1 ± 4.6 years, height 175.1 ± 7.9 cm, weight 71.9 ± 13.8 kg, mean ± SD) with no known musculoskeletal disorder participated in this study. All participants received detailed written and verbal information and signed an informed consent before inclusion. The study was conducted in accordance with the Declaration of Helsinki and approved by the local Ethics Committee (N-20090036).
Experimental knee pain
Acute knee pain was induced by bolus injections of sterile hypertonic saline (1.0 ml, 5.8 %) into the medial part of the infrapatellar fat pad of the dominant leg, using isotonic saline (1.0 ml, 0.9 %) as control. The needle was withdrawn immediately after the injection. The fat pad is a pain-sensitive structure due to high presence of nociceptive afferent fibers and is considered a contributing source of knee pain in knee OA patients (Clockaerts et al. 2010). Injections were performed using a 1-ml plastic syringe with a disposable needle (25G, 25 mm). The pain intensity was assessed on a 10-cm electronic visual analogue scale (VAS), where 0 cm indicated “no pain” and 10 cm “maximal pain”. Immediately after the injection, the signal from the VAS was recorded continuously for 10 min (sampling frequency of 0.5 Hz) while subjects were asked to update the VAS before and after each trial by adjusting an external handheld slider.
Force recordings
Three-dimensional forces were recorded using a high-sensitivity six-axis force sensor, yielding three force and three moment components (MC3A, AMTI, USA; sensitivity of force components F x , F y , F z : 0.054, 0.054, 0.0134 V/N; moment components M x , M y , M z : 2.744, 2.744, 2.124 V/Nm) and thus allowing the assessment of force magnitude and direction [Fig. 1a; angle θ ZX = atan(F x /F z ); angle θ ZY = atan(F y /F z )]. The sensor was attached to a metal plate, which was fixed to a heavy chair by a pair of L-shaped bars (Fig. 1b). The height of the sensor was adjusted to 5 cm above the medial malleolus of the dominant leg of each subject, while the hip was flexed at 90° and the knee extended at 120° (180° = straight leg). The thigh was strapped and the arms were crossed in front of the chest. The analogue output of the sensor was low-pass filtered at 500 Hz, amplified (MSA-6, AMTI, USA), sampled at 1 kHz, and stored after 12 bits A/D conversion.

Schematic representation of the three-dimensional force components relative to the surface of the six-axis sensor (a) used to assess isometric knee extension forces (b). F z is the task-related force and tangential forces are represented as F x and F y
Surface electromyography (EMG)
EMG signals were recorded from m. rectus femoris (RF), m. vastus lateralis (VL), m. vastus medialis (VM), m. biceps femoris (BF), and m. semitendinosus (ST) using pairs of disposable Ag/AgCl surface electrodes (Ambu Neuroline 720, Denmark) in bipolar configuration, placed 2 cm apart and positioned according to standard recommendations (Hermens et al. 2000). Signals were amplified (Counterpoint MK2, Dantec, Denmark), filtered (10–500 Hz), sampled at 1 kHz, and stored after 12 bits A/D conversion.
Protocol
A randomized, blinded, placebo controlled, crossover design was used in order to assess the effects of experimental knee pain on the variability of force. Subjects performed three agonist and three antagonist isometric maximal voluntary contractions (MVCs, 5 s), each followed by at least 1.5 min of rest. Subjects then performed a total of six series of submaximal isometric knee extensions (13 s) with the dominant leg, corresponding to before, during, and after the effects of a painful or non-painful injection (hereafter designated pre, during and post conditions). In total, subjects received two injections, in random order: one painful and one non-painful, each performed before a series of submaximal contractions. Both the subject and the experimenter were naive to the order of injections, which was randomized and balanced across subjects by the responsible medical doctor. The post-injection condition was initiated 1 min after the subject reported no pain sensation. Contractions were performed in random order at 2.5, 5, 20, 50, and 80 % of MVC force, each followed by at least 20 s of rest, and additional 1.5 min of rest between series. During each contraction, a ramp-and-hold feedback of the task-related force component (F z ) was provided on a computer screen (2 s of ramp phase, 11 s of hold phase) using a variable visual gain, resulting in a constant visual scale across all target forces. The full ramp-and-hold target was constantly shown on the screen, while the trace representing the force performed by the subject was updated in real-time on the same time scale. Before starting the recordings, subjects were familiarized with the setup and the protocol by performing maximal and submaximal practice trials.
Data analysis
The EMG signals were digitally band-pass filtered at 20–400 Hz using a Butterworth filter of second order. The root mean square (RMS) value of each EMG signal was calculated over epochs of 1 s, normalized using the peak RMS epoch from the MVC task, and assessed as the difference from baseline assessments. Using the same epoch length, the mean frequency (MNF) was extracted to assess potential fatigue effects.
The following parameters were extracted from each submaximal contraction: mean VAS pain score, mean force magnitude in each direction, mean and range of force angles (θ ZX and θ ZY ), coefficient of variation (CV = standard deviation/mean force) of the task-related force component, total excursion of the center of pressure (CoP), mean normalized RMS and standard deviation (SD) of each EMG channel. A time window of 6 s was used for analysis (2 s from end of ramp; Fig. 2), avoiding excessive fluctuations due to slow force development and anticipation of trial termination. The CV of force was assessed only for the task-related force component because the magnitude of the tangential components approached zero during some trials, resulting in inconsistently high values of the CV of force. Hence, similar to previous investigations, the variability of tangential forces was indirectly assessed by changes in the CoP (Zhang et al. 2010). In the present study, the total excursion of the CoP was extracted, which represents the total length of the CoP path during a given time interval, thus assessing the lateral displacements of quasi-static forces (Salomoni and Graven-Nielsen 2012b).

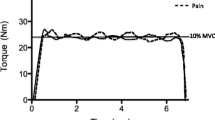
Representative recordings of task-related force (F z ), tangential forces (F x , F y ), and m. vastus medialis (VM) EMG signals assessed during isometric knee extensions at 50 % MVC force following injections of isotonic (non-painful) and hypertonic (painful) saline into the infrapatellar fat pad. The 6-s shaded area represents the time window used for data analysis
Statistical analysis
All parameters were assessed using a three-way repeated measures analysis of variance (RM-ANOVA) with injection (isotonic, hypertonic), condition (pre, during, post), and force (2.5, 5, 20, 50, and 80 % MVC force) as within-subject factors. In case of significant factors or interactions the Newman–Keuls (NK) post hoc test was applied incorporating correction for multiple comparisons. Pearson coefficient of correlation was estimated between EMG measures (RMS, SD) and parameters of force variability (CV of force, total excursion of CoP). Statistical significance was considered for P values lower than 0.05. All results are reported as mean ± standard error of the mean (SEM).
Results
Experimental muscle pain
Hypertonic saline injections in the infrapatellar fat pad elicited significantly higher VAS scores than isotonic saline injections [Fig. 3; RM-ANOVA: F(1, 14) = 44.5, P < 0.00001; NK: P < 0.0002]. All the VAS scores were zero during pre- and post-pain conditions.

Mean (±SEM, shaded area) VAS scores after intramuscular injection of hypertonic (HYP) and isotonic (ISO) saline into the infrapatellar fat pad. Injections of hypertonic saline elicited higher VAS scores than isotonic saline
Force parameters
Experimental knee pain reduced the magnitude of the task-related force component compared with non-painful conditions during contractions at 80 % MVC force [Fig. 4; F z ; RM-ANOVA: F(8, 112) = 2.44, P < 0.018; NK: P < 0.0001]. No significant changes were observed in the magnitude of tangential force components across trials. Although the mean force angles were non-significantly affected by pain (Fig. 5a), the RM-ANOVA of both ranges of force angle (θ ZX and θ ZY ) presented interactions between injection, condition and force level, revealing higher ranges of force angle during painful compared with non-painful contractions at 2.5 % MVC force [Fig. 5b; RM-ANOVA: F(8, 112) > 2.03, P < 0.05; NK: P < 0.05]. Knee pain also elicited significantly higher CV of the task-related force component compared with non-painful assessments [Fig. 6a; RM-ANOVA: F(2, 28) > 10.8, P < 0.0003; NK: P < 0.0005]. Moreover, increased total excursion of the CoP was detected at 5 % MVC during painful compared with non-painful conditions [Fig. 6b; RM-ANOVA: F(8,112) > 3.04, P < 0.004; NK: P < 0.0002].

Mean (+SEM) force magnitude (F x , F y , F z ) during isometric knee extensions. Knee pain reduced the magnitude of the task-related force component compared with non-painful (baseline, post and after isotonic saline) contractions at 80 % MVC force (lower compared with all other conditions, NK: † P < 0.0001)

Mean (+SEM) absolute force angle (a θ ZX and θ ZY ), and range of force angle (b θ ZX and θ ZY ) during isometric knee extensions. Although the mean force angle was not significantly affected by pain, greater ranges of force angle were observed during painful compared with non-painful (baseline, post and after isotonic saline) contractions at 2.5 % MVC force (higher compared with all other conditions, NK: *P < 0.05)
Muscle activity
Decreased RMS of EMG was observed in VM muscle during painful contractions at 80 % MVC compared with non-painful assessments [Table 1; RM-ANOVA: F(4, 56) > 7.42, P < 0.00007; NK: P < 0.007]. Moreover, the activity of VM muscle at 80 % MVC increased post-hypertonic injection condition compared with all other conditions (NK: P < 0.05). No significant differences were detected across pain conditions in the mean RMS EMG of the other muscles assessed, as well as no significant changes in the MNF or the SD of EMG (data not shown). When data were pooled across isotonic and hypertonic injection sessions, significant correlations were found between the total excursion of the CoP and the SD of EMG of VL (2.5–50 % MVC, P < 0.014, 0.26 < r < 0.39) and RF (20–50 % MVC, P < 0.003, 0.31 < r < 0.58) muscles.

Mean (+SEM) coefficient of variation (a CV) of task-related force and total excursion of the CoP (b) during isometric knee extensions. Experimental knee pain elicited greater CV of task-related force compared with non-painful (baseline, post and after isotonic saline) assessments at all force levels, while total excursion of the CoP increased during pain only at 5 % MVC force (NK: *P < 0.0002)
Discussion
This is the first study to assess the effects of experimental knee pain on the variability of three-dimensional force output. The results show less steady knee extensions during painful compared with non-painful assessments, particularly at low force levels. While the variability of the task-related force component (i.e. CV of force) increased over a wide range of force levels, the variability of tangential force components was most affected at low forces, as revealed by increased range of force angles and increased total excursion of the CoP. In addition, decreased activity of VM muscle during painful contractions performed close to maximal voluntary force was associated with failure to sustain the required force-matching task, with a subsequent increase in VM muscle activity post-hypertonic saline condition.
Force variability and knee pain
In line with the present findings, increased force variability during pain has been previously observed during both chronic and experimental conditions (Hortobágyi et al. 2004; Bandholm et al. 2006, 2008; Del Santo et al. 2007; Muceli et al. 2011). Since pain causes a reduction of motor unit firing rates of agonist and synergist muscles (Farina et al. 2004), increased force variability may result from a compensatory motor strategy in order to sustain the required force output, potentially involving increased central drive (Del Santo et al. 2007), selective recruitment of high-threshold motor units (Hodges et al. 2008), and increased motor unit synchronization (Yao et al. 2000). In addition, activation of nociceptive pathways from group III and IV afferents, which converge on common interneurons with segmental reflex pathways from group Ia and Ib afferents (Schomburg et al. 1999), may hinder the interpretation of proprioceptive information by the central nervous system, thus modulating force variability (Shinohara et al. 2005).
The precise orientation of forces produced by individual motor units within each muscle depends on muscle fiber angle and attachments (Herrmann and Flanders 1998), and changes in motor unit population may alter the resultant force vector (Tucker and Hodges 2010). Since the relative contribution of a single motor unit is higher in a small population of motor units, greater pain-induced impairments in the steadiness of tangential force components were observed at low compared with high target forces, further supporting the involvement of changes in motor unit behavior such as altered recruitment strategy and increased variability of the synaptic input to the active motoneurons (Farina et al. 2012). Conversely, a smaller contribution of these mechanisms at high forces could explain why, despite significant modulation of muscle activity, no changes were observed in tangential force variability at 80 % MVC, as it is likely that all motor units are active at this contraction level, even in large muscles (De Luca et al. 1982). This argument is supported by the absence of correlation between the SD of EMG and the total excursion of the CoP at 80 % MVC. Corroborating, delayed onset muscle soreness is known to elicit higher increase of force fluctuations at low compared with high force levels (Semmler et al. 2007). Although Hortobágyi et al. (2004) reported that steadiness of the lower limb of knee OA patients is equally impaired at low and moderate force levels, their assessments were limited to absolute target forces corresponding roughly to 15–40 % of MVC force. Considering that clinical knee joint pain can originate from multiple structures, including the infrapatellar fat pad (Felson 2005), additional translational studies are needed to investigate the impact of symptomatic knee OA in force variability during contraction levels beyond these limits, particularly below 10 % MVC.
Increased variability of multidirectional forces and movements has been associated with the development of musculoskeletal disorders (Madeleine 2010). Moreover, force steadiness of the quadriceps muscle has been suggested as a predictor of functional performance of healthy subjects and patients with knee or hip OA during chair rising and stair climbing tasks (Hortobágyi et al. 2004; Seynnes et al. 2005; Pua et al. 2010). Although conservative recommendations for the management of knee OA emphasize muscle strengthening (Zhang et al. 2008), knee extensor steadiness training may act as an important cofactor for the improvement of functional performance, particularly in patients with relatively well preserved muscle strength (Pua et al. 2010). Corroborating, it has been shown that mere repetition of contractions without skill or precision does not necessarily produce changes in muscle coordination (Tsao and Hodges 2007) or cortical reorganization (Remple et al. 2001).
Muscle activity and knee pain
In the present study, reduced activity of VM muscle and inability to sustain 80 % MVC target forces were observed during knee pain condition, which most likely reflect a reduction of quadriceps strength caused by experimental knee pain (Henriksen et al. 2011). Supporting this argument, inability to sustain maximal and 75 % MVC knee extension forces has previously been reported following injection of hypertonic saline in the rectus femoris muscle, caused by inhibition of the central drive (Graven-Nielsen et al. 2002). Although acute experimental pain does not replicate the long-term aspects of clinical knee pain, this finding is relevant for patients with knee OA because it has been argued that reduced strength of the quadriceps muscle precedes development of radiographic knee OA (Segal et al. 2010) and pain-induced muscle weakness in early stages may accelerate structural damage, thus contributing to physical disability of knee OA patients (O’Reilly et al. 1998). Therefore, analgesic treatment may be valuable to increase the pain-free range of forces in which patients can exercise during rehabilitation (Graven-Nielsen et al. 2002). Corroborating, it has been recently shown that patients with knee OA may improve muscle strength gain during exercise in combination with interventions aimed at blocking pain sensation (Pietrosimone et al. 2011), although the risk of overload needs to be carefully considered in the design of a specific rehabilitation program.
As a consequence of pain-induced inhibitory effects, the same relative target force may impose a more strenuous effort during painful compared with non-painful contractions (Sørensen et al. 2012). Hence, the increased VM activity observed at post-pain condition (after the effects of hypertonic saline) may originate from the subjects’ expectation of a greater effort, so that an attempt to generate forces close to maximal results in a tendency to overshoot. Alternatively, muscle fatigue could have developed over the repeated sustained contractions, resulting in increased muscle activity. However, since the order of injections and target forces were randomized, other pain conditions and force levels would have also been affected, which was not observed. Another possibility is that it could be part of a protective mechanism where larger areas of the muscle are activated in order to better stabilize the knee joint, although this hypothesis cannot be confirmed by the bipolar EMG recordings used in this study.
The most commonly accepted theory to explain pain-induced changes in motor control, the pain adaptation model proposed by Lund et al. (1991), predicts that movement amplitude and velocity are reduced during pain due to inhibition of agonist muscles and excitation of antagonist muscles. Although reduced activity of VM muscle was observed during pain at 80 % MVC force, the results do not fully support the pain adaptation theory, as no significant changes were detected in any other agonist or antagonist muscles involved in knee extensions or at low and moderate force levels. Furthermore, muscle fatigue arising from repeated isometric trials could reduce the ability of muscles to generate force (Bigland-Ritchie and Woods 1984), but no changes were observed in the MNF of EMG, indicating no significant effects of fatigue in the EMG signals.
According to recent findings from Tucker and Hodges (2010), deep-tissue pain elicits a heterogeneous reorganization of activity within and between muscles, which includes decreased firing rates, inhibition of some motor units and selective recruitment of additional high-threshold motor units, which are not likely to be detected using bipolar EMG electrodes. Using a pair of unidirectional force transducers to assess medial and lateral knee extension forces, it was found that this pain-induced adaptation may affect the direction of the resultant force vector (Tucker and Hodges 2010). The present study extended their findings by employing a three-dimensional force sensor in order to thoroughly assess how experimental knee pain affects the generation and stability of knee extension forces. The results, which include increased force variability during pain, absence of changes in the surface EMG activity (except at very high forces), and significant association between variability of muscle activity and tangential force displacements, support the theory of heterogeneous pain effects on different motor units. In addition, the observed increase in the range of force angles and in the variability of task-related and tangential forces during pain provides evidence that the new motor strategy adopted during painful conditions is less efficient (or at least less steady) than the strategy used in the absence of pain, particularly at low force levels. Combined with the impaired proprioception that is commonly observed in patients with knee OA (Bennell et al. 2003; Hortobágyi et al. 2004), this mechanism contributes to the impaired ability of these patients to generate and control smooth forces during daily activities.
One limitation of the present study is that only isometric contractions were assessed, while previous studies have shown greater force fluctuations during dynamic compared with isometric contractions (Christou and Carlton 2002). Therefore, the impact of pain on the stability of dynamic functional tasks may be even greater than the impairments reported here.
Conclusion
Experimental knee pain significantly increased variability of task-related and tangential forces during isometric knee extensions. Although the steadiness of the force output was particularly impaired at low target forces, changes in muscle activity were only detected at force levels close to maximal. The absence of changes in the mean RMS EMG activity and the association between SD of EMG and tangential force displacements at low and moderate target forces suggest heterogeneous pain adaptations in muscle activity. These results suggest that pain relief may improve the efficiency of rehabilitation in patients with symptomatic knee OA.
References
Bandholm T, Rasmussen L, Aagaard P, Jensen BR, Diederichsen L (2006) Force steadiness, muscle activity, and maximal muscle strength in subjects with subacromial impingement syndrome. Muscle Nerve 34:631–639
Bandholm T, Rasmussen L, Aagaard P, Diederichsen L, Jensen BR (2008) Effects of experimental muscle pain on shoulder-abduction force steadiness and muscle activity in healthy subjects. Eur J Appl Physiol 102:643–650
Bennell KL, Hinman RS, Metcalf BR, Crossley KM, Buchbinder R, Smith M, McColl G (2003) Relationship of knee joint proprioception to pain and disability in individuals with knee osteoarthritis. J Orthopaed Res 21:792–797
Bigland-Ritchie B, Woods JJ (1984) Changes in muscle contractile properties and neural control during human muscular fatigue. Muscle Nerve 7:691–699
Carville SF, Perry MC, Rutherford OM, Smith ICH, Newham DJ (2007) Steadiness of quadriceps contractions in young and older adults with and without a history of falling. Eur J Appl Physiol 100:527–533
Christou EA, Carlton LG (2002) Age and contraction type influence motor output variability in rapid discrete tasks. J Appl Physiol 93:489–498
Clockaerts S, Bastiaansen-Jenniskens YM, Runhaar J, Van Osch G, Van Offel JF, Verhaar JAN, De Clerck LS, Somville J (2010) The infrapatellar fat pad should be considered as an active osteoarthritic joint tissue: a narrative review. Osteoarthr Cartil 18:876–882
De Luca CJ, LeFever RS, McCue MP, Xenakis AP (1982) Behaviour of human motor units in different muscles during linearly varying contractions. J Physiol 329:113–128
Del Santo F, Gelli F, Spidalieri R, Rossi A (2007) Corticospinal drive during painful voluntary contractions at constant force output. Brain Res 1128:91–98
Dye SF, Vaupel GL, Dye CC (1998) Conscious neurosensory mapping of the internal structures of the human knee without intraarticular anesthesia. Am J Sport Med 26:773–777
Ervilha UF, Arendt-Nielsen L, Duarte M, Graven-Nielsen T (2004) Effect of load level and muscle pain intensity on the motor control of elbow-flexion movements. Eur J Appl Physiol 92:168–175
Farina D, Arendt-Nielsen L, Merletti R, Graven-Nielsen T (2004) Effect of experimental muscle pain on motor unit firing rate and conduction velocity. J Neurophysiol 91:1250–1259
Farina D, Negro F, Gizzi L, Falla D (2012) Low frequency oscillations of the neural drive to the muscle are increased with experimental muscle pain. J Neurophysiol 107:958–965
Felson DT (2005) The sources of pain in knee osteoarthritis. Curr Opin Rheumatol 17:624–628
Graven-Nielsen T, Lund H, Arendt-Nielsen L, Danneskiold-Samsøe B, Bliddal H (2002) Inhibition of maximal voluntary contraction force by experimental muscle pain: a centrally mediated mechanism. Muscle Nerve 26:708–712
Henriksen M, Rosager S, Aaboe J, Graven-Nielsen T, Bliddal H (2011) Experimental knee pain reduces muscle strength. J Pain 12:460–467
Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G (2000) Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol 10:361–374
Herrmann U, Flanders M (1998) Directional tuning of single motor units. J Neurosci Methods 18:8402–8416
Hodges PW, Ervilha UF, Graven-Nielsen T (2008) Changes in motor unit firing rate in synergist muscles cannot explain the maintenance of force during constant force painful contractions. J Pain 9:1169–1174
Hodges PW, Mellor R, Crossley K, Bennell KL (2009) Pain induced by injection of hypertonic saline into the infrapatellar fat pad and effect on coordination of the quadriceps muscles. Arthr Rheum 61:70–77
Hortobágyi T, Garry J, Holbert D, Devita P (2004) Aberrations in the control of quadriceps muscle force in patients with knee osteoarthritis. Arthritis Rheum 51:562–569
Kouzaki M, Shinohara M, Masani K, Fukunaga T (2004) Force fluctuations are modulated by alternate muscle activity of knee extensor synergists during low-level sustained contraction. J Appl Physiol 97:2121–2131
Kutch JJ, Kuo AD, Bloch AM, Rymer WZ (2008) Endpoint force fluctuations reveal flexible rather than synergistic patterns of muscle cooperation. J Neurophysiol 100:2455–2471
Lund JP, Donga R, Widmer CG, Stohler CS (1991) The pain-adaptation model: a discussion of the relationship between chronic musculoskeletal pain and motor activity. Can J Physiol Pharm 69:683–694
Madeleine P (2010) On functional motor adaptations: from the quantification of motor strategies to the prevention of musculoskeletal disorders in the neck–shoulder region. Acta Physiol 199:1–46
Madeleine P, Mathiassen SE, Arendt-Nielsen L (2008) Changes in the degree of motor variability associated with experimental and chronic neck–shoulder pain during a standardised repetitive arm movement. Exp Brain Res 185:689–698
Muceli S, Farina D, Kirkesola G, Katch F, Falla D (2011) Reduced force steadiness in women with neck pain and the effect of short term vibration. J Electromyogr Kinesiol 21:283–290
O’Reilly SC, Jones A, Muir KR, Doherty M (1998) Quadriceps weakness in knee osteoarthritis: the effect on pain and disability. Ann Rheum Dis 57:588–594
Pietrosimone BG, Saliba SA, Hart JM, Hertel J, Kerrigan DC, Ingersoll CD (2011) Effects of transcutaneous electrical nerve stimulation and therapeutic exercise on quadriceps activation in people with tibiofemoral osteoarthritis. J Orthop Sports Phys Ther 41:4–12
Pua YH, Clark RA, Bryant AL (2010) Physical function in hip osteoarthritis: relationship to isometric knee extensor steadiness. Arch Phys Med Rehabil 91:1110–1116
Remple MS, Bruneau RM, VandenBerg PM, Goertzen C, Kleim JA (2001) Sensitivity of cortical movement representations to motor experience: evidence that skill learning but not strength training induces cortical reorganization. Behav Brain Res 123:133–141
Salomoni SE, Graven-Nielsen T (2012a) Experimental muscle pain increases normalized variability of multidirectional forces during isometric contractions. Eur J Appl Physiol. doi:10.1007/s00421-012-2343-7
Salomoni SE, Graven-Nielsen T (2012b) Muscle fatigue increases the amplitude of fluctuations of tangential forces during isometric contractions. Hum Mov Sci. doi:10.1016/j.humov.2011.08.012
Schomburg ED, Steffens H, Kniffki KD (1999) Contribution of group III and IV muscle afferents to multisensorial spinal motor control in cats. Neurosci Res 33:195–206
Segal NA, Glass NA, Torner J, Yang M, Felson DT, Sharma L, Nevitt M, Lewis CE (2010) Quadriceps weakness predicts risk for knee joint space narrowing in women in the MOST cohort. Osteoarthr Cartil 18:769–775
Semmler JG, Tucker KJ, Allen TJ, Proske U (2007) Eccentric exercise increases EMG amplitude and force fluctuations during submaximal contractions of elbow flexor muscles. J Appl Physiol 103:979–989
Seynnes O, Hue OA, Garrandes F, Colson SS, Bernard PL, Legros P, Fiatarone SMA (2005) Force steadiness in the lower extremities as an independent predictor of functional performance in older women. J Aging Phys Act 13:395–408
Shinohara M, Moritz CT, Pascoe MA, Enoka RM (2005) Prolonged muscle vibration increases stretch reflex amplitude, motor unit discharge rate, and force fluctuations in a hand muscle. J Appl Physiol 99:1835–1842
Slemenda C, Heilman DK, Brandt KD, Katz BP, Mazzuca SA, Braunstein EM, Byrd D (1998) Reduced quadriceps strength relative to body weight: a risk factor for knee osteoarthritis in women? Arthr Rheum 41:1951–1959
Sørensen TJ, Langberg H, Hodges PW, Bliddal H, Henriksen M (2012) Experimental knee joint pain during strength training increases muscle strength gain in healthy subjects: a randomised controlled trial. Arthr Care Res 64:108–116
Tsao H, Hodges PW (2007) Immediate changes in feedforward postural adjustments following voluntary motor training. Exp Brain Res 181:537–546
Tucker KJ, Hodges PW (2010) Changes in motor unit recruitment strategy during pain alters force direction. Eur J Pain 14:932–938
Yao W, Fuglevand RJ, Enoka RM (2000) Motor-unit synchronization increases EMG amplitude and decreases force steadiness of simulated contractions. J Neurophysiol 83:441–452
Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden NK, Bierma-Zeinstra S, Brandt KD, Croft P, Doherty M (2008) OARSI recommendations for the management of hip and knee osteoarthritis, part II: OARSI evidence-based, expert consensus guidelines. Osteoarthr Cartil 16:137–162
Zhang W, Gordon AM, Fu Q, Santello M (2010) Manipulation after object rotation reveals independent sensorimotor memory representations of digit positions and forces. J Neurophysiol 103:2953–2964
Acknowledgments
The study has been financed by Svend Andersen Fonden (Aalborg, Denmark).
Conflict of interest
The authors declare no conflicts of interest, financial or otherwise.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Toshio Moritani.
Rights and permissions
About this article
Cite this article
Salomoni, S.E., Ejaz, A., Laursen, A.C. et al. Variability of three-dimensional forces increase during experimental knee pain. Eur J Appl Physiol 113, 567–575 (2013). https://doi.org/10.1007/s00421-012-2461-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-012-2461-2