
Abstract
Sporting compression garments (CG) are used widely during exercise despite little evidence of benefits. The purpose of this study was to investigate coverage and pressure effects of full-body CG on cardiovascular and thermoregulatory function at rest and during prolonged exercise, and on exercise performance. Twelve recreationally trained male cyclists [mean (SD) age, 26 (7) years; \( \dot{V}{\text{O}}_{2\max } \), 53 (8) mL kg−1 min−1] completed three sessions (counterbalanced order), wearing either correctly-sized CG (CSG; 11–15 mmHg), over-sized CG (OSG; 8–13 mmHg), or gym shorts (CONT). Test sessions were conducted in temperate conditions [24 (1)°C, 60 (4)% relative humidity; ~2 m s−1 air velocity during exercise], consisting of resting on a chair then on a cycle ergometer, before 60-min fixed-load cycling at ~65% \( \dot{V}{\text{O}}_{2\max } \) and a 6-km time trial. Wearing CG (CSG or OSG) did not mitigate cardiovascular strain during mild orthostatic stress at rest (p = 0.20–0.93 for garment effects). During exercise, cardiac output was ~5% higher in the CG conditions (p < 0.05), which appears to be accounted for via non-significant higher end-exercise heart rate (~4–7%, p = 0.30; p = 0.06 for greater heart rate drift in CSG); other cardiovascular variables, including stroke volume, were similar among conditions (p = 0.23–0.91). Covered-skin temperature was higher in CG conditions (p < 0.001) but core (oesophageal) temperature was not (p = 0.79). Time-trial performance (mean power, time taken) was similar with or without CG (p = 0.24–0.44). In conclusion, any demonstrable physiological or psychophysical effects of full-body CG were mild and seemingly reflective more of surface coverage than pressure. No benefit was evident for exercise performance.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sporting compression garments (CG) are promoted as being beneficial for various aspects of athletic performance and physiological function, and although empirical evidence for benefits is available it is generally limited (MacRae et al. 2011). CG are available in a number of styles (upper body, lower body; full length, partial length), and the applied pressures can differ considerably. While studies on CG in sporting cohorts are becoming more common, fundamental effects on cardiovascular and thermoregulatory strain remain unclear, as are the effects on exercise performance.
There appear to be no published data on local perfusion during orthostatically stressful exercise, and until recently (Sperlich et al. 2011), this was also so for cardiac output (\( \dot{Q} \)) and stroke volume (SV). Rather, claimed evidence for cardiovascular effects of CG has often been based on work in the fields of clinical and therapeutic medicine. Limb compression, commonly via graduated compression stockings (knee length or thigh length), has been shown to increase venous flow velocity (e.g. Lawrence and Kakkar 1980; Sigel et al. 1975) and reduce vein diameter or cross-sectional area (Coleridge Smith et al. 1991) and venous pooling (Sparrow et al. 1995), although effects for people in upright postures are mixed (Liu et al. 2008; Lord and Hamilton 2004). These findings are of limited value in exercise because of differences in participants (health, posture, movement), applied pressures, and variables measured. For example, suggestions that CG influence venous return are often based on studies involving patients with venous disorders (e.g. Agu et al. 2004; Ibegbuna et al. 2003) or studies where findings need to be extrapolated (e.g. Berry and McMurray 1987; Lawrence and Kakkar 1980). Evidence indicating benefits of CG on SV and \( \dot{Q} \) is limited (Stenger et al. 2010; Watanuki and Murata 1994), and to our knowledge, confined to stationary participants. The one identified study in which \( \dot{Q} \) and SV were measured during exercise indicated that CG (ankle to knee; applied pressures at the calf ranging from ~14 to 39 mmHg) had no significant effect (Sperlich et al. 2011). Possible influences of greater body coverage appear unknown despite being of principal importance. Augmented local perfusion has been reported for the forearm and leg (Bochmann et al. 2005; Mayrovitz and Larsen 1997), and may account for increases in muscle oxygenation (calf) at rest (Bringard et al. 2006a). Data on cardiovascular strain during exercise are typically limited to heart rate (HR), and indicate no significant effect during various forms of running (Ali et al. 2007, 2010; Bringard et al. 2006b; Duffield et al. 2008; Duffield and Portus 2007; Goh et al. 2010; Higgins et al. 2009; Houghton et al. 2009; Kemmler et al. 2009) and cycling (Scanlan et al. 2008).
Use of CG likely alters heat exchange between the body and environment whether desired or not. Exercising skin temperatures have typically been higher when covered by CG (Duffield et al. 2008; Duffield and Portus 2007; Goh et al. 2010; Houghton et al. 2009), but without significant effect on sweat rate/mass loss (Duffield et al. 2008; Duffield and Portus 2007; Goh et al. 2010; Houghton et al. 2009) or core temperature (Duffield et al. 2008; Goh et al. 2010; Houghton et al. 2009) in cool to hot environments. Influences on local skin temperature are likely primarily due to the inherent insulation of the garment and associated air, however, pressure per se is known to affect skin perfusion (Mayrovitz and Delgado 1996; Mayrovitz and Sims 2003) and, thus, potentially also heat storage and cardiovascular function. There may be a distinction between effects of pressure per se versus coverage per se, although this has not yet been addressed directly. Hence, further clarification of thermoregulatory effects is required, particularly during prolonged exertional heat stress.
Finally, clarification is also required for CG effects on exercise performance. When CG were worn during exercise, ergogenic effects have been demonstrated but are relatively few (MacRae et al. 2011). Aspects of jump performance have improved in some situations (e.g. Kraemer et al. 1998), however, these findings are mixed (e.g. Higgins et al. 2009). Performance measures during prolonged exercise were typically similar with or without CG (Ali et al. 2007; Berry and McMurray 1987; Duffield and Portus 2007; Goh et al. 2010; Scanlan et al. 2008; Sperlich et al. 2010), although benefits have been reported with statistical significance (Kemmler et al. 2009) or practical significance (effect size = 0.86) (Higgins et al. 2009).
The aim of this study was to examine the effects of full-body CG on cardiovascular and thermoregulatory function during rest and exercise, and on exercise performance. The effects of pressure and skin coverage were each examined using controlled trials in which commercially available graduated CG were compared against oversized CG (i.e. same skin coverage but lower applied pressures) and against no CG. The purpose of the oversized CG was to attempt to discriminate between compressive versus thermally insulative effects of the garments and control for placebo effects. High body coverage was most conducive to examining pressure versus insulation effects, hence full-body CG were used as opposed to garments with sport-specific coverage (e.g. thigh, or thigh and leg for cycling). This usage of CG by athletes is also not unconventional.
Methods
Participants
Twelve recreationally trained male cyclists were recruited for this study [mean (SD) age, 26 (7) years; mass 79 (9) kg; height 1.80 (0.07) m; \( \dot{V}{\text{O}}_{2\max } \) 53 (8) mL kg−1 min−1]. Participants were informed orally and in writing of all procedures and protocols before giving written consent, and study approval was granted by the University of Otago Human Ethics Committee. All participants were healthy, non-smokers and not taking any medication, and were required to complete a basic medical screening questionnaire before taking part.
Preliminary procedures and garment information
In a preliminary session, the \( \dot{V}{\text{O}}_{2\max } \) of each participant was determined in ambient laboratory conditions (~20°C) using a ramp protocol to voluntary exhaustion on a cycle ergometer (RacerMate Velotron; Seattle, WA, USA), and an online gas analysis system (COSMED Quark CPET; Rome, Italy). Following a uniform rest period, the power output (watts) required to elicit ~65% \( \dot{V}{\text{O}}_{2\max } \) was determined and noted for the experimental sessions. A familiarisation 6-km cycle time trial was performed.
Full-length upper- and lower-body CG (Skins™; Riverwood, Australia) were used in this study (body coverage: neck and wrist to waist; waist to ankle). The garments were made from knit fabrics, with the fibre reported as 76% nylon and 24% elastane. Relevant fabric properties are given in Table 1, as determined from samples cut (British Standards Institution 1999) from new CG tops that had been pre-treated with six wash cycles (procedure 8A; International Organization for Standardization 2000a) to stabilise the fabric (Gore et al. 2006). Fabrics were conditioned for 24 h in a controlled standard environment (20 ± 2°C and 65 ± 4% RH; International Organization for Standardization 2005), and tested in a relaxed state in that same environment.
Mass, standing height, and chest circumference of each participant were measured and used to fit the CG. Each participant was allocated two sets of upper- and lower-body CG: one set correctly-sized according to the manufacturer’s guidelines (correctly-sized garments; CSG), and one set over sized by at least two size designations to a maximum of XXL (over-sized garments; OSG). The sleeves and legs of OSG were cut and re-hemmed to match the sleeve and leg length of each participant’s respective CSG to standardise body coverage. Although over sized, OSG were still ‘form-fitting’.
Experimental procedures
Each participant completed the experimental session three times, at the same time of day and separated by at least 5 days. The order of testing was pseudo randomised to ensure balancing. Each experimental session was identical apart from clothing condition: the three conditions were full-body CSG, full-body OSG, or gym shorts only (CONT). The participants’ own underwear, shoes, and socks were consistent among sessions. Before each experimental session, participants were asked to hydrate adequately and abstain from alcohol, caffeine, and exercise within 24 h, and from strenuous exercise within 40 h. The participants were required to replicate what they had eaten the night before and the morning of the first trial for each subsequent trial. Experimental trials were conducted in an environmental chamber under the controlled conditions of 24 (1)°C and 60 (4)% RH. Exercise consisted of cycling on a cycle ergometer. Cycling provided substantial exercise-induced physiological stress while maintaining a relatively stationary upper body (allowing measurement of forearm vasodilator response and beat-to-beat blood pressure profiles for derivation of cardiac effects).
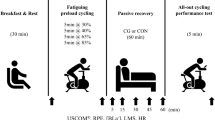
Following arrival at the laboratory each participant emptied his bladder before being weighed seminude. Urine was analysed (Atago hand refractometer; Tokyo, Japan) to confirm hydration status (urine specific gravity ≤ 1.020). The participant entered the test environment and sat for instrumentation. A schematic of the test session is shown in Fig. 1. Following at least 20 min of seated rest, a 30-min pre-exercise period was used to obtain baseline data. This pre-exercise period consisted of three stages: seated rest on chair not wearing CG (rest1); donning of the relevant CG in the CSG and OSG conditions (in CONT, the participant remained seated); and seated rest on the cycle ergometer with legs extended, feet resting on foot rests (rest2). Fixed-load exercise began immediately following the baseline period, and consisted of cycling at ~65% \( \dot{V}{\text{O}}_{2\max } \) for 60 min [fixed load; 186 (27) W], before a self-paced 6-km time trial in which all external cues apart from distance were masked. Convective airflow was provided during all exercise with a large-diameter fan (655 mm, ~2 m s−1) at a uniform distance and orientation. Fluid consumption during the fixed-load exercise was 2 mL kg−1 body mass at approximately 15-min intervals. The fluid contained 50 g sucrose and 2 g NaCl per litre of water. Ethically imposed cut-off criteria were core temperature > 39.5°C or HR > 95% of the pre-determined maximum HR range for each participant. Body mass (seminude) was re-measured at the end of the trial after each participant had wiped himself dry with a towel.

Experimental session schematic. The sessions consisted of seated rest on a chair (Rest1), donning of the relevant compression garments (CG) in CG conditions (in the control condition the participants remained seated), rest on the cycle ergometer with legs extended (Rest2), fixed-load exercise, and a 6-km self-paced time trial (TT)
Measurements
Sub-garment pressures were measured before and during exercise at the posterolateral forearm (at widest part), anterior thigh (mid-way along the femur), and posterior calf (at widest part) using small circular air-filled bladders (diameter = 40 mm, inflated thickness = 5 mm) connected to pressure transducers (Honeywall 26PCAFA1G; Golden Valley, MN, USA) via plastic airlines (internal diameter = 1.5 mm). Data were recorded at 100 Hz throughout the trial (PowerLab and Chart 5; ADInstruments, Dunedin, New Zealand). The pre-exercise measurement (i.e. at rest) was made immediately following garment donning in CSG and OSG conditions, when participants were required to stand relaxed with feet shoulder width apart for ~1 min.
The HR was measured from the R–R interval of ventricular depolarisation and recorded at 1-min intervals (Polar S810 HR monitor; Kempele, Finland). Systemic arterial blood pressure (systolic, diastolic, mean) was measured at 200 Hz during collection periods (3-min periods; at rest1 and rest2, and after 27, 42, and 57 min of exercise; the exercise data were subsequently pooled into one exercise value for each variable) using finger photoplethysmography (Finometer Midi, TPD Biomedical Instrumentation; Amsterdam, The Netherlands). Additional output variables (SV, \( \dot{Q} \), total peripheral resistance, left ventricular ejection time, and rate of blood pressure increase at ejection) were generated from the aortic pressure or aortic flow waveforms using the model-flow method, incorporating the sex, height, age, and body mass of the participant (BeatScope 1.0, TPD Biomedical Instrumentation). This method has been shown to provide a reliable estimate of changes in \( \dot{Q} \) during exercise (Sugawara et al. 2003).
The core temperature was measured using an oesophageal thermistor (Mallinckrodt Medical 400 series; St Louis, MO, USA) inserted via the nasal passage to the lower third of the oesophagus, directly posterior to the left ventricle (Mekjavic and Rempel 1990). Skin temperature was measured using skin thermistors (Grant Instruments, Cambridge, UK) taped to the skin at eight sites: forehead, scapula, upper chest, anterior bicep, posterolateral forearm, finger, anterior thigh, and posterior calf (International Organization for Standardization 2004). Core and skin temperatures were recorded at 1-min intervals (Grant Instruments squirrel data logger; Cambridge, UK). Relative humidity was measured using hygrometers (Hycal HIH-3602-A; El Monte, CA, USA) taped to the skin at two sites: scapula and upper chest; data were recorded at 100 Hz throughout the trial (PowerLab and Chart 5).
The vasodilator response of the forearm was measured using venous occlusion plethysmography. A flexible indium–gallium strain gauge (Hokanson Inc; Bellevue, WA, USA) was placed around the right forearm where the circumference was maximal, and venous outflow was occluded for brief periods (~5 s) to allow measurement of forearm expansion. An inflatable cuff was placed around the bicep and inflated to 50 mmHg during the occlusion period (Groothuis et al. 2003) where arterial inflow was maintained; data were recorded at 100 Hz (PowerLab; Chart 5) during rest1 and rest2, and after 17, 33, and 48 min of exercise.
Ratings of perceived thermal state [−4 (very cold) to +4 (very hot)], evaluations of thermal and wetness comfort [0 (comfortable) to 4 (extremely uncomfortable)] (International Organization for Standardization 1995b), and ratings of perceived exertion [6 (7 = very, very light) to 20 (19 = very, very hard)] (Borg 1982) were taken at rest2 (minute −2) and during exercise (minutes 19, 36, and 57). Time, power, and cadence were recorded during the 6-km time trial. Near-nude dry body mass (±20 g; Wedderburn electronic scales; Dunedin, New Zealand) and garment mass (±5 g; Teraoka DS-671 electronic scales; Tokyo Japan) were measured before and after each experimental trial.
Calculations
Exercise sub-garment pressures were calculated as cyclic minima and maxima values for both the calf and thigh. Minima and maxima values were sampled from 1-min periods at the beginning and end of fixed-load exercise (when the pressure trace satisfied conditions of cyclic regularity—indicative of consistent pedalling dynamics). Beginning and end-exercise values were pooled for each trial to obtain an exercise mean.
Mean covered and exposed skin temperatures were calculated using the body site weightings described elsewhere (International Organization for Standardization 2004). Covered sites were: scapula, chest, bicep, forearm, thigh, and calf (‘covered’ refers to the body sites as in the CSG and OSG conditions); exposed sites were: forehead and finger. Next-to-skin absolute vapour pressures were calculated from relative humidity and temperature data using formulae previously described (Santee and Gonzalez 1988). Whole-body sweat rate was estimated from change in body mass using the formula (Mitchell et al. 1972) which corrects for respiratory losses. The slope of forearm expansion was taken as the mean of three determinations for each time point. A digital 20-Hz low-pass filter was applied to the data trace. Forearm perfusion was expressed as a factor of baseline (rest1; i.e. near nude in all conditions).
For data collected throughout the trial, mean values were calculated over suitable periods for rest and during exercise: HR, minutes −30 to −26 (rest1), −4 to 0 (rest2), 15 to 17 (early exercise), 34 to 36, and 57 to 59 (end exercise); core temperature, minutes −30 to −26 (rest1), −6 to −2 (rest2), 17 to 21 (early exercise), 46 to 48, and 58 to 60 (end exercise); and skin temperature, −30 to −26 (rest1), −6 to −2 (rest2), 6 to 8 (early exercise), 31 to 35, and 58 to 60 (end exercise).
Statistical analysis
Descriptive statistics were mean (SD). Inferential statistical analyses were performed using SPSS statistical software (SPSS 16.0; Chicago, IL, USA) with an alpha level of 0.05. For all measures excluding psychophysical sensory ratings, rest and exercise data were analysed separately: resting data were absolute values and exercise data were change scores from rest2. A linear mixed model (Bonferroni correction as required) with an unstructured repeated covariance matrix was used to test for differences among garment types and, where applicable, time periods for sub garment pressures, cardiovascular variables, core and skin temperatures, forearm perfusion, whole-body sweat rate, next-to-skin vapour pressures, and time-trial duration, mean power, and cadence. Other covariance structures (diagonal, compound symmetry, compound symmetry heterogeneous) were trialled, but some were considered less appropriate and others failed to fit. A Friedman analysis of variance by ranks was used to test for the effect of garment type on psychophysical sensory ratings (Siegel and Castellan 1988). Where significance was found, a Tukey test for differences between the mean ranks was used to identify differences among garment types (Zar 1984).
Results
For rest and fixed-load exercise, cardiovascular and thermoregulatory responses are presented in Tables 2 and 3, and psychophysical ratings are presented in Table 4.
Sub-garment pressures
Sub-garment pressures were significantly lower in OSG than CSG during both rest and exercise (p = 0.001–0.02). The pressures during rest were 13 (2) mmHg (forearm), 11 (2) mmHg (thigh), 15 (1) mmHg (calf) for CSG, and 9 (2) mmHg (forearm), 8 (2) mmHg (thigh), 13 (2) mmHg (calf) for OSG. During exercise, pressures at the thigh and calf fluctuated between minima and maxima values in phase with cycling cadence, with an amplitude of ~6 and 5 mmHg when wearing CSG and OSG, respectively. The absolute values (minima–maxima) were 10 (2)–16 (1) mmHg (thigh) and 11 (1)–18 (2) mmHg (calf) for CSG, and 8 (2)–13 (3) mmHg (thigh) and 9 (1)–14 (2) mmHg (calf) for OSG.
Rest
HR, \( \dot{Q} \), SV, arterial pressures (systolic, diastolic, mean), rate of blood pressure increase at ejection, and total peripheral resistance were similar among all conditions (p = 0.20–0.93), although all of these variables were altered in going from rest1 (chair) to rest2 (cycle ergometer) (p = 0.001–0.01) excluding systolic arterial pressure (p = 0.87). Left ventricular ejection time was longer in CSG than OSG (~5 ms, or ~2%; p = 0.04), although the magnitude of the difference was unlikely to be of practical importance.
Wearing CG had no effect on temperature of the core (p = 0.56) or exposed skin temperature (p = 0.39), but tended to increase chest and scapula next-to-skin vapour pressures (p = 0.07), and increased covered skin temperature by 0.8–0.9°C in both CG conditions (p = 0.02). Garment condition had a small effect on forearm perfusion (p = 0.05), with OSG and CSG numerically greater than CONT, although mean values were highly variable and subsequent pairwise comparisons were not significant (p = 0.12–1.00). No significant differences were evident among the garment conditions for relevant psychophysical ratings (p = 0.07–1.00; Table 4).
Fixed-load exercise
While HR was similar among garment conditions during fixed-load exercise (p = 0.39), steady-state HR did increase (p = 0.001) and tended to be higher at end exercise in CSG and OSG (by 3–5 beats min−1; p = 0.06 for garment condition and time effect interaction). Garment type had an effect on \( \dot{Q} \) (p = 0.04), with values in CSG and OSG conditions each ~0.6 L min−1 higher than CONT (although for pairwise comparisons: CSG vs. CONT, p = 0.08; OSG vs. CONT, p = 0.10; CSG vs. OSG, p = 1.00). Exercising SV, left ventricular ejection time, rate of pressure increase at ejection, arterial pressures (systolic, diastolic, mean), and total peripheral resistance were each similar irrespective of whether or not CG were worn (p = 0.23–0.91). The mean HR data from photoplethysmography (provided for direct comparison with \( \dot{Q} \) and SV data; c.f. HR data from R–R intervals above) were (change from rest2): CONT, 72 (11) beats min−1; CSG, 77 (13) beats min−1; OSG, 75 (10) beats min−1.
Wearing either CSG or OSG (vs. CONT) increased covered skin temperature (by 0.5–0.9°C; p = 0.001), but there was no garment effect on exposed skin temperature (p = 0.42), or core temperature (p = 0.79). Following the initial rise in core temperature with exercise, it remained stable (p = 0.06). Next-to-skin vapour pressure at the chest was similar irrespective of whether CG were worn or not (p = 0.10), but vapour pressure at the scapula was greater by 0.8–1.1 kPa in CSG and OSG versus CONT (p = 0.001). Forearm perfusion tended to be higher in CSG or OSG (vs. CONT), although not significantly so (p = 0.13). Whole-body sweat rate throughout the trial appeared to be greater when CG were worn [CSG, 0.85 (0.25) L h−1; OSG, 0.79 (0.30) L h−1] than in CONT [0.75 (0.25) L h−1], but not significantly so (p = 0.14).
During exercise, wearing CSG were rated as warmer and less comfortable than CONT (p < 0.05) but no different from OSG (p > 0.05); skin wetness was perceived as similarly comfortable among all conditions (p = 0.11–0.63). Although an effect of garment type was evident in early exercise (p = 0.01; Tukey’s groupings not identifiable, p > 0.05), ratings of perceived exertion were generally similar throughout fixed-load exercise (p = 0.62–0.75).
Time-trial performance
Time taken, mean power, and cadence were similar irrespective of garment condition (p = 0.24–0.66), and irrespective of trial order (p = 0.37–0.50). Group mean values for time taken and mean power, respectively, were: CONT, 571 (32) s and 287 (43) W; CSG, 576 (33) s and 280 (46) W; OSG, 573 (37) s and 287 (49) W. Mean power during the time trial for each participant is shown in Fig. 2.

Mean power output during a 6-km cycling time trial for each participant in each garment condition (CONT gym shorts, CSG correctly-sized garments, OSG over-sized garments)
Discussion
Sporting CG are promoted as having positive effects on exercise performance and numerous aspects of underlying physiological or physical function. The present study was undertaken because very few data exist on integrative cardiovascular and thermoregulatory effects of sporting CG. Further clarification of central cardiovascular effects was also warranted.
Here, an integrative approach was taken to investigate coverage and pressure effects of CG on cardiovascular and thermoregulatory function. Wearing full-body commercially available CG (resting applied pressures <15 mmHg at the calf, thigh, and forearm) did not significantly augment SV during rest or prolonged dynamic exercise, and hence indicate no observable benefit for cardiac preload. Any demonstrable effects of wearing full-body CG were similar irrespective of being CSG or OSG. These garments caused increases in skin temperature and exercising \( \dot{Q} \) without significantly affecting core temperature, SV, arterial blood pressure, or exercise performance.
Rest
Adequate compression at the surface of the body compresses underlying tissues, thereby decreasing the relative vascular transmural pressure and also vascular volumes. Through these processes CG can have passive and active effects on cardiovascular function, although such effects presumably depend on many factors such as the cardiovascular variable (e.g. SV), applied pressures, areas compressed, vascular health, posture, and activity. Previously demonstrated passive effects include decreases in venous cross-sectional area and pooling (e.g. Coleridge Smith et al. 1991; Sparrow et al. 1995) and oedema (presumably via reduced hydrostatic pressures across the vessel wall; Jonker et al. 2001). Demonstrated active effects include local perfusion augmentations (Bochmann et al. 2005; Mayrovitz and Larsen 1997), which are possibly (at least in part) mediated by a reflex arteriolar dilatation in response to locally reduced transmural pressures (i.e. a myogenic response). Peripheral vascular effects may then influence central cardiovascular function (e.g. by reducing afterload and/or increasing preload), although this is not clear, and is difficult to interpret in closed-loop systems. If present, altered central cardiovascular function may arise from reduced venous volumes and increased venous return (increased preload), and reduced peripheral resistance locally or via reduced muscle sympathetic nerve activity (decreased afterload).
Sitting on a cycle ergometer with legs extended (rest2) represented a mild increase in orthostatic stress versus sitting on a chair with legs bent at the knee (rest1). Wearing CG did not mitigate the associated cardiovascular strain, as the posture-induced decreases in SV and \( \dot{Q} \), and increase in HR were each similar irrespective of whether CG were worn or not. Reported effects of CG on venous pooling/limb volume are mixed in ‘healthy’ limbs, particularly when upright (e.g. Bringard et al. 2006a; Kraemer et al. 2000; Liu et al. 2008; Lord and Hamilton 2004). Together, these findings indicate threshold pressures are likely (above which effects are demonstrable), and that these thresholds may reduce as the orthostatic stress is prolonged. The applied pressures of medical CG (classes I–IV) span a greater pressure range than typical for sporting CG. The relatively mild applied pressures of off-the-shelf sporting CG possibly account for the lack of effect on cardiovascular strain observed in the present study. For example with venous pooling, decreased cross-sectional area of the long saphenous, short saphenous, and popliteal veins were reported with graduated compression stockings (36–47 mmHg) versus without, but only at the popliteal vein were the differences significant with stockings of lesser applied pressures (10–14 and 18–21 mmHg; Liu et al. 2008). Similarly, benefits of lower-body CG on SV have been demonstrated on occasions where the applied pressures were greater [~55, 18, and 6 mmHg at the ankle, posterior knee, and thigh, respectively (Stenger et al. 2010); 25 and 20 mmHg at leg and thigh, respectively (Watanuki and Murata 1994)] than those in the current study (at rest, 15 and 11 mmHg for CSG, calf and thigh, respectively). In the study of Watanuki and Murata (1994), SV and \( \dot{Q} \), measured using the CO2 re-breathing technique, were significantly higher (by ~15 mL and 0.5 L min−1, respectively), and HR lower (by ~5 beats min−1) when wearing compression stockings than without during prolonged stationary standing. The minimum pressures required to influence \( \dot{Q} \) when standing were estimated at 17 and 15 mmHg for the leg and thigh, respectively (Watanuki and Murata 1994), which are consistent with the lack of any significant effect observed here. Supporting the notion of pressure thresholds for cardiovascular effects, tissue oxygenation of the gastrocnemius medialis during supine and standing rest was greater when lower-body CG (23–24 mmHg at the calf) were worn versus CG of lesser applied pressures (5–6 mmHg at the calf) or no CG (Bringard et al. 2006a). It appears likely that higher pressures than those of the commercially available garments used in this study are required to significantly mitigate cardiovascular strain in ‘healthy’ people at rest, although considerations such as comfort (and hence compliance) and freedom of movement must be taken into account. Notwithstanding our findings, CG may still be of benefit for hypotensive/orthostatically intolerant athletes, at least following exercise (Privett et al. 2010).
Forearm muscle perfusion is typically unchanged or reduced during passive heat stress or exercise in the lower limbs, therefore increases in total forearm perfusion usually reflect thermoregulatory increases in skin perfusion (Johnson and Rowell 1975). When CG were worn (vs. without), the tendency for forearm perfusion to be greater (30–70%) was consistent with higher covered-skin temperature (~1°C), indicating that CG may cause mild heat stress and compensatory increases in skin perfusion. However, compression of the forearm (13–23 mmHg) has been shown to increase forearm perfusion without changes in local skin temperature (Bochmann et al. 2005). A myogenic response is thought to occur with limb compression, whereby transmural pressures of underlying vessels are reduced, causing an autoregulatory dilation, and increased local perfusion (Bochmann et al. 2005; Mayrovitz and Larsen 1997). In the present study, venous occlusion plethysmography was used and hence distribution of perfusion within the limb could not be identified. In the work of Bochmann et al. (2005; also using venous occlusion plethysmography), perfusion showed some tendency to increase as applied pressures increased over a range from 13–20 mmHg. We found no such trend with increased pressure, although differences in applied pressures at the forearm between CG conditions were modest (CSG, ~13 mmHg; OSG, ~9 mmHg). While pressure or coverage effects on forearm perfusion are difficult to distinguish with the present findings, perhaps more important was that overall, wearing full-body CG during rest in temperate conditions had little demonstrable influence on any physiological or psychophysical responses measured.
Submaximal exercise
Wearing full-body CG (CSG or OSG) during fixed-load exercise modestly elevated cardiovascular and thermoregulatory strain, as indicated by higher covered-skin temperature and tendencies for greater \( \dot{Q} \) (p = 0.04), forearm perfusion (p = 0.13) and drift in HR (for CSG; p = 0.06). While increased \( \dot{Q} \) indicates increased venous return, any effects on SV are not statistically supported. Rather, it appears that HR drift (i.e. higher late-exercise HR) or interplay between non-significant differences in mean-exercise HR (p = 0.39) and SV (p = 0.26) account for changes in \( \dot{Q} \).
The apparent lack of CG effect on cardiac preload, as indicated by SV, supports previous work (Sperlich et al. 2011), and is perhaps indicative of the effectiveness of skeletal muscle pumps and venous valves during continuous dynamic exercise. As an alternative, CG effects on preload may be present but masked by other increases in tissue perfusion (e.g. forearm in the present study) reducing central blood volume (although not supported by the estimated total peripheral resistance). In this alternative, CG would still be of little functional relevance because the garments themselves would be the cause of the added demand for perfusion (thermoregulatory or myogenic). Interestingly, lower-body CG (21 and 15 mmHg, ankle and calf, respectively) provided no benefit for HR or arterial pressure during wheelchair exercise in people with spinal cord injury (Rimaud et al. 2007). Again, either CG did not mitigate venous pooling (even with the absence of muscle-pump action in the lower limbs), or benefits on venous pooling were matched by garment-induced increases in local perfusion.
Sperlich et al. (2011) recently reported that knee-high CG of increasing applied pressures (~14, 23, 32, 39 mmHg at the calf), versus no compression (0 mmHg), did not benefit \( \dot{Q} \), cardiac index, SV, arterio-venous difference in O2 saturation, or other metabolic responses during 45-min fixed-load running at ~70% \( \dot{V}{\text{O}}_{2\max } \) for male endurance athletes (\( \dot{V}{\text{O}}_{2\max } \) ~ 57 mL kg−1 min−1). These findings (wide range of applied pressures) in association with our own (high body coverage) seem to indicate that CG do not mitigate cardiovascular strain during dynamic exercise. Exercising HR has consistently been similar with or without CG (inter-study differences in applied pressures and body coverage, although typically lower-body garments) during cycling (Chatard et al. 2004; Scanlan et al. 2008) and running (Ali et al. 2007, 2010; Bringard et al. 2006b; Duffield et al. 2008; Duffield and Portus 2007; Goh et al. 2010; Higgins et al. 2009; Houghton et al. 2009; Kemmler et al. 2009). In the present study, although HR was not significantly different, it was numerically higher in CG conditions as exercise was prolonged. This finding indicates that CG with high body coverage or worn in warm-hot environmental conditions have limited adverse cardiovascular effects in the short term, but warrant further investigation as exercise is prolonged (>1 h). While aforementioned limitations of occlusion plethysmography precludes differentiating flow distribution within the limb, it appears that wearing CG with applied pressures of <15 mmHg (resting vales reported for consistency with other studies) do not mechanically prevent increases in thermoregulatory skin perfusion as forearm perfusion continued to increase from early to end exercise.
Given the similar physiological responses between the CSG and OSG conditions, it appears that garment coverage had a greater influence on thermoregulatory and cardiovascular strain than did the difference in these particular applied pressures. However, it remains possible that physiological effects are not linearly related to the applied pressures, or that the differences in applied pressures between CSG and OSG were, although significant (p < 0.05), not great enough. Perhaps more importantly, however, was that the effects of both compression and body coverage were minimal because of a general lack of difference from CONT. Elsewhere, compression stockings of different applied pressures (4 and 4, 11 and 8, 26 and 15 mmHg; ankle and calf, respectively) were worn during 40-min fixed-load running and no significant differences were identified for \( \dot{V}{\text{O}}_{2} \), HR, or blood lactate (Ali et al. 2010). Compression garments differing in body coverage (below knee, below waist, whole body) were investigated by Sperlich et al. (2010) but neither HR nor thermoregulatory variables were reported, and garment type did not measurably affect blood lactate, \( \dot{V}{\text{O}}_{2} \), and O2 arterial saturation or partial pressure. Whether greater applied pressures than those used in this study lead to benefits for central or peripheral cardiovascular function during exercise seems not to be supported (Sperlich et al. 2011). Further investigation using lower-body CG that cover both calf and thigh is warranted. Perhaps ankle-to-knee coverage (Sperlich et al. 2011) is not adequate, and upper-body coverage (present study) negates any benefit provided by the lower-body CG because of additional demands for perfusion (thermoregulatory or myogenic). Note that a lack of significant (reported) physiological effects does not necessarily preclude significant performance effects, and vice versa. For example, despite similarities in variables such as HR and \( \dot{V}{\text{O}}_{2} \) at anaerobic and aerobic thresholds, the interpolated running speeds at these metabolic thresholds were significantly higher by 1.5–2% when lower-body CG (18–20 mmHg at the calf) were worn versus without (Kemmler et al. 2009).
Despite the large difference in body coverage between CG and CONT conditions in the present study, the garment-associated heat stress was relatively minor during moderate-intensity exercise. That wearing CG resulted in higher covered-skin temperature was not surprising, and is consistent with the other studies (Duffield et al. 2008; Duffield and Portus 2007; Goh et al. 2010; Houghton et al. 2009), as is the lack of significant effect on core temperature (Duffield et al. 2008; Goh et al. 2010; Houghton et al. 2009) and mass loss (Duffield et al. 2008; Duffield and Portus 2007; Goh et al. 2010; Houghton et al. 2009), including when full-body CG were worn (Duffield and Portus 2007). While clothing is a barrier to heat transfer, the prevailing conditions (convective air flow, warm air) and fabric properties (<1 mm thick, high air permeability, high capacity to hold free moisture) likely mitigated adverse effects in the present study. The similarity in next-to-skin vapour pressure at the chest (directly exposed to airflow from the fan) irrespective of coverage (CSG and OSG vs. CONT) supports this assertion. It is suggested that thermal or cardiovascular effects may be more pronounced during prolonged higher-intensity exercise or in sports where movement is intermittent (i.e. without constant air flow), although these require elucidation.
Exercise performance
Wearing CG did not significantly improve 6-km time-trial performance, which is consistent with most previous reports for exercise (typically running) performance (Ali et al. 2007; Berry and McMurray 1987; Duffield and Portus 2007; Goh et al. 2010; Scanlan et al. 2008; Sperlich et al. 2010). Our findings corroborate those of Scanlan et al. (2008), who had reported that cycling performance (mean and peak power output, work output) during a 1-h time trial was similar with or without lower-body CG. There has been some support for positive effects of CG on endurance performance. Running performance, as indicated by duration of a stepwise exercise test to voluntary maximum, was ~4% longer for active runners (\( \dot{V}{\text{O}}_{2\max } \) ~ 52 mL kg−1 min−1) when CG were worn versus without (Kemmler et al. 2009). However, elsewhere, running time to exhaustion was similar with or without CG for trained endurance athletes (\( \dot{V}{\text{O}}_{2\max } \) ~ 64 mL kg−1 min−1; Sperlich et al. 2010). In these two studies, the applied pressures (~18–20 mmHg at the calf) were reportedly similar, and the CG covered at least the ankle to knee; placebo garments were not used in either case. While complete blinding for garment condition is unlikely, practicable steps to mitigate placebo effects or identify physiological benefits are essential for determining whether and why CG improves performance. Note that effects of wearing CG during recovery are beyond the scope of this study.
Conclusions
Full-body commercially available sporting CG (applied pressures at rest of <15 mmHg) did not mitigate cardiovascular strain during mild orthostatic stress at rest. Wearing these CG (vs. no CG) during fixed-load sub-maximal cycling caused mild increases in thermoregulatory and cardiovascular strain (covered skin temperature and blood flow), although without adversely affecting core body temperature or arterial pressure. Physiological and psychophysical responses were similar irrespective of being CSG or OSG; thus, while body coverage appeared to be more influential than differences with these particular applied pressures, any effects were overshadowed by the general lack of difference from the no-CG control. Any differences in exercise performance in the 6-km time-trial were also not significant. Hence, wearing full-body CG did not benefit cardiovascular or thermoregulatory function or cycling performance.
References
Agu O, Baker D, Seifalian AM (2004) Effect of graduated compression stockings on limb oxygenation and venous function during exercise in patients with venous insufficiency. Vascular 12:69–76
Ali A, Caine MP, Snow BG (2007) Graduated compression stockings: physiological and perceptual responses during and after exercise. J Sports Sci 25:413–419
Ali A, Creasy R, Edge J (2010) Physiological effects of wearing graduated compression stockings during running. Eur J Appl Physiol 109:1017–1025
Berry MJ, McMurray RG (1987) Effects of graduated compression stockings on blood lactate following an exhaustive bout of exercise. Am J Phys Med 66:121–132
Bochmann RP, Seibel W, Haase E, Hietschold V, Rödel H, Deussen A (2005) External compression increases forearm perfusion. J Appl Physiol 99:2337–2344
Borg GAV (1982) Psychophysical bases of perceived exertion. Med Sci Sports Exerc 14:377–381
Bringard A, Denis R, Belluye N, Perrey S (2006a) Effects of compression tights on calf muscle oxygenation and venous pooling during quiet resting in supine and standing positions. J Sports Med Phys Fit 46:548–554
Bringard A, Perrey S, Belluye N (2006b) Aerobic energy cost and sensation responses during submaximal running exercise—positive effects of wearing compression tights. Int J Sports Med 27:373–378
British Standards Institution (1990) BS 7209: water vapour permeable apparel fabrics. British Standards Institution, London
British Standards Institution (1998) BS EN 12127: textiles—fabrics—determination of mass per unit area using small samples. British Standards Institution, London
British Standards Institution (1999) BS EN 12751: textiles—sampling of fibres, yarns and fabrics for testing. British Standards Institution, London
Chatard JC, Atlaoui D, Farjanel J, Louisy F, Rastel D, Guézennec CY (2004) Elastic stockings, performance and leg pain recovery in 63-year-old sportsmen. Eur J Appl Physiol 93:347–352
Coleridge Smith PD, Hasty JH, Scurr JH (1991) Deep vein thrombosis: effect of graduated compression stockings on distension of the deep veins of the calf. Br J Surg 78:724–726
Duffield R, Portus M (2007) Comparison of three types of full-body compression garments on throwing and repeat-sprint performance in cricket players. Br J Sports Med 41:409–414
Duffield R, Edge J, Merrells R, Hawke E, Barnes M, Simcock D, Gill N (2008) The effects of compression garments on intermittent exercise performance and recovery on consecutive days. Int J Sports Physiol Perform 3:454–468
Goh S, Laursen P, Dascombe B, Nosaka K (2010) Effect of lower body compression garments on submaximal and maximal running performance in cold (10°C) and hot (32°C) environments. Eur J Appl Physiol. doi:10.1007/s00421-010-1705-2
Gore SE, Laing RM, Wilson CA, Carr DJ, Niven BE (2006) Standardizing a pre-treatment cleaning procedure and effects of application on apparel fabrics. Text Res J 76:455–464
Groothuis JT, van Vliet L, Kooijman M, Hopman MTE (2003) Venous cuff pressures from 30 mmHg to diastolic pressure are recommended to measure arterial inflow by plethysmography. J Appl Physiol 95:342–347
Higgins T, Naughton GA, Burgess D (2009) Effects of wearing compression garments on physiological and performance measures in a simulated game-specific circuit for netball. J Sci Med Sport 12:223–226
Houghton LA, Dawson B, Maloney SK (2009) Effects of wearing compression garments on thermoregulation during simulated team sport activity in temperate environmental conditions. J Sci Med Sport 12:303–309
Ibegbuna V, Delis KT, Nicolaides AN, Aina O (2003) Effect of elastic compression stockings on venous hemodynamics during walking. J Vasc Surg 37:420–425
International Organization for Standardization (1993) ISO 11092: textiles—physiological effects—measurement of thermal and water-vapour resistance under steady-state conditions (sweating guarded-hotplate test). International Organization for Standardization, Geneva
International Organization for Standardization (1995a) ISO 9237: textiles–determination of the permeability of fabrics to air. International Organization for Standardization, Geneva
International Organization for Standardization (1995b) ISO 10551: ergonomics of the thermal environment—assessment of the influence of the thermal environment using subjective judgement scales. International Organization for Standardization, Geneva
International Organization for Standardization (1996) ISO 5084: textiles—determination of thickness of textiles and textile products. International Organization for Standardization, Geneva
International Organization for Standardization (2000a) ISO 6330: textiles—domestic washing and drying procedures for textile testing. International Organization for Standardization, Geneva
International Organization for Standardization (2000b) ISO 9073-6: textiles—test methods for nonwovens—Part 6: absorption. International Organization for Standardization, Geneva
International Organization for Standardization (2004) ISO 9886: ergonomics—evaluation of thermal strain by physiological measurements. International Organization for Standardization, Geneva
International Organization for Standardization (2005) ISO 139: textiles—standard atmospheres for conditioning and testing. International Organization for Standardization, Geneva
Johnson JM, Rowell LB (1975) Forearm skin and muscle vascular responses to prolonged leg exercise in man. J Appl Physiol 39:920–924
Jonker MJ, de Boer EM, Adèr HJ, Bezemer PD (2001) The oedema-protective effect of Lycra® support stockings. Dermatology 203:294–298
Kemmler W, Stengel Sv, Köckritz C, Mayhew J, Wassermann A, Zapf J (2009) Effect of compression stockings on running performance in men runners. J Strength Cond Res 23:101–105
Kraemer WJ, Bush JA, Newton RU, Duncan ND, Volek JS, Denegar CR, Canavan P, Johnston J, Putukian M, Sebastianelli WJ (1998) Influence of a compression garment on repetitive power output production before and after different types of muscle fatigue. Sports Med Training Rehabil 8:163–184
Kraemer WJ, Volek JS, Bush JA, Gotshalk LA, Wagner PR, Gómez AL, Zatsiorsky VM, Duzrte M, Ratamess NA, Mazzetti SA, Selle BJ (2000) Influence of compression hosiery on physiological responses to standing fatigue in women. Med Sci Sports Exerc 32:1849–1858
Lawrence D, Kakkar VV (1980) Graduated, static, external compression of the lower limb: a physiological assessment. Br J Surg 67:119–121
Liu R, Lao T, Kwok Y, Li Y, Ying M (2008) Effects of graduated compression stockings with different pressure profiles on lower-limb venous structures and haemodynamics. Adv Ther 25:465–478
Lord RSA, Hamilton D (2004) Graduated compression stockings (20–30 mmHg) do not compress leg veins in the standing position. ANZ J Surg 74:581–585
MacRae BA, Cotter JD, Laing RM (2011) Compression garments and exercise: garment considerations, physiology, and performance. Sports Med (in press)
Mayrovitz HN, Delgado M (1996) Effect of compression bandaging on lower extremity skin microcirculation. Wounds 8:200–206
Mayrovitz HN, Larsen PB (1997) Effects of compression bandaging on leg pulsatile blood flow. Clin Physiol 17:105–117
Mayrovitz HN, Sims N (2003) Effects of ankle-to-knee external pressures on skin blood perfusion under and distal to compression. Adv Skin Wound Care 16:198–202
Mekjavic IB, Rempel ME (1990) Determination of esophageal probe insertion length based on standing and sitting height. J Appl Physiol 69:376–379
Mitchell JW, Nadel ER, Stolwijk JA (1972) Respiratory weight losses during exercise. J Appl Physiol 32:474–476
Privett SE, George KP, Whyte GP, Cable NT (2010) The effectiveness of compression garments and lower limb exercise on post-exercise blood pressure regulation in orthostatically intolerant athletes. Clin J Sport Med 20:362–367
Rimaud D, Calmels P, Roche F, Mongold J, Trudeau F, Devillard X (2007) Effects of graduated compression stockings on cardiovascular and metabolic responses to exercise and exercise recovery in persons with spinal cord injury. Arch Phys Med Rehabil 88:703–709
Santee WR, Gonzalez RR (1988) Characteristics of the thermal environment. In: Pandolf KB, Sawka MN, Gonzalez RR (eds) Human performance physiology and environmental medicine at terrestrial extremes. Benchmark Press Inc, Indianapolis, pp 1–43
Scanlan AT, Dascombe BJ, Reaburn PRJ, Osborne M (2008) The effects of wearing lower-body compression garments during endurance cycling. Int J Sports Physiol Perform 3:424–438
Siegel S, Castellan NJ (1988) Nonparametric statistics for the behavioral sciences. McGraw-Hill, New York
Sigel B, Edelstein AL, Savitch L, Hasty JH, Felix WR (1975) Type of compression for reducing venous stasis: a study of lower extremities during inactive recumbency. Arch Surg 110:171–175
Sparrow RA, Hardy JG, Fentem PH (1995) Effect of ‘antiembolism’ compression hosiery on leg blood volume. Br J Surg 82:53–59
Sperlich B, Haegele M, Achtzehn S, Linville J, Holmberg H-C, Mester J (2010) Different types of compression clothing do not increase sub-maximal and maximal endurance performance in well-trained athletes. J Sports Sci 28:609–614
Sperlich B, Haegele M, Krüger M, Schiffer T, Holmberg H-C, Mester J (2011) Cardio-respiratory and metabolic responses to different levels of compression during submaximal exercise. Phlebology 26:102–106
Stenger MB, Brown AK, Lee SMC, Locke JP, Platts SH (2010) Gradient compression garments as a countermeasure to post-spaceflight orthostatic intolerance. Aviat Space Environ Med 81:883–887
Sugawara J, Tanabe T, Miyachi M, Yamamoto K, Takahashi K, Iemitsu M, Otsuki T, Homma S, Maeda S, Ajisaka R, Matsuda M (2003) Non-invasive assessment of cardiac output during exercise in healthy young humans: comparison between Modelflow method and Doppler echocardiography method. Acta Physiol Scand 179:361–366
Watanuki S, Murata H (1994) Effects of wearing compression stockings on cardiovascular responses. Ann Physiol Anthropol 13:121–127
Zar JH (1984) Biostatistical analysis 2nd edition. Prentice-Hall, Englewood Cliffs
Acknowledgments
We are thankful to Nigel Barrett, Dene Irvine, and Clare Nicholls for technical assistance, to Sport and Recreation New Zealand (specifically Richard Young) for supplying the garments, and to the participants for their commitment. The authors declare they have no conflicts of interest.
Conflict of interest
The authors declare they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Narihiko Kondo.
Rights and permissions
About this article
Cite this article
MacRae, B.A., Laing, R.M., Niven, B.E. et al. Pressure and coverage effects of sporting compression garments on cardiovascular function, thermoregulatory function, and exercise performance. Eur J Appl Physiol 112, 1783–1795 (2012). https://doi.org/10.1007/s00421-011-2146-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-011-2146-2