
Abstract
Purpose
The aim of the current study was to examine the impact of lower body compression garments (CG) on cardiac autonomic control of heart rate (HR) prior to, during and following submaximal exercise.
Methods
Thirty (15 males, 15 females) healthy, active adults undertook consecutive 10-min stages of supine rest, moderate–intensity upright cycling and supine recovery while wearing either normal clothing (CONTROL) or normal clothing plus CG tights in a randomised order. Heart rate (HR) and rating of perceived exertion (RPE) were assessed every minute while cardiovascular autonomic responses were assessed during the final 5 min of each stage via HR variability (HRV). The change in HR at 1-min (HRR1) and 2-min (HRR2) post-exercise and the time constant of HR recovery (HRtau) were assessed as indices of cardiac autonomic reactivation. Differences between variables were assessed via repeated measures ANOVA and corrected pairwise comparisons.
Results
Compared to rest, exercise resulted in a reduction of HRV that was similar for CONTROL and CG. A main effect for condition was identified for one non-linear, long-term HRV variable only with a significantly lower value (61.4 ± 47.8 vs. 67.1 ± 50.2 ms, p < 0.05) for CG compared to CONTROL. Cardiac autonomic reactivation (HRR1, 42.0 ± 16.8 vs. 45.5 ± 13.4 bpm; HRR2, 58.9 ± 10.5 vs. 58.9 ± 8.2 bpm; HRtau, 63.4 ± 22.3 vs. 65.1 ± 23.0 s, p > 0.05) was comparable for CONTROL and CG.
Conclusion
Lower body CG failed to alter most cardiac autonomic responses during rest, moderate-intensity exercise or recovery. Mechanisms for potential ergogenic benefits of CG remain to be characterised.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Athletes employ a wide range of methods to enhance their performance including varying training modalities, nutritional practices and recovery strategies to assist their preparation (Harty et al. 2018; Mujika et al. 2018). Of these, recovery strategies have generated immense interest in recent times including the use of cold water immersion (Dupuy et al. 2018; Maruyama et al. 2019), massage (Dupuy et al. 2018) and compression garments (CG) (Brown et al. 2017; Dupuy et al. 2018; Maruyama et al. 2019). Interest in CG use has risen with numerous benefits of CG for performance and recovery promoted including improved cycling and running performance (Broatch et al. 2018; Engel et al. 2016; Sear et al. 2010), improved anaerobic exercise performance (Ballmann et al. 2019), enhanced muscle oxygenation (Scanlan et al. 2008; Sear et al. 2010), increased blood flow (Broatch et al. 2018; Dascombe et al. 2011; Piras and Gatta 2017), reduced mean exercise heart rate (HR) (Driller and Halson 2013; Varela-Sanz et al. 2011), reduced exercise-induced muscle damage (Mizuno et al. 2017), and lower oxygen consumption during exercise (Varela-Sanz et al. 2011). However, others have reported no such beneficial effects with CG during submaximal and/or maximal exercise (Dascombe et al. 2011; Duffield et al. 2010, 2008; Sperlich et al. 2011), during recovery after repeated sprint training (Zinner et al. 2017), and for exercise-induced muscle damage, soreness and recovery (Geldenhuys et al. 2019; Goto et al. 2017; Heiss et al. 2018). Differences in CG brands, degree of compression, location of CG use, exercise modality and intensity, age, sex and health of population examined, and outcome variables assessed make conclusions about CG benefits difficult (MacRae et al. 2011). Despite these differences, CG remains topical with particular interest in the mechanisms by which CG may work.
One potential mechanism by which CG may improve exercise performance and subsequent recovery may be through the alteration in cardiac autonomic function (e.g., reduced maximum HR, accelerated HR recovery, HRR). Given that cardiac autonomic changes are blood volume-dependent (Leicht et al. 2009), CG-induced augmentation in venous return may alter HR control and contribute to lower cardiovascular stress and potentially enhanced performance. To our knowledge, few studies have examined CG use and cardiac autonomic function via heart rate variability (HRV). Medical, compression stockings were demonstrated to increase post-exercise, sympathetic activity and lower HRV in patients with spinal cord injury (Rimaud et al. 2012). Conversely and more recently, improved HRV and hemodynamic function (i.e. increased cardiac output, increased venous return, decreased peripheral resistance) were reported following maximal exercise in healthy adults using CG (Piras and Gatta 2017). The contradictory results for CG use and HRV highlight a need to investigate further the physiological effects of CG including cardiac autonomic function. Therefore, the aims of the current study were to: (1) examine the impact of lower body CG on physiological and perceptual responses during and following submaximal exercise; and (2) identify cardiac autonomic control (HRV) as a potential mechanism for CG-enhanced performance and/or recovery.
Methods
Participants
Healthy, non-smoker, active adults (15 males, 15 females) volunteered for this study with their mean age, height, mass and body mass index being 19.8 ± 1.9 years, 1.75 ± 0.09 m, 71.7 ± 12.4 kg and 23.2 ± 2.5 kg m−2, respectively. All participants completed a general pre-screening questionnaire and provided informed written consent prior to participation. All procedures were conducted in accordance with the approval of the James Cook University Human Research Ethics Committee (H3451).
Study design
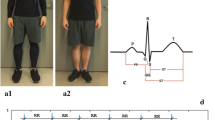
On 2 separate days, one week apart, participants undertook three consecutive 10-min stages: (1) supine rest; (2) submaximal cycling; (3) and passive supine recovery, while wearing either normal clothing (i.e. underwear, shorts, singlet, socks, shoes—CONTROL) or normal clothing and lower body CG (SKINS™ Sport, SKINS Compression Garments Pty Ltd, Australia), in a randomised order. Participants wore CG in accordance with manufacturer’s guidelines following identification of the most appropriate CG size during a familiarisation session. The degree of compression was not assessed in the current study but has been reported by others to be greatest at the medial ankle thereafter decreasing up the lower limbs (Scanlan et al. 2008). The familiarisation session was conducted approximately 1 week prior to the first testing session and also included the determination of the submaximal exercise workload. Exercise consisted of cycling at a moderate intensity recommended for maintaining health and equivalent to 70% age-predicted maximum HR (Garber et al. 2011) with the same absolute exercise workload (expressed in watts) experienced for each testing session.
Procedures
Participants refrained from food/alcohol/caffeine and physical activity for a minimum of 12 and 24 h respectively, and arrived at the laboratory in the morning (08:00–12:00) at the same time of day for each session. For female participants, menstrual cycle phase was not controlled as these hormonal fluctuations were reported to have little impact on HRV (Leicht et al. 2003). Height was determined using a stadiometer (Seca 202, Seca, Hamburg, Germany), and body mass determined via scales (TANITA TBF 521, TANITA Corporation of America, Arlington Heights, ILL). Body mass index (BMI) was calculated as mass/height in metres squared. Participants were fitted with a wireless HR monitor (TEAM POLAR2, POLAR, Kempele, Finland) and undertook supine rest on a floor mat with HR recorded every second and RR-intervals recorded beat-by-beat (i.e. sampling rate of 1 kHz). Following the resting period, participants moved to an upright cycle ergometer (MONARK 828E, Varberg, Sweden) and undertook cycling at the pre-determined moderate intensity workload. At the end of the submaximal cycling bout, participants relocated to the floor mat within 10 s for the supine recovery period. Throughout each session, participants were monitored for HR, rating of perceived exertion (RPE) using Borg’s 6–20 scale (Borg 1982) each minute during exercise and recovery; and blood capillary lactate (La) levels via an ACCUTREND analyser (Roche, Mannheim, Germany) at the end of rest, within the last minute of exercise and 5 and 10 min, post-exercise. Breathing was spontaneous and natural throughout all stages with HRV responses reported to be similar between spontaneous and metronome-based breathing during rest and sympathetic challenges (Patwardhan et al. 1995).
Data analysis
Average HR, RPE and HRV were assessed during the final 5 min of each 10-min stage (i.e. rest, steady state exercise and recovery). For each stage, RR-intervals were identified using the POLAR detection threshold and then exported for later analysis using dedicated HRV analysis software (KUBIOS, Biosignal Analysis and Medical Imaging Group, Department of Physics, University of Kuopio, Kuopio, Finland). Recordings were analysed as previously described (Leicht et al. 2011) with the following linear and non-linear HRV measures examined: standard deviation of all normal-normal RR intervals (SDNN); root mean square of successive differences in normal-normal RR intervals (RMSSD); percentage of successive normal-normal RR intervals different by more than 50 ms (pNN50); low (LF, 0.04–0.15 Hz) and high frequency (HF, 0.15–0.4 Hz) components in absolute (ms2) and normalised units (nu); LF/HF ratio; short (SD1, reflecting short-term instantaneous RR modulation) and long (SD2, long-term RR modulation) axes of the Poincare plot; Sample entropy (SampEn); and short- (α1) and long-term (α2) fractal scaling exponents. Both linear and non-linear HRV measures were examined as reproducible measures during short-term recordings (Maestri et al. 2007). During recovery, the absolute change in HR during the first (HRR1) and second (HRR2) minute (Fecchio et al. 2019), as well as the rate of change or time constant of HR recovery (HRtau) were also examined as indicators of parasympathetic reactivation, as previously described (Pierpont et al. 2000). The HRtau was calculated by fitting a first-order exponential curve (Sigmaplot™, SPSS Inc, Chicago, ILL) to the HR data recorded each second (Pierpont et al. 2000) with the fit of each curve assessed by the correlation coefficient (R).
Statistical analysis
All data (mean ± standard deviation) were analysed using the Statistical Package for the Social Sciences (SPSS Inc., Chicago, ILL) with normality confirmed via the Kolmogorov–Smirnov statistic with a Lilliefors significance correction. Significant differences between variables were examined using 1-way (condition) or 2-way (condition × time) repeated measures ANOVA and post-hoc pairwise comparisons with a Bonferroni correction. A p value < 0.05 was set as the level of significance. Based upon prior work examining HRV during CG use (Piras and Gatta 2017), and during blood volume changes via intravenous saline (Leicht et al. 2009), a sample of at least 16 participants was required to detect a significant difference (p < 0.05, 90% power) in frequency and non-linear measures of HRV.
Results
The submaximal exercise workload completed by participants was similar between CONTROL and CG sessions (119 ± 30 Watts) and equated to a similar relative exercise intensity (71.2 ± 4.4% vs. 71.5 ± 5.0% age-predicted maximum HR, p > 0.05).
As expected, HR was stable at rest, increased significantly (p < 0.001) during exercise and then decreased during recovery (Fig. 1a). No effect of condition or interaction between factors were identified for HR (Table 1). Similarly, RPE increased during exercise (p < 0.001) and thereafter decreased during recovery (Fig. 1b). No main effect for condition (p = 0.321) or interaction between factors (p = 0.628) were evident for RPE. During exercise, La increased and remained above resting levels during recovery (p < 0.001, Fig. 1c). No effect of condition (p = 0.796) or interaction (p = 0.414) was evident for La.

Mean (± standard deviation) heart rate (a), rating of perceived exertion (b) and blood lactate (c) prior to (rest), during (exercise) and following (recovery) submaximal cycling with (CG) and without (CONTROL) lower body compression garments
A significant main effect for time was identified for all HRV measures with lower HRV during exercise compared to rest for most measures (Table 1). No significant main effect for condition was noted for HRV measures (Table 1) except for SD2, which was significantly greater for CONTROL compared with CG (67.1 ± 50.2 ms vs. 61.4 ± 47.8 ms, p = 0.048). A significant interaction effect was identified for SampEn (p = 0.047) with this effect reinforcing the main effect of time (Table 1).
During recovery, the fit for each HRtau curve was excellent with the average R being similar for CONTROL and CG (0.949 ± 0.035 vs. 0.949 ± 0.027, p = 0.845). There were no significant main effects for condition (CONTROL vs. CG) on HRR1 (42.0 ± 16.8 vs. 45.5 ± 13.4 bpm, p = 0.246), HRR2 (58.9 ± 10.5 vs. 58.9 ± 8.2 bpm, p = 1.000) or HRtau (63.4 ± 22.3 vs. 65.1 ± 23.0 s, p = 0.679).
Discussion
The current study identified that, compared to the CONTROL session, lower body CG had minimal impact on physiological and perceptual responses during and following submaximal exercise in healthy adults. Further, the majority of cardiac autonomic control measures (i.e. HRV, HRR) was unaltered during CG use with this cardiovascular mechanism unlikely to be a key contributor to any potential CG enhancements during submaximal exercise performance or immediate recovery in healthy adults. The mechanisms for, and ergogenic benefits of, CG use during and following exercise remains to be clarified.
Prior studies have reported mixed results for CG-induced benefits of exercise performance and recovery with both positive (Ballmann et al. 2019; Broatch et al. 2018; Dascombe et al. 2011; Driller and Halson 2013; Engel et al. 2016; Mizuno et al. 2017; Piras and Gatta 2017; Scanlan et al. 2008; Sear et al. 2010; Varela-Sanz et al. 2011) and negative-minimal (Dascombe et al. 2011; Duffield et al. 2010, 2008; Geldenhuys et al. 2019; Goto et al. 2017; Heiss et al. 2018; Sperlich et al. 2011) findings. The current study adds further support to the negative-minimal effects of CG with similar cardiac autonomic control (i.e. HRV and HRR) to that of a non-CG experience (CONTROL). While most HRV measures were similar between conditions, a main effect for SD2 was observed with significantly greater (~ 9%) values and long-term modulation for CONTROL compared with CG. This result suggested an autonomic impairment with CG however, was likely a result of a greater rest value during the CONTROL session with similar values during and following exercise (Table 1) that confirm the lack of cardiac autonomic control change with CG use. Our HRV findings were in contrast to prior work that reported greater recovery (improved HRV and hemodynamic parameters) after maximal aerobic performance (Piras and Gatta 2017). Differences in exercise intensity (submaximal vs. maximal) likely explain the discrepancy with maximal exercise inducing greater changes in cardiac autonomic activity and blood flow compared to submaximal exercise (White and Raven 2014). Consequently, the degree of physiological change during exercise may be important to observe any benefits of CG with further studies needed to clearly document CG advantages.
Based upon prior work, it was postulated that CG would augment muscle blood flow and venous return (Broatch et al. 2018; Dascombe et al. 2011; Piras and Gatta 2017) and subsequent blood-volume, dependent changes in cardiac autonomic control (Leicht et al. 2009). However, no change in cardiac autonomic outcome was observed and may indicate minimal changes in localised blood flow and venous return during the current CG use. Increased venous return via CG was reported to aid the removal of muscle metabolites including La (Berry and McMurray 1987; MacRae et al. 2011) with the current results of similar La responses for both CG and CONTROL sessions adding support to minimal changes in La clearance, and likely localised muscle blood flow contributing to venous return, in the current study (not assessed). Our findings are in line with previous studies reporting no beneficial effects of CG on blood La clearance (Broatch et al. 2018; Duffield et al. 2010). Future studies are encouraged to examine localised muscle blood flow and its contributions to venous return and central blood volume as potential contributors to CG-induced responses during and following exercise. Further, differences in CG brands and degree of compression may be crucial when examining CG benefits (MacRae et al. 2011). It was possible that the degree of compression used in the current study was not sufficient to induce changes in localised blood flow with greater compression needed to alter venous return and provide physiological benefits such as changes in HRV, HRR, etc. Previously, medical graduated compression stockings resulted in greater HF and a slight suppression of HR (~ 4–5 bpm) after an hour of seated rest compared to a non-stocking condition, possibly as a result of increased venous return that was not assessed (Horiuchi et al. 2018). Similar resting HR and HRV was observed between CONTROL and CG sessions in the current study, with the degree and time of compression (10 min vs. > 1 h), as well as resting position (supine vs. seated), likely to explain differences between the current and prior study. Subsequently, it was unlikely that commercial CG use over a short timeframe (~ 10 min), as examined in the current study, was able to alter localised blood flow, and subsequently venous return, sufficiently to impact upon resting HR and HRV. Further studies may clarify the role of CG and degree of compression on localised blood flow and venous return, and subsequent cardiac autonomic affects.
This study has shown uniquely, the minimal effects of CG on exercise and recovery cardiac autonomic control for young healthy adults. However, some limitations of the current study should be acknowledged. Firstly, a single bout of upright, submaximal, cycling exercise was examined with the impact of other exercise intensities (e.g. relative or absolute including maximal exercise), modes (e.g. running), positions (supine vs upright), and/or multiple bouts potentially contributing to different results. Secondly, a single, commercial CG brand was examined with other CG brands and/or varying degrees of compression needing further investigation to verify the ergogenic benefits, and their mechanisms, of CG. Thirdly, CG were used during supine rest/recovery and upright exercise with different positions potentially influencing cardiac autonomic function (da Cruz et al. 2019). Next, muscle blood flow, central blood volume and venous return was not assessed to confirm its mechanistic role with CG use and future studies are encouraged to include these assessments. Lastly, a modest sample of young, healthy and active adults were studied that may limit the generalisability of the current results to all populations. The current study examined a larger sample of participants compared to prior reports of HRV and CG (Piras and Gatta 2017; Rimaud et al. 2012), and participant types likely to be the predominant buyers/users of CG that will assist future work.
Conclusions
The current study identified that lower body CG had minimal impact on physiological and perceptual responses during and following submaximal exercise in young, healthy adults. Further, cardiac autonomic control was unaffected during CG use and unlikely to be a primary mechanism for potential CG enhancements during submaximal exercise or immediate recovery. The ergogenic benefits of CG use during and following submaximal exercise remain to be elucidated.
Abbreviations
- α1:
-
Short-term fractal scaling exponent
- α2:
-
Long-term fractal scaling exponent
- CG:
-
Compression garments
- HF:
-
High (0.15–0.4 Hz)-frequency component of HRV
- HR:
-
Heart rate
- HRR1:
-
Change in heart rate during the first minute of recovery
- HRR2:
-
Change in heart rate during the first 2 min of recovery
- HRtau :
-
Time constant of heart rate change during recovery
- HRV:
-
Heart rate variability
- La:
-
Capillary blood lactate
- LF:
-
Low (0.04–0.15 Hz) frequency component of HRV
- LF/HF:
-
Ratio of low to high frequency components of HRV
- ms:
-
Milliseconds
- nu:
-
Normalised units
- pNN50:
-
Percentage of successive normal-normal RR intervals different by more than 50 ms
- RPE:
-
Rating of perceived exertion
- RMSSD:
-
Root mean square of successive differences in normal-normal RR intervals
- SampEn:
-
Sample entropy
- SD1:
-
Short axis of the Poincare plot—short-term instantaneous RR modulation
- SD2:
-
Long axis of the Poincare plot—long-term RR modulation
- SDNN:
-
Standard deviation of all normal–normal RR intervals
References
Ballmann C, Hotchkiss H, Marshall M, Rogers R (2019) The effect of wearing a lower body compression garment on anaerobic exercise performance in Division I NCAA basketball players. Sports 7(6).
Berry MJ, McMurray RG (1987) Effects of graduated compression stockings on blood lactate following an exhaustive bout of exercise. Am J Phys Med 66(3):121–132
Borg GA (1982) Psychophysical bases of perceived exertion. Med Sci Sports Exerc 14(5):377–381
Broatch JR, Bishop DJ, Halson S (2018) Lower limb sports compression garments improve muscle blood flow and exercise performance during repeated-sprint cycling. Int J Sports Physiol Perform 13(7):882–890
Brown F, Gissane C, Howatson G, van Someren K, Pedlar C, Hill J (2017) Compression garments and recovery from exercise: a meta-analysis. Sports Med 47(11):2245–2267
da Cruz CJG, Porto LGG, da Silva RP, de Souza PD, Garcia GL, Molina GE (2019) Impact of heart rate on reproducibility of heart rate variability analysis in the supine and standing positions in healthy men. Clinics (Sao Paulo) 74:e806
Dascombe BJ, Hoare TK, Sear JA, Reaburn PR, Scanlan AT (2011) The effects of wearing undersized lower-body compression garments on endurance running performance. Int J Sports Physiol Perform 6(2):160–173
Driller MW, Halson SL (2013) The effects of wearing lower body compression garments during a cycling performance test. Int J Sports Physiol Perform 8(3):300–306
Duffield R, Edge J, Merrells R, Hawke E, Barnes M, Simcock D, Gill N (2008) The effects of compression garments on intermittent exercise performance and recovery on consecutive days. Int J Sports Physiol Perform 3(4):454–468
Duffield R, Cannon J, King M (2010) The effects of compression garments on recovery of muscle performance following high-intensity sprint and plyometric exercise. J Sci Med Sport 13(1):136–140
Dupuy O, Douzi W, Theurot D, Bosquet L, Dugue B (2018) An evidence-based approach for choosing post-exercise recovery techniques to reduce markers of muscle damage, soreness, fatigue, and inflammation: a systematic review with meta-analysis. Front Physiol 9:403
Engel FA, Holmberg HC, Sperlich B (2016) Is there evidence that runners can benefit from wearing compression clothing? Sports Med 46(12):1939–1952
Fecchio RY, Brito L, Leicht AS, Forjaz CLM, Pecanha T (2019) Reproducibility of post-exercise heart rate recovery indices: a systematic review. Auton Neurosci Basic Clin 221:102582
Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, Nieman DC, Swain DP, American College of Sports M (2011) American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 43(7):1334–1359
Geldenhuys AG, Swart J, Bosch A (2019) Investigation of the impact of below-knee compression garments on markers of exercise-induced muscle damage and performance in endurance runners: a prospective randomized controlled trial. Sports Health 11(3):254–264
Goto K, Mizuno S, Mori A (2017) Efficacy of wearing compression garments during post-exercise period after two repeated bouts of strenuous exercise: a randomized crossover design in healthy, active males. Sports Med Open 3(1):25
Harty PS, Zabriskie HA, Erickson JL, Molling PE, Kerksick CM, Jagim AR (2018) Multi-ingredient pre-workout supplements, safety implications, and performance outcomes: a brief review. J Int Soc Sports Nutr 15(1):41
Heiss R, Hotfiel T, Kellermann M, May MS, Wuest W, Janka R, Nagel AM, Uder M, Hammon M (2018) Effect of compression garments on the development of edema and soreness in delayed-onset muscle soreness (DOMS). J Sports Sci Med 17(3):392–401
Horiuchi M, Takiguchi C, Kirihara Y, Horiuchi Y (2018) Impact of wearing graduated compression stockings on psychological and physiological responses during prolonged sitting. Int J Environ Res Public Health 15(8)
Leicht AS, Hirning DA, Allen GD (2003) Heart rate variability and endogenous sex hormones during the menstrual cycle in young women. Exp Physiol 88(3):441–446
Leicht AS, Sinclair WH, Patterson MJ, Rudzki S, Tulppo MP, Fogarty AL, Winter S (2009) Influence of postexercise cooling techniques on heart rate variability in men. Exp Physiol 94(6):695–703
Leicht AS, Crowther RG, Golledge J (2011) Influence of peripheral arterial disease and supervised walking on heart rate variability. J Vasc Surg 54(5):1352–1359
MacRae BA, Cotter JD, Laing RM (2011) Compression garments and exercise: garment considerations, physiology and performance. Sports Med 41(10):815–843
Maestri R, Pinna GD, Porta A, Balocchi R, Sassi R, Signorini MG, Dudziak M, Raczak G (2007) Assessing nonlinear properties of heart rate variability from short-term recordings: are these measurements reliable? Physiol Meas 28(9):1067–1077
Maruyama T, Mizuno S, Goto K (2019) Effects of cold water immersion and compression garment use after eccentric exercise on recovery. J Exerc Nutr Biochem 23(1):48–54
Mizuno S, Arai M, Todoko F, Yamada E, Goto K (2017) Wearing compression tights on the thigh during prolonged running attenuated exercise-induced increase in muscle damage marker in blood. Front Physiol 8:834
Mujika I, Halson S, Burke LM, Balague G, Farrow D (2018) An integrated, multifactorial approach to periodization for optimal performance in individual and team sports. Int J Sports Physiol Perform 13(5):538–561
Patwardhan AR, Evans JM, Bruce EN, Eckberg DL, Knapp CF (1995) Voluntary control of breathing does not alter vagal modulation of heart rate. J Appl Physiol 78(6):2087–2094
Pierpont GL, Stolpman DR, Gornick CC (2000) Heart rate recovery post-exercise as an index of parasympathetic activity. J Auton Nerv Syst 80(3):169–174
Piras A, Gatta G (2017) Evaluation of the effectiveness of compression garments on autonomic nervous system recovery after exercise. J Strength Cond Res 31(6):1636–1643
Rimaud D, Calmels P, Pichot V, Bethoux F, Roche F (2012) Effects of compression stockings on sympathetic activity and heart rate variability in individuals with spinal cord injury. J Spinal Cord Med 35(2):81–88
Scanlan AT, Dascombe BJ, Reaburn PR, Osborne M (2008) The effects of wearing lower-body compression garments during endurance cycling. Int J Sports Physiol Perform 3(4):424–438
Sear JA, Hoare TK, Scanlan AT, Abt GA, Dascombe BJ (2010) The effects of whole-body compression garments on prolonged high-intensity intermittent exercise. J Strength Cond Res 24(7):1901–1910
Sperlich B, Haegele M, Kruger M, Schiffer T, Holmberg HC, Mester J (2011) Cardio-respiratory and metabolic responses to different levels of compression during submaximal exercise. Phlebology 26(3):102–106
Varela-Sanz A, Espana J, Carr N, Boullosa DA, Esteve-Lanao J (2011) Effects of gradual-elastic compression stockings on running economy, kinematics, and performance in runners. J Strength Cond Res 25(10):2902–2910
White DW, Raven PB (2014) Autonomic neural control of heart rate during dynamic exercise: revisited. J Physiol 592(12):2491–2500
Zinner C, Pelka M, Ferrauti A, Meyer T, Pfeiffer M, Sperlich B (2017) Responses of low and high compression during recovery after repeated sprint training in well-trained handball players. Eur J Sport Sci 17(10):1304–1310
Acknowledgements
The authors would like to thank SKINS™ (Australia) for their generous donation of compression garments; and Brett Fforde, Lewan Parker and the numerous students who assisted with this study.
Author information
Authors and Affiliations
Contributions
AL and FN conceived and designed the study with AL collecting/analysing the data. All authors (AL, MA, FN) interpreted results, wrote the manuscript, and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The current study was conducted in accordance with the laws of Australia and the National Statement on Ethical Conduct in Human Research by the National Health and Medical Research Council. All procedures were conducted in accordance with the approval of the James Cook University Human Research Ethics Committee (H3451).
Additional information
Communicated by Massimo Pagani.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Leicht, A.S., Ahmadian, M. & Nakamura, F.Y. Influence of lower body compression garments on cardiovascular autonomic responses prior to, during and following submaximal cycling exercise. Eur J Appl Physiol 120, 1601–1607 (2020). https://doi.org/10.1007/s00421-020-04391-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-020-04391-9