
Abstract
Purpose
To investigate sports compression garment (CG)-induced recovery hemodynamics and their potential impact on subsequent cycling performance.
Methods
In a randomized crossover design, 13 physically active men (20.9 ± 1.4 years; 65.9 ± 7.8 kg; 173.3 ± 4.8 cm; peak power output 254.2 ± 27.2 W) underwent 2 experimental trials. During each experimental trial, the subjects performed 20-min fatiguing preload cycling followed by 60-min passive recovery wearing either a sports CG (28.6 ± 9.4 mmHg) or gymnastic pants (CON). A 5-min all-out cycling performance test was subsequently conducted and power output and cadence were recorded. Cardiac output (CO) and stroke volume (SV) were measured using Doppler ultrasound (USCOM®). Heart rate (HR), blood lactate [BLa−], ratings of perceived exertion (RPE), leg muscle soreness (LMS), mean arterial pressure (MAP) and systemic vascular resistance (SVR) were monitored at 5, 15, 30, 45, 60 min during passive recovery.
Results
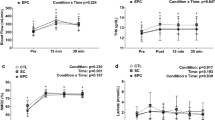
During the subsequent 5-min all-out cycling performance test, power output (215.2 ± 24.0 vs. 210.8 ± 21.5 W, CG vs. CON) and cadence (72.5 ± 3.8 vs. 71.2 ± 4.8 rpm, CG vs. CON) were higher in CG than CON (P < 0.05). SV was higher at 15, 30 and 45 min (P < 0.05), CO was higher at 5 and 45 min (P < 0.05), HR was lower at 15 and 30 min (P < 0.05) and [BLa−] was lower at 5 and 15 min (P < 0.05) during passive recovery, while LMS was lower at all time-points (P < 0.05) compared with CON.
Conclusion
Sports CG improves subsequent cycling performance by enhancing hemodynamic responses and attenuating perceived muscle soreness during passive recovery in physically active men.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Wearing sports compression garments (CG) has been suggested as an effective recovery strategy for multisport athletes to endure frequent training, and may benefit subsequent exercise performance (Brown et al. 2017; de Glanville and Hamlin 2012). The claimed benefits of CG in terms of enhanced exercise performance (Ali et al. 2010; MacRae et al. 2012) and recovery (Chatard et al. 2004; Driller and Halson 2013; Menetrier et al. 2013) remain controversial, with contradictory findings from studies (Ali et al. 2007; Chan et al. 2016; Goto et al. 2017; Stickford et al. 2015) due to diverse experimental settings and the type of CG used. Although recent reviews suggest that sports CG may enhance recovery performance, reduce perceived exertion and the severity of delayed onset muscle soreness (DOMS), the potential mechanisms and relationship between sports CG and enhanced recovery remain elusive (Beliard et al. 2015; Brown et al. 2017; Engel et al. 2016; Hill et al. 2014a).
The major claimed physiological benefit of wearing sports CG is to enhance cardiovascular performance by improving hemodynamic responses; i.e., enhancing venous return, which increases cardiac output (CO) and stroke volume (SV) (Born et al. 2013; Lee et al. 2020; MacRae et al. 2011). Limited studies have examined CG-induced hemodynamic responses during exercise (MacRae et al. 2012; Sperlich et al. 2011) and have reported contradictory findings. Sperlich et al. (2011) found no significant improvement in CO and SV using rebreathing techniques during submaximal running with compression socks in well-trained male endurance athletes. In contrast, using finger photoplethysmography, MacRae et al. (2012) reported higher CO during submaximal cycling in trained male cyclists wearing a full-body sports CG. The discrepancy in findings may be attributed to the fact that hemodynamic responses vary considerably when different body parts are covered by CG (MacRae et al. 2011). Furthermore, differences in measuring methods, applied compression pressure and exercise modality may contribute to the disparity between findings. In addition, recently published studies report the positive effects of CG on post-exercise hemodynamic responses (Dorey et al. 2018; Piras and Gatta 2017) and psychological responses (Smale et al. 2018) however, they do not examine the subsequent exercise performance. While the aforementioned studies have provided some evidence on CG-induced hemodynamic responses during exercise (MacRae et al. 2012; Sperlich et al. 2011) and post-exercise (Dorey et al. 2018; Piras and Gatta 2017; Smale et al. 2018), such effects, during recovery in addition to subsequent exercise, warrant further investigation.
Studies examining the direct effect of compression pressure on hemodynamic responses during recovery are limited (Beliard et al. 2015; Brown et al. 2017). In addition to heart rate (HR), Doppler ultrasound can accurately monitor CO and SV non-invasively at rest (Zhang et al. 2016). Previous CG studies on recovery performance have focused on the evaluation of blood biomarkers (Hill et al. 2014b, 2017), post-recovery jumping performance (Hill et al. 2017) and subjective muscle soreness (Hill et al. 2014b, 2017). We previously demonstrated, using Doppler ultrasound, that wearing CG positively influenced hemodynamic responses during an orthostatic challenge in healthy individuals (Lee et al. 2018, 2019). Our published data revealed that a compression at calf (38.8 ± 4.4 mmHg), knee (26.2 ± 4.3 mmHg) and thigh (21.3 ± 2.3 mmHg) enhanced CO and SV in physically active individuals at rest (Lee et al. 2019). Wearing CG during post-exercise recovery possibly improve venous return, thereby enhancing CO and SV (Lee et al. 2020; Lim and Davies 2014), which reduce exercise-induced CK concentration (Hill et al. 2014a) and DOMS (Engel et al. 2016; Hill et al. 2014a; Marques-Jimenez et al. 2016) and enhance recovery (Born et al. 2013; MacRae et al. 2011). Since the experimental design was without exercise in these studies (Lee et al. 2018, 2019), the extrapolation of the findings may not be valid for the purported hemodynamic responses during passive recovery between exercise bouts.
Numerous studies have used ratings of perceived exertion (RPE) to evaluate the subjective sense of effort toward wearing CG (Ali et al. 2010; Brophy-Williams et al. 2017; Chan et al. 2016; Chatard et al. 2004; MacRae et al. 2012). Moreover, wearing of graduated compression stockings during a submaximal run was reported to attenuate the post-exercise leg muscle soreness in trained triathletes (Ali et al. 2010) however, limited published studies have reported on the effects of CG between exercises on RPE (Brophy-Williams et al. 2017; Chatard et al. 2004). In the current study, by monitoring of RPE between exercises may provide a new perspective for understanding the comprehensive mechanism and compression garment use and recovery performance, and be of practical utility for physically active populations seeking frequent exercise.
This study aimed to examine the effect of wearing sports CG on (1) hemodynamic responses during passive recovery between exercise using Doppler ultrasound (USCOM®, Sydney, Australia) (Lee et al. 2018, 2019), (2) subsequent exercise performance, and (3) the leg muscle soreness and biomarkers in physically active individuals. It was hypothesized that sports CG would improve biomarkers and hemodynamic responses by increasing SV and CO while decreasing HR during passive recovery after fatiguing preload exercise and enhance subsequent exercise performance and attenuate leg muscle soreness.
Methods
Participants
Thirteen healthy male participants (age: 20.9 ± 1.4 years; height: 173.3 ± 4.8 cm; weight: 65.9 ± 7.8 kg; Peak Power Output (PPO): 254.2 ± 27.2 W, Table 1) with no history of unexplained syncope, leg venous insufficiency or artificial/metal implants were recruited for the study. The participants were physically active, engaging in recreational physical activity for ≥ 5 h per week.
Experimental design
The participants attended six separate testing sessions over 4 weeks at the laboratory (20–22 °C and 40–50% relative humidity). During week 1, the participants underwent preliminary measurements and measured the pressure exerted by CG (Table 2), then completed an incremental cycling test to establish PPO. In week 2, the participants completed two full fatiguing preload cycling as familiarization trials, separated by 4 days. The participants completed a 24-h food diary before the first familiarization trial and replicated those diets as closely as possible before the second familiarization trial and subsequent experimental trials. In week 3, another incremental cycling test was conducted to establish the final PPO for each subject. In the fourth and final week, two experimental trials (Fig. 1) were conducted using a randomized, crossover design with participants wearing either sports CG or gymnastic pants (CON) during a subsequent 60-min passive recovery period, with each trial separated by 4 days. Each subject refrained from strenuous exercise and caffeine intake for at least 24 and 12 h, respectively, prior to each trial. In addition, the participants consumed 500 mL of water 3 h prior to each trial to ensure good hydration. Upon arrival at the laboratory, a standardized breakfast with a carbohydrate drink (Pocari Sweat; 6% carbohydrate content) and muesli bars (PowerBar; 20 g of carbohydrate per bar) were provided to participants to be consumed ad libitum in their first trial, with consumption levels matched for the subsequent trials. Then, it was followed by 30 min of seated rest before undertaking trials. All testing was performed at the same time of day and the tests were performed on the same cycle ergometer.

Schematic diagram of the experimental trial. Fatiguing preload cycling based on 30%, 40%, 65% and 85% of peak power output. CG sports compression garment, CON control garment, USCOM® hemodynamic measurements using Doppler ultrasound, RPE ratings of perceived exertion, LMS leg muscle soreness, [BLa−] blood lactate, HR heart rate
Exerted pressure
A pressure monitor (PicoPress 35020 Ponte S. Nicolò PD, Italy) with three transducers of 50 mm in caliber was positioned at the right calf, knee and thigh before donning the garment to measure the exerted pressure (Lee et al. 2019). The exerted pressure at these landmarks was measured while the participants were in a standing position.
Incremental test
To determine the participants’ PPO, an incremental test was conducted on a cycle ergometer (Monark LC7, Stockholm, Sweden) and the protocol was described elsewhere (Driller and Halson 2013). During the test, the participants were encouraged to give maximal effort. PPO was determined using the following formula:
where Wcompleted is the power output for the last full workload completed, t is the time in seconds for which the final uncompleted workload was sustained, 60 is the target number of seconds in each workload, and 25 is the workload increment in watts as previously stated (Driller and Halson 2013).
Familiarization trials
The participants wore identical sporting attire during all familiarization cycling trials. They underwent 20 min of fatiguing preload cycling, consisting of four 5-min bouts performed at 30%, 40%, 65% and 85% PPO (Menetrier et al. 2013). The CO, SV, HR, mean arterial pressure (MAP) and systemic vascular resistance (SVR), perceptual and affective responses and blood lactate [BLa−] were measured pre- and post-familiarization trials while the participants remained seated on the ergometer.
Experimental trial
It involved identical fatiguing preload cycling as in the familiarization trials, followed by 60 min of passive recovery in a semi-reclined position after either a sports CG or CON garment was donned within 3 min after the fatiguing preload cycling, followed by a 5-min all-out cycling performance test (PT) wearing identical sports attire as during the fatiguing preload cycling (Fig. 1). During the PT, participants were encouraged to give maximal effort and to produce the greatest mean possible power output for the whole 5-min cycling bout, and the time countdown was the only information communicated to the participants (Driller and Halson 2013; Menetrier et al. 2013). The participants were fitted with a heart rate chest strap (ANT + Soft Strap Premium Heart Rate Monitor, Garmin International, Kansas City, MO) and HR was recorded at the same time point of hemodynamic responses. The average power output and cadence were calculated for each cycling stage. Hemodynamic responses and leg muscle soreness (LMS) were measured while the participants remained seated on the ergometer pre- and post-fatiguing preload cycling, at 5, 15, 30, 45 and 60 min during passive recovery (semi-reclined position) and post-PT, using USCOM®; finger prick blood samples were then taken and [BLa−] (L+, Nova Biomedical, USA) was measured (Fig. 1). During the PT, the participants were not informed of their performance results.
Hemodynamics examination by USCOM
The USCOM (a noninvasive transcutaneous Doppler ultrasound device) was used to measures CO intermittently. A handheld probe placed in the sternal notch was used to insonate the blood flow across the aortic valve by an experienced investigator; SV was calculated as the product of the velocity time integral and aortic valve cross-sectional area derived using an internal algorithm based on the height of participant; MAP and SVR were also derived using an internal algorithm in USCOM (Lee et al. 2018, 2019; Zhang et al. 2016). Baseline CO, SV, HR, MAP and SVR were obtained after the participants underwent 10 min of seated rest or reached a steady HR on the ergometer before the experimental trials. After the fatiguing preload cycling and PT, the participants were seated upright on the ergometer and all hemodynamic measurements were repeated within 2 min (Lee et al. 2018, 2019).
Lower-body compression garments
The sports CG consisted of a combination of commercially available sports compression flex leg sleeves (UA 3568b, 2XU, Melbourne, Australia) worn on top of sport compression tights (MA1959b, 2XU, Melbourne, Australia), the size and design were according to the previous study (Lee et al. 2019). The CON consisted of gymnastic pants made of 80% polyester and 20% elastane, sourced from a local market.
Perceptual and affective responses
RPE was assessed with a modified Borg scale from 0 (rest) to 10 (maximal). LMS was monitored at the right leg at six anatomical landmarks (Ali et al. 2010) with a hand-held pressure algometer (FDIX, Wagner Instruments, Greenwich, CT) and a visual analog scale (VAS) (Goddard et al. 2004). Likert scales were used to assess comfort, tightness and any associated pain from wearing the CG and CON throughout the trials and the participants rated each variable from 1 (very uncomfortable, slack/loose, no pain) to 10 (very comfortable, very tight, very painful) (Ali et al. 2010).
Statistical analyses
Data are reported as mean ± SD. Two-way repeated measures analysis of variance (ANOVA) with repeated factors was used to explore differences in cycling power output and cadence, [BLa−], perceptual responses and hemodynamic responses between the CG and CON trials and the interactions between variables. When significant differences between interventions were identified, paired t tests, using the Holm–Bonferroni adjustment, were applied. To compare the practical relevance and meaningfulness of the various findings, effect sizes (d; 0.20, 0.50 and 0.80; small, medium and large, respectively) were calculated (Cohen 1988). SPSS (Version 20, Chicago, IL) was used for all analyses. The level of significance was set at P < 0.05.
Results
All participants completed all trials. An interaction of garment × time was observed for W (P = 0.01) and cadence (P = 0.02), with a higher W (P = 0.03; Fig. 2) and cadence during the PT in CG than in CON (P = 0.04; Table 3). There was no main effect of garment on W (P = 0.65) and cadence (P = 0.25), and the overall cadence was similar (P = 0.11; Table 3) between the CG and CON trials. An effect of time was observed on W (P < 0.001), increasing throughout the fatiguing preload cycling until the PT (Table 3).

Mean power output of all participants completing 5-min all-out cycling performance test (PT) in different trials; filled bars show mean ± SD, whereas lines represent individual performance. CG sports compression garment trial, CON control garment trial
An interaction of garment × time (P < 0.001) was observed for [BLa−], such that [BLa−] was lower at 5 min (P < 0.001) and 15 min (P = 0.004) during passive recovery with CG than with CON (Table 4). There was a main effect of garment on [BLa−] (5.3 ± 0.8 vs. 5.9 ± 1.0 mmol·L−1, CG vs. CON; P = 0.03; Cohen’s d = 0.7). Moreover, a main effect of time on [BLa−] was observed; it decreased during passive recovery and increased at post-PT (P < 0.05; Table 4).
Interaction of garment × time for SV (P = 0.001), CO (P = 0.012) and HR (P = 0.017) were found. SV was higher at 15 min (P = 0.01), 30 min (P = 0.01) and 45 min (P = 0.02) during passive recovery and at post-PT with CG than with CON (Table 4). CO was higher at 5 min (P = 0.04) and 45 min (P = 0.04) during passive recovery (Table 4) and HR was lower at 15 min (P = 0.04) and 30 min (P = 0.04, Table 4) in CG than CON. There was a main effect of garment on SV (51.9 ± 16.2 vs. 47.8 ± 14.6 cm3; CG vs. CON; P = 0.02; Cohen’s d = 0.3) as well as a main effect of time on SV (P = 0.014). SV decreased throughout passive recovery and increased at post-PT (Table 4). CO was similar between garments (P = 0.074) but a main effect of time was observed (P < 0.001); CO decreased throughout passive recovery (Table 4). There was no main effect of garment on HR but there was a main effect of time (P < 0.001); HR decreased during passive recovery (Table 4). A main effect of time was observed (P < 0.001) on MAP; however, no difference was found between time points after Bonferroni adjustment (P > 0.05; Table 4). There was no main effect of garment (P > 0.05) and no interaction of garment × time for MAP (Table 4). There was a main effect of time on SVR (P < 0.001); SVR increased during passive recovery and was lower at post-PT (Table 4). There was no main effect of garment (P > 0.05) and no interaction of garment × time on SVR (P > 0.05; Table 4).
There was an interaction of garment × time on LMS (P < 0.001), with LMS lower in CG than CON throughout passive recovery (P < 0.001; Table 4). However, LMS was similar at post-PT for both garments (P = 0.36; Table 4). Furthermore, LMS was lower in CG (17.2 ± 9.9 vs. 26.7 ± 11.0, CG vs. CON; P = 0.001; Cohen’s d = 0.9) and increased over time (P < 0.001; Table 4). RPE decreased over time (P < 0.001) but there was no garment (P = 0.073) or interaction (P = 0.14) effects (Table 4).
Discussion
The aim of this study was to examine the effects of wearing CG on recovery responses (hemodynamics, biomarkers and LMS) and their potential impact on subsequent exercise performance. The main findings were that CG induced (1) higher SV and CO and lower HR during passive recovery, (2) lower [BLa−] and LMS during passive recovery and 3) enhanced subsequent exercise performance.
This is the first study to measure CG-induced hemodynamic responses using Doppler ultrasound (USCOM®) during passive recovery after fatiguing exercise. We observed a higher SV and CO and lower HR throughout passive recovery with CG, affirming the increase in venous return (Avril et al. 2010) and the postulated hemodynamic advantages of wearing a CG (Born et al. 2013; MacRae et al. 2011). An improvement in local blood flow with compression stockings has been previously demonstrated in chronic venous disease patients (Mosti and Partsch 2014). Researchers suggested that the calf is more compressible than other parts of the leg, therefore wearing compression stockings can effectively reduce blood pooling and improve venous return of the legs at rest (Avril et al. 2010). However, equivocal results have been reported from studies involving healthy individuals wearing lower-body CG after fatiguing exercise (Menetrier et al. 2015; Sperlich et al. 2013). Menetrier et al. (2015) demonstrated improved femoral blood flow with compression stockings (thigh: 14 mmHg, calf: 27 mmHg, ankle: 15 mmHg) while Sperlich et al. (2013) reported decreased thigh blood flow with compression shorts (thigh: 35 mmHg). However, hemodynamic responses were not reported in either study. Furthermore, it has been suggested that calf compression is more important than compression of other leg regions for improving hemodynamic responses (Mosti and Partsch 2014). In contrast, the positive hemodynamic responses in the current study may be attributable to the wearing of a lower-body CG (thigh: 24.1 ± 2.4 mmHg, calf: 47.4 ± 8.8 mmHg) resulting in effective compression pressure, which narrows superficial leg vessels and dilates deep vessels (Lee et al. 2019), thus reducing blood pooling and potentially enhancing venous pumping function (Lim and Davies 2014; Mosti and Partsch 2014), resulting in improved venous return and enhancing hemodynamic responses. However, direct comparison of these results with previous studies may not be appropriate due to heterogeneity in study design, hemodynamic measurements and the compression pressure applied (Menetrier et al. 2015; Sperlich et al. 2013). Therefore, the effect of wearing different types of CG on recovery hemodynamic responses warrants investigation.
Improved lactic acid clearance while wearing CG, measured by monitoring [BLa−] during passive recovery, has been reported in well-trained cyclists (Driller and Halson 2013; Menetrier et al. 2013) and elderly cyclists (Chatard et al. 2004). In contrast, others have reported non-significant reductions in post-exercise [BLa−] in highly trained cyclists during passive recovery with CG after sprint cycling (Argus et al. 2013). The heterogeneity of study protocols may have led to these differences in [BLa−] results, with some studies involving submaximal cycling (Chatard et al. 2004; Driller and Halson 2013; Menetrier et al. 2013) while others involved multiple cycles of sprinting and recovery spinning (Argus et al. 2013). The recovery spinning may have obscured the recovery performance of the CG, as the claimed benefit of CG is the enhancement of limb blood flow and hemodynamic responses (MacRae et al. 2011). Furthermore, the effect of CG on [BLa−] clearance and submaximal exercise performance have been suggested to be trivial in trained individuals (Ali et al. 2010; Brown et al. 2017). That being the case, whether spinning (active recovery) and wearing CG have independent and/or additive effects on lactic acid clearance warrants further investigation. In addition, the participants in current study donned the CG within 3 min after the fatiguing preload cycling. Lower [BLa−] at the beginning of passive recovery was observed with CG than with CON (Table 4), which may be attributed to enhanced CO and SV when wearing CG. This finding aligns with the results of Menetrier et al. (2013) although a higher compression pressure was applied in our study. It has been suggested that wearing CG might increase lactic acid retention in the muscle bed as opposed to less lactate being produced or a greater clearance of lactate from the muscle (Berry and McMurray 1987). In our study, the [BLa−] levels after fatiguing preload cycling were similar for both trials, but significantly lower at 5 min and 15 min during the passive recovery in the CG trial was observed. Similar concentrations were recorded at the end of both trials during passive recovery. This suggests that lactic acid may potentially be removed more efficiently from the muscle when wearing CG during passive recovery. Therefore, the current results do not fully support the earlier findings of Berry and McMurray (1987). In contrast, Chatard et al. (2004) demonstrated that wearing CG significantly lowered [BLa−] throughout 80 min of passive recovery in elderly cyclists. This discrepancy may be due to an age-associated decline in hemodynamic responses (Stratton et al. 1994), i.e., lactic acid might take longer to clear in the elderly. Therefore, CG application for optimal recovery within different populations remains to be determined.
One of the main reasons for the observation of benefits in the present findings may be the well-controlled performance test with a high test–retest reproducibility (Chatard et al. 2004; Driller and Halson 2013; Menetrier et al. 2013), and appropriate timing of donning of the CG. The increased CO and SV may have facilitated lactic acid clearance from the bloodstream and subsequently enhanced BLa− oxidation, thereby improving subsequent endurance performance (MacRae et al. 2011). The current study found that 9 of the 13 (~ 70%) participants had higher mean power output after passive recovery with CG than with CON (Fig. 2). We showed that participants wearing CG had higher power output and cadence in subsequent endurance performance after passive recovery from fatiguing preload exercise (Table 3). In contrast, a recent meta-analysis suggested that wearing CG for recovery performance may have small yet significant and very likely benefits (Brown et al. 2017). The small effect sizes could be related to the inconsistency in study design and measured variables (Armstrong et al. 2015; Chatard et al. 2004; Driller and Halson 2013; de Glanville and Hamlin 2012; Menetrier et al. 2013). Furthermore, we applied a higher compression pressure than what might be required to improve hemodynamic responses in patients (Mosti and Partsch 2014). Moreover, the duration of CG application may affect endurance performance recovery (Brown et al. 2017). CG application for 15 to 80 min after exhaustive exercise appears to be more effective in enhancing lactic acid removal and improving subsequent endurance performance (Chatard et al. 2004; Driller and Halson 2013; Menetrier et al. 2013). Although subsequent endurance performance has been reported to improve with longer CG application (Armstrong et al. 2015; de Glanville and Hamlin 2012), other factors might obscure this effect, as the effects of nutrition, sleep quality and the recovery process have not previously been well documented (Armstrong et al. 2015; de Glanville and Hamlin 2012). Any potential interaction of CG, sleep quality and nutrition remain unclear, and further work is necessary to reveal the optimal duration of CG application for effective performance recovery.
The LMS was lowered throughout passive recovery with CG. LMS has been widely used to evaluate CG recovery performance (MacRae et al. 2011) and is associated with DOMS. While the exact mechanism of DOMS has not been confirmed, damage to muscle tissue and acute inflammatory response, specifically edema formation, have been postulated (Cheung et al. 2003; Hill et al. 2014b). Wearing CG has been shown to reduce edema in leg pain patients (Lim and Davies 2014) and in healthy individuals (Driller and Halson 2013). The exerted pressure from wearing CG may reduce the change in osmotic pressure and therefore reduce inflammation (Hill et al. 2014b), in turn relieving pain sensation. Although leg circumference was not measured directly in this study, the application of compression pressure has previously been demonstrated to reduce in vivo muscle circumference (Lee et al. 2019), which may have contributed to the positive LMS responses reported herein. The application of CG has been reported to alleviate perceived muscle soreness (Hill et al. 2014b), consistent with the findings of the current study. The relationship between the compression pressure of CG and its beneficial effects on perceived muscle soreness and limb circumference is a crucial indicator of performance recovery (Cheung et al. 2003; Hill et al. 2014b) and merits investigation.
Some limitations of our study may affect the generalization of our findings. A placebo effect may exist when conducting a performance study using CG. The beliefs of athletes in the efficacy of compressions garments may play a role in their performance (Brophy-Williams et al. 2017). We acknowledge that despite the challenging nature, no placebo was used in the current study. It must also be recognized that the clear differences in [BLa−] and hemodynamic responses between the two trials—which are not under the voluntary control of the participants—suggest that placebo effect may be unlikely and contributed to the improved performance. Furthermore, the 5-min PT was not included in the familiarization trials. Participants performed consistently throughout the fatiguing preload cycling and the post-PT lactate was well over 9 mmol, which demonstrated that the trials were well controlled and participants exerted their maximal effort (Edvardsen et al. 2014). Finally, because the participants were physically active men, the findings may not apply to other populations. Future studies should investigate the effect of CG on performance recovery in various populations.
Conclusions
Wearing sports compression garment (CG) has been suggested as an effective recovery strategy for athletes to endure frequent training, and may benefit subsequent exercise performance. Our study indicates that wearing sports CG after fatiguing exercise enhance passive recovery hemodynamics and subsequent cycling performance in physically active young men. The results of this study indicate that recovery CO, SV, HR, blood lactate clearance and LMS were improved with wearing sports CG after fatiguing cycling. Concomitantly, the subsequent cycling performance was improved. This suggests that wearing the sports CG could be useful for physically active individuals seeking to engage in multiple bouts of exercise in a single day.
Abbreviations
- BLa− :
-
Blood lactate
- CG:
-
Compression garment
- CO:
-
Cardiac output
- CON:
-
Gymnastic pants
- DOMS:
-
Delayed onset muscle soreness
- HR:
-
Heart rate
- LMS:
-
Leg muscle soreness
- MAP:
-
Mean arterial pressure
- PPO:
-
Peak power output
- PT:
-
Performance test
- RPE:
-
Ratings of perceived exertion
- SV:
-
Stroke volume
- SVR:
-
Systemic vascular resistance
- USCOM:
-
Doppler ultrasound
References
Ali A, Caine MP, Snow BG (2007) Graduated compression stockings: physiological and perceptual responses during and after exercise. J Sports Sci 25(4):413–419. https://doi.org/10.1080/02640410600718376
Ali A, Creasy RH, Edge JA (2010) Physiological effects of wearing graduated compression stockings during running. Eur J Appl Physiol 109(6):1017–1025. https://doi.org/10.1007/s00421-010-1447-1
Argus CK, Driller MW, Ebert TR, Martin DT, Halson SL (2013) The effects of 4 different recovery strategies on repeat sprint-cycling performance. Int J Sports Physiol Perform 8(5):542–548
Armstrong SA, Till ES, Maloney SR, Harris GA (2015) Compression socks and functional recovery following marathon running: a randomized controlled trial. J Strength Cond Res 29(2):528–533. https://doi.org/10.1519/JSC.0000000000000649
Avril S, Bouten L, Dubuis L, Drapier S, Pouget JF (2010) Mixed experimental and numerical approach for characterizing the biomechanical response of the human leg under elastic compression. J Biomech Eng 132(3):031006. https://doi.org/10.1115/1.4000967
Beliard S, Chauveau M, Moscatiello T, Cros F, Ecarnot F, Becker F (2015) Compression garments and exercise: no influence of pressure applied. J Sport Sci Med 14(1):75–83
Berry MJ, McMurray RG (1987) Effects of graduated compression stockings on blood lactate following an exhaustive bout of exercise. Am J Phys Med 66(3):121–132
Born DP, Sperlich B, Holmberg HC (2013) Bringing light into the dark: effects of compression clothing on performance and recovery. Int J Sports Physiol Perform 8(1):4–18. https://doi.org/10.1123/Ijspp.8.1.4
Brophy-Williams N, Driller MW, Kitic CM, Fell JW, Halson SL (2017) Effect of compression socks worn between repeated maximal running bouts. Int J Sports Physiol Perform 12:1–22
Brown F, Gissane C, Howatson G, van Someren K, Pedlar C, Hill J (2017) Compression garments and recovery from exercise: a meta-analysis. Sports Med 47(11):2245–2267. https://doi.org/10.1007/s40279-017-0728-9
Chan V, Duffield R, Watsford M (2016) The effects of compression garments on performance of prolonged manual-labour exercise and recovery. Appl Physiol Nutr Metab 41(2):125–132. https://doi.org/10.1139/apnm-2015-0335
Chatard JC, Atlaoui D, Farjanel J, Louisy F, Rastel D, Guezennec CY (2004) Elastic stockings, performance and leg pain recovery in 63-year-old sportsmen. Eur J Appl Physiol 93(3):347–352. https://doi.org/10.1007/s00421-004-1163-9
Cheung K, Hume P, Maxwell L (2003) Delayed onset muscle soreness: treatment strategies and performance factors. Sports Med 33(2):145–164. https://doi.org/10.2165/00007256-200333020-00005
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Academic Press, Hillsdale
de Glanville KM, Hamlin MJ (2012) Positive effect of lower body compression garments on subsequent 40-km cycling time trial performance. J Strength Cond Res 26(2):480–486. https://doi.org/10.1519/JSC.0b013e318225ff61
Dorey TW, O’Brien MW, Robinson SA, Kimmerly DS (2018) Knee-high compression socks minimize head-up tilt-induced cerebral and cardiovascular responses following dynamic exercise. Scand J Med Sci Sports 28(7):1766–1774. https://doi.org/10.1111/sms.13084
Driller MW, Halson SL (2013) The effects of lower-body compression garments on recovery between exercise bouts in highly-trained cyclists. J Sci Cycl 2(1):45–50
Edvardsen E, Hem E, Anderssen SA (2014) End criteria for reaching maximal oxygen uptake must be strict and adjusted to sex and age: a cross-sectional study. PLoS ONE 9(1):e85276
Engel FA, Holmberg HC, Sperlich B (2016) Is there evidence that runners can benefit from wearing compression clothing? Sports Med 46(12):1939–1952. https://doi.org/10.1007/s40279-016-0546-5
Goddard G, Karibe H, McNeill C (2004) Reproducibility of visual analog scale (VAS) pain scores to mechanical pressure. Cranio 22(3):250–256. https://doi.org/10.1179/crn.2004.030
Goto K, Mizuno S, Mori A (2017) Efficacy of wearing compression garments during post-exercise period after two repeated bouts of strenuous exercise: a randomized crossover design in healthy, active males. Sports Med-Open 3(1):25
Hill JA, Howatson G, van Someren K, Leeder J, Pedlar C (2014a) Compression garments and recovery from exercise-induced muscle damage: a meta-analysis. Br J Sports Med 48(18):1340–1346. https://doi.org/10.1136/bjsports-2013-092456
Hill JA, Howatson G, van Someren KA, Walshe I, Pedlar CR (2014b) Influence of compression garments on recovery after marathon running. J Strength Cond Res 28(8):2228–2235. https://doi.org/10.1519/JSC.0000000000000469
Hill JA, Howatson G, van Someren K, Gaze D, Legg H, Lineham J, Pedlar C (2017) The effects of compression-garment pressure on recovery after strenuous exercise. Int J Sports Physiol Perform 12(8):1078–1084. https://doi.org/10.1123/ijspp.2016-0380
Lee DCW, Lee SWY, Khaw K, Ali A, Sheridan SE, Wong SHS (2018) Haemodynamic responses of wearing low-pressure sports compression tights during an orthostatic challenge in healthy individuals. J Sci Med Sport 21(10):1062–1067. https://doi.org/10.1016/j.jsams.2017.12.004
Lee DCW, Law HKW, Ali A, Sheridan SE, Wong SHS, Lee SWY (2019) Compression garment-induced leg changes increase hemodynamic responses in healthy individuals. Int J Sports Med. https://doi.org/10.1055/a-0970-5399
Lee DCW, Ali A, Sheridan S, Chan DK, Wong SH (2020) Wearing compression garment enhances central hemodynamics? A systematic review and meta-analysis. J Strength Cond Res. https://doi.org/10.1519/JSC.0000000000003801
Lim CS, Davies AH (2014) Graduated compression stockings. CMAJ 186(10):E391-398. https://doi.org/10.1503/cmaj.131281
MacRae BA, Cotter JD, Laing RM (2011) Compression garments and exercise: garment considerations, physiology and performance. Sports Med 41(10):815–843. https://doi.org/10.2165/11591420-000000000-00000
MacRae BA, Laing RM, Niven BE, Cotter JD (2012) Pressure and coverage effects of sporting compression garments on cardiovascular function, thermoregulatory function, and exercise performance. Eur J Appl Physiol 112(5):1783–1795. https://doi.org/10.1007/s00421-011-2146-2
Marques-Jimenez D, Calleja-Gonzalez J, Arratibel I, Delextrat A, Terrados N (2016) Are compression garments effective for the recovery of exercise-induced muscle damage? A systematic review with meta-analysis. Physiol Behav 153:133–148. https://doi.org/10.1016/j.physbeh.2015.10.027
Menetrier A, Beliard S, Ravier G, Mourot L, Bouhaddi M, Regnard J, Tordi N (2013) Effects of recovery using contrast water therapy or compression stockings on subsequent 5-min cycling performance. J Sci Cycl 2(2):49
Menetrier A, Mourot L, Degano B, Bouhaddi M, Walther G, Regnard J, Tordi N (2015) Effects of three postexercice recovery treatments on femoral artery blood flow kinetics. J Sports Med Phys Fitness 55(4):258–266
Mosti G, Partsch H (2014) Improvement of venous pumping function by double progressive compression stockings: higher pressure over the calf is more important than a graduated pressure profile. Eur J Vasc Endovasc 47(5):545–549
Piras A, Gatta G (2017) Evaluation of the effectiveness of compression garments on autonomic nervous system recovery following exercise. J Strength Cond Res 31(6):1636–1643. https://doi.org/10.1519/JSC.0000000000001621
Smale BA, Northey JM, Smee DJ, Versey NG, Rattray B (2018) Compression garments and cerebral blood flow: influence on cognitive and exercise performance. Eur J Sport Sci 18(3):315–322
Sperlich B, Haegele M, Kruger M, Schiffer T, Holmberg HC, Mester J (2011) Cardio-respiratory and metabolic responses to different levels of compression during submaximal exercise. Phlebology 26(3):102–106. https://doi.org/10.1258/phleb.2010.010017
Sperlich B, Born DP, Kaskinoro K, Kalliokoski KK, Laaksonen MS (2013) Squeezing the muscle: compression clothing and muscle metabolism during recovery from high intensity exercise. PLoS ONE 8(4):e60923. https://doi.org/10.1371/journal.pone.0060923
Stickford AS, Chapman RF, Johnston JD, Stager JM (2015) Lower-leg compression, running mechanics, and economy in trained distance runners. Int J Sports Physiol Perform 10(1):76–83. https://doi.org/10.1123/ijspp.2014-0003
Stratton JR, Levy WC, Cerqueira MD, Schwartz RS, Abrass IB (1994) Cardiovascular responses to exercise. Effects of aging and exercise training in healthy men. Circulation 89(4):1648–1655. https://doi.org/10.1161/01.cir.89.4.1648
Zhang J, Critchley LAH, Lee DCW, Khaw KS, Lee SWY (2016) The effect of head up tilting on bioreactance cardiac output and stroke volume readings using suprasternal transcutaneous Doppler as a control in healthy young adults. J Clin Monit Comput 30(5):519–526. https://doi.org/10.1007/s10877-016-9835-7
Acknowledgements
The authors would like to thank Sure Step Asia Pacific Ltd. for providing the CG. We also thank Khaw K.S., Lee S.W.Y., Wong E.S.Y. and Mak M.H.Y., who assisted in data collection and equipment support, and all study participants. This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The results of the study are presented clearly, honestly, without fabrication, falsification, or inappropriate data manipulation. No conflicts of interest, financial or otherwise, are declared by the authors. The results of the current study do not constitute endorsement of the product by the authors or the journal.
Author information
Authors and Affiliations
Contributions
DL, SS, AA, and SW conceived and designed research. DL performed experiments. DL and AA analyzed data. DL, SS, and AA interpreted results of experiments. DL and DS prepared figures. DL drafted manuscript. DL, SS, and AA edited and revised manuscript. DL, AA, and SW approved final version of manuscript.
Corresponding author
Ethics declarations
Conflict of interest
No potential conflict of interest was reported by the authors.
Ethical approval
The study was approved by the University Ethics Committee (CREC Ref. No.: 2016.584-T) in accordance with the latest version of the Declaration of Helsinki.
Informed consent
All participants gave written informed consent and were not made aware of the study hypothesis.
Consent for publication
All co-authors were aware of the publication of this study.
Additional information
Communicated by George Havenith.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lee, D.C.W., Sheridan, S., Ali, A. et al. Wearing compression tights post-exercise enhances recovery hemodynamics and subsequent cycling performance. Eur J Appl Physiol 121, 2091–2100 (2021). https://doi.org/10.1007/s00421-021-04661-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-021-04661-0