
Abstract
Background
The custom-made, flexible artificial iris developed by HumanOptics and Koch can reconstruct the anterior segment of patients with aniridia. The aim of this study was to evaluate the long-term clinical outcome and complication spectrum after artificial iris implantation and the role of the embedded fiber mesh in view of specific complications.
Methods
In this retrospective interventional case series, patients received an artificial iris between 2004 and 2013. Only eyes with a minimum follow-up period of 2 years were included. Indications were congenital, traumatic, or iatrogenic aniridia. The artificial iris was used either with or without embedded fiber mesh for partial or full prostheses.
Results
We included 34 patients (mean age 48.8 years; SD ±17.2) with a mean follow-up of 50.0 months (SD ±18.9 months). No repositioning of prostheses was necessary. In cases of keratopathy (17.6 %) visual function increased from baseline mean 1.6 logMAR (SD ±0.7) to 1.2 logMAR (SD ±0.7) after artificial iris implantation. The remaining iris tissue darkened during the follow-up in 23.5 % (83.3 % with and 10.7 % without mesh), 8.8 % developed glaucoma (50 % with and 0 % without mesh) and 14.7 % needed consecutive surgery after prostheses implantation (50 % with and 7.1 % without mesh). In three out of seven trauma cases (42.9 %) silicone oil was spilled into the anterior chamber after 2.5 years on average.
Conclusion
The artificial iris prosthesis revealed a good clinical outcome in terms of long-term stability, cosmetic appearance, visual function, and represents a good functional iris diaphragm for compartmentalisation. Complications such as glaucoma, darkening of iris tissue, and need for consecutive anterior segment surgery are clearly associated with implants with integrated fiber mesh, but not to those without. Hence, the use of full iris prostheses without embedded fiber mesh, even in cases with remnant iris, and the use of slightly smaller implants than officially recommended may be beneficial.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pupil or iris defects may cause decreased visual acuity (VA), increased glare, reduction in contrast sensitivity, and loss in depth of focus. Most cases of aniridia occur after severe ocular trauma, less common causes are congenital, ICE-syndrome, or an iatrogenic iris defect. While small defects can be repaired with specific suture techniques [1], more complex cases require an iris prosthesis [2, 3]. Due to limited flexibility of the iris tissue, better iris implants have evolved over the last decade with soft and foldable material for easy and minimal invasive implantation and with enough structural stability for suturing [4].
The flexible and foldable artificial iris was developed by HumanOptics and Koch [5]. It has a diameter of 12.8 mm and a decreasing thickness from pupil margin (0.4 mm) towards periphery (0.25 mm). It can be easily cut with scissors or with a trephine and then inserted through small incisions into the ciliary sulcus of pseudophakic or aphakic eyes [6]. The iris prosthesis is custom-made to match the color of the patient’s natural iris. The multi-layered implant consists of a core matrix made of silicon with incorporated color pigment, coated with another layer of medical-grade silicone. The color pigment is not applied on the surface but embedded within the material, creating a three-dimensional impression. This way the natural iris with its topographic surface is simulated optimally resulting in an improved aesthetic appearance [7–9].
The artificial iris is available in two variants, with or without embedded fiber mesh. The model without fiber mesh is more flexible, can be folded easily and adapts very well to the anatomical structure of the sulcus. However, the soft material is only fairly suited for suture fixation because tension of the sutures can easily damage the material. Therefore, implants without an embedded fiber mesh are preferred for full prostheses implantation [10]. Implants with an additional fiber mesh are more rigid and provide a better tensile strength for sutures. Hence, it is rather used for partial implant surgery when side-to-side anastomosis is required in addition to transscleral suture fixation [10]. However, the use of implants with integrated fiber mesh has been suspected to provoke specific complications due to exposing sharp endings if trephined or cut in size [10].
To reconstruct partial or full aniridia, the artificial iris is an improved technique for satisfactory cosmetic and visual outcomes [7–9]. However, the long-term biocompatibility of an artificial iris has not been investigated in a large cohort yet. The aim of this study was to evaluate the long-term clinical outcome and complication spectrum of eyes with artificial iris implantation and the role of the embedded fiber mesh in view of specific complications, thereby identifying risk factors to minimize long-term complications.
Methods
In this retrospective interventional case series, we analysed the long-term outcome of patients who consecutively received an artificial iris with or without integrated fiber mesh between 2004 and 2013. Only those eyes with a minimum follow-up period of 2 years were included. Indications for artificial iris implantation were congenital, traumatic or iatrogenic aniridia (e.g., after complicated phacoemulsification).
The manufacturer recommends a diameter of iris prosthesis that corresponds to the horizontal white-to-white (WTW) distance plus 0.5 mm. But previously, we have recommended rather to use a smaller size to decrease the risk of glaucoma. We suggest a diameter equivalent to the vertical WTW distance, from which 0.5 – 1.0 mm should be subtracted in most cases. In more practical terms, a diameter of 11 mm after trephination is suitable for most eyes, occasionally 10 mm in smaller eyes. A detailed description of the surgical implantation procedure was published earlier by Szurman et al. [10] (Fig. 1). Briefly, a superior corneoscleral tunnel incision of 4-5 mm was made and a transscleral suture fixation “ab interno” was performed [11]. The base of the iris prosthesis was fixed at both edges to an anchor through the loop stitch without any knot. The prosthesis was then inserted through the scleral tunnel incision with a forceps [14], positioned into the sulcus and kept in place by stretching the transscleral sutures in opposite directions. The side-to-side anastomosis for partial prosthesis was performed as previously described by Engels [12]. The final transscleral fixation of the implant was performed using the Z-suture technique [13] or a scleral flap.

Surgical technique of implantation of partial prosthesis. For this purpose, an iris implant with fiber meshwork is more suitable. Preparation of the artificial iris with a trephine (a) and scissors (b). Be aware, when cutting the model with a fiber meshwork, some sharp-edged polymer fibers can get pulled out and exposed. Therefore, we advise to size it slightly smaller than originally planned. The base of the iris prosthesis is fixed at both edges to an anchor through the loop stitch without any knot (c). Implant segments larger than 5 clock hours need three points of fixation. The transscleral suture fixation is performed using an “ab interno” technique [11] (d). The prosthesis is then inserted through the scleral tunnel incision with a forceps (e), positioned into the sulcus (f). Note that half-implants do not exceed 5 mm so that they do not need to be folded. Since half-prostheses are less flexible, the prosthesis diameter should be sized so that it prevents chronic pressure in the sulcus area as well as damage of the surrounding uveal tissue. For partial prostheses larger than 4 clock hours, the diameter should correspond to the vertical white-to-white (WTW) distance shortened by 0.5-1 mm. For smaller prostheses, the vertical WTW distance is appropriate. The side-to-side anastomosis is performed as previously described by Engels [12] (g). It might be helpful to press against the opposite side of the prosthesis with a push-pull hook to facilitate the puncture. After watertight closure of the scleral tunnel incision, the final transscleral fixation of the implant is performed using the Z-suture technique [13]. This may help reduce complications such as scleral necrosis, suture erosion, and infections
The implantation of mesh-free prostheses is relatively easy due to the flexibility and foldability of the material. A corneoscleral tunnel incision of 3.5 – 4.0 mm is usually sufficient to insert the implant. In principle, the use of an injector is possible, but only if there is no need for additional suture fixations like in the case of traumatic mydriasis where enough iris root is available. Be aware, that with an injector, uncontrolled unfolding can occur and the endothelium may get damaged. Therefore, an implantation with forceps with a slightly larger incision size should be preferred in most cases. The transscleral suture fixation of the implant is performed at three locations maximum: 4, 8, and 12 o’clock and follows the same “ab interno” technique and Z-suture technique as described in the above section for “partial prostheses”. During insertion into the sulcus, the transscleral sutures are tightened carefully as they can tear easily with full prosthesis.
Some aphakic eyes required permanent or long-standing silicone oil tamponade to maintain retina re-attachment or to prevent phthisis. Practically, full prosthesis without fiber mesh was used and a semicircular inferior ando-iridectomy was created with a 4 mm trephine. In eyes with silicone oil, a larger implant diameter can be used to tightening the sulcus.
To analyse differences in VA and intraocular pressure (IOP) before and after implantation, data were analysed using ANOVA variance analysis. Bonferroni corrected p-values of p ≤ 0.05 were considered statistically significant.
Results
We included 34 eyes of 34 patients with a mean age of 48.8 years (SD ±17.2, range 28 - 85 years). Twenty-two (64.7 %) were male and 11 (35.3 %) were female. The mean follow-up time was 50.0 months (SD ±18.9 months, range 12-84 months). Reasons for prosthesis implantation were congenital aniridia in six eyes (17.6 %), congenital coloboma in one eye (2.9 %), traumatic iris defect in 23 eyes (67.6 %), and iatrogenic iris defect after complicated phacoemulsification in four eyes (11.7 %). Before artificial iris implantation, 14 eyes were pseudophakic (41.2 %), 15 were aphakic (44.1 %), and five were phakic (14.7 %). The mean number of ocular interventions prior artificial iris surgery was 1.9 (SD ±1.5; range 0-6). At baseline, 5 eyes were hypotonic (14.7 %), 10 eyes had glaucoma (29.4 %), 6 eyes had pre-existing keratopathy (17.6 %), and in four eyes there was silicone oil in the anterior chamber (11.8 %). The iris defect before surgery showed a complete aniridia in 17 eyes (50 %), a partial aniridia in eight eyes (23.5 %), a circular remnant iris in six eyes (17.6 %), a coloboma in one eye (2.9 %), and a half-moon shaped defect in two eyes (5.9 %). Those eight eyes with partial aniridia had a mean iris defect of 5.8 hours (SD ±2.5; range 3-10 hours). All artificial iris implantations were performed by the same surgeon. Twenty-eight eyes received a full artificial iris prosthesis without mesh (82.4 %, Fig. 2) and six eyes a partial prosthesis with mesh (17.6 %, Fig. 3). The mean size of the artificial iris was 11.2 mm (SD ±0,5 mm; range 10-12 mm). The mean size of incision was 3.9 mm (SD ±0.7 mm; range 3.5-6.5 mm). The final transscleral fixation of the implant was performed using the Z-suture technique in 26 cases (76.5 %) and with a scleral flap in eight eyes (23.5 %). There was no case of suture failure during the follow-up. In addition, for artificial iris implantation, vitrectomy was performed in eight cases (23.5 %), one eye received a cerclage (2.9 %) and four eyes a corneal graft (11.8 %).

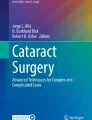
Fellow eye (a) for colour comparison. Full iris prosthesis before (b) and 20 months after surgery (c)

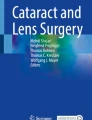
Fellow eye (a) for colour comparison. Partial iris prosthesis before (b) and 17 months after surgery (c)
Clinical success
In none of the 34 cases repositioning of the artificial iris was necessary.
In eight of 17 eyes with remnant iris (47.1 %), all of them were trauma cases, the remaining iris tissue darkened during the follow-up (Fig. 4). Interestingly, darkening of the remnant iris appeared in 83.3 % of eyes with an implant with mesh (five of six eyes) and only in 10.7 % of eyes with an implant without mesh (three of 28 eyes) (Table 1).

Exemplary photograph of a large partial iris prosthesis with exposed mesh fibers. Note darkening of the remaining iris tissue within 12 months
Eleven eyes (32.4 %) developed complications such as glaucoma (three eyes, 8.8 %), keratopathy (two eyes, 5.9 %), silicone oil in the anterior chamber (three eyes, 8.8 %), haemorrhage of the remnant iris (one eye, 2.9 %), and retinal detachment (two eyes, 2.9 %). Only five eyes (14.7 %), again all of them trauma cases, needed a consecutive surgery: one penetrating keratoplasty (progressive keratopathy), one Ahmed Valve implant (progressive glaucoma), two vitrectomies (retinal detachment with proliferative vitreoretinopathy (PVR)), and one anterior chamber lavage (recurrent haemorrhage of the remnant iris). Presumably, the iris haemorrhage was caused by pulled-out sharp-edged polymer fibers of the artificial iris mesh (Fig. 5). Interestingly, the other two anterior segment surgeries (penetrating keratoplasty and Ahmed Valve implantation) also occurred in eyes with an artificial iris with mesh. Therefore, eyes with artificial iris with mesh showed a high rate of consecutive surgeries of 50 % (three of six eyes, all anterior segment surgeries). In contrast, the rate of consecutive surgeries in eyes with an artificial iris without mesh was much lower with 7.1 % (two of 28 eyes, all vitrectomies due to retinal detachment with PVR) (Table 1). All 34 patients had an attached retina at the last follow-up visit. Two of them had a mild but stable PVR-reaction (5.9 %).

Detail view of a partial iris prosthesis with mesh. Indicated are sharp-edged polymer fibers that are pulled out (arrow head)
Visual acuity
Prior artificial iris implantation, mean VA of all 34 eyes was 1.0 logMAR (SD ±0.6. Compared to baseline, mean VA increased in all subgroups (traumatic, congenital, and iatrogenic iris defects) at the final follow-up (Fig. 6, p = 0.56). At the final examination, 16 eyes (47.1 %) gained two or more VA lines, 15 eyes (44.1 %) remained stable, and three eyes (8.8 %) lost two or more VA lines. Moreover, in the 6 eyes with pre-existing keratopathy before artificial iris implantation (17.6%) VA increased from a mean baseline of 1.6 logMAR (SD ±0.7) to a mean of 1.2 logMAR (SD ±0.7) at the last follow-up examination (p=0.4). At the final examination, two eyes (33.3 %) gained two or more VA lines and four eyes (66.7 %) remained stable. No eye lost two or more VA lines. In seven patients with silicone oil tamponade, prior artificial iris surgery VA was stabilized in six eyes (85.7 %) from 1.84 logMAR (SD ±0.5) at baseline to 1.86 logMAR (SD ±0.5) at the last follow-up, just one eye (14.3 %) lost two VA lines.

Box plot visualizes course of the visual acuity (logMAR) in patients with traumatic, congenital, and iatrogenic iris defect (ID) at baseline and at the final follow-up. ANOVA Bonferroni, p = 0.56
Intraocular pressure (IOP)
Mean IOP before artificial iris surgery was 14.6 mmHg (SD ±5.6 mmHg). At the final follow-up examination, mean IOP showed no significant difference compared to baseline (mean 14.7 mmHg, SD ±16.7 mmHg, p = 0.06, Fig. 7). There was no statistically significant difference between the subgroups traumatic, congenital, and iatrogenic iris defects, neither at baseline, nor at the final follow-up (p = 0.07). However, all three eyes, which developed glaucoma (8.8 %), received an artificial iris with mesh. In contrast, none of the eyes with implantation of an artificial iris without mesh developed glaucoma (Table 1). Hypotony was existent in five eyes before artificial iris implantation (mean IOP 3.8 mmHg, SD ±2.9 mmHg). All of them were eyes with a traumatic iris defects and a silicone oil tamponade (both was pre-existent in seven eyes in total). In all five eyes hypotony persisted at the final follow-up examination (3.2 mmHg, SD ±2.2 mmHg).

Box plot visualizes course of the intraocular pressure (mmHg) in patients with traumatic, congenital, and iatrogenic iris defect (ID) at baseline and at the final follow-up. . ANOVA Bonferroni, p = 0.07
Artificial iris diaphragm
Out of all 34 patients reviewed, seven of 23 eyes with traumatic aniridia (30.4 %) required a permanent silicone oil tamponade. All seven eyes received a full prosthesis without mesh and with ando-iridectomy in combination with a pars plana vitrectomy and change of the silicone oil. Prior to artificial iris implantation, all these eyes were aphakic. Two of them additionally received a sclera fixated intraocular lens together with the artificial iris implantation. The mean number of ocular interventions before artificial iris surgery in those seven eyes was a mean of 4.4. Four of seven eyes had silicone oil in the anterior chamber before prosthesis implantation. In three eyes, all were hypotonic, silicone oil returned into the anterior chamber after 2.5 years on average.
Discussion
The development of foldable, custom-tailored iris prostheses has been a significant advance for anterior segment iris reconstruction in patients with partial or full aniridia [15]. The artificial iris set a new standard with improved cosmetic results and improvements in VA, contrast sensitivity, depth of focus, and decreased glare from lights [16, 17].
This retrospective case series presents a large data collection with a long-term follow-up after full or partial artificial iris implantation of 34 patients with traumatic, congenital, or iatrogenic iris defects. The study evaluated the clinical outcome and complication spectrum of eyes with artificial iris implantation with and without fiber mesh identifying risk factors to subsequently minimize long-term complications.
Concerning VA, we could show a gain in 47 % and a stabilisation in 44 % after artificial iris implantation. A severe complication after artificial iris implantation is glaucoma [6]. In this study, 9 % developed glaucoma after implantation. All received an artificial iris with mesh. No patient of the group with an artificial iris without mesh developed glaucoma. We could demonstrate that trephination and cutting of the artificial iris expose the sharp-edged polymer fiber ends in artificial iris implants with mesh. It might be speculated that this could lead to chronic irritation of the surrounding tissues causing glaucoma. This is supported by the fact that implants with exposed mesh fibers provoke hyperpigmentation of iris remnants as a sign of chronic tissue irritation. Therefore, in order to avoid potential complications with partial prostheses, we recommend to use full prosthesis without mesh and to size it slightly smaller than originally planned. These implants exerted significantly less complications. According to our experience, a diameter of 11 mm after trephination is suitable for most eyes. This might be the reason why we did not see a significant increase of IOP after artificial iris implantation compared to previous studies [6]. Mayer et al. also recommend a smaller diameter and achieved a low complication rate with glaucoma [16].
Consecutive surgery was necessary in 15 %, all trauma cases. Predominantly artificial iris with mesh showed a higher rate of consecutive surgery (50 %) than artificial iris without mesh 7 %. Strikingly, consecutive surgeries of the artificial iris with mesh were performed at the anterior segment because of glaucoma, keratopathy, and iris haemorrhage. This might be in coherence with the rigid mesh-material or exposed sharp-edged polymer fibers. However all eyes needing consecutive surgery were trauma cases being often associated with numerous other ocular pathologies. Therefore, the retinal detachment with PVR seen in two eyes with an artificial iris without mesh might be associated with the preexisting trauma and not with the implant.
Besides aniridia, common associated pathologies after trauma may require treatment with silicone oil tamponade. For the trauma eyes, 30 % required permanent or long-standing silicone oil tamponade to sustain retina attachment. These eyes require an intact iris-lens-diaphragm to prevent the passage of silicone oil into the anterior chamber. Our study shows that in about 60 % of these eyes silicone oil could be kept behind the artificial iris even in the long-term. All eyes with silicone oil spilled into the anterior chamber were hypotonic. In general the artificial iris represents a good functional iris diaphragm for compartmentalisation in the presence of silicone oil tamponade [18], although less effective in hypotonic eyes.
Furthermore, we could demonstrate for the first time an over-pigmentation of the remaining iris tissue in 47 % of the eyes during the follow-up. Interestingly, in the majority of cases (83 %) the remnant iris darkened in eyes with an artificial iris with mesh, compared to only 11 % in eyes with an implant without mesh. All eyes were trauma cases, therefore artificial iris with mesh and trauma might be a risk factor for darkening of the remnant iris. We could show that cutted prostheses with mesh can have sharp-edged polymer fibers possibly leading to chronic irritation of the surrounding tissues with subsequent over-pigmentation of the remaining iris tissue. Therefore, we recommend using a full artificial iris prosthesis without mesh also in eyes with remaining iris to avoid darkening of the remnant iris and accordingly improve the cosmetic outcome. This is consistent with long-term results of Mayer et al. who recommended using full prosthesis with a smaller diameter [16].
Summarized, our long-term results suggest that artificial iris implantation represents an advance for anterior segment iris reconstruction in patients with partial or full aniridia, even in complex cases. The artificial iris implant revealed a good clinical outcome in terms of long-term stability, cosmetic appearance, and visual function. Furthermore, it represents a good functional iris diaphragm for compartmentalisation with satisfactory aesthetic results. However, limitations of the study are a wide range of aniridia causes and variation in disease and management. Therefore, direct correlation of the success rate and the surgical technique might be critical.
However, our study shows that long-term complications such as glaucoma, over-pigmentation of the remaining iris tissue, and need for a secondary surgery are significantly associated with implants with integrated fiber mesh, but not to implants without mesh. This might be due to the fact that exposed sharp-edged fibers exert a chronic tissue inflammation with specific complications.
Therefore, we recommend using full iris prosthesis without embedded fiber mesh even in cases with remnant iris. In addition we recommend sizing the artificial iris slightly smaller than originally planned to avoid exerting chronic pressure to the trabecular meshwork.
References
Brauweiler P (2011) Iris sutures. Ophthalmologe 108(8):710–713
Mavrikakis I, Mavrikakis E, Syam PP, Bell J, Casey JH, Casswell AG, Brittain GP, Liu C (2005) Surgical management of iris defects with prosthetic iris devices. Eye 19:205–209
Srinivasan S, Ting DS, Snyder ME, Prasad S, Koch HR (2014) Prosthetic iris devises. Can J Ophthalmol 49(1):6–17
Wolff J (2011) Prosthetic iris devices. Ophthalmologe 108(8):714–719
Koch HR (2008) A new foldable artificial iris Indications, surgical techniques and first results. Clin Exp Ophthalmol 36(s1):A1–A61
Jonsson NJ, Sahlmüller MC, Ruokonen PC, Torun N, Rieck P (2011) Complications after cosmetic iris implantation. Ophthalmologe 108:455–458
Forlini C, Forlini M, Cavallini GM (2013) Simultaneous correction of post-traumatic aphakia and aniridia with the use of artificial iris and IOL implantation. Graefes Arch Clin Exp Ophthalmol 251(10):2493–2494
Burk SE, Da Mata AP, Snyder ME, Cionni RJ, Cohen JS, Osher RH (2001) Prosthetic iris implantation for congenital, traumatic, or functional iris deficiencies. J Cataract Refract Surg 27:1732–1740
Thomas BC, Rabsilber TM, Auffarth GU (2013) Aniridia-IOL and artificial iris reconstruction. Klin Monatsbl Augenheilkd 230(8):786–790
Szurman P, Jaissle G (2011) Artificial iris. Ophthalmologe 108:720–727
Smiddy WE, Sawusch MR, O’Brian TP, Scott DR, Huang SS (1990) Implantation of scleral-fixated posterior chamber intraocular lenses. J Cataract Refract Surg 16:691–696
Engels T (1998) Irisnähte in der geschlossenen Vorderkammer. Ophthalmol Chirurgie 10:21–28
Szurman P, Petermeier K, Aisenbrey S, Spitzer MS, Jaissle G (2010) Z-suture - a new knotless technique for transscleral suture fixation of intraocular implants. Br J Ophthalmol 94:167–169
Szurman P, Petermeier K, Grisanti S, Jaissle GB, Bartz-Schmidt KU (2007) A new small-incision technique for injector implantation of transsclerally sutured foldable lenses. Ophthalmic Surg Lasers Imaging 38:76–80
Koch KR, Heindl LM, Cursiefen C, Koch HR (2014) Artificial iris devices: benefits, limitations, and management of complications. J Cataract Refract Surg 40(3):376–382
Mayer CS, Hoffmann AE (2015) Surgical treatment with an artificial iris. Ophthalmologe 112(10):865–868
Spitzer MS, Nessmann A, Wagner J, Yoeruek E, Bartz-Schmitz KU, Szurman P, Szurman G (2016) Customized humanoptics silicone iris prosthesis in eyes with posttraumatic iris loss: outcomes and complications. Acta Ophthalmol (Copenh). doi:10.1111/aos12946
Hermann MM, Muether PS, Kuhn L, Kirchhof B, Fauser S (2012) Clinical outcome of the artificial iris diaphragm in silicone oil surgery. Br J Ophthalmol 96(7):1008–1011
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Informed consent
For this type of study formal consent is not required.
Funding
No funding was received for this research.
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Rights and permissions
About this article

Cite this article
Rickmann, A., Szurman, P., Januschowski, K. et al. Long-term results after artificial iris implantation in patients with aniridia. Graefes Arch Clin Exp Ophthalmol 254, 1419–1424 (2016). https://doi.org/10.1007/s00417-016-3292-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-016-3292-3