
Abstract
Current management guidelines for refractory status epilepticus (RSE) recommend the use of intravenous continuous anesthetic therapy, but there is little evidence to guide the selection of the most efficacious and safest drug. We conducted a retrospective study to evaluate the efficacy and safety of midazolam versus thiopental for treatment of RSE. Retrospective case–control series of prospectively identified patients treated with midazolam or thiopental for RSE between January 2007 and December 2014. The primary outcome was control of RSE. Secondary outcomes included the rate of adverse events, intensive care unit (ICU) and hospital length of stay, hospital mortality and long-term neurological outcome, assessed with the extended Glasgow outcome scale (GOS-E) at discharge and at six 6 months. A total of 33 patients were included, 19 treated with midazolam and 14 with thiopental. Groups were similar for demographic data, clinical variables, comorbidity and the underlying cause of RSE. The rate of control of SE did not differ between groups (63 vs. 64 %). Adverse events including hypotension (mean arterial pressure <70 mmHg) requiring vasopressors, infections, anemia requiring red blood cells transfusion, leucopenia (<4000/mm3), and hyponatremia (<130 mEq/l) were more frequent during thiopental infusion. Furthermore, patients treated with midazolam had a shorter median ICU length of stay (6 vs. 15 days; p = 0.02) and better GOS-E at 6 months (8 [8] vs. 4 [4, 5]; p = 0.01). These findings suggest that continuous midazolam administration is as efficacious as thiopental infusion for the treatment of RSE; however, midazolam was associated with a significantly lower number of adverse events. These findings should be confirmed in larger multicenter trials.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Refractory status epilepticus (RSE) is defined as status epilepticus (SE) resistant to a first-line of short-acting well dosed benzodiazepine and a second-line of antiepileptic drug [1, 2]. This condition is associated with a high morbidity and mortality [3–5]. High-level evidence is lacking for therapeutic management of RSE. In case of refractory generalized convulsive status epilepticus (GCSE), current guidelines recommend the administration of a continuous infusion of an anesthetic drug. In case of non-convulsive status epilepticus (NCSE), the same guidelines suggest to withhold pharmacological coma until several trials of conventional anti-seizure medications have failed, although many patients with NCSE will eventually require anesthetics [1]. Available agents for continuous infusion include midazolam, propofol and barbiturates (pentobarbital or thiopental). A systematic review of cases published up to 2002 [6] found that patients receiving pentobarbital had a lower rate of therapeutic failure or recurrence of seizures than patients receiving midazolam. However, these results were biased because continuous electroencephalogram (cEEG) was used less frequently in the pentobarbital group and the rate of non-convulsive seizures (NCSz), which represent the most common form of seizures among critically ill patients [7], was likely underestimated in that group. Another important limitation is that the doses of midazolam were usually below 0.4 mg/kg/h, while a recent study indicates that higher doses are sometimes required to control RSE [8]. More recently, a randomized controlled trial attempted to compare propofol and barbiturates in RSE patients but was interrupted because of the low enrollment rate [5]. Although the groups were too small to show any difference between the two drugs on seizure control, patients treated with barbiturates required a longer duration of mechanical ventilation. This result was secondary to the very long half-life of barbiturates compared to propofol and midazolam, which are much shorter-acting agents. Another concern with barbiturates is their potent cardiovascular depressant effect, leading more frequently to hypotension and the need for vasopressors than other drugs [6]. Finally, propofol may be associated with a risk of cardiovascular complications (e.g., the so-called “propofol infusion syndrome”), at least when given at high doses for several days [9–11], and, compared to midazolam, a higher rate of complications and mortality [11].
For all these reasons, midazolam is becoming the drug of choice as first-line anesthetic for RSE, as indicated in a recent survey of experts [12]. In our institution, thiopental was considered the first-line anesthetic for RSE until 2010, as intensivists were familiar with its use in the management of intracranial hypertension. From 2011 onwards, intensivists and neurologists jointly decided to shift to midazolam, in particular for its safer profile.
The aim of this retrospective case–control study was to compare the efficacy and safety of midazolam and thiopental as first-line anesthetic for the treatment of RSE, using patients treated with thiopental as a historical control group.
Methods
Patient identification and inclusion criteria
In our institution, we maintain a prospective database of patients undergoing continuous EEG monitoring (CEEG). Patients were included in this study (January 2007 to December 2014) if: (1) RSE was identified, according to standard definitions [1]; (2) patients received at least one anesthetic drug (midazolam, propofol or thiopental). Exclusion criteria were: post-anoxic brain injury; treatment with propofol alone. The study was approved by the Ethics Committee of Hôpital Erasme, which waived the need for an informed consent.
Standard management of patients with RSE
While some variability is inevitable given the retrospective observational nature of this study, the following steps define our protocol for the treatment of SE. Intravenous lorazepam (0.1 mg/kg) is administered as first-line non-anesthetic agent in all patients, followed by intravenous (IV) administration of phenytoin (20 mg/kg), valproate (20–40 mg/kg) or levetiracetam (20–40 mg/kg). In case of refractory GCSE, a continuous IV infusion of anesthetics is immediately started, while in case of refractory NCSE, at least one other attempt of non-anesthetic anti-seizure medication is made. If a continuous infusion of anesthetics is decided, thiopental is given as a bolus of 1 mg/kg followed by continuous infusion at an initial rate of 1 mg/kg/h. Midazolam is initiated as a bolus of 0.2 mg/kg followed by continuous infusion at an initial rate of 0.1 mg/kg/h. If needed, boluses are sequentially re-administered and the infusion rate is progressively increased until seizure control is achieved or the maximal tolerated dose is reached. Breakthrough seizures are treated by new boluses and increases in the infusion rate until SE is controlled or the maximal tolerated dose is reached. Once SE is controlled for at least 24 h (defined as cessation of both clinical and electrographic SE), the anesthetic is progressively weaned over a 24–48 h period. Short infrequent seizures are tolerated during the weaning process but seizures of increasing frequency or duration are considered to represent impeding SE relapse and treated with re-administration of a continuous anesthetic infusion. The decision to reinstate sedation would be decided not only on the basis of seizure frequency and duration, but will also depend on seizure type, the underlying etiology and each patient’s individual status. Since 2006, all patients with RSE at our institution are monitored with CEEG. Monitoring is requested if a patient does not regain consciousness soon after convulsions are controlled or if nonconvulsive seizures are suspected in a stuporous or comatose patient. Patients are monitored during the entire duration of the anesthetic treatment and up to at least 24 h after the last seizure is observed after the weaning process.
Clinical and EEG variables
We recorded demographics and location at time of diagnosis of SE. The severity of SE was assessed with the Status epilepticus severity score (STESS) [13], which includes age, level of consciousness (categorized as stuporous/comatose or better), history of epilepsy and type of SE (generalized convulsive, non-convulsive in coma, complex partial, simple partial or absence). Co-morbidities on admission were quantified with the Charlson co-morbidity index (CCI) [14]. Severity of non-neurological critical illness at the time of diagnosis of SE was measured with the Sequential Organ Failure Assessment (SOFA) score minus its neurological component [15]. The etiology of SE was categorized as acute, remote, progressive or unknown as proposed by the International League Against Epilepsy (ILAE) [16].
Variables related to anesthetic treatment included time from diagnosis of SE to initiation of treatment, the number and type of non-anesthetic treatment attempts prior to anesthetics, the duration of treatment and the maximal infusion rate.
New complications arising after the onset of anesthesia were recorded and defined as follows: hypotension (defined as mean arterial pressure <70 mmHg requiring new administration of or increase in the dose of vasopressors), myocardial infarction (elevation of troponin levels >40 ng/l and/or ST segment elevation on ECG), cardiac arrhythmia (atrial flutter, atrial fibrillation, ventricular tachycardia, and second or third degree auriculo-ventricular block), thromboembolic complications (including deep vein thrombosis demonstrated by lower extremities ultrasound and pulmonary embolism demonstrated by lung CT-angiography), acute respiratory distress syndrome (ARDS, according to the Berlin criteria) [17], ileus (defined as absence of bowel movements in the absence of evidence of mechanical obstruction), intestinal ischemia (confirmed by surgical exploration), gastrointestinal bleeding (both overt and covert demonstrated by occult bleeding test), acute liver failure (elevation of transaminases >3 times the upper limit of the normal values and an international normalized ratio >1.5), pancreatitis (elevation of lipase >3 times the upper limit of the normal values), acute kidney injury (need for renal replacement therapy), bacteremia (positive blood cultures), ventilator-associated pneumonia [18], urinary tract infection (positive urine culture with presence of leukocytes), central line-associated bloodstream infection [18], Clostridium difficile infection (positive feces culture or toxin), anemia (hemoglobin levels <8 g/dl) requiring blood transfusion, thrombocytopenia (platelet count <150,000/mm3), leukopenia (<4000 cells/mm3), neutropenia (<1000 cells/mm3), lymphopenia (<1500 cells/mm3), hyponatremia (<130 mEq/l) and hypernatremia (>150 mEq/l).
Outcome assessment
The primary outcome measure was control of SE with no need for re-administration of anesthetic drugs after weaning during the same hospital stay. Failure to immediately control SE by the maximal tolerated dose of the chosen anesthetic (“acute failure”), the occurrence of breakthrough seizures that did not respond to the maximal tolerated dose of the chosen anesthetic and the occurrence of withdrawal seizures during or after weaning were considered as the three possible causes of treatment failure. One author (NG), blinded to treatment, re-reviewed all the EEG recordings from the beginning of the anesthesia until the trial of a new round of anesthetics was prescribed or until the end of monitoring to confirm acute failure, breakthrough seizures or withdrawal seizures, and to record occurrence of suppression-burst and complete suppression during treatment.
Secondary outcome measures included ultimate control of SE, length of ICU and hospital stay, hospital mortality and functional outcome at hospital discharge and at 6 months after discharge, when available. Functional outcome was assessed with the extended Glasgow outcome scale (GOS-E), inferred from the clinical examination at discharge and during follow-up visits. Good outcome was defined as a GOS-E score ≥6 (independent at home, able to return to work even with special arrangement).
Statistical analysis
Comparisons of categorical and ordinal variables were performed with Fisher exact tests and Mann–Whitney tests, respectively. Given the exploratory nature of this work, a p value <0.05 was considered significant.
Results
Study cohort
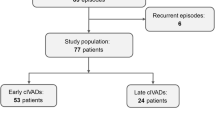
We identified 136 patients with non-anoxic SE over the study period. Of those, 53 (39 %) had RSE, of which 34 (64 %) received at least one anesthetic drug. One patient was treated only with propofol and was excluded. Thus, 33 patients were included, of which 19 received midazolam alone and 14 received thiopental alone as their first anesthetic drug. None of the drugs were used in combination with each other or with another anesthetic drug.
Demographic and clinical data are presented in Table 1; patients treated with midazolam had similar characteristics than those treated with thiopental.
Treatment
We observed no differences between groups in the delay to anesthetic treatment, duration of treatment and number and type of non-anesthetic anti-seizure medications administered prior to the anesthetic treatment (Table 2). Of note, lacosamide was available as a treatment option only during the second period of the study, during which midazolam was mostly used. Suppression-burst was achieved in 1/19 (5 %) patient in the midazolam group while it occurred in 11/14 (79 %) patients in the thiopental group (p < 0.001). Complete suppression was never reached in any group.
Outcome
The rate of SE control by the first round of anesthetics and the rate of ultimate SE control did not differ significantly between groups (12/19 [63 %] vs. 9/14 [64 %]). Similarly, the rates of acute failure, breakthrough and withdrawal seizures did not differ between groups (Table 3). In the midazolam group, we found no relationship between maximum infusion rate and acute failure (0.20 [0.20–0.27] vs. 0.25 [0.10–0.60]; p = 0.93), breakthrough (0.20 [0.10–0.53] vs. 0.30 [0.20–0.50]; p = 0.75) and withdrawal seizures (0.30 [0.10–0.75] vs. 0.20 [0.20–0.45]; p = 0.76). Individual details of maximal infusion rate and outcome are presented in supplemental Table 1. Length of ICU stay was significantly shorter in the midazolam group (6 [3–12] vs. 15 [8–23]; p = 0.02), including when considering only survivors (6 [3–11] vs. 23 [14–24]; p = 0.03). Functional outcome at discharge was better in the midazolam group (GOS-E: 1 [1–6] vs. 1 [1–3]; p = 0.04), with 3 (16 %) patients achieving good outcome compared to one (7 %) in the thiopental group. Mortality was high and did not differ between groups. Functional outcome at 6 months was better in the midazolam group than in the thiopental group (GOS-E 8 [8–8] vs. 4 [3–4]; p = 0.03), with 6/7 and 1/5 patients achieving good outcome, respectively.
Adverse events
Hypotension was significantly more frequent in the thiopental group (Table 4; 3/19 [15 %] vs. 8/14 [57 %]; p = 0.02). More patients developed infections in the thiopental group (5/19 [26 %] vs. 9/14 [64 %]; p = 0.04), in particular non-respiratory infections. Anemia requiring transfusion (3 [16 %] vs. 6 [42 %]; p = 0.04) and lymphopenia (7 [37 %] vs. 13 [93 %]; p < 0.01) were significantly more frequent in the thiopental group. This was associated with a higher mean corpuscular volume in the thiopental group (93.8 [88.8–96.6] vs. 96.7 [96.0–101.7]; p = 0.01). Hyponatremia was more frequent in the thiopental group, as well.
One patient who had been receiving thiopental to suppression-burst for 7 days developed bowel ischemia. He was also hypotensive, requiring co-administration of vasopressors.
Discussion
In this retrospective, single-center case–control study of patients undergoing CEEG for the management of RSE and treated with continuous IV midazolam or continuous IV thiopental, we found that: (1) the rate of SE control was similar in both groups (63 vs. 64 %); (2) the rates of adverse events, in particular hypotension requiring vasopressors, non-respiratory infections, cytopenias and hyponatremia were higher in patients treated with thiopental; (3) length of ICU stay was significantly longer in patients treated with thiopental and (4) functional outcome at discharge and at 6 months after discharge was worse in patients treated with thiopental. This study thus suggests that the use of CIV midazolam should be favored over the use of CIV thiopental for the treatment of RSE.
Doses of thiopental and midazolam used in this cohort were similar to those reported in other studies and within the ranges advocated by currently available guidelines [1], although midazolam doses were still lower when compared to those administered in a recent study that suggested a greater efficacy of high versus low daily regimens [8]. Thus it is possible that the rate of SE control, but also of adverse events, could have been higher if higher doses of midazolam had been used. We did not observe any significant difference in the rate of breakthrough and withdrawal seizures between groups, indicating that the differences observed in the systematic review [6] were likely due to differences in CEEG usage or to low doses of midazolam. We did not observe any relationship between SE control and the maximal infusion rate of midazolam, likely because the drugs were administered at the discretion of the treating physician without any limitation from a pre-specified protocol.
A controversy exists regarding the optimal EEG target for treatment of RSE: seizure suppression, suppression-burst or complete suppression [18–20] Our findings confirm that suppression-burst is achieved more often with barbiturates than with midazolam [8–18], but also indicate that control of RSE can be achieved independently of the degree of EEG suppression.
As expected, the rate of substantial hypotension was higher with thiopental than with midazolam [6], while the two groups were similar in terms of co-morbidity and severity of critical illness. This further confirms the better hemodynamic safety profile of midazolam in this setting. We also found a higher rate of infections, and in particular of extra-respiratory infections, in the thiopental group. This rate was similar to previous studies [5, 21, 22]. Transient bone marrow suppression and lymphopenia are a known side effect of barbiturate administration and can lead to reversible immune suppression [23–26]. Our findings indicate that midazolam also has a better safety profile with respect to the risk of nosocomial infections. Anemia requiring transfusion was more frequent and the mean corpuscular volume was significantly higher in the thiopental group. Barbiturates have been associated with megaloblastic hematopoiesis, macrocytosis and anemia in patients with chronic epilepsy [27, 28]. Folate deficiency, a typical cause of megaloblastic anemia, can occur due to inhibition of the activity of the folate carrier by barbiturates [29] but it is an unlikely mechanism in this acute setting. Megaloblastic changes and macrocytosis have also been observed in patients taking barbiturates with a normal folate level, indicating that barbiturates also directly interfere with hematopoiesis [27]. As we did not routinely measure folate levels or perform bone marrow analysis, we cannot exclude that anemia was due to another cause, such as infections, which were more frequent in the thiopental group, or occult bleeding.
Dysnatremia occurs in a third of critically ill patients [30]. In the neuro-ICU, the three main etiologies of hyponatremia are osmotic diuresis, the syndrome of inappropriate antidiuretic hormone secretion (SIADH) and the cerebral salt wasting syndrome [31]. Barbiturates are not known to directly cause SIADH. On the other hand, pentobarbital has been shown to interfere with the secretion of atrial natriuretic peptide in animals [32] and it has been hypothesized that its use could lead to cerebral salt wasting syndrome [33]. We cannot exclude that hypotension, which was more frequent in the thiopental group, also contributed to the development of hyponatremia through volume-dependent ADH secretion.
Bowel ischemia is a rare, but potentially lethal complication of treatment of RSE with profound anesthesia with thiopental [34] or with a combination of two or more anesthetic drugs [35]. As in all reported cases, our patient had been treated to suppression-burst for at least a week.
Overall, midazolam appeared to be safer than thiopental and this translated into a slight difference in outcome at discharge, although mortality did not differ between groups. One possible explanation is that the risk of mortality was mostly dictated by the underlying etiology, which was similar in both groups, while functional outcome in survivors was also influenced by the negative effect of a more prolonged ICU stay [36–38]. Another expected advantage of midazolam is that a shorter ICU stay and lower complication rate are associated with reduced costs. Mortality was high in both groups, reflecting the severity of SE episodes in this selected population with a high prevalence of elderly individuals in coma with an acute symptomatic etiology and severe forms of SE [13, 39].
Our study has several limitations: the design, a single-center retrospective study is probably the most important. However, a multi-center randomized control study of RSE has been shown to be difficult to perform [5]. With 33 patients, our study compares favorably to most series of RSE and is one of the few to offer direct comparison between two different agents. Our two groups have been treated during two different periods, resulting in some differences in standard of care between them, mostly due to the changing availability of anti-seizure medications. For example, lacosamide became available in 2010 and was only available in the midazolam cohort. However, the impact of newer anti-epileptic drugs on the management and outcome of SE is unclear [40]. Other changes in ICU care unexplored in this study might also have contributed to the better outcomes in recent years. However, we find it unlikely, since outcome after RSE has not significantly improved over the last 20 years [3, 4, 20, 36, 41].
Conclusions
This single-center retrospective study indicates that midazolam is as efficacious as thiopental for the treatment of RSE and presents a better safety profile. It is associated with a lower incidence of adverse events, especially hypotension and infections, and a shorter duration of ICU stay.
References
Brophy GM, Bell R, Claassen J, Alldredge B, Bleck TP, Glauser T et al (2012) Guidelines for the evaluation and management of status epilepticus. Neurocrit Care 17(1):3–23
Meierkord H, Boon P, Engelsen B, Göcke K, Shorvon S, Tinuper P et al (2010) EFNS guideline on the management of status epilepticus in adults. Eur J Neurol Off J Eur Fed Neurol Soc 17(3):348–355
Mayer SA, Claassen J, Lokin J, Mendelsohn F, Dennis LJ, Fitzsimmons B-F (2002) Refractory status epilepticus: frequency, risk factors, and impact on outcome. Arch Neurol 59(2):205–210
Novy J, Logroscino G, Rossetti AO (2010) Refractory status epilepticus: a prospective observational study. Epilepsia 51(2):251–256
Rossetti AO, Milligan TA, Vulliémoz S, Michaelides C, Bertschi M, Lee JW (2011) A randomized trial for the treatment of refractory status epilepticus. Neurocrit Care 14(1):4–10
Claassen J, Hirsch LJ, Emerson RG, Mayer SA (2002) Treatment of refractory status epilepticus with pentobarbital, propofol, or midazolam: a systematic review. Epilepsia 43(2):146–153
Claassen J, Mayer SA, Kowalski RG, Emerson RG, Hirsch LJ (2004) Detection of electrographic seizures with continuous EEG monitoring in critically ill patients. Neurology 62(10):1743–1748
Fernandez A, Lantigua H, Lesch C, Shao B, Foreman B, Schmidt JM et al (2014) High-dose midazolam infusion for refractory status epilepticus. Neurology 82(4):359–365
Parke TJ, Stevens JE, Rice AS, Greenaway CL, Bray RJ, Smith PJ et al (1992) Metabolic acidosis and fatal myocardial failure after propofol infusion in children: five case reports. BMJ 305(6854):613–616
Stelow EB, Johari VP, Smith SA, Crosson JT, Apple FS (2000) Propofol-associated rhabdomyolysis with cardiac involvement in adults: chemical and anatomic findings. Clin Chem 46(4):577–581
Prasad A, Worrall BB, Bertram EH, Bleck TP (2001) Propofol and midazolam in the treatment of refractory status epilepticus. Epilepsia 42(3):380–386
Riviello JJ, Claassen J, LaRoche SM, Sperling MR, Alldredge B, Bleck TP et al (2013) Treatment of status epilepticus: an international survey of experts. Neurocrit Care 18(2):193–200
Rossetti AO, Logroscino G, Milligan TA, Michaelides C, Ruffieux C, Bromfield EB (2008) Status epilepticus severity score (STESS): a tool to orient early treatment strategy. J Neurol 255(10):1561–1566
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40(5):373–383
Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H et al (1996) The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on sepsis-related problems of the European Society of Intensive Care Medicine. Intensive Care Med 22(7):707–710
Commission on epidemiology and prognosis, International league against epilepsy (1993) Guidelines for epidemiologic studies on epilepsy. Epilepsia 34(4):592–596
ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E et al (2012) Acute respiratory distress syndrome: the Berlin definition. JAMA 307(23):2526–2533
Krishnamurthy KB, Drislane FW (1999) Depth of EEG suppression and outcome in barbiturate anesthetic treatment for refractory status epilepticus. Epilepsia 40(6):759–762
Rossetti AO, Logroscino G, Bromfield EB (2005) Refractory status epilepticus: effect of treatment aggressiveness on prognosis. Arch Neurol 62(11):1698–1702
Hocker SE, Britton JW, Mandrekar JN, Wijdicks EFM, Rabinstein AA (2013) Predictors of outcome in refractory status epilepticus. JAMA Neurol 70(1):72–77
Horan TC, Andrus M, Dudeck MA (2008) CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 36(5):309–332
Parviainen I, Uusaro A, Kälviäinen R, Kaukanen E, Mervaala E, Ruokonen E (2002) High-dose thiopental in the treatment of refractory status epilepticus in intensive care unit. Neurology 59(8):1249–1251
Schalén W, Messeter K, Nordström CH (1992) Complications and side effects during thiopentone therapy in patients with severe head injuries. Acta Anaesthesiol Scand 36(4):369–377
Stover JF, Stocker R (1998) Barbiturate coma may promote reversible bone marrow suppression in patients with severe isolated traumatic brain injury. Eur J Clin Pharmacol 54(7):529–534
Loop T, Humar M, Pischke S, Hoetzel A, Schmidt R, Pahl HL et al (2003) Thiopental inhibits tumor necrosis factor alpha-induced activation of nuclear factor κB through suppression of κB kinase activity. Anesthesiology 99(2):360–367
Keel M, Mica L, Stover J, Stocker R, Trentz O, Härter L (2005) Thiopental-induced apoptosis in lymphocytes is independent of CD95 activation. Anesthesiology 103(3):576–584
Wickramasinghe SN, Williams G, Saunders J, Durston JH (1975) Megaloblastic erythropoiesis and macrocytosis in patients on anticonvulsants. Br Med J 4(5989):136–137
Reynolds EH, Chanarin I, Milner G, Matthews DM (1966) Anticonvulsant therapy, folic acid and vitamin B12 metabolism and mental symptoms. Epilepsia 7(4):261–270
Halwachs S, Kneuer C, Honscha W (2007) Downregulation of the reduced folate carrier transport activity by phenobarbital-type cytochrome P450 inducers and protein kinase C activators. Biochim Biophys Acta 1768(6):1671–1679
Vandergheynst F, Sakr Y, Felleiter P, Hering R, Groeneveld J, Vanhems P et al (2013) Incidence and prognosis of dysnatraemia in critically ill patients: analysis of a large prevalence study. Eur J Clin Invest 43(9):933–948
Rabinstein AA, Wijdicks EFM (2003) Hyponatremia in critically ill neurological patients. Neurologist 9(6):290–300
Seul KH, Cho KW, Kim SH, Hwang YH, Park CU, Koh GY (1993) Single injection of pentobarbital induces long-lasting effects on ANP synthesis and gene expression in the rat atria. Life Sci 52(16):1351–1359
Kontogiorgi M, Opsimoulis P, Diamanti-Kandarakis E, Karabinis A (2011) Cerebral salt wasting syndrome in traumatic brain injury following therapeutic barbiturate coma. Acta Neurochir (Wien) 153(8):1719–1720
Cereda C, Berger MM, Rossetti AO (2009) Bowel ischemia: a rare complication of thiopental treatment for status epilepticus. Neurocrit Care 10(3):355–358
Rizek P, Ikeda KM, Mele T, Garcia B, Gofton TE (2016) Bowel ischemia in refractory status epilepticus: report of two cases and review of the literature. Neurocrit Care 24(1):128–131
Sutter R, Marsch S, Fuhr P, Rüegg S (2013) Mortality and recovery from refractory status epilepticus in the intensive care unit: a 7-year observational study. Epilepsia 54(3):502–511
Hocker SE, Britton JW, Mandrekar JN, Wijdicks EFM, Rabinstein AA (2013) Predictors of outcome in refractory status epilepticus. JAMA Neurol 70(1):72–77
Kowalski RG, Ziai WC, Rees RN, Werner JK, Kim G, Goodwin H et al (2012) Third-line antiepileptic therapy and outcome in status epilepticus: the impact of vasopressor use and prolonged mechanical ventilation. Crit Care Med 40(9):2677–2684
Rossetti AO, Logroscino G, Bromfield EB (2006) A clinical score for prognosis of status epilepticus in adults. Neurology 66(11):1736–1738
Jaques L, Rossetti AO (2012) Newer antiepileptic drugs in the treatment of status epilepticus: impact on prognosis. Epilepsy Behav EB 24(1):70–73
Holtkamp M, Othman J, Buchheim K, Meierkord H (2005) Predictors and prognosis of refractory status epilepticus treated in a neurological intensive care unit. J Neurol Neurosurg Psychiatry 76(4):534–539
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors report no conflict of interest.
Ethical standards
This study has been approved by the appropriate ethics committee and has therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. Waiver of conset was granted given the retrospective nature of the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Bellante, F., Legros, B., Depondt, C. et al. Midazolam and thiopental for the treatment of refractory status epilepticus: a retrospective comparison of efficacy and safety. J Neurol 263, 799–806 (2016). https://doi.org/10.1007/s00415-016-8074-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-016-8074-7