
Abstract
Purpose
Preoperative localization of a parathyroid adenoma is usually obtained by the combination of ultrasound and scintigraphy with technetium-99m methoxyisobutylisonitrile. We evaluated the role of F18-fluorocholine in neck positron emission tomography/magnetic resonance imaging as a novel tool for localizing parathyroid adenomas.
Methods
Patients with primary hyperparathyroidism were recruited from February 2016 to August 2017 and F18-fluorocholine positron emission tomography/magnetic resonance imaging was performed to localize the parathyroid adenoma prior to surgery. We compared sensitivity and accuracy of this modality with ultrasound and technetium-99m methoxyisobutylisonitrile scintigraphy using the verified location of the diseased parathyroid as found in surgery.
Results
Nineteen patients were included in our study (15 women and 4 men, mean age 60.5 ± 9.8 years). Positron emission tomography/magnetic resonance imaging precisely localized the pathologic parathyroid gland in 16/19 cases (84.2%) and predicted the diseased side in 19/19 cases (100%). Ultrasound and technetium 99 m methoxyisobutylisonitrile sestamibi scintigraphy predicted the location of the parathyroid adenoma in 16/19 (84.2%) and 14/19 (74%), respectively. In 3/19 patients, positron emission tomography/magnetic resonance imaging localized the parathyroid adenoma where as other modalities failed. Positron emission tomography/magnetic resonance imaging was more accurate when compared to each modality separately (p < 0.001, p = 0.017), however, when comparing the three modalities all together no differences were found (p = 0.506).
Conclusions
Localizing parathyroid adenomas with F18-fluorocholine positron emission tomography/magnetic resonance imaging may be a promising secondary imaging modality.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Minimally invasive parathyroidectomy (MIP) has become the standard of care for the treatment for primary hyerparathyroidism (PHPT) [1], replacing the conventional bilateral neck exploration as the standard surgical approach [2]. This method has shown to shorten the time of surgery and reduce post-operative complications including, hypocalcemia and recurrent laryngeal nerve injury [3]. The ability to perform MIP is attributed to the evolving capabilities and imaging techniques enabling preoperative localization of diseased parathyroid glands [4].
Ultrasound (US) and Technetium 99 m methoxyisobutylisonitrile scintigraphy (99mTc-MIBI) are usually the preferred primary imaging modalities [4]. The reported sensitivity of US and 99mTc-MIBI in localizing single gland disease is 76.1% and 78.9%, respectively [3]. Combining these modalities may yield better results with a sensitivity ranging from 74 to 95% [4]. However, the accuracy of these modalities is significantly compromised in patients with multiple gland disease (MGD) [3].
Contrast enhanced computerized tomography (CECT) and magnetic resonance imaging (MRI) have similar sensitivities in the range of 40–71% thus, they are infrequently used [3]. Another alternative is the four-dimensional computed tomography (4D–CT) which allows capture of the consecutive stages of enhancement and clearance of contrast in the parathyroid gland when performing computed tomography (CT) angiography [5]. In recent years, 4D–CT has become a prevalent method as several studies have reported its superiority in localizing a parathyroid adenoma (PTA) [1,2,3, 5]. This modality is effective in diagnosing MGD and can be of great value in detecting ectopic glands [3]. Therefore, this modality is gradually gaining popularity as the modality of choice when other techniques fail to localize PTAs [5]. However, the main disadvantage of 4D–CT is the relatively high dose of radiation distributed to the thyroid region [3].
Several publications have reported the performance of positron emission tomography (PET) in localization of PTAs in patients with primary hyperparathryroidism [6,7,8,9,10,11]. The reported sensitivity of L–(11C) methionine (11C–MET), the most commonly used tracer, in detecting PTA is 77% [6]. Various studies have reported good results in patients who failed standard imaging modalities [7,8,9].
F18-fluorocholine (18F-FCH) is an alternative tracer whose utility has not been sufficiently studied in combination with PET–CT to localize PTAs [6, 10]. 18F-FCH has the advantage of a longer half-life of 110 min, as compared to 20 min with 11C–MET, sparing the need for on-site production [6]. The sparse data regarding 18F-FCH PET–CT have reported a good detection ability in patients with negative single photon emission tomography (SPECT), higher spatial resolution, lower radiation, and quicker scanning abilities [6]. The reported sensitivity of 18F-FCH PET–CT is in the range of 80–100% and 18F-FCH is considered the best known tracer to be used in PET–CT scan for detecting parathyroid disease [6]. Nonetheless, the search for an ideal imaging modality for localizing PTAs continues. The desired modality must be highly sensitive and avoid radiation exposure to patients, especially when other methods have failed. Thus, there are no known modalities that best combine these features.
Combined PET/MRI is gaining popularity in research and clinical use as combined PET/MRI has the advantage of providing both functional and high resolution soft tissue morphological data [12]. Potential applicability for this modality includes oncologic, cardiovascular and neurosurgical disorders, including follow-up after the treatment of central nervous system tumors [12, 13]. Emerging data suggest that PET/MRI may play a key role in the context of pediatric oncology and in evaluating inflammatory diseases such as inflammatory bowel disease, rheumatoid disorders and chronic infectious diseases [12, 14]. In this study, we present our primary results of 18F-FCH PET–MRI in localizing pathologic parathyroid glands before surgery in patients with primary hyperparathyroidism.
Methods
Study design and population
The study was approved by the local Institutional Review Board (IRB) and was conducted in accordance with the Helsinki Declaration. Following approval, we conducted an observational, comparative study on patients with PHPT who were candidates for parathyroidectomy between February 2016 and August 2017. All recruited patients received 18F-FCH PET–MRI at the Department of Radiology in our institution. Our inclusion criteria consisted of adult patients above 18 years old with PHPT and who had recently completed both US and dual time-point single photon emission tomography (SPECT) 99mTc-MIBI studies prior to surgery. All patients were required to sign an informed consent prior to the study.
18F-FCH PET–MRI protocol
Patients were injected with 2.5 mCi (93.75 MBq) of 18F-FCH with an estimated effective dose equivalent of 2.8 mSv that complies with the single-study FDA limit of 3.0 mSv for research subjects. Immediately after injection, FCH PET/MRI was performed in a single bed position with the patient centered on the thyroid bed on a hybrid PET/MRI system (Biograph mMR, Siemens AG, healthcare sector, Erlangen, Germany). Simultaneously, we performed PET and MRI imaging acquisition for 16 min. PET data were acquired in the list mode and reconstructed with 3D-OSEM, (3 iterations, 21 subsets and 4 mm Gaussian filter) on 172 matrices. Coronal Dixon-based sequences for MRI attenuation correction (MRAC) was obtained. Increased focal FCH uptake in the neck region above background was considered to represent parathyroid adenoma (Figs. 1, 2).

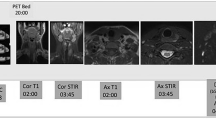
a MR image axial STIR of patient with parathyroid adenoma showing left lower pole thyroidal lesion/high signal on T2-weighted sequence corresponding to PET high uptake adenoma. b Axial AC PET, high choline uptake in left lower thyroid lesion. c MR image coronal T1-weighted post contrast showing enhancing lesion in lower pole of thyroid corresponding to PET

a MR image coronal STIR of patient with PTA/large cystic component with upper hypointense solid component. b Coronal fusion of PET/MRI with large cystic component and high uptake area at the upper pole of lesion
MRI acquisition was obtained using a 16 channel head and neck RF coil integrated within the MRI bed. The MRI sequences for pre- and post-Dotarem were 0.1 mmol/kg, 3 cc/s. Injection included T1 TSE axial images TR-620 TE-11 FA-150, FOV 200*200 MM T2 TSE Dixon sagittal and coronal images TR-5310 TE-82 FA-160, FOV 300*270 MM. Inclusion also consisted of T2 TSE Dixon axial images TR-4970 TE-73 FA-160, FOV 192*240. We used Vibe T1 dynamic scan post-contrast for 20 phases immediately post injection every 6 s (TR-5 TE 1.8 FA 15 260*260 FOV), in addition to, T1 TSE axial and coronal Fat-Sat images (TR-670 TE-11 FA-150). All images were 3 mm thick.
Imaging analysis
Interpretation of the PET/MRI studies were conducted by a nuclear radiologist that reported the PET portion of the study and by a dedicated head and neck radiologist that reported on the MRI. Both physicians were aware of clinical diagnosis of hyperparathyroidism and blinded to previous conventional images. Final interpretation of the presence and localization of the abnormal parathyroid was based on the combined assessment of both modalities.
Surgery
All patients underwent MIP. Prior to surgery, the surgeons reviewed all three localization modalities. The intraoperative location of the pathological parathyroid (PPT) gland was confirmed by frozen section pathology. All patients were discharged either on the same day or one night after surgery. Serum calcium levels were checked during hospitalization after surgery. Based on clinical judgment, intraoperative serum parathyroid hormone levels (IOPTH) were examined prior to surgery and at the time of dissection of the adenoma (10 min after the gland excision) in a few patients.
Statistical analysis
Continuous data (such as age, serum levels) were summarized as mean, standard deviation and range, and categorical data (such as gender) as number and percent. Sensitivity was calculated using MedCalc for Windows, version 17.9 (MedCalc Software, Ostend, Belgium).
We compared accuracy of the three imaging modalities using the Chi-square test. Post-hoc analyses were administered to test differences between each combination of two imaging modalities, using a Bonferroni correction with significant level of p < 0.017. In addition, inter-modality compatibility was assessed using Cohen’s kappa for each pair of the three modalities using Bonferroni correction, and Fleiss kappa for multiple imaging modalities. The level of agreement was classified as poor (≤ 0.01), slight (0.01–0.20), fair (0.21–0.40), moderate (0.41–0.60), substantial (0.61–0.80), and almost perfect (0.81–1.00) [15, 16]. These analyses were calculated using the SPSS statistical package (Version 24, IBM Inc., Chicago, IL).
Results
Study population
A total of 24 patients with PHPT were recruited in this study. Nineteen patients underwent surgery and were included in this study. Five patients were excluded (two were advised to withhold surgery by the endocrinologist, two decided to postpone surgery for other health considerations, and one underwent surgery elsewhere with no follow-up). Participants consisted of 4 males and 15 females. The age ranged between 40 and 75 years, mean age 60.5 ± 9.8 years.
Eleven patients (57.8%) presented with osteoporosis or osteopenia, three of which experienced previous pathologic fractures. Six patients (31.6%) had renal colic, five reported symptoms of weakness, and two patients reported mood changes. One patient was asymptomatic and was diagnosed incidentally during goiter workup (Table 1, patient #19).
Preoperative calcium level ranged from 10.2 to 12.7 mg/dl (mean 11.2 ± 0.62). Preoperative PTH levels ranged from 88 to 399 pg/ml (mean 176.68 ± 85.45).
Imaging analysis
Preoperatively, US accurately predicted the pathologic parathyroid gland (PPT) location in 16/19 patients (sensitivity 84.2%). In 2/19 patients (10.5%) US failed to predict the diseased gland, while in 1/19 (5.3%) US suggested the side of the neck with the presumably diseased gland. In this patient, US could not identify the PTA being embedded into the thyroid parenchyma (88.9% side sensitivity). Dual time-point SPECT 99mTc-MIBI accurately predicted the PPT gland locations in 14/19 cases (sensitivity; 73.7%). Meanwhile, it failed to localize in two patients and localized only the side of the neck in three cases in which the parathyroid glands were embedded in the thyroid (88.9% side sensitivity). In 14/19 patients, US and 99mTc-MIBI results matched. This match precisely localized the disease in 13/14 cases (sensitivity: 92.8%). In the remaining patient US and 99mTc-MIBI predicted the side, however, could not identify the PTA as being embedded into the thyroid parenchyma.
The correct location of the PPT was suggested by F18-FCH PET/MRI in 16/19 patients (84.2%) (sensitivity;84.2%) (Fig. 1). However, F18-FCH PET/MRI failed to precisely localize the PPT gland in three patients. While it accurately predicted the side of the diseased glands, which were all embedded in the thyroid parenchyma, it did not predict the intraparenchymal location (100% side sensitivity). Out of the three failures, one had cystic upper PTA with enlarged ipsilateral thyroid gland, a finding that was also missed by the other two modalities (Table 1, patient #15) (Fig. 2). In three cases, F18-FCH PET/MRI localized the PPT gland where either US or 99mTc-MIBI failed, and could predict the side of the pathology in all 19 patients (Table 2).
When comparing the accuracy of the three modalities all together, there was no significant difference between them (p = 0.506), however, PET/MRI was found to be more accurate when compared to MIBI and US separately (p < 0.001, p = 0.017, respectively). In contrast, there was no significant difference between MIBI and US (p = 0.082) (Table 2).
Overall inter-modality compatibility among all three imaging modalities was moderate (Fleiss kappa = 0.466, p < 0.001). PET/MRI and US also showed moderate compatibility (Cohen’s kappa = 0.441, p = 0.004), as in 16/19 patients both of them located PPT at the same level of accuracy, and in 3/19 patients they located it at different accuracy level; in two patients, out of these three, US failed to locate PPT while PET/MRI succeeded to locate it accurately in one patient and located the side of the neck in the other patient (Table 1, patients #12, 15, respectively), and in one patient US succeeded to locate PPT accurately, while PET/MRI localized only the side of the neck (Table 1, patient #9). PET/MRI and MIBI showed the highest compatibility rate (Cohen’s kappa = 0.703, p < 0.001), as in 17/19 patients the PPT was located similarly by these two imaging modalities, and in only 2/19 patients PET/MRI localized PPT precisely, while MIBI failed to locate it (Table 1, patients #13–14). In contrast, MIBI and US showed the lowest compatibility rate, which was not statistically significant (Cohen’s kappa = 0.269, p = 0.099).
Surgery
Surgical excision of the PPT gland was successfully performed in all 19 patients (100%). In 11/19 cases (57.9%) the PPT glands were located in the right side and all were in a lower position. In 8/19 patients (42.1%) the PPT was found to be in the left side (7/8 patients were on the lower pole and 1/8 were on the upper pole). Our results also showed that in 3/19 patient cases, PPT glands were located in an intra-thyroid location. In addition, 4/19 patients had hemithyroidectomy; 2/4 due to associated thyroid gland pathology (adenoma and goiter), as well as, 2/4 patients had their hemithyroid excised when the PTA was not found (in both cases the parathyroid adenoma was found within the thyroid parenchyma). All participants (100%) were examined intraoperatively by frozen section to verify the excision of the diseased parathyroid gland. In 5/19 patients underwent quick intra-operative PTH (IOPTH) assay test which was taken before and after PTA excision (Table 1, patients #6, 9, 12, 14 and 15,). In these patients, excluding patient number 6, at least one of the three modalities failed to show precise localization of the PTA before surgery. However, results showed that there were significant drops in PTH value confirming sufficient surgical excision in all patients. Final pathological results showed that 18/19 patients had PTA, while one patient had suspected parathyroid carcinoma (Table 1, patient #7). Post-operative blood calcium levels were obtained for all patients and were found within normal limits.
Discussion
In this observational, comparative study we evaluated the performance of hybrid PET/MRI, using 18F-FCH as a tracer, for the preoperative evaluation of patients with PHPT. We hypothesized that PET/MRI had an advantage over other imaging modalities used due to its ability to supply both functional and anatomic data that may be valuable in searching for the enlarged parathyroids in the neck. We found that hybrid PET/MRI, using the 18F-FCH tracer, was as accurate as US and 99mTc-MIBI in localization of the precise location of the PPT gland(s), and even superior to the other modalities when compared to each separately (p < 0.001, p = 0.017, respectively). Moreover, hybrid PET/MRI was superior to the other modalities in determining the side of the pathology where it was successful in all the patients 19/19 in our study (Table 2). In most cases, 18F-FCH PET/MRI also performed well in patients where the other modalities failed as presented in Table 1 (patients #12–15). This is also evident from the inter-modality compatibility analyses, as this study found substantial compatibility between PET/MRI and MIBI, and moderate compatibility between PET/MRI and US. This moderate compatibility with US is consequently of the fact that in two patients US could not detect the location while PET/MRI detect it accurately or partially and in one patient, US could detect the location more precisely than 18F-FCH PET/MRI (Table 1, patient #9). This emphasizes the role of US, in experienced hands, as the first used modality during PHPT work-up.
PET/MRI failed to precisely localize the PPT gland in three patients. In all three of patients the diseased glands were located inside the thyroid parenchyma. However, the uptake of 18F-FCH was found to localize the correct side of the lesion. The exact intra-thyroid location of the PTA could, therefore, not be determined preoperatively. In one of these cases, a cystic parathyroid was found presenting as a rim enhancement of 18F-FCH around the cyst suggesting a cystic parathyroid, but as mentioned previously, the exact intra-thyroid location of the adenoma could not be identified.
Current scientific literature is lacking regarding intra-thyroid PTAs as this entity is relatively rare. In a recent study, Ryan and colleagues [17], found an intra-thyroid location of the adenoma in 4% of their patients. In our experience, the high frequency of intra-thyroid PTAs was uncommon. However, since no localization of intra-thyroid adenomas was observed, it seems that PET/MRI may be less useful in patients with intra-parenchymal PPT glands. Nonetheless, when a PTA is not found during surgery and we cannot identify a parathyroid, these data suggest consideration of excision of the ipsilateral thyroid lobe based on the positive 18F-FCH uptake with 100% side sensitivity, preventing contra-lateral exploration. This recommendation is even stronger in the presence of a thyroid nodule in the ipsilateral side (of the 18F-FCH uptake) on pre-operative imaging modalities. However, this study is limited by the low number of patients, thus these results need to be validated with larger prospective studies. We do not have an explanation for the high incidence of intra-thyroid parathyroid adenoma and a rate of 3/19 is certainly higher than usual. In our experience with hundreds of cases per year, the incidence was usually much lower. This finding may be just coincidence in small cohort of patients.
In a previous publication examining the accuracy of PET/MRI for the localization of PTAs, Kluijfhout et al. [18], evaluated the performance of 18F-FCH PET/MRI in patients with PHPT. All the participants exhibited non-localized diseases via traditional modalities. In this pilot study, FCH PET/MRI correctly localized the adenoma in 9/10 patients (90% sensitivity) with no false positive results (100% positive predictive value) [18]. In another recent published report [19], the authors accurately localized parathyroid adenomas in 25 out of 26 (96.2%) patients; using PET/CT in 11 patients and PET/MRI in 15 patients. This is in accordance with our results where parathyroid adenomas were identified in 16 out of 19 (84.2%) patients. Furthermore, positive uptake of 18F-FCH showed a correlation with the correct side of the adenoma in 100% of our patients.
PET/MRI is associated with significantly lower amounts of radiation when compared to CT, PET/CT and 99mTc-MIBI [12, 18]. Reports suggest a lower number of required imaging studies using this modality [12]. Furthermore, the imaging time is shorter [18]. All indicate that PET-MRI may be a second line imaging modality for patients with PHPT saving patients from undergoing more invasive and non-invasive studies. Considering unnecessary radiation exposure and extended surgeries with a higher rate of morbidity, the increase in the overall cost may be considerable.
Several studies have reported good results of MIP without the use of IOPTH monitoring based on good localization of the gland prior to surgery by US and 99mTc-MIBI [20,21,22,23].
In our study, rapid IOPTH assays were obtained in five patients, which prompted our physicians to seek further confirmation for excising the pathology. Following our policy guidelines, during the study, we did not routinely monitor IOPTH in all parathryoid surgeries, but rather performed this test in a selective manner. We utilized both US and 99mTc-MIBI before surgery in concordance with localizing the gland because IOPTH monitoring is not standard protocol, unless the lead surgeon decides otherwise. We recommend tailored IOPTH monitoring according to the surgery’s course, surgeon experience, and the ability to accurately localize the pathological gland before surgery.
One of our major limitations in this study was the small population size which affected our ability to accurately reflect significance. Moreover, five patients were excluded after PET/MRI, four of which did not undergo surgery and one of which underwent surgery elsewhere and was lost to follow-up. Obtaining a larger sample size may be very challenging due to the poor availability of PET/MRI devices and lack of professionally skilled personnel available to perform and interpret the results. Therefore, incorporating PET/MRI as a standard imaging modality may be limited at some facilities due to the costs associated with PET/MRI.
Conclusion
This study shows that F18-FCH PET/MRI is highly sensitive and accurate in localizing PPT gland in patients with PHPT. Along with proven safety and feasibility, we suggest this modality as a second line option when traditional modalities (US and 99mTc-MIBI scan) fail to localize the adenoma. This may result in a quicker and more accurate localization of the adenoma, with less radiation exposure and may, therefore, ultimately be more cost-effective. Further studies with larger patient sample sizes are required to establish the role of F18-FCH PET/MRI in localizing PTAs.
References
Brown SJ, Lee JC, Christie J, Maher R, Sidhu SB, Sywak MS, Delbridge LW (2015) 4DCT for parathyroid localization. ANZ J Surg 85:483–487. https://doi.org/10.1111/ans.12571
Suh YJ, Choi JY, Kim SJ, Chun IK, Yun TJ, Lee KE, Kim JH, Cheon GJ, Youn YK (2015) Comparison of 4D CT, ultrasonography, and 99mTc sestamibi SPECT/CT in localizing single-gland primary hyperparathyroidism. Otolaryngol Head Neck Surg 152:438–443. https://doi.org/10.1177/0194599814562195
Kunstman JW, Kirsch JD, Mahajan A, Udelsman R (2013) Clinical review: parathyroid localization and implications for clinical management. J Clin Endocrinol Metab 98:902–912. https://doi.org/10.1210/jc.2012-3168
Kelly HR, Hamberg LM, Hunter GJ (2014) 4D–CT for preoperative localization of abnormal parathyroid glands in patients with hyperparathyroidism: accuracy and ability to stratify patients by unilateral versus bilateral disease in surgery-naïve and re-exploration patients. AJNR Am J Neuroradiol 35:176–181. https://doi.org/10.3174/ajnr.A3615
Rameau A, Eng S, Vu J, Saket R, Jun P, Friduss M (2017) Four-dimensional computed tomography scan utility in parathyroidectomy for primary hyperparathyroidism with low baseline intact parathyroid hormone. Laryngoscope 127:1476–1482. https://doi.org/10.1002/lary.26201
Kluijfhout WP, Pasternak JD, Drake FT et al (2016) Use of PET tracers for parathyroid localization: a systematic review and meta-analysis. Langenbecks Arch Surg 401:925–935
Yuan L, Liu J, Kan Y, Yang J, Wang X (2017) The diagnostic value of 11C-methionine PET in hyperparathyroidism with negative 99mTc-MIBI SPECT: a meta-analysis. Acta Radiol 58(5):558–564. https://doi.org/10.1177/0284185116661878
Noltes ME, Coester AM, Van der Horst-Schrivers ANA et al (2017) Localization of parathyroid adenomas using 11C-methionine pet after prior inconclusive imaging. Langenbecks Arch Surg 402:1109–1117. https://doi.org/10.1007/s00423-017-1549-x
Weber T, Gottstein M, Schwenzer S, Beer A, Luster M (2017) Is C-11 methionine PET/CT able to localise sestamibi-negative parathyroid adenomas? World J Surg 41:980–985. https://doi.org/10.1007/s00268-016-3795-4
Kluijfhout WP, Vorselaars WM, van den Berk SA et al (2016) Fluorine-18 fluorocholine PET-CT localizes hyperparathyroidism in patients with inconclusive conventional imaging: a multicenter study from the Netherlands. Nucl Med Commun 37:1246–1252
Kluijfhout WP, Vorselaars WM, Vriens MR, Borel Rinkes IH, Valk GD, de Keizer B (2015) Enabling minimal invasive parathyroidectomy for patients with primary hyperparathyroidism using Tc-99m-sestamibi SPECT-CT, ultrasound and first results of (18)F-fluorocholine PET-CT. Eur J Radiol 84:1745–1751. https://doi.org/10.1016/j.ejrad.2015.05.024
Gatidis S, Bender B, Reimold M, Schäfer JF (2017) PET/MRI in children. Eur J Radiol 94:A64–A70. https://doi.org/10.1016/j.ejrad.2017.01.018
Mittal BR, Singh S (2017) Hybrid PET/MR imaging for evaluation of recurrence in gliomas: standard of care or luxury? Neurol India 65:302–304. https://doi.org/10.4103/0028-3886.201846
Domachevsky L, Leibovitzh H, Avni-Biron I et al (2017) Correlation of 18F-FDG PET/MRE metrics with inflammatory biomarkers in patients with Crohns disease. a pilot study. Contrast Media Mol Imaging 19:7167292. https://doi.org/10.1155/2017/7167292
McHugh ML (2012) Interrater reliability: the kappa statistic. Biochem Med (Zagreb) 22:276–282
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Ryan S, Courtney D, Moriariu J, Timon C (2017) Surgical management of primary hyperparathyroidism. Eur Arch Otorhinolaryngol 274:4225–4232. https://doi.org/10.1007/s00405-017-4776-4
Kluijfhout WP, Pasternak JD, Gosnell JE et al (2017) 18F fluorocholine PET/MR imaging in patients with primary hyperparathyroidism and inconclusive conventional imaging: a prospective pilot study. Radiology 284:460–467. https://doi.org/10.1148/radiol.2016160768
Huber GF, Hüllner M, Schmid C et al (2018) Benefit of 18F-fluorocholine PET imaging in parathyroid surgery. Eur Radiol 28:2700–2707. https://doi.org/10.1007/s00330-017-5190-4
Soyder A, Ünübol M, Ömürlü İK et al (2015) Minimally invasive parathyroidectomy without using intraoperative parathyroid hormone monitoring or gamma probe. Ulus Cerrahi Derg 31:9–14. https://doi.org/10.5152/UCD.2014.2572
Patel KN, Caso R (2016) Intraoperative parathyroid hormone monitoring: optimal utilization. Surg Oncol Clin N Am 25:91–101. https://doi.org/10.1016/j.soc.2015.08.005
Sakimura C, Minami S, Hayashida N et al (2013) Can the use of intraoperative intact parathyroid hormone monitoring be abandoned in patients with hyperparathyroidism? Am J Surg 206:574–577. https://doi.org/10.1016/j.amjsurg.2013.01.043
Helbrow J, Owais A, Sidwell A, Frank L, Lucarotti M (2016) The use of intraoperative parathyroid hormone monitoring in minimally invasive parathyroid surgery. Ann R Coll Surg Engl 98:516–519. https://doi.org/10.1308/rcsann.2016.0201
Acknowledgements
Nyall R. London Jr. MD, PhD. Ohio State University—College of Medicine. Department of Otolaryngology—Head and Neck Surgery. Columbus, Ohio 43210. Performed grammar and English language review.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Khafif, A., Masalha, M., Landsberg, R. et al. The role of F18-fluorocholine positron emission tomography/magnetic resonance imaging in localizing parathyroid adenomas. Eur Arch Otorhinolaryngol 276, 1509–1516 (2019). https://doi.org/10.1007/s00405-019-05301-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-019-05301-2