
Abstract
Purpose
Identification of pathologic parathyroid glands in primary hyperparathyroidism, traditionally based on neck ultrasound (US) and/or 99mTc-Sestamibi scintigraphy, can be challenging. PET/CT with 18F-Fluorocholine (18F-FCH) might improve the detection of pathologic parathyroid glands. We aimed at comparing the diagnostic performance of 18F-FCH-PET/CT with that of dual-phase dual-isotope parathyroid scintigraphy and neck US.
Methods
Thirty-four consecutive patients with primary hyperparathyroidism were prospectively enrolled, 7 had normocalcemic hyperparathyroidism, and 27 had classic hypercalcemic hyperparathyroidism. All patients underwent high-resolution neck US, dual-phase dual-isotope 99mTc-Pertechnetate/99mTc-Sestamibi scintigraphy, and 18F-FCH-PET/CT.
Results
In the whole patients’ group, the detection rates of the abnormal parathyroid gland were 68% for neck US, 71% for 18F-FCH-PET/CT, and only 15% for 99mTc-Sestamibi scintigraphy. The corresponding figures in normocalcemic and hypercalcemic hyperparathyroidism were 57 and 70% for neck US, 70 and 71% for 18F-FCH-PET/CT, and 0 and 18% for 99mTc-Sestamibi scintigraphy, respectively. In the 17 patients in whom the abnormal parathyroid gland was identified, either at surgery or at fine needle aspiration cytology/biochemistry, the correct detection rate was 82% for neck US, 89% for 18F-FCH-PET/CT, and only 17% for 99mTc-Sestamibi scintigraphy.
Conclusions
18F-FCH-PET/CT can be considered a first-line imaging technique for the identification of pathologic parathyroid glands in patients with normocalcemic and hypercalcemic hyperparathyroidism, even when the parathyroid volume is small.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Primary hyperparathyroidism is diagnosed biochemically and further characterized with ultrasonographic, radiologic, and nuclear medicine techniques. Preoperative detection of abnormal parathyroid glands is becoming more and more challenging, since primary hyperparathyroidism is increasingly being diagnosed in a subclinical or asymptomatic stage of the disease, i.e., with small size or mildly hyperfunctioning gland(s). Indeed, normocalcemic primary hyperparathyroidism (NPHPT) has been formally recognized in 2009 at the Third International Workshop on the Management of Asymptomatic Primary Hyperparathyroidism [1]. The prevalence of this entity in an unselected population is difficult to assess, but is reported to range between 0.4 and 3% of the general population [2]. NPHPT is now considered a milder form of primary hyperparathyroidism, that confers, however, a risk of complications higher than in the general population [3, 4].
Ultrasonography of the neck is routinely performed in patients with biochemical or clinical disease, but radionuclide parathyroid imaging using 99mTc-Sestamibi also plays a major role, mainly because of its capability to detect multiple abnormal glands, even in ectopic locations. Nevertheless, parathyroid scintigraphy remains an intriguing challenge both because of the small size/weight of normal parathyroid glands and because they are frequently embedded within the thyroid, which has a much greater mass and a higher metabolic activity. Therefore, in the large majority of cases, parathyroid scintigraphy is diagnostically useful only when these glands are abnormally enlarged and/or strongly hyperfunctioning, as it mainly occurs in overt clinical hyperparathyroidism [5, 6] or in parathyroid carcinomas [7], which, however, constitute < 1% of all cases of hyperparathyroidism.
The development of hybrid SPECT/CT gamma cameras, which simultaneously exploit morphologic information provided by CT, further improved radionuclide images, both by providing anatomical correlates to functional findings and by allowing accurate attenuation correction. A further advantage of PET imaging over single-photon imaging is the ability to detect mediastinal adenomas, because high-energy gamma (511 keV) rays originating from the annihilation reaction are less attenuated by the sternum and chest cage than the 140 keV gamma rays emitted by 99mTc.
Preoperative imaging of abnormally functioning parathyroid glands is particularly challenging in patients with normocalcemic primary hyperparathyroidism, a milder form of the disease. In a 2012 study involving a limited number of patients, the sensitivity of both 99mTc-Sestamibi scintigraphy and ultrasonography was lower in normocalcemic patients (40 and 50%, respectively) than in hypercalcemic patients (57 and 53%, respectively) [8]. In a recent study by Šiprová et al., 99mTc-Sestamibi scintigraphy localized abnormal parathyroid glands in only 6% of patients with the normocalcemic disease and in 14% of those who subsequently developed hypercalcemia [9]. Besides occasional case reports in single patients, so far, only a few ad-hoc studies have been published on preoperative imaging of pathologic parathyroid glands with 18F-Fluorocholine (18F-FCH) PET/CT [10,11,12]. In a recent study, Thanseer et al. showed that 18F-FCH-PET/CT performed better for preoperative localization of parathyroid glands than neck ultrasonography and 99mTc-Sestamibi scintigraphy. However, the majority of patients included in this study had overt hypercalcemic hyperparathyroidism (mean PTH 171 pg/mL and mean calcium 11.9 mg/dL) [13], therefore, leaving unsettled the issue about the diagnostic performance of 18F-FCH-PET/CT in patients with the normocalcemic stage of the disease.
To better evaluate the possible clinical role of 18F-FCH-PET/CT in patients with primary hyperparathyroidism, we hereby report our experience in a series of 34 consecutive patients and 38% of whom had normocalcemic hyperparathyroidism. The results of 18F-FCH-PET/CT were compared with those obtained with 99mTc-Sestamibi scintigraphy and neck ultrasonography.
Materials and methods
Patients
Between February and October 2016, 34 consecutive patients with primary hyperparathyroidism, 24 women and 10 men (mean age 63 ± 12 SD years; range 26–82 years) were prospectively enrolled by the Nuclear Medicine Department of a multicenter hospital with five large inpatients clinics located in different counties all over Lombardia. All of them were affected by sporadic primary hyperparathyroidism. Exclusion criteria were a history of neoplastic disease or pregnancy, hydrochlorothiazide or lithium medication, a diagnosis hypercalciuria, or gastrointestinal disorders associated with calcium malabsorption, moderate–severe renal failure (eGFR < 60 mL/min). The diagnosis of primary hyperparathyroidism was based on clinical data and/or raised serum parathyroid hormone (PTH) levels after successful correction of any vitamin D deficiency (25-hydroxyvitamin D level greater than 30 ng/mL). The study group included 7 patients (20% of the overall population) with the so-called normocalcemic hyperparathyroidism, and 28 patients with classic hypercalcemic hyperparathyroidism. Normocalcemic hyperparathyroidism was defined according to the stringent criteria of Bilezikian and Silverberg [14], namely these patients had at least two normal albumin-adjusted total serum calcium results, which were confirmed by ionized calcium measurement.
The classic hypercalcemic hyperparathyroidism group also included three patients with apparently normal serum PTH levels, which, however, were inappropriate because of concomitant, persistent hypercalcemia. The mean age of these three patients did not differ from that of the whole-study group. Ten out of thirty-four patients (29%) had a concomitant multinodular goiter and 7/34 patients (20%) had chronic autoimmune thyroiditis.
All patients gave their written consent to be enrolled for the study, which had been approved by the Institutional Ethical Committee of the Maugeri’s Foundation on 18.01.2016, no. 2003-CEC.
Methods
In vitro lab tests
Total serum calcium was measured using the COBAS Analyzer (Roche diagnostic GmbH Mannheim, Germany). The reference range was 8.8–10.2 mg/dL. Serum intact PTH was measured using a chemiluminescent double antibody immunometric assay with intra-assay and inter-assay coefficients of variation of 2.6 and 5.4%, respectively. Normal range for serum PTH was 11.5–78.4 ng/mL.
Ionized calcium was measured in heparin-treated venous blood using an electro-chemical method run by Radiometer ABL 800 FLEX gas analyzer. The normal range was 1.15–1.29 mmol/L.
High-resolution neck ultrasonography (US)
Neck US was performed using a real-time US device equipped with a linear transducer operating at 7.5 MHz (ESAOTE, Mylab 70XVG). Neck lesions possibly related to pathologic parathyroid gland/s were characterized according to the following features: localization, structure (i.e., solid, cystic, or mixed), size, and color-flow Doppler pattern. Volume was calculated by the elliptical shape formula (length × width × depth × 0.52). All neck US scans were performed by the same experienced operator (S.C.). Fine needle aspiration cytology (FNAC) coupled with measurement of PTH in the needle washout liquid was also performed.
Dual-phase dual-isotope 99mTc-Pertechnetate/99mTc-Sestamibi scintigraphy
All patients underwent dual-phase dual-isotope 99mTc-Pertechnetate/99mTc-Sestamibi scintigraphy. Thyroid scintigraphy (TS) was acquired 20 min after the intra-venous administration of 74 MBq of 99mTc-pertechnetate (Tekcis, IBA Molecular). Subsequently, early (20 min) and delayed (2 h) scans were obtained after the i.v. injection of 8.8 MBq/kg of 99mTc-Sestamibi (Stamicis, IBA Molecular). Thyroid and parathyroid images were acquired with an SPECT/CT gamma camera (Infinia Hawkeye 4 GP3, GE Healthcare) using an LEHR collimator, the FOV extending from the salivary glands to the myocardium. Anterior views of the patient in supine position with hyperextended neck were acquired. In each patient, the same strictly controlled position was used for both thyroid and parathyroid scintigraphy (PS). At the end of the second 99mTc-Sestamibi acquisition, an SPECT/CT scan of the neck and upper thorax was acquired (30 s/step, with a 3° rotation angle, and 360° rotation), which was reconstructed using an OSEM algorithm (2 iterations and 10 subset); attenuation correction was also carried out using the CT transmission data. Visual image interpretation of planar and SPECT/CT scans was followed by analysis of the images obtained by subtracting TS from PS (both early and delayed images). The results of 99mTc-Pertechnetate/99mTc-Sestamibi scintigraphy were evaluated by two experienced nuclear medicine physicians (G.T. and C.V.) blinded to each other. Images were defined as positive or negative, the former instance indicating a pathologic parathyroid. When a scan was judged as positive, the number and location of suspected parathyroid glands (right or left, superior or inferior, and ectopic) were also defined.
18F-Fluorocholine PET/CT
Patients underwent PET/CT using a Discovery 690 VCT PET/CT scanner (GE Healthcare). First, a low-dose CT (120 kV, 80 mA) was acquired. After CT acquisition, the patient, still lying inside the gantry, was injected i.v. with 3–3.5 MBq/kg of 18F-FCH (IASOcholine®, IASON GmbH) followed by 10 mL of saline solution. Static images were acquired 9 and 60 min after tracer injection (3 min/bed), and were reconstructed using an OSEM algorithm (3 iterations, 18 subsets, and FWHM of the Gaussian filter 5 mm). TOF and PSF corrections were also performed, as well as attenuation and scatter correction. Two experienced nuclear medicine physicians (M.H., I.B.) interpreted the 18F-FCH-PET/CT images by visually evaluating suspicious hyperfunctioning parathyroid glands. The same color scale as for the 99mTc-Sestamibi scan was used. Physicians were blinded to each other and to the results of the 99mTc-Sestamibi scan. Disparities were resolved by consensus.
Statistical analysis
Mean values ± SD were used for descriptive analysis. Comparison between percentages was performed by the Chi-squared test. Comparison between means was performed by T test. Sensitivity and specificity were calculated in patients who underwent surgery or of FNAC/biochemistry (gold standard). When these data were not available, clinical and biochemical descriptive data were reported.
Results
None of the three patients who had inappropriately normal serum PTH levels (with concomitant, persistent hypercalcemia) exhibited peculiarities regarding the imaging findings. Therefore, to the purpose of the present study, these three patients were included in the group of patients diagnosed as having classic hypercalcemic hyperparathyroidism.
All patients submitted to surgical neck exploration were found to have a single parathyroid adenoma derived from chief cells. Surgical cure of hyperparathyroidism was confirmed by biochemical tests at follow-up.
As shown in Table 1, the abnormal parathyroid gland was detected in 68% of the whole patients’ group by neck US, and in 71% by 18F-FCH-PET/CT. The detection rate was much lower using 99mTc-Sestamibi scintigraphy (15%). Stratification of patients according to normocalcemia or hypercalcemia showed that, in the former group, 18F-FCH-PET/CT had a higher detection rate (71%) than neck US (57%), while 99mTc-Sestamibi scintigraphy was useless, having a null detection rate. As shown in Table 2, comparison of the three imaging techniques in the whole group of patients indicated a good concordance rate between neck US and 18F-FCH-PET/CT (53%). On the contrary, the concordance rate between 99mTc-Sestamibi scintigraphy and 18F-FCH-PET/CT was low (6%).
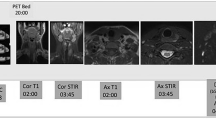
Figure 1 shows an example of the imaging results with the three techniques (Panel 1: neck US, Panel 2–3: 99mTc-Sestamibi scintigraphy, Panel 4–5: 18F-FCH-PET/CT) in a case of normocalcemic hyperparathyroidism which was later confirmed with surgery. Neck US and 18F-FCH-PET/CT showed concordant results, while 99mTc-Sestamibi failed to show any abnormal parathyroid.

An example of the imaging results with the three techniques in a case of normocalcemic hyperparathyroidism which was later confirmed with surgery. Panel 1: US imaging of the suspicious hyperfunctioning parathyroid gland of the inferior left group, measuring 7 × 14 mm, in a patient with normocalcemic hyperparathyroidism. Panel 2: dual-phase dual-isotope 99mTc-Pertechnetate/99mTc-Sestamibi scans of the same patient: no evidence of hyperfunctioning parathyroid, even in the subtraction image (early subtraction image shown in panel 3). Panels 4–5: early (panel 4) and delayed (panel 5) 18F-FCH-PET/CT images, showing a focal area of increased tracer uptake in the left inferior parathyroid group. Histology confirmed the presence of a parathyroid adenoma
Results were also analyzed in the subgroup of patients in whom the abnormal parathyroid gland was eventually identified, either at surgery or by fine needle aspiration cytology/biochemistry (Table 3). In these 17 patients, the correct detection rate was high (82%) for neck US and 18F-FCH-PET/CT (89%), while it was poor for 99mTc-Sestamibi scintigraphy (17%). Comparison of the three imaging techniques in patients with definitely identified abnormal parathyroid gland, as shown in Table 4, indicated a good concordance rate between neck US and 18F-FCH-PET/CT (67%), which did not decrease after stratification according to normocalcemia or hypercalcemia. No patient was simultaneously positive at 99mTc-Sestamibi scintigraphy and 18F-FCH-PET/CT.
No significant difference was observed by comparing the mean serum PTH levels in patients with positive or negative imaging using any of the three techniques. Most of the lesions in the neck identified as parathyroid-like were small in size and their mean (± SD) volume being 0.6 ± 0.5 mL (range 0.1–1.8 mL). No significant difference was observed when comparing the mean parathyroid size, as assessed by US, in patients with positive or negative imaging using the three different techniques.
Considering histopathology and/or cytology/biochemistry as the gold standard, the following sensitivities were calculated: 99mTc-Sestamibi scintigraphy = 17%, neck US = 82%, and 18F-FCH-PET/CT = 88%. No false-positive result was obtained with 99mTc-Sestamibi scintigraphy or 18F-FCH-PET/CT, while there was one false-positive result with neck US.
Discussion
At present, the majority of patients with primary hyperparathyroidism are diagnosed by biochemical tests when their disease is still in a preclinical or subclinical stage. Thus, the identification of the hyperfunctioning parathyroid gland(s) is becoming more and more challenging. Neck US currently remains the first-line diagnostic imaging procedure in patients with primary hyperparathyroidism, although its accuracy is limited by the operator’s experience. Further limitations of neck US stem from the coexistence of multinodular thyroid disease and from the possible occurrence of multiple adenomas or parathyroid hyperplasia as a cause of primary hyperparathyroidism. In a systematic review of 20,225 cases of primary hyperparathyroidism, the sensitivity of neck US dropped from 78.5 to 34.9% in patients with parathyroid hyperplasia, and to 16.2% in those with double adenoma [15]. Using high-frequency US, sensitivity decreased from 89 to 84% in patients with concomitant primary hyperparathyroidism and multinodular goiter [16]. The inability of neck US to detect most ectopic parathyroid adenomas represents a further limitation. In this scenario, dual-tracer 99mTc-Sestamibi scintigraphy is considered by many authors as a first-line imaging procedure to identify the hyperfunctioning parathyroid gland(s) in patients with primary hyperparathyroidism. This imaging technique is frequently associated with neck US, because the diagnostic accuracy is increased using the two imaging procedures combined [17]. However, the 99mTc-Sestamibi technique has many limitations, mainly related to a low spatial resolution and to the frequently unsatisfactory lesion/background ratio in patients with an autonomously functioning or hyperfunctioning thyroid gland. Detecting small mediastinal adenomas may be also difficult due to the attenuation of the low-energy 99mTc gamma rays by the sternum and the rib cage. Concomitant thyroid or neck pathologic conditions (such as thyroiditis, metastatic lymph nodes, and follicular and Hurthle cell carcinomas) may also cause equivocal results [18]. The detection performance of 99mTc-Sestamibi scintigraphy is particularly disappointing in patients with normocalcemic primary hyperparathyroidism, probably, because, in these patients, size and metabolic activity of the abnormal parathyroid are lower than in hypercalcemic patients [9]. In view of the above considerations, a great interest is kindled on the PET technique [19], which allows significantly higher spatial resolution, better lesion-to-noise ratio, and lower attenuation by rib cage and sternum, because of the higher energy of photons produced by annihilation. Due to these peculiarities, PET can detect lesions with a maximum diameter smaller than 1 cm. Thus, compared with 99mTc-Sestamibi scintigraphy, significant advantages are expected, in preclinical conditions caused by small neoplasms, in the presence of a high thyroid activity, and in ectopic adenomas. Among the many investigated radio-fluorinated compounds, 18F-FCH bears some advantages: first, it does not require an in-house cyclotron to be produced and, second, 18F-FCH is already available in many nuclear medicine departments because of its widespread use in patients with prostate cancer. In a systematic review and meta-analysis on the use of PET tracers for parathyroid localization, Kluijfhout et al. concluded that 18F-FCH-PET may produce more accurate results than [11C] methionine PET [19]. Further support to the use of 18F-FCH-PET derives from the previous demonstrations of its ability to detect not only parathyroid adenomas, but also carcinomas [20] and multiple adenomas, and even gland hyperplasia in patients with secondary hyperparathyroidism.
In the present study, we investigated the diagnostic performance of 18F-FCH-PET/CT in a series of patients with primary hyperparathyroidism, which also included a consistent percentage of the normocalcemic ones. The high frequency of the latter patients, as compared with what reported in the general population, can be explained by the fact that our series is a selected one. Indeed, our Nuclear Medicine Department is the hub of a multicenter hospital mainly devoted to the rehabilitation of patients with neuromotor diseases or with bone injuries resulting from traumas and/or osteoporosis. As a consequence, both calcium and parathyroid hormone measurements are routinely performed. In line with the early stage of the disease, most identified parathyroid-like neck lesions were small in size, their mean (± SD) US volume being 0.6 ± 0.5 mL (range 0.1–1.8 mL). This observation together with the high prevalence (nearly 50%) of concomitant multinodular goiter or chronic autoimmune thyroiditis justifies the poor diagnostic performance of 99mTc-Sestamibi scintigraphy, which was able to identify only a minority of hyperfunctioning parathyroid glands (15%). In this clinical setting, the detection rate of 18F-FCH-PET/CT was impressively high (71%), even when compared with that of neck US (68%). The diagnostic performance of 18F-FCH-PET/CT was even more obvious in patients with normocalcemic hyperparathyroidism, with a detection rate of 69 versus 61% for neck US, and a complete failure of 99mTc-Sestamibi scintigraphy to detect any hyperfunctioning parathyroid gland. Similar results were obtained when patients with a definitely identified parathyroid adenoma either at surgery or at fine needle aspiration cytology/biochemistry were considered. In this subgroup of patients with primary hyperparathyroidism, the estimated sensitivities were 88, 82, and 17% for 18F-FCH-PET/CT, neck US, and 99mTc-Sestamibi scintigraphy, respectively. Our study is the first report about the effectiveness of 18F-FCH-PET/CT in a cohort of patients with normocalcemic hyperparathyroidism, since the previous reports included mainly patients with overt hyperparathyroidism and severe hypercalcemia [13]. The results of this study support the use of this new technique, especially in this subset of patients, since the traditional imaging with 99mTc-Sestamibi has proven ineffective also in previous studies [9]. These data are extremely relevant, because, at present, primary hyperparathyroidism is often diagnosed in an early stage of the disease. Correct identification of the pathologic parathyroid allows an easier surgical approach, thus preventing the progression of these milder cases to overt hyperparathyroidism with its related complications. The row cost of 18F-FCH-PET/CT is of course greater (about 400 euros per patient) compared with that of 99mTc-Sestamibi (about 100 euros per patient). However, indirect costs should also be considered, because 99mTc-Sestamibi requires a longer scanning time and a longer utilization of the dedicated personnel. The cost/effectiveness evaluation also favors 18F-FCH-PET/CT, because of its higher diagnostic performance resulting in a more accurate pre-surgical identification of the affected parathyroid gland.
Our study is the first report about the effectiveness of 18F-FCH-PET/CT in a cohort of patients, which included a consistent number of those with normocalcemic or mild primary hyperparathyroidism, since the previous reports mainly investigated patients with overt hyperparathyroidism and severe hypercalcemia. There are, however, two main limitations: first, the limited number of evaluated patients and, second, the relatively small percentage of those who received surgical or cytological confirmation of the pathologic parathyroid gland. In conclusion, this study shows that 18F-FCH-PET/CT can be considered the first-line investigation to identify pathologic parathyroid glands both in patients with normocalcemic hyperparathyroidism and in the hypercalcemic ones, when the disease is still in its initial stage and size of the abnormal parathyroid gland is small.
References
Bilezikian JP, Khan AA, Potts JT, Hyperthyroidism TIWotMoAP (2009) Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the third international workshop. J Clin Endocrinol Metab 94:335–339. https://doi.org/10.1210/jc.2008-1763
Cusano NE, Maalouf NM, Wang PY, Zhang C, Cremers SC, Haney EM et al (2013) Normocalcemic hyperparathyroidism and hypoparathyroidism in two community-based nonreferral populations. J Clin Endocrinol Metab 98:2734–2741. https://doi.org/10.1210/jc.2013-1300
Lowe H, McMahon DJ, Rubin MR, Bilezikian JP, Silverberg SJ (2007) Normocalcemic primary hyperparathyroidism: further characterization of a new clinical phenotype. J Clin Endocrinol Metab 92:3001–3005. https://doi.org/10.1210/jc.2006-2802
Chen G, Xue Y, Zhang Q, Xue T, Yao J, Huang H et al (2015) Is normocalcemic primary hyperparathyroidism harmful or harmless? J Clin Endocrinol Metab 100:2420–2424. https://doi.org/10.1210/jc.2014-4432
Mariani G, Gulec SA, Rubello D, Boni G, Puccini M, Pelizzo MR et al (2003) Preoperative localization and radioguided parathyroid surgery. J Nucl Med 44:1443–1458
Mariani G, Mazzeo S, Rubello DCB (2015) Preoperative localization of abnormal parathyroid glands. In: Bilezikian JP, Marcus R, Levine MA, Marcocci C, Silverberg SJ, Potts JT Jr (eds) The parathyroids, 3rd edn. Elsevier, Oxfrod
Guidoccio F, Mazzarri SGM, Mazzeo S (2017) Diagnostic applications of nuclear medicine: parathyroid tumors. In: Strauss H, Mariani G, Volterrani D, Larson S (eds) Nuclear oncology. Springer, Berlin
Wade TJ, Yen TW, Amin AL, Wang TS (2012) Surgical management of normocalcemic primary hyperparathyroidism. World J Surg 36:761–766. https://doi.org/10.1007/s00268-012-1438-y
Šiprová H, Fryšák Z, Souček M (2016) Primary hyperparathyroidism, with a focus on management of the normocalcemic form: to treat or not to treat? Endocr Pract 22:294–301. https://doi.org/10.4158/EP15704.OR
Michaud L, Burgess A, Huchet V, Lefèvre M, Tassart M, Ohnona J et al (2014) Is 18F-fluorocholine-positron emission tomography/computerized tomography a new imaging tool for detecting hyperfunctioning parathyroid glands in primary or secondary hyperparathyroidism? J Clin Endocrinol Metab 99:4531–4536. https://doi.org/10.1210/jc.2014-2821
Vorselaars WM, Kluijfhout WP, Vriens MR, van der Pol CC, Borel Rinkes IH, Valk GD et al (2016) Detection of synchronous parathyroid adenoma and breast cancer with (18)F-Fluorocholine PET-CT. Nucl Med Mol Imaging 50:180–182. https://doi.org/10.1007/s13139-015-0357-x
Lezaic L, Rep S, Sever MJ, Kocjan T, Hocevar M, Fettich J (2014) 18F-Fluorocholine PET/CT for localization of hyperfunctioning parathyroid tissue in primary hyperparathyroidism: a pilot study. Eur J Nucl Med Mol Imaging 41:2083–2089. https://doi.org/10.1007/s00259-014-2837-0
Thanseer N, Bhadada SK, Sood A, Mittal BR, Behera A, Gorla AKR et al (2017) Comparative effectiveness of ultrasonography, 99mTc-Sestamibi, and 18F-Fluorocholine PET/CT in detecting parathyroid adenomas in patients with primary hyperparathyroidism. Clin Nucl Med 42:e491–e497. https://doi.org/10.1097/RLU.0000000000001845
Bilezikian JP, Silverberg SJ (2010) Normocalcemic primary hyperparathyroidism. Arq Bras Endocrinol Metabol 54:106–109
Ruda JM, Hollenbeak CS, Stack BC (2005) A systematic review of the diagnosis and treatment of primary hyperparathyroidism from 1995 to 2003. Otolaryngol Head Neck Surg 132:359–372. https://doi.org/10.1016/j.otohns.2004.10.005
Erbil Y, Barbaros U, Yanik BT, Salmaslioğlu A, Tunaci M, Adalet I et al (2006) Impact of gland morphology and concomitant thyroid nodules on preoperative localization of parathyroid adenomas. Laryngoscope 116:580–585. https://doi.org/10.1097/01.MLG.0000203411.53666.AD
Liddy S, Worsley D, Torreggiani W, Feeney J (2017) Preoperative imaging in primary hyperparathyroidism: literature review and recommendations. Can Assoc Radiol J 68:47–55. https://doi.org/10.1016/j.carj.2016.07.004
Vattimo A, Bertelli P, Cintorino M, Burroni L, Volterrani D, Vella A et al (1998) Hürthle cell tumor dwelling in hot thyroid nodules: preoperative detection with technetium-99m-MIBI dual-phase scintigraphy. J Nucl Med 39:822–825
Kluijfhout WP, Pasternak JD, Drake FT, Beninato T, Gosnell JE, Shen WT et al (2016) Use of PET tracers for parathyroid localization: a systematic review and meta-analysis. Langenbecks Arch Surg 401:925–935. https://doi.org/10.1007/s00423-016-1425-0
Deandreis D, Terroir M, Al Ghuzlan A, Berdelou A, Lacroix L, Bidault F et al (2015) 18Fluorocholine PET/CT in parathyroid carcinoma: a new tool for disease staging? Eur J Nucl Med Mol Imaging 42:1941–1942. https://doi.org/10.1007/s00259-015-3130-6
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Irene Bossert declares that she has no conflict of interest. Spyridon Chytiris declares that he has no conflict of interest. Marina Hodolic is Clinical Research Supervisor, Iason, Graz, Austria. Laura Croce declares that she has no conflict of interest. Luigi Mansi declares that he has no conflict of interest. Luca Chiovato declares that he has no conflict of interest. Giuliano Mariani declares that he has no conflict of interest. Giuseppe Trifirò declares that he has no conflict of interest.
Ethical approval
This article does not contain any studies with animals performed by any of the authors. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Bossert, I., Chytiris, S., Hodolic, M. et al. PETC/CT with 18F-Choline localizes hyperfunctioning parathyroid adenomas equally well in normocalcemic hyperparathyroidism as in overt hyperparathyroidism. J Endocrinol Invest 42, 419–426 (2019). https://doi.org/10.1007/s40618-018-0931-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-018-0931-z