
Abstract
Introduction
Intraoperative kinematic analysis using a navigation system in total knee arthroplasty (TKA) has been increasing. The purpose of the present study was to assess the reproducibility of the intraoperative kinematics analysis in TKA using the image-free knee navigation system.
Materials and methods
Fifty-one knees in 45 patients who received TKA, performed by a single surgeon (the senior consultant) with the resident, were included in this retrospective study. There were 7 men and 38 women and the mean age was 74.3 years. Cruciate retaining (CR) type and posterior stabilized (PS) type implants were inserted into 38 and 13 knees. The senior consultant and the resident analyzed initial kinematics, the axial rotation of the tibia and the coronal alignment of the lower limb, three times in each knee on manual passive knee flexion intraoperatively using the navigation system. Intra-class correlation coefficients (ICC) with 95 % confidence intervals were calculated to determine the reproducibility of this analysis.
Results
In regard to intra-rater reproducibility with axial rotation of the tibia, the ICC of the senior consultant was 0.965 for CR knees and 0.972 for PS knees while the ICC of the resident were 0.966 and 0.956. Inter-rater reproducibility was excellent for both knee types (ICC, 0.885 for CR knees and 0.864 for PS knees). In regard to intra-rater reproducibility with coronal alignment of the lower limb, ICC of the senior consultant was 0.990 for CR knees and 0.996 for PS knees while those of the resident were 0.990 and 0.995. Inter-rater reproducibility was also excellent for both knee types (ICC, 0.978 for CR knees and 0.994 for PS knees).
Conclusions
Manual intraoperative kinematic analysis using a navigation system in TKA showed excellent reproducibility. This result may encourage further studies about intraoperative kinematic analysis using a navigation system in TKA.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Total knee arthroplasty (TKA) has become one of the most common and successful orthopedic interventions. Despite favorable long-term implant survival after TKA, as many as 20 % of patients are not satisfied with their improvement [1]. Another study reported that patients undergoing primary TKA seem to have worse clinical outcomes than patients undergoing primary total hip arthroplasty at 1-year follow-up [2]. A previous study indicated that this problem has not been resolved by only using the navigation system [3]. On the other hand, this dissatisfaction could be explained partly by the change of knee kinematics between pre-arthritis and TKA [4–6]. To evaluate kinematics in TKA, various evaluation methods have been reported [7–9]. Particularly, kinematic analysis using a navigation system is advantageous in that it provides intraoperative information with a high accuracy in the measurement of angles and distances [10, 11]. Thus, reports of intraoperative kinematic analysis using a navigation system have been increasing.
However, the reliability of intraoperative kinematic analysis has been questioned because the analysis is done by hand in anesthetized patients. Nevertheless, only a few previous studies have focused on the reliability of intraoperative kinematic analysis using a navigation system [12, 13]. To our knowledge, no study has evaluated intra-rater and inter-rater reproducibility of navigation-based intraoperative kinematic analysis. The aim of this study was to determine the reproducibility of intraoperative kinematics analysis done by hand using a navigation system in TKA.
Materials and methods
After obtaining approval from the institutional review board of our hospital, data from 51 knees in 45 consecutive patients who underwent TKA between March and December 2008 were reviewed. There were 44 female and 9 male patients and their average age was 74.3 years (range 62–84). The average height was 150.9 cm (range 136–165) and the average weight was 58.3 kg (range 45–75). The image-free knee navigation system (Stryker Navigation version 1.0, Kalamazoo, MI, USA) with infrared cameras and light-emitting diodes was used, and the Scorpio NRG (Stryker Orthopaedics, Mahwah, NJ, USA) was implanted in all patients. The cruciate retaining (CR) type implant was inserted into 38 knees while the other 13 received the posterior stabilized (PS) type. All patients provided informed consent for this study.
Surgical procedure
Every surgery was performed using a tourniquet and a standard medial parapatellar approach. Registration of the navigation system was done in each case following the manufacturer’s protocol. The measured resection technique was used for bone resection. The posterior cruciate ligament (PCL) was sacrificed if its tension was insufficient, as it would poorly resist the posteriorly directed shear force on the tibia derived from the extensor mechanism. If a CR type implant was selected, the bony island resection was performed while preserving the PCL. The femoral rotational axis was set parallel to the surgical epicondylar axis, and the tibial rotational alignment was directed along the line from the medial border of the tibial tubercle to the middle of the posterior cruciate ligament [14]. The width of the flexion–extension gap and ligament balance were checked using a spacer block to avoid laxity, and the thickness of the polyethylene insert was determined. The patella was always resurfaced. After releasing the tourniquet, the components of tibia and patella were cemented. Finally, the cementless femoral component was assembled. A single surgeon, the senior consultant, performed all the procedures with the aid of the resident.
Evaluation of intraoperative kinematics
After assembling each component and cementation onto the tibia surface, the capsule was closed with two forceps. In each knee, kinematic analysis was performed three times by the senior consultant and the resident using the navigation system. The knee was flexed by placing the patient’s heel on the examiner’s palm, and the other hand of the examiner was placed beside the patient’s knee for support without the tourniquet. Care was taken to avoid intentional rotation of the knee throughout flexion. The navigation system automatically recorded the rotation angle of the tibia (internal rotation as positive) and coronal alignment of the lower limb (valgus alignment as positive) at 30°, 60°, 90° and 120° during continuous knee passive flexion.
Statistical analysis
All statistical analyses were performed using IBM SPSS statistical software (SPSS v.21.0 for Mac OS X). Intra-class correlation coefficients (ICC) were used to quantify reproducibility for two evaluations. The ICC is a well-established statistical tool for estimating reliability [15]. The ICC (1, 1), as an intra-rater ICC, was calculated from data from three evaluations performed by the senior consultant and the resident. The ICC (2, 1), as an inter-rater ICC, was also calculated from data of the first evaluation with comparison between the two examiners. According to a previous study [16], intra-rater ICC and inter-rater ICC were evaluated for reproducibility. The thresholds for assessment of intra-class correlations as suggested by Landis et al. [17] were used: <0.2, slight correlation; between 0.21 and 0.40, fair correlation; between 0.41 and 0.60, moderate correlation; between 0.61 and 0.80, substantial correlation; >0.81, almost perfect correlation. A threshold of P < 0.05 was considered statistically significant for all statistical analyses.
Results
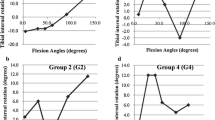
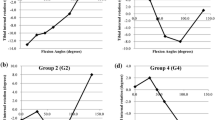
Patient data are summarized in Table 1. The axial rotation angle of the tibia at each angle of knee flexion, in CR knees and PS knees, are shown in Figs. 1 and 2. Both CR and PS knees showed internal rotation during knee flexion. The coronal alignment of the lower limb was slightly valgus during knee flexion (Figs. 3, 4). Each parameter is also summarized in Table 2.

Internal rotation of the tibia during knee flexion in CR knees. Error bars indicate standard deviation

Internal rotation of the tibia during knee flexion in PS knees. Error bars indicate standard deviation

Coronal alignment of the lower limb during knee flexion in CR knees. Error bars indicate standard deviation

Coronal alignment of lower limb during knee flexion in PS knees. Error bars indicate standard deviation
Data of the ICC are given in Table 3. In regard to intra-rater reproducibility with axial rotation of the tibia, the ICC of the senior consultant was 0.965 for CR knees and 0.972 for PS knees, while those of the resident were 0.966 and 0.956, respectively. These results demonstrated almost perfect reproducibility (ICC > 0.81). Inter-rater reproducibility was excellent with both knee types (ICC, 0.885 and 0.864). In regard to intra-rater reproducibility with the coronal alignment of the lower limb, the ICC of the senior consultant was 0.990 for CR knees and 0.996 for PS knees, while those of the resident were 0.990 and 0.995, respectively. Inter-rater reproducibility was also excellent for both knee types (ICC, 0.978 and 0.994).
Both intra- and inter-rater ICC indicated almost perfect reproducibility of the intraoperative kinematic analysis by manual passive knee flexion.
Discussion
The most important finding of the present study was that the reproducibility of intraoperative kinematic analysis using the image-free navigation system is almost perfect. Despite the subjective evaluation by manual flexion, intra- and inter-rater ICC were high in 51 knees.
With the widespread use of a navigation system in TKA, reports of intraoperative kinematic analysis using a navigation system have been increasing. Klein et al. [18] evaluated the effect of two different tibial inserts and reported a significant difference in femoral–tibial rotational motion using a navigation system. Mihalko et al. [19] assessed the change in coronal deformity throughout knee flexion using a navigation system. Ishida et al. [20] divided rotational patterns into four groups and evaluated correlation of preoperative contracture and varus deformity with both pre- and postoperative maximum flexion angles. Matsuzaki et al. [21] measured soft-tissue balance parameters in a navigation system using an offset-type tensor. From the point of view of surgical technique, Baier et al. [22] described a modified gap-balancing technique with navigation of the tibia.
Intraoperative kinematic analysis using a navigation system has been conducted extensively, but few studies have evaluated the reliability of knee kinematics. Some studies demonstrated reliability of kinematics during surgery for anterior cruciate ligament (ACL) injury [23, 24]. However, these studies revealed reliability by assessing the size of standard deviation or performing the Mann–Whitney test, not by examining ICC. In addition, in relation to kinematics in TKA, it has been suggested that the kinematics of the natural knee were not maintained in all respects after arthroplasty using an implant that had equal sized circular femoral condyles, when loaded and moved in vivo [5]. Therefore, an analysis of the reliability of knee kinematics especially in TKA using a navigation system is needed. Although various authors have demonstrated poor intra- and inter-rater reliability, Hauschild et al. [25] described excellent inter- and intra-rater ICC for dynamic monitoring of coronal leg alignment and extension range in TKA using a navigation system in a cadaveric study. Baier et al. [26] assessed the difference in pre- and postoperative in vivo kinematics between CR and PS TKA using a navigation system in passive range of movement. For each patient, the combination of movements was registered three times. An electric leg holder was used rather than hand support. They performed statistical comparisons but did not assess reliability. Use of an electric leg holder might be required to prevent rotation of the lower leg, which would alter the rotational kinematics of the tibia. Nevertheless, it is important that intraoperative kinematic evaluation in TKA using a knee navigation system is commonly done by manual knee flexion. Casino et al. [12] described in vivo kinematic evaluation of knee stability before and after total and unicondylar knee replacement by utilizing navigation. The procedures were conducted by the same surgeon who performed the reconstruction and navigated the acquisitions. The reliability of three repeated motions for each patient was assessed only with intra-rater ICC, but not with the inter-rater ICC. Seon et al. [13] assessed the repeatability of preoperative and postoperative anterior–posterior femoral translation and internal–external rotation of the femur in passive knee flexion by calculating only the intra-rater ICC. They reported that intra-rater ICC in postoperative knees ranged from 0.96 to 0.99 for anterior–posterior femoral translation, and the ICC ranged from 0.96 to 0.98 for internal–external rotation. They pointed out that their study has limitations in that all kinematic measurements were taken by a single surgeon and inter-rater reliability, as reproducibility, was not measured. Our results, including high reproducibility, may support previous studies and encourage future ones about intraoperative kinematics analysis using a navigation system in TKA.
There are several limitations to our study. First, measurements were performed only for internal rotation of the tibia and alignment of the lower limb. There is a lack of kinematic data on anteroposterior, mediolateral and superoinferior dimensions because knee kinematics includes 6 degrees of freedom. However, in previous studies, rotational axis and coronal alignment were mostly used to evaluate knee kinematics. Our data are meaningful for previous and future studies because they were shown to be highly reproducible. Second, although the reproducibility of intraoperative kinematics by manual passive flexion was verified, the relationship between intraoperative kinematics in a passive unloading situation and postoperative kinematics in an active loading situation was not examined. Furthermore, we do not know whether the intraoperative kinematic pattern persists during recovery. It is important to investigate the correlation between postoperative kinematics and intraoperative kinematics to predict postoperative function based on intraoperative evaluation. A solution to overcome this limitation was suggested in a recent study which reported that intraoperative kinematics directly affects postoperative deep knee flexion angle and patient-reported outcomes after TKA. Nishio et al. [27] suggested that patients who showed an intraoperative medial pivot pattern had significantly better outcomes as evaluated by the Knee Society Score. The correlation between not only postoperative kinematics but also postoperative clinical outcomes and intraoperative kinematics should probably be assessed.
Conclusion
Reproducibility of intraoperative kinematic analysis using a knee navigation system in TKA with passive knee flexion by hand was almost perfect. This indicates that intraoperative kinematic analysis has a high reproducibility.
References
Nilsdotter AK, Toksvig-Larsen S, Roos EM (2009) Knee arthroplasty: are patient’s expectations fulfilled? Acta Orthop 80:55–61. doi:10.1080/17453670902805007
Bourne RB, Chesworth B, Davis A et al (2010) Comparing patient outcomes after THA and TKA: is there a difference? Clin Orthop Relat Res 468:542–546. doi:10.1007/s11999-009-1046-9
Singisetti K, Muthumayandi K, Abual-Rub Z, Weir D (2015) Navigation-assisted versus conventional total knee replacement: no difference in patient-reported outcome measures (PROMs) at 1 and 2 years. Arch Orthop Trauma Surg 135:1595–1601. doi:10.1007/s00402-015-2314-7
Bull AMJ, Kessler O, Alam M, Amis AA (2008) Changes in knee kinematics reflect the articular geometry after arthroplasty. Clin Orthop Relat Res 466:2491–2499. doi:10.1007/s11999-008-0440-z
Howell SM (2010) Assessment of the radii of the medial and lateral femoral condyles in varus and valgus knees with osteoarthritis. J Bone Jt Surg 92:98. doi:10.2106/JBJS.H.01566
Eckhoff DG, Bach JM, Spitzer VM et al (2005) Three-dimentional mechanics, kinematics, and morphology of the knee viewed in virtual reality. J Bone Joint Surg Am 87(Suppl 2):71–80. doi:10.2106/JBJS.E.00440
Li G, Suggs J, Hanson G et al (2006) Three-dimensional tibiofemoral articular contact kinematics of a cruciate-retaining total knee arthroplasty. J Bone Joint Surg Am 88:395–402. doi:10.2106/JBJS.D.03028
Hanson GR, Suggs JF, Freiberg AA et al (2006) Investigation of in vivo 6DOF total knee arthoplasty kinematics using a dual orthogonal fluoroscopic system. J Orthop Res 24:974–981. doi:10.1002/jor.20141
Jung M-C, Chung JY, Son K-H et al (2014) Difference in knee rotation between total and unicompartmental knee arthroplasties during stair climbing. Knee Surg Sports Traumatol Arthrosc 22:1879–1886. doi:10.1007/s00167-014-3064-8
Ballas R, Philippot R, Cartier J-L et al (2013) Computer-assisted total knee arthroplasty: impact of the surgeon’s experience on the component placement. Arch Orthop Trauma Surg 133:397–403. doi:10.1007/s00402-012-1666-5
Bin Abd Razak HR, Pang HN, Yeo SJ et al (2013) Joint line changes in cruciate-retaining versus posterior-stabilized computer-navigated total knee arthroplasty. Arch Orthop Trauma Surg 133:853–859. doi:10.1007/s00402-013-1738-1
Casino D, Martelli S, Zaffagnini S et al (2009) Knee stability before and after total and unicondylar knee replacement: in vivo kinematic evaluation utilizing navigation. J Orthop Res 27:202–207. doi:10.1002/jor.20746
Seon JK, Park JK, Jeong MS et al (2011) Correlation between preoperative and postoperative knee kinematics in total knee arthroplasty using cruciate retaining designs. Int Orthop 35:515–520. doi:10.1007/s00264-010-1029-1
Akagi M, Mori S, Nishimura S et al (2005) Variability of extraarticular tibial rotation references for total knee arthroplasty. Clin Orthop Relat Res 436:172–176
Shrout PE, Fleiss JL (1979) Intraclass correlations: uses in assessing rater reliability. Psychol Bull 86:420–428
Bartlett JW, Frost C (2008) Reliability, repeatability and reproducibility: analysis of measurement errors in continuous variables. Ultrasound Obstet Gynecol 31:466–475. doi:10.1002/uog.5256
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Klein GR, Parvizi J, Rapuri VR et al (2004) The effect of tibial polyethylene insert design on range of motion: evaluation of in vivo knee kinematics by a computerized navigation system during total knee arthroplasty. J Arthroplasty 19:986–991. doi:10.1016/j.arth.2004.07.002
Mihalko WM, Ali M, Phillips MJ et al (2008) Passive knee kinematics before and after total knee arthroplasty: are we correcting pathologic motion? J Arthroplast 23:57–60. doi:10.1016/j.arth.2006.12.048
Ishida K, Shibanuma N, Matsumoto T et al (2015) Factors affecting intraoperative kinematic patterns and flexion angles in navigated total knee arthroplasty. Knee Surg, Sport Traumatol Arthrosc. doi:10.1007/s00167-015-3572-1
Matsuzaki T, Matsumoto T, Kubo S et al (2014) Tibial internal rotation is affected by lateral laxity in cruciate-retaining total knee arthroplasty: an intraoperative kinematic study using a navigation system and offset-type tensor. Knee Surg Sports Traumatol Arthrosc 22:615–620. doi:10.1007/s00167-013-2627-4
Baier C, Fitz W, Craiovan B et al (2014) Improved kinematics of total knee replacement following partially navigated modified gap-balancing technique. Int Orthop 38:243–249. doi:10.1007/s00264-013-2140-x
Martelli S, Lopomo N, Bignozzi S et al (2007) Validation of a new protocol for navigated intraoperative assessment of knee kinematics. Comput Biol Med 37:872–878. doi:10.1016/j.compbiomed.2006.09.004
Zaffagnini S, Bignozzi S, Martelli S et al (2006) New intraoperative protocol for kinematic evaluation of ACL reconstruction: preliminary results. Knee Surg, Sport Traumatol Arthrosc 14:811–816. doi:10.1007/s00167-006-0057-2
Hauschild O, Konstantinidis L, Strohm PC et al (2009) Reliability of leg alignment using the OrthoPilot system depends on knee position: a cadaveric study. Knee Surg, Sport Traumatol Arthrosc 17:1143–1151. doi:10.1007/s00167-009-0825-x
Baier C, Springorum H-R, Götz J et al (2013) Comparing navigation-based in vivo knee kinematics pre- and postoperatively between a cruciate-retaining and a cruciate-substituting implant. Int Orthop 37:407–414. doi:10.1007/s00264-013-1798-4
Nishio Y, Onodera T, Kasahara Y et al (2014) Intraoperative medial pivot affects deep knee flexion angle and patient-reported outcomes after total knee arthroplasty. J Arthroplast 29:702–706. doi:10.1016/j.arth.2013.06.035
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Wada, K., Mikami, H., Hamada, D. et al. Measurement of rotational and coronal alignment in total knee arthroplasty using a navigation system is reproducible. Arch Orthop Trauma Surg 136, 271–276 (2016). https://doi.org/10.1007/s00402-015-2402-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-015-2402-8