
Abstract
Introduction
The treatment of adult non-traumatic avascular necrosis of the femoral head (AVN; N-ANFH) within an estimated incidence of 5000–7000 cases per annum in Germany remains a challenge. Risk factors include steroids, alcohol abuse, chemotherapy and immunosuppressive medication, but a genetic predisposition has been suggested. Early diagnosis of this often bilateral disease process is essential for successful conservative or joint preserving surgical management. In this review, we present the update German consensus S3 guideline “diagnosis and management for N-ANFH” as a concise summary.
Materials and methods
This systematic review is based on the published literature from January 1, 1970 to April 31, 2013 (German and English language). Inclusion criteria were systematic reviews, meta-analyses and relevant peer review publications. We identified a total of 3715 related publications, of which 422 were suitable according to the SIGN criteria, but only 159 fulfilled our inclusion criteria.
Results and conclusions
Clinical suspicion of N-ANFH mandates radiographic evaluation. If radiographs are normal MRI scans are recommended, which should be evaluated according to the ARCO-classification. Differential diagnoses include transient osteoporosis, bone bruise, insufficiency fracture and destructive arthropathy. Untreated, subchondral fractures commonly occur within 2 years, during which the risk for contralateral involvement is high—thereafter unlikely. Conservative management with Ilomedin and Alendronat can be tried, but other pharmacological or physical treatments are inappropriate. No specific joint preserving procedure can be recommended, but core decompression should be considered in early stages if necrosis is <30 %. In ARCO stages IIIc or IV total hip arthroplasty (THA) should be contemplated, which offers similar outcome compared to osteoarthritis. Young age is the main risk factor for higher revision rates after THA for N-ANFH.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
Non-traumatic avascular necrosis of the femoral head (N-ANFH) usually affects adults of young/middle age and occurs bilaterally. An increasing incidence of idiopathic cases has been reported, but steroid and immunosuppression therapy (e.g., transplant patients), alcohol misuse and chemotherapy remain important causes. Early diagnosis is essential to allow for joint preserving surgical management attempts. Femoral head collapse commonly occurs within 2 years after onset and necessitates total hip arthroplasty (THA).
The German S3 guidelines have been developed under the patronage of the German society for Orthopaedics and Traumatology (DGOOC) and the German societies of Radiology (DRG), of Physical Therapy and Rehabilitation (DGPMR) and Osteology (DVO). The up to date evidence was reviewed in 2013 in order to establish the current status of diagnosis and management of N-ANFH, both in terms of conservative/pharmacological and stage-dependent surgical management.
The purpose of this review to provide a concise summary of the originally in German published S3 guidelines in English to reach a wider readership. The full length S3 guidelines from 2014 (http://www.awmf.org/leitlinien/detail/ll/033-050.html) give 38 evidence based recommendations, some of which have already published in German sub-specialty journals [1–4].
Materials and methods
An extensive literature search of all topic relevant and related published articles was carried out using internet sites of the AWMF (“Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften e.V.” or Association of the Scientific Medical Societies in Germany) [5], the “National Guideline Clearinghouse” and the “Guidelines International Network”, a further systematic literature search was done using the data bases of the US National Library of Medicine National Institutes of Health (http://www.ncbi.nlm.nih.gov/pubmed) and the Cochrane Library (www.cochranelibrary.com). The following keywords were used “Femur Head Necrosis” [Majr:NoExp] NOT “Legg-Perthes Disease” [Mesh] capturing the period from January 1, 1970 to May 31, 2013.
-
The inclusion and exclusion criteria are presented in Table 1.
Table 1 Inclusion and exclusion literature search criteria (search period Jan 1, 1970–May 31, 2013) -
A limitation to randomised studies was not feasible due to the lack of sufficient numbers and hence per reviewed publications of lower evidence level had to be included.
-
The level of evidence (LoE) as defined by the Scottish Intercollegiate Guidelines Network (SIGN) [6] was applied.
-
Furthermore clinical relevance, study endpoints, clinical applicability, patient preference and ethics and economic aspects were evaluated.
-
For the expert consensus based recommendations (ER) the AMFW Grading System [AWMF 2012] was used: “A = must”, “B = should”, “0 = may”.
-
The strength of participating expert consensus (EC) was judged as “strong” (agreement >95 %) and “medium” (agreement 75–95 %).
-
In cases of discrepancies between LoE and recommendation grade the specific reasons were stated in the original S3 guideline (http://www.awmf.org/leitlinien/detail/ll/033-050.html).
Results
The search revealed a total of 3715 articles (1606 prior to 1991 and 2109 from 1991 to May 31, 2013), of which 422 were pre-selected. Based on the criteria set out in Table 1, a total of 159 articles (43 in relation to national history and conservative management, 72 in relation to diagnosis/imaging and 64 in relation to operative intervention) were included for detailed evaluation.
The relevant findings and conclusions are presented on a point-by-point basis with the respective level of evidence (LoE) and recommendation grade (EC). Relevant important literature is quoted where necessary.
Diagnosis of N-ANFH: imaging
Conclusions
-
In cases of clinical suspicion (groin pain and/or around hip/thigh >6 weeks, underlying known risk factors, antalgic limp, painful restriction of movement, absence of other cause/diagnosis) radiographs (pelvis ap and lateral hip/Lauenstein view) should be obtained (EC “strong”) [7–20].
-
Radiographic grading using the ARCO classification is recommended (EC “medium”) [21–32]*.
-
If radiographs are normal and symptoms persist an MRI scan of both hips due to potential bilateral disease should be requested (LoE 2++, ER B, EC “strong”) [15, 16, 18, 33–39].
-
In radiographic stages ARCO 2 and 3 MRI scans are also recommended to determine area and extent of necrosis and to exclude/confirm subchondral fracture and collapse (LoE 2-3, ER B, EC “strong”) [21, 29, 40–51].
-
In stage ARCO 2 a CT scan will aid to clarify the presence/extent of subchondral fracture if the MRI is inconclusive (LoE 2++, ER B. EC “strong”) [7, 52].
-
Bone scanning is not indicated (LoE 2++, ER 0, EC “strong”) [49–51].
-
The algorithm (Fig. 1) proposed by Reppenhagen et al. (2007) is recommended to allow for timely and stage-dependent diagnostic assessment when suspecting N-ANFH (EC “strong”) [53].
Fig. 1 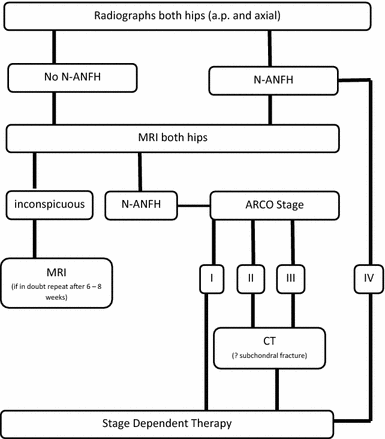
Stage-dependent use of imaging techniques in clinical suspicion of N-ANFH (according Reppenhagen [53])

Supporting evidence and further comments
*The ARCO classification [54] as outlined in Table 2 is based on the grading systems proposed by Ficat and Arlet [22], Steinberg et al. [24, 25] and also Ohzono et al. [27]. The original ARCO grading is primarily based on radiographs. Both MRI and CT scanning are helpful to better differentiate between stage 2 and 3 (“crescent”) sign, establish extent of necrosis and allow a more pragmatic and clinically relevant approach. Stage 0 has become obsolete as not clinically relevant.
Diagnostic challenges/differential diagnoses
-
Transient osteoporosis of the hip (TOH) is an important differential diagnosis (DD). A diffuse oedema pattern on MRI may be seen in both entities, but a more patchy pattern and the absence of focal defects and subchondral changes is suggestive of TOH (EC “medium”) [55–69].
-
As other DD stress-/insufficiency fractures, osteonecrosis and destructive arthropathies should be considered (EC “medium”) [70–78].
Natural history/untreated N-ANFH and risk factors
-
N-ANFH is a progressive disease and subchondral fractures and collapse femoral head usually occurs within 2 years, hence making hip joint preserving surgical intervention impossible. This is particularly the case in patients with bilateral involvement and uncontrollable factors/causes (LoE 2+/2++, EC “strong”) [36, 37, 39, 79–82].
-
After diagnosis of unilateral N-ANFH the risk of contralateral N-ANFH is high within the first 2 years, but diminishes thereafter (LoE 2+/2++, EC “strong”) [41, 44, 45, 82, 83].
Conservative management
-
Conservative treatment of N-ANFH alone does not provide prolonged symptomatic relief and does not prevent disease progression (LoE 2+/2++, EC “strong”) [79, 84].
-
Pharmacological vasodilation with the prostacyclin analogon Iloprost can be considered in ARCO stages 1–2 for reduction of pain and bone marrow oedema in patients where surgical intervention is contraindicated or declined. Administration of Iloprost is considered as off-label use and inappropriate when a subchondral fracture has already occurred (LoE 2+, ER 0, EC “strong”) [85–89].
-
Bisphosphonates (Alendronate) with their bone resorption inhibitive properties have been shown to delay structural femoral head damage/collapse and to reduce levels of pain (LoE 2+, ER 0, EC “medium”) [36, 90–95].
-
There is insufficient evidence to support the use of anticoagulant drugs (LMWH, Warfarin) and are hence not recommended (LoE 2+, ER A, EC “strong”) [96, 97].
-
Statines do not reduce the risk for N-ANFH and are hence not recommended (LoE 2+, ER A, EC “strong”) [98, 99].
-
Hyperbaric oxygen therapy (HBO) has been shown to improve tissue oxygenation, reduces oedema, induces angiogenesis and reduces intraosseous hypertension with improved microcirculation, but no evidence is available to show that femoral head collapse can be delayed. Currently the use of HBO is not recommended (LoE 2+, ER B, EC “strong”) [85, 100–102].
-
There is no evidence to support that extracorporeal shock wave therapy (ESWT) and ultrasound may delay femoral head collapse and are hence not recommended (LoE 1, ER B, EC “strong”) [85, 103–107].
-
Electrostimulation and pulsating electromagnetic fields (PEMF) may improve symptoms in early disease, but no evidence is available to show that femoral head collapse can be delayed. Their use in the treatment of N-ANFH is not recommended (LoE 2+, ER B, EC “strong”) [108–114].
Joint preserving operative interventions: timing, rationale and indications
-
The evidence suggests that joint preserving operative procedures can be offered/tried in ARCO stage 1–3 (LoE: 2+, EC “strong”).
-
No specific procedure can be identified as being superior. The type of surgery depends on the extent of femoral head involvement/necrosis (LoE: 2++, EC “strong”) [45, 115–119].
-
Core decompression is indicated and should be offered in early and potential reversible stages of N-ANFH, i.e. ARCO 1, but also stage ARCO 2 (irreversible early stage) if the area of necrosis is medial or central and <30 %.(LoE 2++, ER A, EC “strong”).
-
In ARCO 3 with infraction of the femoral head core decompression may be considered for short term symptomatic relief (LoE 2++, ER 0, EC “strong”) [36, 38, 79, 84, 88, 105, 108, 114, 120–126].
-
Additional electric stimulation (in combination with core decompression) may improve pain, but does not improve radiographic outcome (LoE 2+, EC “strong”) [108, 112, 113, 127–129].
-
Core decompression plus systemic Alendronate (off-label use) may reduce pain and disease progression compared to core decompression alone (LoE 2+, ER O, EC “medium”) [95].
-
Core decompression plus bone grafting is not superior to core decompression alone, but both are superior to conservative management. [45, 123, 130–134]. Core decompression should only be offered if the area of necrosis is <20 % and if the Kerboul angle is <200° (LoE: 2+, ER B, EC “strong”).
-
Vascularised fibular transplant/graft is technically demanding and is not recommended as a routine procedure and variable outcomes have been reported with small and larger defect/necrosis sizes. It may be offered in specialised treatment centres in younger patients with ARCO 1 and 2 (LoE 2+, ER B, EC “strong”) [122, 135–144].
-
Osteochondral allografts cannot be recommended, as the outcome is not yet clear (LoE 3, ER B, EC “strong”) [145].
-
Autogenous cancellous bone grafting cannot be recommended, as the outcome is not yet clear (LoE 2+, ER B, EC “strong”) [85, 130, 132].
-
Corrective femoral osteotomies are accepted, but technically extremely demanding procedures and should only be considered/offered for younger patients in specialised treatment centres in early disease (LoE 2++, ER B, EC “strong”) [125, 146, 147].
-
There is no scientific evidence for efficacy of Tantalum-implants and the avascular necrosis rod, which are not recommended (LoE 2+, ER B, EC “strong”) [148, 149].
-
In stage ARCO 3c and 4, core decompression is not indicated and total hip replacement (THR) should be discussed (LoE 2++, ER B, EC “strong”) [36, 38, 79].
Total hip replacement: outcome and implant fixation
Results after primary THR and risk factors for revision
-
Revision rates after THR for N-ANFH have significantly fallen since 1990 and are now similar to global failure rates reported nationally [122, 150–152].
-
The short-, medium- and long-term results after THR for N-ANFH are comparable to outcome after THR for osteoarthritis [154–165].
-
THR after preceding procedures, i.e., fibular graft and osteotomies, maybe more complex [153].
-
All types and stages of femoral head necrosis can be treated successfully with THR, but less favourable clinical outcome has to be expected in alcohol or steroid related N-ANFH [153–156].
-
The main risk factor for premature failure and re-operation/implant revision is the young patient age. The revision risk also seems to depend on the underlying aetiology: higher failure rates occur with sickle cell disease, Gauchers disease, renal failure or in patients after renal transplant surgery (LoE: 2+ to 2++, EC “strong”) [153–156].
Prothesis type/mode of fixation
-
Similar outcome can be expected after implantation of cemented and uncemented THR, both of which are recommended as the gold standard (LoE 2+ to 2++, ER B, EC “strong”) [153, 158, 160, 164, 165].
-
Hip resurfacing in younger men (<55 years) can be considered if femoral head quality is adequate for implant fixation. Metal ion wear related complications must be discussed (LoE 2+ to 2++, ER 0, EC “strong”) [159, 160].
-
No sufficient evidence currently exists to support recommendation of short femoral stem designs [153].
References
Bohndorf K, Beckmann J, Jäger M et al (2015) S3-Leitlinie. Teil 3: atraumatische Femurkopfnekrose des Erwachsenen—Diagnose und Differentialdiagnose. Z Orthop Unfall 153:375–386
Roth A, Beckmann J, Smolenski U et al (2015) S3-Leitlinie. Teil 2: atraumatische Femurkopfnekrose des Erwachsenen—unbehandelter Verlauf und konservative Behandlung. Z Orthop Unfallchir 153:488–497
Maus U, Roth A, Tingart M et al (2015) S3-Leitlinie. Teil 3: atraumatische Femurkopfnekrose des Erwachsenen—Operative Therapie der atraumatischen Femurkopfnekrose des Erwachsenen. Z Orthop Unfallchir 153:498–507
Beckmann J, Roth A, Niethard C et al (2015) Knochenmarködem und atraumatische Femurkopfnekrose: Therapie. Orthopäde 153:488–497
German Association of the Scientific Medical Societies (AWMF) Standing Guidelines Commission (2012) AWMF guidance manual and rules for guideline development, 1st edn. English version. http://www.awmf.org/leitlinien/awmf-regelwerk.html. Accessed 15 Sept 2015
Scottish Intercollegiate Guidelines Network (SIGN). SIGN 50: a guideline developer’s handbook. Edinburgh: SIGN; 2014. (SIGN publication no. 50). [October 2014]. http://www.sign.ac.uk. Accessed 15 Sept 2015
Meier R, Kraus TM, Schaeffeler C et al (2014) Bone marrow oedema on MR imaging indicates ARCO stage 3 disease in patients with AVN of the femoral head. Eur Radiol 24:2271–2278
Mitchell DG (1989) Using MR imaging to probe the pathophysiology of osteonecrosis. Radiology 71:25–26
Markisz JA, Knowles RJ, Altchek DW et al (1987) Segmental patterns of avascular necrosis of the femoral heads: early detection with MR imaging. Radiology 162:717–720
Beltran J, Burk JM, Herman LJ et al (1987) Avascular necrosis of the femoral head: early MRI detection and radiological correlation. Magn Reson Imaging 5:431–442
Beltran J, Herman LJ, Burk JM et al (1988) Femoral head avascular necrosis: MR imaging with clinical-pathologic and radionuclide correlation. Radiology 166:215–220
Bassett LW, Gold RH, Reicher M et al (1987) Magnetic resonance imaging in the early diagnosis of ischemic necrosis of the femoral head. Preliminary results. Clin Orthop Relat Res 214:237–248
Robinson HJ Jr, Hartleben PD, Lund G et al (1989) Evaluation of magnetic resonance im aging in the diagnosis of osteonecrosis of the femoral head. Accuracy compared with radiographs, core biopsy, and intraosseous pressure measurements. J Bone Joint Surg Am 71:650–663
Grimm J, Hopf C, Higer HP (1989) Die Femurkopfnekrose. Diagnostik und morphologische Analyse mittels Röntgen, Szintigraphie, Computertomographie und Magnetresonanztomographie. Z Orthop 127:680–690
Kopecky KK, Braunstein EM, Brandt KD (1991) Apparent avascular necrosis of the hip: appearance and spontaneous resolution of MR findings in renal allograft recipients. Radiology 179:523–527
Fordyce MJ, Solomon L (1993) Early detection of avascular necrosis of the femoral head by MRI. J Bone Joint Surg Br 75:365–367
Coleman BG, Kressel HY, Dalinka MK, Scheibler ML, Burk DL, Cohen EK (1988) Radiographically negative avascular necrosis: detection with MR imaging. Radiology 168:525–528
Stulberg BN, Bauer TW, Belhobek GH et al (1989) A diagnostic algorithm for osteonecrosis of the femoral head. Clin Orthop Relat Res 249:176–182
Seiler JG 3rd, Christie MJ, Homra L (1989) Correlation of the findings of magnetic resonance imaging with those of bone biopsy in patients who have stage-I or II ischemic necrosis of the femoral head. J Bone Joint Surg Am 71:28–32
Talamo G, Angtuaco E, Walker RC et al (2005) Avascular necrosis of femoral and/or humeral heads in multiple myeloma: results of a prospective study of patients treated with dexamethasone-based regimens and high-dose chemotherapy. J Clin Oncol 23:5217–5223
Mont MA, Marulanda GA, Jones LC et al (2006) Systematic analysis of classification systems for osteonecrosis of the femoral head. J Bone Joint Surg Am 88(Suppl 3):16–26
Arlet J, Ficat RP (1964) Forage-biopsie de la tête femorale dans I’osteonecrose primative. Observations histo-pathologiques portant sur huit forages. Rev Rhum 31:257–264
Ficat RP (1985) Idiopathic bone necrosis of the femoral head: early diagnosis and treatment. J Bone Joint Surg Br 67:3–9
Marcus ND, Enneking WF, Massam RA (1973) The silent hip in idiopathic aseptic necrosis. Treatment by bone-grafting. J Bone Joint Surg Am 55:1351–1366
Steinberg ME, Hayken GD, Steinberg DR (1984) A new method for evaluation and staging of avascular necrosis of the femoral head. In: Arlet J, Ficat RP, Hungerford DS (eds) Bone circulation. Williams and Wilkins, Baltimore, pp 398–403
Steinberg ME, Hayken GD, Steinberg DR (1995) A quantitative system for staging avascular necrosis. J Bone Joint Surg Br 77:34–41
Ohzono K, Saito M, Takaoka K et al (1991) Natural history of nontraumatic avascular necrosis of the femoral head. J Bone Joint Surg Br 73:68–72
Lee GC, Steinberg ME (2012) Are we evaluating osteonecrosis adequately? Int Orthop 36:2433–2439
Zibis AH, Karantanas AH, Roidis NT et al (2007) The role of MR imaging in staging femoral head osteonecrosis. Eur J Radiol 63:3–9
Smith SW, Meyer RA, Connor PM et al (1996) Interobserver reliability and intraobserver reproducibility of the modified Ficat classification system of osteonecrosis of the femoral head. J Bone Joint Surg Am 78:1702–1706
Schmitt-Sody M, Kirchhoff C, Mayer W et al (2008) Avascular necrosis of the femoral head: inter- and intraobserver variations of Ficat and ARCO classifications. Int Orthop 32:283–287
Jawad MU, Haleem AA, Scully SP (2012) In brief: Ficat classification: avascular necrosis of the femoral head. Clin Orthop Relat Res 470:2636–2639
Stulberg BN, Levine M, Bauer TW et al (1989) Multimodality approach to osteonecrosis of the femoral head. Clin Orthop Relat Res 240:181–193
Lee MS, Chang YH, Chao EK et al (2002) Conditions before collapse of the contralateral hip in osteonecrosis of the femoral head. Chang Gung Med J 25:228–237
Piyakunmala K, Sangkomkamhang T, Chareonchonvanitch K (2009) Is magnetic resonance imaging necessary for normal plain radiography evaluation of contralateral non-traumatic asymptomatic femoral head in high osteonecrosis risk patient. J Med Assoc Thai 92(Suppl 6):147–151
Koo KH, Kim R, Ko GH et al (1995) Preventing collapse in early osteonecrosis of the femoral head. A randomised clinical trial of core decompression. J Bone Joint Surg Br 77:870–874
Mont MA, Hungerford DS (1995) Non-traumatic avascular necrosis of the femoral head. J Bone Joint Surg Am 77:459–474
Stulberg BN, Davis AW, Bauer TW et al (1991) Osteonecrosis of the femoral head. A prospective randomized treatment protocol. Clin Orthop Relat Res 268:140–151
Hungerford DS, Zizic TM (1980) II. The treatment of ischemic necrosis of bone in systemic lupus erythematosus. Med Baltim 59:143–148
Malizos KN, Siafakas MS, Fotiadis DI et al (2001) An MRI-based semiautomated volumetric quantification of hip osteonecrosis. Skelet Radiol 30:686–693
Ha YC, Jung WH, Kim JR et al (2006) Prediction of collapse in femoral head osteonecrosis: a modified Kerboul method with use of magnetic resonance images. J Bone Joint Surg Am 88:35–40
Sakai T, Sugano N, Nishii T et al (2008) Extent of osteonecrosis on MRI predicts humeral head collapse. Clin Orthop Relat Res 466:1074–1080
Ito H, Matsuno T, Kaneda K (1999) Prognosis of early stage avascular necrosis of the femoral head. Clin Orthop Relat Res 358:149–157
Mont MA, Zywiel MG, Marker DR et al (2010) The natural history of untreated asymptomatic osteonecrosis of the femoral head. J Bone Joint Surg Am 92:2165–2170
Lieberman JR, Engstrom SM, Meneghini RM et al (2012) Which factors influence preservation of the osteonecrotic femoral head? Clin Orthop Relat Res 470:525–534
Bassounas AE, Karantanas AH, Fotiadis DI et al (2007) Femoral head osteonecrosis: volumetric MRI assessment and outcome. Eur J Radiol 63:10–15
Liu B, Yi H, Zhang Z et al (2012) Association of hip joint effusion volume with early osteonecrosis of the femoral head. Hip Int 22:179–183
Potter HG, Schachar J (2010) High resolution noncontrast MRI of the hip. J Magn Reson Imaging 31:268–278
Whitehouse R, Bohndorf K (2013) Nekrosen am Skelett. In: Bohndorf K, Imhoff H, Wörtler K (eds) Radiologische Diagnostik der Knochen und Gelenke. Thieme Verlag 3. Auflage
Hofmann S, Kramer J, Plenk H Jr (2002) Die Osteonekrose des Hüftgelenkes im Erwachsenenalter. Radiologe 42:440–450
Mont MA, Ulrich SD, Seyler TM et al (2008) Bone scanning of limited value for diagnosis of symptomatic oligofocal and multifocal osteonecrosis. J Rheumatol 35:1629–1634
Stevens K, Tao C, Lee SU et al (2003) Subchondral fractures in osteonecrosis of the femoral head: comparison of radiography, CT, and MR imaging. AJR Am J Roentgenol 180:363–368
Reppenhagen S, Kenn W, Reichert J (2007) Bildgebung der aseptischen Femurkopfnekrose des Erwachsenen. Orthopäde 36:436–440
Gardeniers JVM (1993) Report of the committee of staging and nomenclature. ARCO news 5:79–82
Turner DA, Templeton AC, Selzer PM et al (1989) Femoral capital osteonecrosis: MR finding of diffuse marrow abnormalities without focal lesions. Radiology 171:135–140
Mitchell MD, Kundel HL, Steinberg ME et al (1986) Avascular necrosis of the hip: comparison of MR, CT, and scintigraphy. AJR Am J Roentgenol 147:67–71
Solomon L (1993) Bone-marrow oedema syndrome. J Bone Joint Surg Br 75:175–176
Hofmann S, Kramer J, Schneider W et al (1997) Transient osteoporosis may represent a reversible early form of avascular necrosis of the hip joint. Curr Orthop 11:164–172
Iida S, Harada Y, Shimizu K et al (2000) Correlation between bone marrow edema and collapse of the femoral head in steroid-induced osteonecrosis. AJR Am J Roentgenol 174:735–743
Kim YM, Oh HC, Kim HJ (2000) The pattern of bone marrow oedema on MRI in osteonecrosis of the femoral head. J Bone Joint Surg Br 82:837–841
Yamamoto T, Kubo T, Hirasawa Y et al (1999) A clinicopathologic study of transient osteoporosis of the hip. Skelet Radiol 28:621–627
McCarthy EF (1998) The pathology of transient regional osteoporosis. Iowa Orthop J 18:35–42
Bohndorf K (2013) Transiente Osteoporose - transientes Knochenmarködem. In: Bohndorf K, Imhoff H, Wörtler K (eds) Radiologische Diagnostik der Knochen und Gelenke. Thieme Verlag 3. Auflage
Fujioka M, Kubo T, Nakamura F et al (2001) Initial changes of non-traumatic osteonecrosis of femoral head in fat suppression images: bone marrow edema was not found before the appearance of band patterns. Magn Reson Imaging 19:985–991
Vande Berg BE, Malghem JJ et al (1992) Avascular necrosis of the hip: comparison of contrast-enhanced and nonenhanced MR imaging with histologic correlation. Radiology 182:445–450
Kubo T, Yamamoto T, Inoue S et al (2000) Histological findings of bone marrow edema pattern on MRI in osteonecrosis of the femoral head. J Orthop Sci 5:520–523
Ito H, Matsuno T, Minami A (2006) Relationship between bone marrow edema and development of symptoms in patients with osteonecrosis of the femoral head. AJR Am J Roentgenol 186:1761–1770
Radke S, Kenn W, Eulert J (2004) Transient bone marrow edema syndrome progressing to avascular necrosis of the hip—a case report and review of the literature. Clin Rheumatol 23:83–88
Emad Y, Ragab Y, El-Shaarawy N et al (2012) Transient osteoporosis of the hip, complete resolution after treatment with alendronate as observed by MRI description of eight cases and review of the literature. Clin Rheumatol 31:1641–1647
Visuri T (1997) Stress osteopathy of the femoral head—10 military recruits followed for 5–11 years. Acta Orthop Scand 68:138–141
Yamamoto T, Schneider R, Bullough PG (2000) Insufficiency subchondral fracture of the femoral head. Am J Surg Pathol 24:464–468
Davies M, Cassar-Pucillino V, Darby A (2004) Subchondral insufficiency fractures of the femoral head. Eur Radiol 14:201–207
Sugano N, Atsumi T, Ohzono K et al (2002) The 2001 revised criteria for diagnosis, classification, and staging of idiopathic osteonecrosis of the femoral head. J Orthop Sci 7:601–605
Mitrovic DR, Riera H (1992) Synovial, articular cartilage, and bone changes in rapidly destructive arthropathy (osteoarthritis) of the hip. Rheumatol Int 12:17–22
Watanabe W, Itoi E, Yamada S (2002) Early MRI findings of rapidly destructive coxarthrosis. Skelet Radiol 31:35–38
Yamamoto T, Bullough PG (2000) The role of subchondral insufficiency fracture in rapid destruction of the hip joint: a preliminary report. Arthr Rheum 43:2423–2427
Yang JH, Oh KJ, Pandher DS (2011) Hydroxyapatite crystal deposition causing rapidly destructive arthropathy of the hip joint. Indian J Orthop 45:569–572
Ilardi SF, Sokoloff L (1984) Secondary osteonecrosis in osteoarthritis of the femoral head. Hum Pathol 15:79–83
Castro FP, Barrack RL (2000) Core decompression and conservative treatment for avascular necrosis of the femoral head: a meta-analysis. Am J Orthop 29:187–194
Stulberg BN, Davis AW, Bauer TW et al (1991) Osteonecrosis of the femoral head. A prospective randomized treatment protocol. Clin Orthop Relat Re. 268:140–151
Steinberg ME, Hayken GD, Steinberg DR (1984) The “conservative” management of avascular necrosis of the femoral head. In: Arlet J, Ficat RP, Hungerford DS (eds) Bone circulation. Williams and Wilkins, Baltimore, pp 334–337
Hofmann S, Mazieres B (2000) Osteonekrose: Natürlicher Verlauf und konservative Therapie. Orthopäde 29:403–410
Tervonen O, Mueller DM, Matteson EL et al (1992) Clinically occult avascular necrosis of the hip: prevalence in an asymptomatic population at risk. Radiology 182:845–847
Neumayr LD, Aguilar C, Earles AN et al (2006) Physical therapy alone compared with core decompression and physical therapy for femoral head osteonecrosis in sickle cell disease. Results of a multicenter study at a mean of three years after treatment. J Bone Joint Surg Am 88:2573–2582
Jäger M, Werner A, Lentrodt S et al (2004) Schmerztherapie bei nichtjuvenilen, aseptischen Osteonekrosen. Schmerz 18:481–491
Tarner IH, Dinser R, Müller-Landner U (2007) Pharmakotherapeutische Aspekte der Femurkopfnekrose. Orthopäde 36:446–450
Disch AC, Matziolis G, Perka C (2005) The management of necrosis-associated and idiopathic bone-marrow oedema of the proximal femur by intravenous iloprost. J Bone Joint Surg Br 87:560–564
Aigner N, Petje G, Schneider W (2005) Bone marrow edema syndrome of the femoral head: treatment with the prostacyclin analogue iloprost vs. core decompression: an MRI-controlled study. Wien Klin Wochenschr 117:130–135
Meizer R, Radda C, Stolz G et al (2005) MRI-controlled analysis of 104 patients with painful bone marrow edema in different joint localizations treated with the prostacyclin analogue iloprost. Wien Klin Wochenschr 117:278–286
Jergesen HE, Khan AS (1997) The natural history of untreated asymptomatic hips inpatients who have non-traumatic osteonecrosis. J Bone Joint Surg Am 79:359–363
Agarwala S, Jain D, Joshi VR et al (2005) Efficacy of alendronate, a bisphosphonate, in the treatment of AVN of the hip. A prospective open-label study. Rheumatol Oxf 44:352–359
Lai KA, Shen WJ, Yang CY (2005) The use of alendronate to prevent early collapse of the femoral head in patients with nontraumatic osteonecrosis. A randomized clinical study. J Bone Joint Surg Am 87:2155–2159
Nishii T, Sugano N, Miki H et al (2006) Does alendronate prevent collapse in osteonecrosis of the femoral head? Clin Orthop Rel Res 443:273–279
Agarwala S, Shah S, Joshi VR (2009) The use of alendronate in the treatment of avascular necrosis of the femoral head. J Bone Joint Surg 91-B:1013–1018
Kang P, Pei F, Shen B et al (2012) Are the results of multiple drilling and alendronate for osteonecrosis of the femoral head better than those of multiple drilling? A pilot study. Joint Bone Spine 79:67–72
Glueck CJ, Freiberg RA, Sieve L et al (2005) Enoxaparin prevents progression of stages I and II osteonecrosis of the hip. Clin Orthop Relat Res 435:164–170
Nagasawa K, Tada Y, Koarada S et al (2006) Prevention of steroid-induced osteonecrosis of femoral head in systemic lupus erythematosus by anti-coagulant. Lupus. 15:354–357
Ajmal M, Matas AJ, Kuskowski M, Cheng EY et al (2009) Does statin usage reduce the risk of corticosteroid-related osteonecrosis in renal transplant population? Orthop Clin North Am 40:235–239
Pritchett JW (2001) Statin therapy decreases the risk of osteonecrosis in patients receiving steroids. Clin Orthop Relat Res 386:173–178
Reis ND, Schwartz O, Militianu D et al (2003) Hyperbaric oxygen therapy as a treatment for stage-I avascular necrosis of the femoral head. J Bone Joint Surg Br 85:371–375
Strauss M, Dvozak T (1999) Femoral head necrosis and hyperbaric oxygen therapy. In: Kindwall EP, Whelan HT (eds) Hyperbaric medicine practice. Best publishing practice. pp 909–926
Strauss MB (1995) A “meta-analysis” and economic appraisal of osteonecrosis of the femoral head treated with hyperbaric oxygen. ARCO News 7:110
Ludwig J, Lauber S, Lauber HJ, Dreisilker U, Raedel R, Hotzinger H et al (2001) High-energy shock wave treatment of femoral head necrosis in adults. Clin Orthop Relat Res 387:119–126
Russo S, Galsso O, Gigliotti S (1999) Shock wave therapy for the treatment of nip necrosis. ESMST/2nd Internat. Congress of the European Society for Musculoskeletal Shock Wave Therapy, London (Proceedings)
Wang CJ, Wang FS, Huang CC et al (2005) Treatment for osteonecrosis of the femoral head: comparison of extracorporeal shock waves with core decompression and bone-grafting. J Bone Joint Surg Am 87:2380–2387
Chen JM, Hsu SL, Wong T et al (2008) Functional outcomes of bilateral hip necrosis: total hip arthroplasty versus extracorporeal shockwave. Arch Orthop Trauma Surg 129:837–841
Wang CJ, Wang FS, Yang KD et al (2008) Treatment of osteonecrosis of the hip: comparison of extracorporeal shockwave with shockwave and alendronate. Arch Orthop Trauma Surg 128:901–908
Aaron RK, Steinberg ME (1991) Electrical stimulation of osteonecrosis of the femoral head. Semin Arthroplasty 2:214–221
Bassett CA, Schink-Ascani M, Lewis SM (1989) Effects of pulsed electromagnetic fields on Steinberg ratings of femoral head osteonecrosis. Clin Orthop Relat Res 246:172–185
Lluch BC, García-Andrade DG, López-Oliva Muñoz F et al (1996) Utilidad de los campos electromagnéticos en el tratamiento de la necrosis avascular de cadera: estudio prospectivo de 30 casas. Rev Clin Esp 2:67–74
Massari L, Fini M, Cadossi R et al (2006) Biophysical stimulation with pulsed electromagnetic fields in osteonecrosis of the femoral head. J Bone Joint Surg Am 88:56–60
Steinberg ME, Brighton CT, Corces A et al (1989) Osteonecrosis of the femoral head. Results of core decompression and grafting with and without electrical stimulation. Clin Orthop Relat Res 249:199–208
Steinberg ME, Brighton CT, Bands RE et al (1990) Capacitive coupling as an adjunctive treatment for avascular necrosis. Clin Orthop Relat Res 261:11–18
Aaron RK, Lennox D, Bunce GE et al (1989) The conservative treatment of osteonecrosis of the femoral head. A comparison of core decompression and pulsing electromagnetic fields. Clin Orthop Relat Res 249:209–218
Im GI, Kim DY, Shin JH et al (2000) Degeneration of the acetabular cartilage in osteonecrosis of the femoral head: histopathologic examination of 15 hips. Acta Orthop Scand 71:28–30
Kawate K, Yajima H, Sugimoto K et al (2007) Indications for free vascularized fibular grafting for the treatment of osteonecrosis of the femoral head. BMC Musculoskelet Disord 8:78
Berend KR, Gunneson EE, Urbaniak JR (2003) Free vascularized fibular grafting for the treatment of postcollapse osteonecrosis of the femoral head. J Bone Joint Surg Am 85:987–993
Yoo MC, Kim KI, Hahn CS et al (2008) Long-term followup of vascularized fibular grafting for femoral head necrosis. Clin Orthop Relat Res 466:1133–1140
Fang T, Zhang EW, Sailes FC et al (2013) Vascularized fibular grafts in patients with avascular necrosis of femoral head: a systematic review and meta-analysis. Arch Orthop Trauma Surg 133:1–10
Schneider W, Breitenseher M, Engel A et al (2000) Der Stellenwert der Bohrung in der Behandlung der Hüftkopfnekrose. Orthopäde 29:420–429
Beltran J, Knight CT, Zuelzer WA (1990) Core decompression for avascular necrosis of the femoral head: correlation between long-term results and preoperative MR staging. Radiology 175:533–536
Scully SP, Aaron RK, Urbaniak JR (1998) Survival analysis of hips treated with core decompression or vascularized fibular grafting because of avascular necrosis. J Bone Joint Surg Am 80:1270–1275
Maniwa S, Nishikori T, Furukawa S et al (2000) Evaluation of core decompression for early osteonecrosis of the femoral head. Arch Orthop Trauma Surg 120:241–244
Lavernia CJ, Sierra RJ (2000) Core decompression in atraumatic osteonecrosis of the hip. J Arthroplasty 15:171–178
Saito S, Ohzono K, Ono K (1988) Joint-preserving operations for idiopathic avascular necrosis of the femoral head. Results of core decompression, grafting and osteotomy. J Bone Joint Surg Br 70:78–84
Mont MA, Carbone JJ, Fairbank AC (1996) Core decompression versus nonoperative management for osteonecrosis of the hip. Clin Orthop Relat Res 324:169–178
Steinberg ME, Brighton CT, Hayken GD (1985) Electrical stimulation in the treatment of osteonecrosis of the femoral head—a 1-year follow-up. Orthop Clin North Am 16:747–756
Trancik T, Lunceford E, Strum D (1990) The effect of electrical stimulation on osteonecrosis of the femoral head. Clin Orthop Relat Res 256:120–124
Mont MA, Jones LC, Seyler TM et al (2007) New treatment approaches for osteonecrosis of the femoral head: an overview. Instr Course Lect 56:197–212
Steinberg ME, Larcom PG, Strafford B (2001) Core decompression with bone grafting for osteonecrosis of the femoral head. Clin Orthop Relat Res 386:71–78
Gangji V, Hauzeur JP, Matos C et al (2004) Treatment of osteonecrosis of the femoral head with implantation of autologous bone-marrow cells. A pilot study. J Bone Joint Surg Am 86:1153–1160
Hernigou P, Beaujean F (2002) Treatment of osteonecrosis with autologous bone marrow grafting. Clin Orthop Relat Res 405:14–23
Mont MA, Etienne G, Ragland PS (2003) Outcome of nonvascularized bone grafting for osteonecrosis of the femoral head. Clin Orthop Relat Res 417:84–92
Mont MA, Einhorn TA, Sponseller PD et al (1998) The trapdoor procedure using autogenous cortical and cancellous bone grafts for osteonecrosis of the femoral head. J Bone Joint Surg Br 80:56–62
Kim SY, Kim YG, Kim PT et al (2005) Vascularized compared with nonvascularized fibular grafts for large osteonecrotic lesions of the femoral head. J Bone Joint Surg Am 87:2012–2018
Garberina MJ, Berend KR, Gunneson EE et al (2004) Results of free vascularized fibular grafting for femoral head osteonecrosis in patients with systemic lupus erythematosus. Orthop Clin North Am 35:353–357
Yen CY, Tu YK, Ma CH et al (2006) Osteonecrosis of the femoral head: comparison of clinical results for vascularized iliac and fibula bone grafting. J Reconstr Microsurg 22:21–24
Chen W, Zhang F, Chang SM (2006) Microsurgical fibular flap for treatment of avascular necrosis of the femoral head. J Am Coll Surg 202:324–334
Kane SM, Ward WA, Jordan LC et al (1996) Vascularized fibular grafting compared with core decompression in the treatment of femoral head osteonecrosis. Orthopedics 19:869–872
Soucacos PN, Beris AE, Malizos K (2001) Treatment of avascular necrosis of the femoral head with vascularized fibular transplant. Clin Orthop Relat Res 386:120–130
Yoo MC, Chung DW, Hahn CS (1992) Free vascularized fibula grafting for the treatment of osteonecrosis of the femoral head. Clin Orthop Relat Res 277:128–138
Plakseychuk AY, Kim SY, Park BC et al (2003) Vascularized compared with nonvascularized fibular grafting for the treatment of osteonecrosis of the femoral head. J Bone Joint Surg Am 85-A:589–596
Urbaniak JR, Coogan PG, Gunneson EB et al (1995) Treatment of osteonecrosis of the femoral head with free vascularized fibular grafting. A long-term follow-up study of one hundred and three hips. J Bone Joint Surg Am 77:681–694
Eward WC, Rineer CA, Urbaniak JR et al (2012) The vascularized fibular graft in precollapse osteonecrosis: is long-term hip preservation possible? Clin Orthop Relat Res 470:2819–2826
Meyers MH (1985) Osteonecrosis of the femoral head treated with the muscle pedicle graft. Orthop Clin North Am 16:741–745
Schneider W, Aigner N, Pinggera O, Knahr K (2002) Intertrochanteric osteotomy for avascular necrosis of the head of the femur. Survival probability of two different methods. J Bone Joint Surg Br 84:817–824
Hasegawa Y, Sakano S, Iwase T et al (2003) Pedicle bone grafting versus transtrochanteric rotational osteotomy for avascular necrosis of the femoral head. J Bone Joint Surg Br 85:191–198
Shuler MS, Rooks MD, Roberson JR (2007) Porous tantalum implant in early osteonecrosis of the hip: preliminary report on operative, survival, and outcomes results. J Arthroplasty 22:26–31
Tsao AK, Roberson JR, Christie MJ et al (2005) Biomechanical and clinical evaluations of a porous tantalum implant for the treatment of early-stage osteonecrosis. J Bone Joint Surg Am 87(Suppl 2):22–27
Johannson HR, Zywiel MG, Marker DR et al (2011) Osteonecrosis is not a predictor of poor outcomes in primary total hip arthroplasty: a systematic literature review. Int Orthop 35:465–473
Kawasaki M, Hasegawa Y, Sakano S et al (2005) Total hip arthroplasty after failed transtrochanteric rotational osteotomy for avascular necrosis of the femoral head. J Arthroplasty 20:574–579
Lim SJ, Moon YW, Eun SS et al (2008) Total hip arthroplasty using the S-ROM modular stem after joint-preserving procedures for osteonecrosis of the femoral head. J Arthroplasty 23:495–501
Beckmann J, Rader C, Lüring C et al (2010) Endoprothetische Gelenkersorgung bei Hüftkopfnekrose. Osteologie 19:46–52
Ritter MA, Helphinstine J, Keating EM et al (1997) Total hip arthroplasty in patients with osteonecrosis. The effect of cement techniques. Clin Orthop Relat Res 338:94–99
Davis ET, McKee MD, Waddell JP et al (2006) Total hip arthroplasty following failure of free vascularized fibular graft. J Bone Joint Surg Am 88(Suppl 3):110–115
Radl R, Hungerford M, Materna W et al (2005) Higher failure rate and stem migration of an uncemented femoral component in patients with femoral head osteonecrosis than in patients with osteoarthrosis. Acta Orthop 76:49–55
Mont MA, Seyler TM, Plate JF et al (2006) Uncemented total hip arthroplasty in young adults with osteonecrosis of the femoral head: a comparative study. J Bone Joint Surg Am 88(Suppl 3):104–109
Stulberg BN, Fitts SM, Zadzilka JD et al (2009) Resurfacing arthroplasty for patients with osteonecrosis. Bull NYU Hosp Jt Dis 67:138–141
Mont MA, Seyler TM, Marker DR, Marulanda GA, Delanois RE et al (2006) Use of metal-on-metal total hip resurfacing for the treatment of osteonecrosis of the femoral head. J Bone Joint Surg Am 88(Suppl 3):90–97
Beaule PE, Amstutz HC, Le Duff M et al (2004) Surface arthroplasty for osteonecrosis of the hip: hemiresurfacing versus metal-on-metal hybrid resurfacing. J Arthroplasty 19(Suppl 3):54–58
Chan YS, Shih CH (2000) Bipolar versus total hip arthroplasty for hip osteonecrosis in the same patient. Clin Orthop Relat Res 379:169–177
Chiu KH, Shen WY, Ko CK et al (1997) Osteonecrosis of the femoral head treated with cementless total hip arthroplasty. A comparison with other diagnoses. J Arthroplasty 12:683–688
D’Antonio JA, Capello WN, Manley MT et al (1997) Hydroxyapatite coated implants. Total hip arthroplasty in the young patient and patients with avascular necrosis. Clin Orthop Relat Res 344:124–138
Kim YH, Oh SH, Kim JS et al (2003) Contemporary total hip arthroplasty with and without cement in patients with osteonecrosis of the femoral head. J Bone Joint Surg Am 85-A:675–681
Ortiguera CJ, Pulliam IT, Cabanela ME et al (1999) Total hip arthroplasty for osteonecrosis: matched-pair analysis of 188 hips with long-term follow-up. J Arthroplasty 14:21–28
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Potential conflict of interest statements have been declared and can be found online on pages 87–93 of the full length German S3 guideline. (http://www.awmf.org/leitlinien/detail/ll/033-050.html). Prof. Andreas Roth: Advisory board Ceramtec, member of a study regarding measurement of periprosthetic ´bone density with Servier in 2012-2014. Johannes Beckmann: Referent for DePuy, Aesculap, ConforMIS and Brainlab, project together with ConforMIS 2006-2009. Prof. Dr. Klaus Bohndorf: Fee for a Symposium with Braun in 2013, shares from Boston Imaging Lab. Dr. Alexander Fischer: nothing. Prof. Christian Heiß: Advisory board Stryker, fee from Amgen, Novartis, Arthrex, Biomet, Projects with Stryker, Aap and Biomet. Prof. Werner Kenn: nothing. Prof. Marcus Jäger: Reports, projects an fee from/with Braun, Aesculap and DePuy. Priv.-Doz. Dr. Uwe Maus: Fee from Lilly, Servier, Abb Vie and Amgen. Prof. Ulrich Nöth: Fee from Lilly, Servier, Abb Vie and Amgen. Prof. Klaus M. Peters: Fee from Amgen, Lilly, Servier, Humantis, shares from Amgen and Sonofi, Project with Amgen. Prof. Christof Rader: nothing. Dr. med. Stephan Reppenhagen: nothing. Prof. Ulrich Smolenski: Reports and fees from several companies. Prof. Markus Tingart: nothing. Prof. Ina Kopp: nothing. Dozent Ivan Sirotin: nothing. Prof. Steffen J. Breusch: nothing.
Rights and permissions
About this article

Cite this article
Roth, A., Beckmann, J., Bohndorf, K. et al. S3-Guideline non-traumatic adult femoral head necrosis. Arch Orthop Trauma Surg 136, 165–174 (2016). https://doi.org/10.1007/s00402-015-2375-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-015-2375-7